Introduction
Lens-induced glaucoma was initially described by Dr Harold Gifford in 1900 as glaucoma associated with hypermature senile cataracts. Around the same time, Dr August Leopold von Ruess independently described lens-induced glaucoma as glaucoma with spontaneous absorption of lens matter through an intact capsule.[1] The literature has described numerous similar entities over the decades. In modern practice, lens-induced glaucoma represents a significant subset of secondary glaucomas that arise when pathological changes in the crystalline lens cause an abnormal rise in intraocular pressure (IOP). Lens-induced glaucoma mimics acute angle-closure glaucoma and is characterized by normal IOP and open angles in the contralateral eye. The condition is associated with prompt symptom relief following cataract extraction.
Historically, lens-induced glaucoma referred primarily to 2 main subtypes (phacolytic and phacomorphic glaucoma), but evolving understanding has expanded the classification to more broadly categorize by pathogenesis—lens protein–related or aqueous flow obstruction–related—in order to include lens particle glaucoma and phacoanaphylactic glaucoma under the former, and glaucomas related to lens subluxation or dislocation under the latter. Some additional causes, such as pseudoexfoliation glaucoma and ciliary block glaucoma, are controversial entities that are sometimes included under lens-induced glaucoma. While these conditions involve the lens in their pathophysiology, the lens is not the primary driver of IOP elevation.[2] Regardless of subtype, the final common pathway involves obstruction of aqueous outflow through the trabecular meshwork or narrowing of the anterior chamber angle.
Classifications of Lens-Induced Glaucoma
Lens protein–related
These include leakage of lens protein across an intact or breached lens capsule:
- Phacolytic glaucoma
- Lens particle–induced glaucoma
- Phacoanaphylactic glaucoma (also known as lens-induced uveitic or phacoantigenic glaucoma)
The first category of lens-induced glaucomas is associated with lens protein leakage. Phacolytic glaucoma typically occurs in eyes with hypermature cataracts, in which leakage of high-molecular-weight lens proteins through microscopic capsular defects induces macrophage-mediated obstruction of the trabecular meshwork. The anterior chamber remains deep, but proteinaceous material, large macrophages, and flare can be seen swirling within the aqueous. Another subtype in this category is lens particle glaucoma, which arises when cortical or nuclear fragments enter the anterior chamber, often after cataract surgery, trauma, or spontaneous capsular rupture. These fragments mechanically obstruct the trabecular meshwork and induce secondary inflammation, which further impedes aqueous flow. Phacoanaphylactic glaucoma, sometimes referred to as lens-induced uveitic or phacoantigenic glaucoma, is a relatively rare immune-mediated variant characterized by a granulomatous reaction to lens proteins following trauma or surgical disruption of the lens capsule, resulting in severe uveitis and trabeculitis.
Aqueous flow obstruction
These include an anatomical obstruction of aqueous flow from the posterior to the anterior chamber:
- Phacomorphic glaucoma
- Pupillary block glaucoma, which includes lens displacement–related cases previously termed phacotopic glaucoma [3]
The second category of lens-induced glaucoma is characterized by anatomical obstruction of aqueous flow. Phacomorphic glaucoma results from an intumescent cataractous lens that pushes the iris forward, causing shallowing of the anterior chamber and relative pupillary block. This mechanical obstruction initiates an acute angle-closure crisis, often accompanied by corneal edema, severe pain, and rapidly rising IOP.[4] In contrast, pupillary block glaucoma develops when the lens becomes subluxated or dislocated, either from trauma, zonular weakness, pseudoexfoliation, or systemic connective tissue disorders, leading to angle closure or direct mechanical obstruction of the aqueous pathways.[4] This type includes the lens displacement–related entity historically known as phacotopic glaucoma.
Clinically, patients with lens-induced glaucoma typically present with sudden ocular pain, conjunctival injection, photophobia, and decreased vision, and they often have accompanying nausea or headache. Examination often reveals elevated IOP, corneal edema hampering visualization, conjunctival congestion, and a mid-dilated or sluggish pupil. Differentiating lens-induced glaucoma from primary acute angle-closure glaucoma is essential because the immediate management priorities differ. In lens-induced glaucomas related to aqueous flow obstruction, the anterior chamber is markedly shallow with a swollen lens evident on slit-lamp examination.
In contrast, in lens protein–related types, the chamber is deep with intense flare, floating white particles, and a hypermature or Morgagnian cataract. Lens particle glaucoma may reveal retained cortical material or nuclear chips, whereas phacoanaphylactic glaucoma presents with granulomatous keratic precipitates and a severe anterior chamber reaction. In eyes with media opacity precluding visualization of the posterior segment, B-scan ultrasonography is a valuable tool for excluding retinal detachment and assessing lens position.[5] Timely diagnosis is essential because sustained IOP elevation can rapidly damage the optic nerve. Training ophthalmologists to recognize early intumescent cataracts, hypermaturity, zonular weakness, or retained lens matter is essential for preventing complications.[6]
Initial management of lens-induced glaucoma focuses on lowering IOP with topical aqueous suppressants, hyperosmotic agents, and systemic medications, while concurrently controlling inflammation. Miotics and prostaglandin analogues are typically avoided in specific subtypes due to the risk of worsening the pupillary block or inflammation, respectively. However, medical therapy alone is only a temporary measure; definitive treatment requires removal of the pathological lens. Early cataract extraction via small-incision cataract surgery or phacoemulsification relieves pupillary block, eliminates lens-derived proteins or particles, and restores normal aqueous outflow.
Surgical challenges may include severe corneal edema, shallow chambers, zonular instability, or the friability of hypermature lenses.[5] Experienced surgical technique and careful intraoperative fluid management are therefore essential. Postoperative inflammation and pressure spikes must be anticipated and managed promptly. The visual prognosis varies with the duration of elevated IOP, the degree of optic nerve damage, and the presence of comorbid ocular disease.
Advances in cataract surgery have reduced the global incidence of lens-induced glaucoma, although certain forms (especially lens particle glaucoma after cataract surgery) persist across all populations. However, the condition remains a significant clinical problem in many low-resource regions, especially in rural parts of India, Nepal, sub-Saharan Africa, and Southeast Asia. Because age-related cataracts may remain asymptomatic until the onset of acute glaucoma, cataracts frequently progress unchecked in areas without accessible screening, resulting in late-stage presentations.
The pursuit of cataract surgery may be further delayed by limited access to ophthalmic services, financial barriers, sociocultural beliefs, lack of awareness, and geographic challenges. Women and older individuals in rural regions are disproportionately affected, often presenting only when pain and severe visual loss compel emergency care attendance. In such settings, cataracts often reach an intumescent or hypermature stage, leading to mechanical, inflammatory, or immunological disturbances that obstruct aqueous outflow or induce pupillary block. These mechanisms can trigger acute, severe elevations in IOP that threaten optic nerve function and result in irreversible blindness if not promptly managed.
From a public health perspective, the potential to eliminate lens-induced glaucoma as a cause of preventable blindness becomes increasingly attainable as surgical techniques continue to advance. As the global population ages, early identification and management of advanced cataracts will be vital to reducing the global burden of lens-induced glaucoma.[7] Strengthened community outreach, cataract screening programs, simplified referral pathways, and timely surgical intervention are critical to reducing morbidity. However, despite declining prevalence in high-resource countries, the global rise in longevity and persistent disparities in healthcare distribution ensure that lens-induced glaucomas will remain clinically relevant for the foreseeable future.[8] Until equitable access to timely cataract care is universal, lens-induced glaucoma will remain a significant clinical and public health concern, requiring vigilance, early diagnosis, and timely management to preserve vision.[9]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Lens-induced glaucoma develops when progressive cataract changes alter the anatomical and biochemical environment of the anterior segment, thereby obstructing aqueous outflow or causing pupillary block. Prolonged cataract maturation increases capsular permeability, the risk of protein leakage, zonular instability, and phacolytic or phacomorphic mechanisms.[10] The underlying etiology varies by subtype, but all mechanisms share a common pathway: increased IOP resulting from impaired aqueous humor drainage (see Table 1).[2]
The first 3 forms of lens-induced glaucoma are related to lens protein leakage:
- Phacolytic ecmhanism (hypermature cataract leakage)
- In hypermature or Morgagnian cataracts, the lens capsule becomes fragile. High-molecular-weight lens proteins leak into the anterior chamber, triggering macrophage recruitment. Swollen macrophages then obstruct the trabecular meshwork, reducing aqueous outflow and sharply elevating IOP. The chamber depth remains regular or deep (see Image. Phacolytic Glaucoma).[11]
- Lens particle–induced mechanism (retained lens matter)
- Following cataract surgery, trauma, or spontaneous capsular rupture, cortical or nuclear lens fragments may enter the anterior chamber. These particles directly obstruct trabecular outflow and induce secondary inflammatory trabeculitis, thereby elevating IOP (see Image. Lens Particle Glaucoma).[12]
- Phacoanaphylactic (lens-induced uveitic) mechanism
- This subtype is an immune-mediated granulomatous reaction to exposed lens proteins after surgery or trauma, resulting in intense anterior uveitis. Fibrin and inflammatory cells, particularly macrophages, clog the trabecular meshwork, dramatically reducing aqueous outflow (see Image. Phacoanaphylactic Glaucoma).[13]
The additional 2 forms of lens-induced glaucoma relate to mechanical obstruction of aqueous flow:
- Phacomorphic mechanism (intumescent lens)
- As a cataract matures, osmotic changes cause the lens to swell. The increased lens volume pushes the iris anteriorly, narrows the anterior chamber angle, and produces a relative pupillary block. This culminates in acute angle-closure glaucoma, often associated with severe pain, corneal edema, and markedly elevated IOP (see Image. Phacomorphic Glaucoma).[8]
- Pupillary block mechanism (lens subluxation/dislocation) (includes the mechanism previously known as phacotopic)
- Zonular dialysis caused by trauma, pseudoexfoliation, or systemic connective-tissue disorders (eg, Marfan, homocystinuria) results in a displaced lens. The dislocated or subluxated lens may:
- Block the pupil
- Tilt forward, causing the angle to narrow
- Mechanically obstruct the trabecular meshwork [2]
- Zonular dialysis caused by trauma, pseudoexfoliation, or systemic connective-tissue disorders (eg, Marfan, homocystinuria) results in a displaced lens. The dislocated or subluxated lens may:
Table 1. Etiologic Classification of Lens-Induced Glaucoma
|
Glaucoma Subtype |
Primary Etiology |
Pathophysiology |
Anterior Chamber |
Key Features |
|
Phacolytic |
Hypermature cataract leaks proteins |
Macrophage-mediated trabecular meshwork (TM) obstruction |
Deep |
Floating proteinaceous material, high flare |
|
Lens Particle–Induced |
Retained cortical fragments (post-surgery/trauma) |
TM blockage by particles + inflammation |
Variable |
Visible fragments, typically postoperative onset |
|
Phacoanaphylactic |
Immune reaction to lens proteins |
Granulomatous uveitis + trabeculitis |
Deep |
Keratic precipitates, fibrin, and severe inflammation |
|
Phacomorphic |
Intumescent cataract | Pupillary block + iris bombe | Shallow | Severe angle closure, pain, corneal edema |
|
Pupillary Block (Phacotopic) |
Lens subluxation/dislocation |
Pupillary block or angle obstruction |
Variable |
Irregular lens position, phacodonesis |
Congenital ectopia lentis can lead to obstruction of aqueous outflow, predisposing affected individuals to lens-induced glaucoma. Various forms include the following:
- Marfan syndrome: Bilateral supero-temporal subluxation of the lens with occasional acute dislocation and primary bilateral glaucoma (PBG) in early childhood [14]
- Homocystinuria: Bilateral inferonasal lenticular subluxation with acute anterior chamber dislocation and PBG [15]
- Weill-Marchesani syndrome: Associated with microspherophakia, ciliary body hypoplasia, PBG, and inverse glaucoma
- Others: Ehler-Danlos syndrome, sulfite oxidase deficiency, hyperlysinemia, aniridia, Alport syndrome, Axenfeld-Rieger syndrome, and Peter anomaly type 3
Acquired causes of lens-induced glaucoma include the following:
- Trauma: Traumatic injury can directly cause anterior lens dislocation and PBG, and lens capsule rupture can cause immediate lens particle–induced glaucoma (LPIG) or delayed phacomorphic angle-closure glaucoma (PAG).
- Post cataract surgery: Retained loose lenticular matter can precipitate an acute attack of LPIG or a chronic PAG.
- Iatrogenic (intraocular procedures): Accidental rupture of the lens capsule can occur during anterior chamber procedures (eg, laser-assisted iridotomy, intracameral injections, trabeculectomy, minimally invasive glaucoma surgeries), posterior lamellar corneal surgeries, or posterior segment procedures (eg, intravitreal injections, pars plana vitrectomy), leading to immediate LPIG or a delayed PAG.
- Intumescent cataract: The enlarged lens may cause phacomorphic glaucoma (PMG), particularly in settings of delayed surgical intervention or limited access to cataract care.
- Hypermature senile cataract: Micro-ruptures in the lens capsule allow leakage of lens proteins, resulting in PLG.[3]
- Zonular weakness or capsular fragility: Systemic conditions affecting the zonules, pseudoexfoliation (PXF) syndrome, and chronic uveitis may predispose to lens subluxation, dislocation, or capsular compromise, increasing the risk of pupillary block glaucoma or lens protein–related glaucoma (see Table 2).[16]
Table 2. Risk Factors for Lens-Induced Glaucoma
|
Category |
Details |
|
Age-related |
Hypermature cataracts, Morgagnian cataracts |
|
Socioeconomic |
Limited access to surgery, rural residence, low awareness |
|
Ocular |
Trauma, pseudoexfoliation, uveitis, retained lens matter |
|
Surgical |
Incomplete lens removal, capsular rupture |
|
Systemic |
Marfan syndrome, homocystinuria, connective tissue disorders |
|
Anatomical |
Small eyeball, shallow anterior chamber, weak zonules |
Epidemiology
Lens-induced glaucoma remains a significant cause of secondary glaucoma globally, although its epidemiology varies significantly between high-, low-, and middle-income countries. The condition is strongly associated with untreated cataract progression, delayed access to surgical care, and demographic factors such as age, socioeconomic status, and geographic location. As a result, its frequency is highest in regions where uptake of cataract surgery is low or significantly delayed.[3] In low-resource countries with more limited access, acquired lens-induced glaucoma from advanced age-related cataracts is the more prevalent subtype. The incidence of lens-induced glaucoma is up to 2.4% at the time of the presentation of age-related cataracts, with a greater preponderance in women.[1] In contrast, the estimated prevalence of congenital ectopia lentis is 6.4 per 100,000 population.[17]
Globally, lens-induced glaucoma accounts for 3% to 10% of all secondary glaucomas, with the highest burden observed in South Asia, Southeast Asia, and sub-Saharan Africa. In rural Indian studies, lens-induced glaucoma may represent 9% to 14% of all acute glaucoma admissions, particularly in underserved populations. Numerous screening programs in India and Nepal have identified hypermature and intumescent cataracts as major precursors of lens-induced glaucoma, reflecting the persistence of late-stage cataracts in these regions. Worldwide, the condition remains tightly linked to the prevalence of age-related hypermature cataracts, which disproportionately affect populations with limited access to surgical ophthalmic care.[2]
In contrast, the incidence of lens-induced glaucoma in high-income countries such as the United States (US), Canada, Japan, and Western Europe is markedly lower. Improved access to cataract surgery, insurance coverage, routine ophthalmic evaluations, and public awareness initiatives have significantly reduced progression to hypermaturity. In the US, lens-induced glaucoma accounts for less than 1% of all glaucoma cases, and acute presentations are rare. However, specific variants (most notably lens particle glaucoma following cataract surgery or trauma) may still occur even in advanced healthcare settings. These cases often result from retained cortical material or delayed postoperative follow-up rather than cataract neglect.[8]
Sex distribution of lens-induced glaucoma varies by region and reflects broader disparities in access to cataract care rather than biological predisposition. Globally, women are disproportionately affected, especially in rural Asia and Africa. In many low-resource settings, women have significantly less access to cataract surgery due to socioeconomic factors, cultural roles, or mobility limitations. As a result, hypermature cataracts and subsequent lens-induced glaucomas occur more frequently in older women, with female-to-male ratios reported between 1.3:1 and 1.8:1 in several community-based studies. However, in regions with equitable healthcare access, such as the US and Western Europe, lens-induced glaucoma does not show a meaningful sex-based predilection.[4]
The epidemiology of lens subluxation–related glaucomas (PBG, or "phacotopic") shows a different pattern (see Table 3). This subset is more common in regions with high prevalence of trauma, pseudoexfoliation syndrome, and hereditary connective tissue disorders. In areas such as Nepal, northern India, and Kurdish regions where PXF is endemic, lens subluxation contributes meaningfully to lens-induced glaucoma burden.
Age remains the strongest epidemiologic determinant (see Table 4). Lens-induced glaucoma primarily affects older individuals with long-standing age-related cataracts. The typical age at presentation in low- and middle-income countries ranges from 60 to 80 years, although cases in the 50 to 60-year age group are increasing in some regions due to earlier cataract onset associated with diabetes, ultraviolet exposure, steroid use, and nutritional deficiencies. In high-income countries, lens particle glaucoma can present at any adult age following cataract surgery, trauma, or complicated procedures. In contrast, phacomorphic and phacolytic variants are typically restricted to individuals in the oldest age strata who have avoided or deferred surgery.[7]
Globally, population aging is expected to increase the number of individuals with cataracts, particularly in Asia and Africa, thereby sustaining the risk of lens-induced glaucoma. According to projections from the World Health Organization, the burden of cataract blindness in low-resource settings is increasing among older adults, who are living longer but may still lack timely access to cataract care. Consequently, although cataract surgery volumes have increased worldwide, the absolute number of people at risk for lens-induced glaucoma remains high in underserved regions.[5]
Rural–urban differences also strongly influence epidemiology. Rural communities, particularly in low-income countries, exhibit significantly higher rates of hypermature cataracts and lens-induced glaucoma due to limited hospital access, long travel distances, a shortage of ophthalmologists, and cultural preferences for home-based or traditional treatments. Studies from India, Nepal, Pakistan, and Ethiopia consistently show a 2 to 4 times higher risk of lens-induced glaucoma in rural versus urban populations.[18]
Socioeconomic status further modifies epidemiologic patterns. Individuals from lower-income groups are more likely to delay cataract surgery due to financial constraints, fear of surgery, or lack of awareness. Community-based surveys have shown that patients presenting with lens-induced glaucoma often have no prior ophthalmic consultation, reinforcing the role of access barriers in disease progression.
Ethnic variation in lens-induced glaucoma prevalence largely parallels global cataract epidemiology. Populations with higher cataract burdens (eg, South Asian and East African) exhibit higher frequencies of lens-induced glaucoma. In the US, racial disparity is less pronounced, although Black and Latino populations exhibit higher rates of postoperative retained lens matter and trauma-related lens complications, potentially influencing the epidemiology of lens particle glaucoma.[19]
Overall, while lens-induced glaucoma is rare in the US and other high-income nations, it remains a significant public health concern in low- and middle-income countries, particularly among older women in rural communities. The frequency of this condition is closely linked to cataract maturity, access to surgical services, population awareness, and age distribution. As global aging and diabetes prevalence rise, the natural incidence of cataract is expected to increase further, underscoring the need for continued public health strategies aimed at timely cataract detection and surgery to prevent the avoidable morbidity of lens-induced glaucoma.[20]
Table 3. Global Epidemiology of Lens-Induced Glaucoma
|
Region |
Prevalence of Lens Induced Galucoma |
Most Common Subtype |
Key Epidemiologic Drivers |
|
United States |
<1% |
Lens particle glaucoma (postoperative) |
High surgery access, rare hypermaturity |
|
Western Europe |
<1% |
Lens particle glaucoma |
Routine cataract extraction, aging population |
|
South Asia (India, Nepal, Bangladesh) |
9%–14% of acute glaucomas |
Phacomorphic, phacolytic |
Late presentation, low surgical access in rural areas |
|
Sub-Saharan Africa |
5%–10% |
Phacomorphic |
High cataract burden, low outreach services |
|
Southeast Asia (Myanmar, Indonesia, Vietnam) |
4%–8% |
Phacolytic |
High prevalence of hypermature cataracts |
|
Middle East |
2%–5% |
Pupillary block (due to trauma/pseudoexfoliation) |
High trauma incidence, pseudoexfoliation clusters |
|
Latin America |
1%–3% |
Mixed |
Variability in cataract care and follow-up |
Table 4. Sex- and Age-Based Distribution of Lens-Induced Glaucoma
|
Category |
Distribution / Findings |
Notes |
|
Sex Distribution (Global) |
Female > Male (1.3–1.8:1) |
Reflects poorer access to cataract surgery among women in rural areas |
|
Sex Distribution (United States/Europe) |
Equal |
Due to equitable surgical access |
|
Age Group Most Affected |
60–80 years |
Age-related cataract maturation is the primary driver |
|
Earlier Age Onset (50–60 years) |
More common in diabetes, chronic steroid use, and ultraviolet light exposure |
Seen more in South Asia and Africa |
|
Lens Particle Lens Induced Glaucoma (all countries) |
Occurs at any adult age |
Depends on surgical or trauma-related events |
|
Pupillary Block (Phacotopic) Lens-Induced Glaucoma |
Younger age possible |
Marfan, homocystinuria, trauma, pseudoexfoliation |
Pathophysiology
Lens-induced glaucoma encompasses a group of secondary glaucomas caused by structural and biochemical alterations of the crystalline lens that disrupt aqueous humor dynamics. Although each lens-induced glaucoma subtype has distinct initiating events, the final common pathway is obstruction of aqueous outflow due to mechanical crowding, trabecular meshwork (TM) blockage, or inflammatory trabeculitis, resulting in elevated IOP. The pathophysiology reflects a complex interaction between lens enlargement, capsular integrity, protein leakage, macrophage activation, zonular disruption, and anterior segment anatomy.[21] The first 3 forms of lens-induced glaucoma are related to lens protein leakage.
Phacolytic Glaucoma (Protein Leakage and Macrophage Blockade)
Phacolytic glaucoma (PLG) occurs in eyes with hypermature or Morgagnian cataracts, in which the lens cortex liquefies due to long-standing degeneration, leading to microscopic defects in the lens capsule that allow high-molecular-weight α-crystallin proteins to progressively leak into the anterior chamber. Flocks coined the term "phacolytic glaucoma", and Epstein described the role of high-molecular-weight lens protein (HMW-LP) in the pathogenesis of PLG.[22][23] These leaked proteins trigger an inflammatory response resulting in:
- Recruitment of macrophages
- Phagocytosis of leaked lens proteins
- Engorgement and impaired mobility of the macrophages
- Accumulation of macrophages and protein aggregates in the trabecular meshwork
The TM becomes clogged, producing severe outflow resistance and acute open-angle glaucoma. Unlike phacomorphic glaucoma, phacolytic glaucoma is characterized by a deep anterior chamber and open angles. Pupillary block is absent; the obstruction is purely at the TM level.[24][23] Clinically, phacolytic glaucoma presents with a red, painful eye and a floating white material (“milky fluid”) in the anterior chamber.
Key mechanisms:
- Lens protein leakage
- Macrophage activation
- TM blockage by protein-laden macrophages
- High IOP due to outflow failure
Notably, a recent theory posits that high-molecular-weight lipopolysaccharides (HMW-LPs) directly obstruct the TM, thereby impeding aqueous outflow and precipitating PLG. The increase in HMW-LP content in the human lens with age supports this theory.
Lens Particle–Induced Glaucoma (Mechanical Obstruction by Cortex/Nucleus)
LPIG occurs when cortical or nuclear fragments enter the anterior chamber after the lens capsule is breached, following:
- Cataract surgery (retained lens matter)
- Trauma
- Spontaneous capsule rupture in hypermature cataracts
In this subtype, lens particles directly obstruct the TM and induce secondary inflammatory trabeculitis, further reducing aqueous flow. The immune response leads to the accumulation of inflammatory cells, fibrin, and debris within the TM. IOP elevation may be acute or subacute, depending on particle load and inflammatory intensity.[4]
Key mechanisms:
- Direct TM obstruction by lens fragments
- Trabeculitis-induced edema of TM
- Secondary inflammation → increased outflow resistance
Because the inflammation in LPIG is secondary to lens capsule breach and subsequent mechanical obstruction by the released particulate lens material, the resulting uveitis is generally more pronounced than in phacolytic glaucoma.[7]
Phacoanaphylactic Glaucoma (Immune-Mediated Granulomatous Reaction)
PAG, sometimes referred to as lens-induced uveitic or phacoantigenic glaucoma, is a rare subtype that results from a type III hypersensitivity reaction to lens proteins after lens capsule rupture. The release of lens particles is similar to LPIG; however, in PAG, the immune system specifically recognizes previously sequestered lens proteins as foreign, triggering a granulomatous inflammatory response. The inflammation of the TM is mediated by an Arthus reaction (a subtype of type III hypersensitivity) involving immunoglobulin G and the complement system.[25] Verhoeff and Lemoine described this entity as endophthalmitis phacoanaphylactica.[26] This is the most immunologically active form of lens-induced glaucoma.
Histopathology shows:
- Giant cell reaction
- Macrophages and lymphocytes
- Zonular and capsular remnants surrounded by inflammatory cells
- Trabecular meshwork infiltration with inflammatory cells
Inflammatory trabeculitis reduces aqueous outflow and sharply increases IOP. There is a sensitization period of 1 to 14 days between the release of the glaucoma-causing agent and the onset of glaucoma.[27] Because the reaction may start days to weeks after surgery or trauma, the presentation may be delayed.
Key mechanisms:
- Autoimmune sensitization to lens proteins
- Granulomatous inflammation
- TM infiltration with immune cells
- Severe outflow obstruction
The additional 2 forms of lens-induced glaucoma are attributable to mechanical obstruction of aqueous outflow.
Phacomorphic Glaucoma (Mechanical Pupillary Block)
PMG develops when an intumescent swollen lens increases in anteroposterior diameter due to the osmotic hydration associated with advanced cataract maturation. As the lens enlarges, it pushes the iris diaphragm forward, resulting in:
- Shallowing of the anterior chamber
- Crowding of the iridocorneal angle
- Iris–lens apposition at the pupillary border
This process produces relative pupillary block, reducing aqueous movement from the posterior to the anterior chamber. Fluid accumulates behind the iris, causing iris bombe, which further narrows or closes the angle. Without intervention, the aqueous outflow decreases dramatically, leading to a rapid rise in IOP. Persistent angle closure may lead to peripheral anterior synechiae (PAS), rendering the condition irreversible over time.
Key mechanisms:
- Increased lens thickness
- Forward displacement of the iris
- Pupillary block → iris bombe
- Angle closure → trabecular outflow obstruction
This mechanism explains the classic presentation of acute, painful, angle-closure glaucoma with corneal edema in the setting of a sudden increase in the volume of a cataractous lens.[28] Clinically, acute angle-closure with a shallow anterior chamber and an open angle in the contralateral eye suggests PMG.[29]
Pupillary Block Glaucoma Due to Lens Displacement (Previously Termed Phacotopic Glaucoma)
In pupillary block glaucoma (historically termed phacotopic glaucoma), zonular weakness due to trauma, PXF, or systemic connective tissue disorders (eg, Marfan syndrome, homocystinuria, Weill-Marchesani syndrome) leads to displacement of the crystalline lens (ectopia lentis) and subsequent blockage of aqueous flow.[30] The lens may:
- Move forward
- Forward subluxation pushes the iris anteriorly, causing:
- Shallow anterior chamber
- Pupillary block
- Acute angle closure [7]
- Forward subluxation pushes the iris anteriorly, causing:
- Dislocate into the anterior chamber
- Direct obstruction of the pupil or TM by the lens
- Dislocate into the vitreous
- May cause reverse pupillary block or intermittent IOP spikes
Key mechanisms:
- Mechanical obstruction of the pupil
- Angle narrowing
- TM compression by a dislocated lens
This subtype is intensely mechanical and often presents acutely. Although phacomorphic and pupillary block (phacotopic) glaucomas arise from different initiating events (lens enlargement versus lens displacement), both ultimately produce pupillary block and secondary angle closure through mechanical obstruction of aqueous flow.
Final Common Pathway: Aqueous Outflow Failure → Elevated IOP
Regardless of the initiating mechanism, lens-induced glaucoma results in one of two final pathways:
Trabecular meshwork obstruction
Seen in:
- Phacolytic glaucoma
- Lens particle glaucoma
- Phacoanaphylactic glaucoma
Pupillary block → angle closure
Seen in:
- Phacomorphic glaucoma
- Anterior lens dislocation (eg, pupillary block glaucoma due to congenital ectopia lentis)
In both pathways, the result is a dramatic rise in IOP, which in some cases exceeds 40 to 60 mm Hg.
Sustained elevated IOP leads to:
- Optic nerve head ischemia
- Retinal ganglion cell apoptosis
- Irreversible glaucomatous optic neuropathy
- Acute loss of visual acuity
Additionally, corneal endothelial dysfunction due to elevated IOP causes corneal edema, further impairing visualization and delaying diagnosis.[4]
Anatomical Predispositions Compounding Pathophysiology
Certain anatomical factors increase susceptibility:
- Pre-existing shallow anterior chamber
- Hyperopic eyes (short axial length)
- Pseudoexfoliative zonulopathy
- Small corneal diameter
- Narrow drainage angles [31]
These factors reduce compensation when the lens enlarges or dislocates, causing earlier and more severe IOP spikes. (see Table 5).
Table 5. Comprehensive Comparison of All Subtypes of Lens-Induced Glaucoma
|
Feature |
Phacolytic Glaucoma |
Lens Particle Glaucoma |
Phacoanaphylactic Glaucoma |
Phacomorphic Glaucoma |
Pupillary Block Glaucoma (Includes Phacotopic) |
|
Primary Etiology |
Hypermature cataract with capsular micro-defects |
Retained cortical/nuclear lens matter after surgery or trauma |
Immune-mediated granulomatous reaction to lens proteins |
Intumescent swollen cataract |
Zonular weakness causing lens subluxation/dislocation (trauma, PXF, Marfan, homocystinuria) |
|
Underlying Mechanism |
Protein leakage → macrophage blockade of TM |
Mechanical TM obstruction + inflammatory trabeculitis |
Autoimmune inflammation → granulomatous TM obstruction |
Pupillary block → iris bombe → angle closure |
Mechanical angle obstruction or pupillary block from a displaced lens |
|
Anterior Chamber Depth |
Deep |
Variable |
Deep |
Shallow |
Variable (deep/shallow depending on lens position) |
|
Angle Status |
Open |
Open or partially blocked by debris |
Open but inflamed |
Closed or very narrow |
May be closed (anterior lens) or open (posterior dislocation) |
|
IOP Rise |
Very high |
High |
Very high |
Very high (often 40–60 mm Hg) |
High; intermittent or sustained |
|
Symptoms |
Pain, redness, blurry vision, milky AC fluid |
Pain, photophobia, and IOP spikes after surgery |
Pain, redness, photophobia, marked uveitis |
Severe pain, headache, halos, nausea, sudden vision drop |
Transient blurry vision, monocular diplopia, pain; history of trauma or PXF |
|
Key Signs |
Deep AC, floating white material, flare, hypermature cataract |
Visible lens fragments in AC, cells/flare |
Granulomatous KPs, fibrin, intense AC reaction |
Shallow AC, swollen lens, mid-dilated pupil, corneal edema |
Lens displacement, phacodonesis, zonular dialysis |
|
Gonioscopy |
Open angle |
Open angle with debris |
Open angle with inflammatory cells |
Closed angle |
Closed (if anterior displacement) or open (if posterior) |
|
Inflammation Level |
Moderate |
Moderate to severe |
Severe granulomatous uveitis |
Mild to moderate |
Mild unless traumatic |
|
Definitive Treatment |
Cataract extraction |
Removal of retained lens fragments |
Lens removal + intensive steroids |
Cataract extraction |
Lens repositioning/removal |
|
Initial IOP Control |
Aqueous suppressants |
Aqueous suppressants + steroids |
Steroids + aqueous suppressants |
Acetazolamide, beta-blockers, hyperosmotics |
Depends on mechanism (block vs TM) |
|
Role of Laser Iridotomy |
No role |
No role |
No role |
May help temporarily (only in relative block cases) |
Possible role if pupillary block is present |
|
Visual Prognosis |
Good if optic nerve preserved |
Good with the timely removal of fragments |
Variable; depends on inflammation severity |
Good if treated early; risk of PAS |
Variable; depends on zonular/retinal status |
|
Typical Patient Population |
Older adults with hypermature cataracts |
Any age (post-surgery/trauma) |
Post-trauma or post-surgery |
Older adults with swollen cataracts |
Patients with trauma, PXF, systemic CTD |
|
Complications |
Persistent inflammation, endothelial damage |
Chronic uveitis, prolonged IOP rise |
Cystoid macular edema, chronic inflammation |
PAS, irreversible angle closure |
Lens instability, retinal complications |
AC, anterior chamber; CTD, connective tissue disease; IOP, intraocular pressure; PXF, pseudoexfoliation; PAS, peripheral anterior synechiae; TM, trabecular meshwork
Histopathology
Lens-induced glaucoma encompasses several pathophysiological mechanisms, each with a characteristic histopathologic signature. Although all subtypes ultimately lead to elevated IOP and glaucomatous optic nerve damage, microscopic evaluation reveals distinct patterns involving the lens capsule, lens proteins, inflammatory cells, and the TM. These changes help differentiate between phacolytic, lens particle, phacoanaphylactic, phacomorphic, and pupillary block (phacotopic) glaucomas.[3]
Histopathology of Phacolytic Glaucoma
The hallmark of phacolytic glaucoma is protein leakage from a hypermature cataract through microscopic capsular defects.
Key microscopic features
- Lens
- Hypermature lens with liquefied cortex (“Morgagnian degeneration”)
- Thin, wrinkled capsule with microfissures
- Anterior chamber
- Abundant high-molecular-weight lens proteins
- Numerous macrophages containing ingested crystallin proteins, often swollen and vacuolated
- Trabecular meshwork
- Obstruction by macrophages, large protein globules, and fine granular material
- Reduced porosity of trabecular spaces
- Mild secondary trabeculitis
- Iris
- Mild inflammatory cell infiltration
- Cornea
- Endothelial cell stress and edema [32]
Phacolytic glaucoma is characterized by protein–macrophage trabecular obstruction, which explains the elevated IOP despite a deep anterior chamber.
Histopathology of Lens Particle Glaucoma
Lens particle glaucoma follows cataract surgery or trauma and involves retained cortical/nuclear fragments.
Key microscopic features
- Lens
- Extruded cortical material within the anterior chamber
- Pink, eosinophilic lens fragments, often with degenerating nuclei
- Inflammatory cells
- Prominent macrophages and neutrophils surrounding lens fragments
- Macrophages containing cortical debris (“phagocytic clusters”)
- Trabecular meshwork
- Mechanical obstruction by lens particles, inflammatory cells, and cellular debris
- Reactive trabeculitis with edema of TM beams
- Iris and ciliary body
- Moderate uveitis with vascular congestion
- Cornea
- Stromal edema from elevated IOP [33]
Lens particle glaucoma is a combination of mechanical obstruction + inflammatory TM dysfunction.
Histopathology of Phacoanaphylactic Glaucoma
This immune-mediated subtype involves a granulomatous hypersensitivity reaction to liberated lens proteins.
Key microscopic features
- Anterior chamber
- Dense granulomatous inflammation
- Giant cells, polymorphonuclear (PMNs) leukocytes, epithelioid histiocytes, and lymphocytes
- Fibrinous exudate
- Lens material
- Residual fibers surrounded by granulomas
- Microscopic capsular breaks
- Trabecular meshwork
- Packed with inflammatory cells and fibrin
- Granulomatous infiltration in TM beams
- Iris and ciliary body
- Severe granulomatous iridocyclitis
- Possible synechiae from chronic inflammation
- Cornea
- Keratic precipitates ("mutton-fat") on the endothelium [32]
This subtype is the most histologically intense, displaying classic autoimmune granulomas directed against lens antigens. Unlike phacolytic glaucoma, which shows a chronic inflammatory reaction with macrophages engulfing lens proteins, phacoanaphylactic glaucoma has a granulomatous reaction zone with giant cells, PMNs, epithelioid cells, and a cuff of lymphocytes and plasma cells.[34][35]
Histopathology of Phacomorphic Glaucoma
Phacomorphic glaucoma arises primarily from mechanical angle closure secondary to a swollen lens, and histopathological changes reflect structural crowding rather than biochemical inflammation.
Key microscopic features
- Lens
- Enlarged, intumescent cortex with liquefaction of superficial fibers
- Intact lens capsule
- Iris
- Anterior bowing due to pupillary block
- Possible focal ischemia from prolonged contact with the lens
- Trabecular meshwork
- Appositional closure with minimal inflammatory cell infiltration
- Secondary formation of peripheral anterior synechiae in chronic cases
- Anterior chamber angle
- Narrow or closed, but devoid of proteinaceous debris
- Cornea
- Endothelial edema due to an acute IOP rise
- Descemet folds [8]
Phacomorphic glaucoma is mechanical and non-inflammatory, and histology primarily reflects changes in iris–lens configuration and anterior chamber angle anatomy, rather than TM obstruction by cells or proteins.
Histopathology of Pupillary Block Glaucoma (Subluxation/Dislocation)
In pupillary block glaucoma (historically termed phacotopic glaucoma), lens displacement causes mechanical obstruction and may damage the trabecular meshwork (see Table 6).
Key microscopic features
- Zonules
- Zonular weakening or rupture
- Pseudoexfoliative deposits (if PXF is present)
- Lens
- Anterior displacement (with angle/pupillary block) or posterior displacement
- Typically intact lens capsule, unless disrupted by trauma
- Trabecular meshwork
- Pigment dispersion, particularly in traumatic lens dislocation
- Possible focal indentation or compression if the lens contacts the angle
- Local collapse or mechanical distortion
- Iris
- Irregular pupil, stretched iris root
- Angle recession in traumatic cases
- Cornea
- Possible endothelial cell loss due to lens–endothelium contact [36]
This subtype is characterized by zonular pathology and mechanical angle changes, not by protein leakage or an immune reaction.
Common Final Histopathologic Pathway (All Forms)
Regardless of subtype, the consequences of untreated lens-induced glaucoma include:
- TM damage and collapse
- Optic nerve head cupping (loss of ganglion cells, lamina cribrosa thinning)
- Retinal nerve fiber layer loss
- Corneal endothelial decompensation
These complications are the result of chronic IOP elevation leading to irreversible glaucomatous optic neuropathy.[37]
Table 6. Histopathologic Fingerprints of Lens-Induced Glaucoma Subtypes
|
Subtype |
Histopathologic Hallmark |
|
Phacolytic |
Protein-laden macrophages clogging the trabecular meshwork, liquefied hypermature cortex |
|
Lens Particle |
Retained lens fragments + inflammatory trabeculitis |
|
Phacoanaphylactic |
Granulomatous giant-cell reaction to lens proteins |
|
Phacomorphic |
Mechanical angle closure by intumescent lens; intact capsule, minimal inflammation |
|
Pupillary Block (Phacotopic) |
Zonular loss, lens displacement, and mechanical trabecular meshwork distortion |
Toxicokinetics
Lens-induced glaucoma is not caused by external toxic substances; rather, the pathogenesis of lens protein–related subtypes closely parallels the principles of ocular toxicokinetics, in which lens-derived proteins, inflammatory mediators, macrophages, and particulate debris function as endogenous “toxins” within the confined ocular environment. Toxicokinetics in lens-induced glaucoma describes how these biologically active materials are released and distributed, how they accumulate and interact with ocular tissues, and how they are ultimately cleared, and how their kinetic behavior contributes to trabecular outflow failure and IOP elevation.
Source of the Endogenous “Toxic Load”
Different subtypes of lens-induced glaucoma introduce unique substances into the aqueous humor.
High-molecular-weight lens proteins (phacolytic glaucoma)
- Derived from a hypermature, liquified cortex
- Include crystallins, degraded peptides, and osmotic proteins
- Leak through microscopic capsular defects
- Overwhelm normal aqueous clearance capacity [3]
Lens cortex/nuclear fragments (lens particle glaucoma)
- Released after capsular rupture due to trauma or surgery
- Act as solid particulate toxins obstructing TM pores [2]
Immunogenic lens proteins (phacoanaphylactic glaucoma)
- Delayed autoimmune granulomatous inflammation triggered by exposed crystallins
- TM damage caused by inflammatory cytokines behaving as biochemical toxins [8]
Mechanical lens mass (phacomorphic and pupillary block [phacotopic] glaucomas)
- Aqueous kinetics altered by mechanical compression, not biochemical release
Absorption and Entry Into Ocular Tissues
The anterior chamber acts as a closed kinetic compartment.
Phacolytic lens proteins
- Enter the aqueous via capsular micro-channels
- Rapidly diffuse through aqueous but poorly traverse the TM due to size
- Protein concentration increases because production > clearance [5]
Lens particles
- Direct retention within the angle
- Become coated with inflammatory cells → greater obstruction
Immunogenic proteins
- Trigger the recruitment of macrophages, T cells, and giant cells
- Widespread diffusion of cytokines (interleukin-1, tumor necrosis factor-alpha, interferon-gamma) in the anterior chamber
Distribution and Accumulation (Key Toxicokinetic Step)
Because the eye has minimal fluid turnover, any foreign proteins or debris accumulate rapidly.[9]
Accumulation in the trabecular meshwork
- TM is the primary site of toxic deposition.
- Macrophage–protein aggregates physically block TM pores.
- Cytokines induce TM edema, reducing outflow facility.
- Particles become lodged in juxtacanalicular tissue.
Accumulation in the anterior chamber
- Protein concentration increases, resulting in a Tyndall (aqueous) flare.
- Lens particles remain suspended until phagocytosed.[38]
Macrophage dynamics
- Macrophages ingest lens proteins and rapidly become ballooned, immobile cells.
- These swollen macrophages cannot exit via the TM, worsening obstruction.
Metabolism, Breakdown, and Biochemical Reactions
The breakdown of lens-derived materials follows unique ocular kinetics.
Lens proteins
- Poorly degraded in aqueous humor due to a lack of proteolytic enzymes
- Persist for long durations, prolonging toxic exposure
- Degraded fragments remain highly osmotic → draw more fluid → inflammatory amplification [39]
Lens particles
- Undergo slow enzymatic degradation by macrophages
- Incomplete breakdown leads to chronic TM loading
Immunogenic proteins
- Trigger granulomatous reactions → cytokines → further TM dysfunction
- Long-term alterations to TM permeability due to persistent inflammation
Clearance and Elimination
Clearance is dramatically impaired in lens-induced glaucoma.
Normal aqueous outflow clearance
- Via TM → Schlemm canal → episcleral veins
- Efficient only for small soluble proteins [3]
Clearance failure in lens-induced glaucoma
- High-molecular-weight proteins cannot pass TM spaces.
- Debris-laden macrophages physically block outflow.
- Granulomatous inflammation reduces trabecular porosity.
- Mechanical angle closure prevents access to outflow pathways.
Thus, the rate of accumulation exceeds the rate of clearance, resulting in an escalating IOP.
Toxicodynamic Effects: How the “Toxic Load” Causes Damage
These biological materials exert toxicodynamic effects on the following ocular tissues (see Table 7).[40]
Trabecular meshwork
- Mechanical obstruction
- Edema from cytokines
- Macrophage infiltration
- Collapse of TM beams
- Reduced outflow capacity
Iris and ciliary body
- Inflammatory hyperemia
- Uveitic infiltrates
- Synechiae formation
Corneal endothelium
- Protein-laden aqueous and high IOP cause endothelial dysfunction.
- Endothelial cell loss leads to persistent corneal edema.
Optic nerve
- Sustained high IOP → ischemia → axonal apoptosis
- Rapid increase in cup–disc ratio in acute lens-induced glaucoma[41]
Table 7. Summary of Toxicokinetic Principles in Lens-Induced Glaucoma
|
Toxicokinetic Step |
Lens-Induced Glaucoma Correlate (Endogenous “Toxin”) |
|
Input/Release |
Lens proteins, particles, and inflammatory cytokines |
|
Absorption |
Entry into the aqueous through capsular defects or through surgical/traumatic openings |
|
Distribution |
Rapid dispersion in the anterior chamber, concentration in the trabecular meshwork |
|
Accumulation |
Trabecular meshworkblockage by debris, macrophages, and granulomas |
|
Metabolism |
Poor degradation → persistent inflammation |
|
Clearance failure |
Outflow pathway obstruction → Intraocular pressure rise |
|
Toxicodynamic Effects |
Trabecular meshwork dysfunction, corneal edema, optic nerve damage |
Clinical Implications of Toxicokinetics in Lens-Induced Glaucoma
- Earlier surgical removal stops protein leakage (“source control”).
- Anti-inflammatory therapy modulates cytokine-mediated toxicodynamics.
- Rapid IOP control protects the corneal endothelium from toxic exposure.
- Delayed clearance leads to chronic TM damage and irreversible vision loss.
History and Physical
In evaluating a patient with suspected lens-induced glaucoma, a detailed history of the onset, duration, and progression of the presenting symptoms is essential. The clinician must note any history of similar episodes or ocular surgery. A clinical history suggestive of a contraindication to systemic steroid use, like osteoporosis, peptic ulcer disease, psychiatric illness, or tuberculosis, should also be elicited. Lens-induced glaucoma typically presents in older individuals with long-standing, untreated cataracts. Presentations vary widely depending on the underlying subtype—phacolytic, lens particle, phacoanaphylactic, phacomorphic, or pupillary block (phacotopic) glaucoma. A careful, detailed history, combined with targeted examination, strongly suggests the diagnosis before imaging or gonioscopy (see Table 8).[3]
History
Presenting concerns
Patients commonly report:
- Sudden or subacute onset of severe unilateral eye pain
- Redness of the eye
- Rapid decline in vision
- Halos around lights
- Headache (often severe, frontal or hemicranial)
- Nausea and vomiting (due to acute IOP rise)
- Photophobia and tearing
Some forms (phacolytic, lens particle glaucoma) may present more subacutely with gradual visual decline and mild pain.[2]
Symptom timeline
- Phacolytic glaucoma: Subacute onset over days to weeks due to hypermature cataract leakage
- Lens particle glaucoma: Symptom onset either postoperative (after cataract surgery) or after ocular trauma; typically within hours to days
- Phacoanaphylactic glaucoma: Develops 1 to 14 days after lens capsule rupture or cataract surgery
- Phacomorphic glaucoma: Acute onset over hours to days; often follows periods of glare or sudden pupillary dilation (dim light, stress, sleep)
- Pupillary block (phacotopic) glaucoma: Intermittent episodes of blurred vision or pain due to shifting lens position (subluxation/dislocation)[42]
Relevant past history
- Ocular history
- Long-standing poor vision from cataract
- History of trauma
- Previous intraocular surgery (phacoemulsification, extracapsular, or intracapsular cataract extraction)
- Retained lens fragments after surgery
- Recurrent episodes of blurry vision or monocular diplopia (lens subluxation)
- Previous episodes of angle closure [21]
- Systemic history
- Diabetes mellitus
- Connective tissue disorders (Marfan, homocystinuria, Weill-Marchesani syndrome)
- PXF
- Steroid use (earlier cataract maturation) [43]
- Delayed access to care
- Fear of surgery
- Socioeconomic constraints
- Rural residence or lack of ophthalmic services [3]
Table 8. Specific History by Subtype
|
Subtype |
History Clues |
|
Phacolytic |
Long-standing hypermature cataract, gradual onset of pain, sensation of cloudy or milky vision due to turbid aqueous, “white reflex” in the cataract |
|
Lens Particle |
Recent cataract surgery, trauma, Nd:YAG capsulotomy; sudden vision loss with pain |
|
Phacoanaphylactic |
History of surgery/trauma 1 to 2 weeks earlier; severe photophobia; autoimmune tendency |
|
Phacomorphic |
Sudden painful vision loss in an eye with a known mature cataract; symptoms worsen in dim light |
|
Pupillary Block (Phacotopic) |
History of trauma, pseudoexfoliation, or systemic connective tissue disorder; intermittent blurry vision when changing posture; prior history of a visibly tremulous lens |
Physical Examination
General inspection
- Signs of patient distress, including nausea or photophobia
- Marked conjunctival congestion and chemosis, especially ciliary flush
- Dilated episcleral vessels
- Eyelid erythema or edema [2]
- Facial asymmetry or abnormal head posture, suggesting associated neurologic or ocular motility abnormalities
- Abnormal binocular alignment, including sensory exotropia in eyes with advanced cataract and poor vision
- Longstanding comitant strabismus since childhood suggests poor visual prognosis in unilateral ectopia lentis (EL) cases
Visual acuity
- Best-corrected visual acuity measured with Snellen or LogMAR chart, with attention to any improvement with the pinhole
- Typically markedly reduced due to cataract and corneal edema
- Ranging from counting fingers to hand motion, depending on corneal clarity and cataract severity
- Cycloplegic refraction performed for EL
Slit-lamp examination
- Cornea
- Stromal edema, subepithelial bullae, and Descemet membrane folds (due to high IOP)
- Microcystic epithelial edema [44]
- Fresh keratitic precipitates (KPs) on the posterior surface of the cornea in PLG and PAG
- Lens proteins are deposited on the posterior surface in LPIG
- Anterior chamber
- Phacolytic
- Lens particle
- Visible lens fragments in AC
- Cells, flare, fibrin
- Phacoanaphylactic
- Severe granulomatous uveitis
- "Mutton-fat" keratic precipitates
- Prominent flare, often intense with fibrin
- Phacomorphic
- Very shallow AC centrally and peripherally
- Intumescent lens
- Pupillary block (phacotopic)
- Lens subluxation or dislocation
- Irregular depth of AC [47]
- Iris
- Anterior bowing of the iris in PMG and PBG
- Posterior synechiae and peripheral anterior synechiae in chronic inflammatory cases (PLG and PAG)
- Rare inflammatory pseudohypopyon in PAG
- Pupil
- Mid-dilated, sluggish pupil in PMG and PBG
- Vertically oval pupils in cases of prolonged IOP elevation due to ischemia of the sphincter pupillae
- Irregular or festooned pupil in chronic inflammatory states (PLG and PAG)
- Poor direct light response in affected eye due to high IOP
- Preserved consensual light reflex in the contralateral eye suggests excellent visual prognosis
- Lens
- Phacolytic
- Mature or hypermature senile cataract
- Morgagnian appearance (liquefied cortex with nucleus sinking)
- Lens particle
- Ruptured lens capsule with a cataractous lens
- Phacoanaphylactic
- Ruptured lens capsule or an anterior capsulorhexis with residual lens matter
- Phacomorphic
- Intumescent mature senile cataract
- Pupillary block (phacotopic)
- Evidence of subluxation/dislocation:
- Phacodonesis
- Iridodonesis
- Visible zonular dialysis
- PBG due to EL: Anteriorly positioned lens
- Evidence of subluxation/dislocation:
- Phacolytic
Intraocular pressure
- Gold standard: Goldmann applanation tonometry
- Markedly elevated in all types (often 40–60 mm Hg) [8]
- Tonometer possibly unreliable in very edematous corneas; rebound tonometry preferred [48]
- iCare rebound tonometry
- Tonopen
Gonioscopy
Angle evaluation with gonioscopy is a mandatory diagnostic step in cases with a clear cornea. Dynamic indentation gonioscopy helps differentiate appositional versus synechial closure. Guideline alignment: American Academy of Ophthalmology Preferred Practice Pattern for Primary Angle Closure 2021 and All India Ophthalmological Society/Glaucoma Society of India 2023
Findings vary by subtype:
- Phacolytic
- Open angles with proteinaceous debris
- TM filled with protein-laden macrophages (visible as fluffy material) [49]
- Synechial angle closure and PAS formation in chronic cases
- Lens particle
- Open angles with particulate debris obstructing the TM
- Phacoanaphylactic
- Angular hyperemia with inflammatory cells and fibrin
- Phacomorphic
- Closed or occludable angle in the involved eye, with iris bombe and appositional closure
- PAS in chronic cases
- Pupillary block (phacotopic)
- Angle narrowing or distortion, depending on lens position
- Possible angle recession in trauma [50]
- An occludable angle in the contralateral eye is highly suggestive of a PBG mechanism
- EL: "Volcano configuration" of the iris, with the pupil forming the central crater
Posterior segment examination
Visualization of the posterior segment is often limited due to corneal edema and dense cataract, making B-scan ultrasonography essential to exclude retinal detachment or vitreous pathology (see Table 9).
Optic nerve examination
- Glaucomatous cupping if IOP elevation has persisted for an extended time
- Acute cases may demonstrate a normal-appearing optic nerve head [51]
Table 9. Summary of History and Physical Findings
|
Subtype |
History |
Key Physical Findings |
|
Phacolytic |
Long-standing hypermature cataract |
Deep AC, protein flare, mobile macrophages |
|
Lens Particle |
Hours–days post-surgery/trauma |
Lens fragments in AC, inflammatory cells |
|
Phacoanaphylactic |
Days–weeks post-surgery/trauma |
Granulomatous uveitis, fibrin, KPs |
|
Phacomorphic |
Acute pain, known cataract | Shallow AC, swollen lens, closed angle |
|
Pupillary Block (Phacotopic) |
Trauma, PXF, systemic CTDs |
Lens displacement, iris/chamber asymmetry |
AC, anterior chamber; CTDs, connective tissue diseases; KP, keratic precipitates; PXF, pseudoexfoliation
Evaluation
Evaluating lens-induced glaucoma centers on the rapid identification of elevated intraocular pressure, assessment of cataract maturity, determination of angle status, and exclusion of alternative causes of secondary glaucoma. Because lens-induced glaucoma can lead to irreversible optic nerve damage within hours to days, a systematic, guideline-driven diagnostic approach is essential.
Clinical Examination (Primary Evaluation Tool)
International guidelines (AAO 2020; ICO Glaucoma Guidelines 2021; AIOS Preferred Practice Patterns 2023) emphasize clinical examination as first-line, consisting of:
- General inspection for patient affect/distress, external ocular signs, gross neurologic symmetry, head posture, and binocular alignment
- Visual acuity with the Snellen or Logarithm of the Minimum Angle of Resolution chart
- Slit lamp biomicroscopy to examine the cornea, AC, iris, and lens [4]
- Lens evaluation using direct illumination, optical sectioning, and retroillumination to assess lens position, integrity, and cataract morphology
- Goldmann applantation tonometry to measure IOP
- If the cornea is significantly edematous:
- iCare rebound tonometry
- Tonopen [8]
- If the cornea is significantly edematous:
- Gonioscopy (gold standard for angle evaluation)
- May include dynamic indentation gonioscopy to differentiate between appositional and synechial closure
- Posterior segment visualization, including fundus examination of the optic nerve head and an assessment for concurrent retinal pathology
- B-scan ultrasonography when the posterior segment view is obscured [5]
B-Scan Ultrasonography (Essential When Media Is Opaque)
The following are supported by the AAO and the ICO Cataract Guidelines (see Table 10).
Indications:
- Dense cataract obscuring the fundus
- Corneal edema blocking reflexes
- Suspected posterior lens dislocation
- Screening for retinal detachment or vitreous hemorrhage [52]
Findings:
- Lens position (subluxated/dislocated)
- Liquefaction in hypermature cataracts
- Intact or ruptured posterior capsule
- Status of vitreous and retina [6]
Anterior Segment Optical Coherence Tomography or Ultrasound Biomicroscopy
Recommended by AIOS 2023 and ICO Comprehensive Ophthalmology Guidelines for complex anterior segment evaluation when available.
Anterior Segment Optical Coherence Tomography
Useful for:
- Measuring anterior chamber depth and angle opening distance
- Assessing angle narrowing and lens vault in PMG
- Demonstrating reduced anterior chamber depth, increased lens vault, and short axial length associated with PMG [53]
- Identifying capsular integrity and lamellar separation in PMG and PLG [54]
- Detecting pseudoexfoliative deposits [39]
Ultrasound Biomicroscopy
More useful for:
- Detecting zonular weakness
- Identifying lens subluxation/dislocation
- Evaluating anterior hyaloid face configuration
- Assessing iris–lens channel obstruction [55]
Laboratory Tests (Situational, Not Routine)
Although routine laboratory tests are not required for diagnosis, some studies may be indicated under specific clinical circumstances.
Erythrocyte sedimentation rate and C-reactive protein
- Considered in cases with severe granulomatous inflammation, as in PAG
Aqueous paracentesis (rare)
- Reserved for cases in which infectious endophthalmitis cannot be confidently excluded, particularly in the postoperative setting
- Acqueous humor cytology may be performed in select cases of uveitis of unknown etiology to help differentiate PLG or PAG from infectious causes
Complete blood count
- Used to evaluate systemic inflammatory states
HbA1c and glucose
- Diabetes accelerates cataract maturation and may influence surgical planning [56]
Diagnostic Red Flags (Require Immediate Attention)
- IOP >40 mm Hg with corneal edema
- Anterior chamber flare with milky fluid
- Sudden painful loss of vision in an older adult with cataract
- Recent cataract surgery with rising IOP
- Suspected lens dislocation in trauma
These require urgent intervention within hours to prevent optic nerve ischemia.[57]
Table 10. Imaging and Evaluation Based on Subtype
|
Subtype |
Key Evaluation Tests |
|
Phacolytic |
Flare + floating proteins on slit lamp; deep AC; B-scan for fundus evaluation |
|
Lens Particle |
Slit-lamp identification of cortical/nuclear fragments; gonioscopy; post-op slit-lamp check |
|
Phacoanaphylactic |
Slit-lamp showing granulomatous uveitis, KPs; UBM for capsular rupture |
|
Phacomorphic |
AC depth (slit lamp, AS-OCT), gonioscopy, IOP |
|
Pupillary Block (Phacotopic) |
UBM for zonules & lens position; B-scan if posterior segment involvement suspected |
AC, anterior chamber; AS-OCT, anterior segment optical coherence tomography; IOP, intraocular pressure; UBM, ultrasound biomicroscopy
Additional Diagnostic Maneuvers
- Digital IOP assessment
- Bedside estimation in emergency settings when tonometry is unavailable
- Light-induced pupillary dynamics
- Used to differentiate pupillary block variants versus open-angle variants [58]
- Evaluation for PXF
- Important in pupillary block (phacotopic) glaucoma: Sampaolesi line, dandruff-like deposits on the lens capsule, zonular laxity
National and International Guidelines Referenced
American Academy of Ophthalmology (AAO)
- PPP: Primary Angle Closure Disease (2021)
- PPP: Cataract in the Adult Eye (2022)
- Recommends:
- Immediate IOP measurement
- Gonioscopy
- Early cataract extraction in phacolytic and phacomorphic glaucoma [59]
International Council of Ophthalmology
- Guidelines for Glaucoma Care (2021)
- Mandatory gonioscopy in secondary glaucomas
- Imaging in unclear cases
AIOS/Glaucoma Society of India
- Preferred Practice Pattern for Secondary Glaucomas (2023)
- B-scan is recommended when a cataract obscures the retinal view
- Advocated for early lens removal in all lens-induced glaucoma subtypes
- Ultrasound biomicroscopy recommended for zonular assessment
Treatment / Management
Management of lens-induced glaucoma requires prompt reduction of IOP, control of inflammation, and definitive removal or repositioning of the pathological lens, which is the only curative intervention. Early treatment is essential to prevent permanent optic nerve damage. International guidelines (AAO 2022; ICO Glaucoma Guidelines 2021; AIOS PPP 2023) uniformly emphasize that cataract extraction or removal of lens material is the definitive management for all subtypes of lens-induced glaucoma.
Immediate/Emergent Management
These steps should begin as soon as lens-induced glaucoma is suspected, particularly when IOP exceeds 35 to 40 mm Hg.
Medical therapy
- Topical aqueous suppressants
- Beta blockers (timolol 0.5%)
- Carbonic anhydrase inhibitors (dorzolamide/brinzolamide)
- Alpha-agonists (brimonidine) [3]
- Systemic IOP-lowering medications
- Intravenous mannitol, 1 to 2 /kg over 30 to 45 minutes
- Both AIOS and AAO recommend administering mannitol preoperatively when the cornea is edematous.
- Oral acetazolamide 250 to 500 mg, unless contraindicated (eg, topical carbonic anhydrase inhibitor already in use)
- Must be paired with vigilant monitoring of kidney function and serum electrolytes
- Corticosteroids
- Topical corticosteroids
- Prednisolone acetate 1% 4 to 6 times/day
- Reduces anterior segment inflammation, macrophage activity, and TM edema (especially in phacolytic and lens particle glaucoma)
- Systemic corticosteroids (select cases)
- Used in severe inflammatory presentations, especially phacoanaphylactic and advanced phacolytic glaucoma
- Help control inflammation prior to definitive cataract extraction
- Cycloplegics
- Atropine 1% or homatropine 2%
- Deepens the anterior chamber and relieves ciliary spasm
- Useful in phacomorphic and phacoanaphylactic glaucoma
- Avoid prostaglandin analogues
- International guidelines advise against the use of prostaglandin analogues in the acute setting due to the risk of worsening inflammation.[3]
Laser interventions (selective use)
Laser procedures do NOT cure lens-induced glaucoma and are insufficient for IOP control, but they may provide short-term relief in select cases.
- Nd: YAG peripheral iridotomy
- Useful only in:
- Phacomorphic glaucoma (relative pupillary block)
- Pupillary block glaucoma (phacotopic)
- Not useful in:
- Phacolytic glaucoma
- Lens particle glaucoma
- Phacoanaphylactic glaucoma [6]
- Useful only in:
- Laser iridoplasty
- Can reduce iris bombe when the cornea is too hazy for Nd:YAG peripheral iridotomy
- Laser capsulotomy
- Contraindicated in phacolytic or phacoanaphylactic glaucoma
- May worsen protein leakage and inflammation [8]
(B2)
Definitive Management: Surgical Treatment
According to AAO, AIOS, and ICO guidelines, lens removal as early as safely possible is the definitive treatment for all subtypes of lens-induced glaucoma. Surgery should be undertaken after adequate IOP control and corneal clearing, ideally within 24 to 48 hours, once visualization permits.[5] Pars plana vitrectomy may be required preoperatively when the AC depth is insufficient to safely proceed with cataract extraction in mature or hypermature intumescent cataracts.[60]
General surgical principles
- Cataract extraction may be performed using phacoemulsification, manual small-incision cataract surgery, or extracapsular cataract extraction, depending on cataract morphology, zonular integrity, and surgeon expertise.
- Complete removal of lenticular material is essential to prevent persistent inflammation or postoperative IOP elevation.
- Cataract surgery may be performed for pain and inflammation control even in eyes with no light perception, when visual recovery is unlikely.
Intraoperative IOP and tissue protection
- Maintain low phaco power and low bottle height
- Use dispersive viscoelastic to protect the corneal endothelium
- Avoid prolonged phaco time to limit inflammation
- Ensure meticulous removal of cortical material [2] (B2)
Subtype-specific surgical management
- Phacolytic glaucoma
- Preferred procedures
- Manual small incision cataract surgery (MSICS) or phacoemulsification, once IOP is controlled [61]
- Key principles
- Remove the hypermature lens (source of protein leakage)
- Perform thorough cortical cleanup
- Exercise caution due to fa ragile, thinned capsule
- Peripheral iridotomy not required (angle is typically open)
- Preferred procedures
- Lens particle glaucoma
- Preferred procedures
- Complete removal of residual lenticular material, which responds well to total lens aspiration
- Techniques
- Anterior chamber washout
- Irrigation/aspiration of retained cortex
- Pars plana vitrectomy for nuclear or posterior lens fragments[3]
- Guideline note
- AAO recommends not delaying the removal of retained nuclear fragments >2 mm
- Preferred procedures
- Phacoanaphylactic glaucoma
- Preferred procedures
- Removal of inciting lens material
- Debridement of granulomatous tissue when present
- Medical adjuncts
- Intensive topical corticosteroids
- Systemic corticosteroids (prednisolone 0.5–1 mg/kg) to suppress immune-mediated inflammation prior to surgery
- Supported by AAO and ICO (see Table 11).[3]
- Preferred procedures
- Phacomorphic glaucoma
- Preferred procedures
- MSICS: favored in resource-limited settings and for markedly swollen lenses
- Phacoemulsification: appropriate in experienced hands with adequate corneal clarity
- Surgical goals
- Remove the intumescent lens
- Relieve pupillary block and mechanically reopen the angle
- Prevent synechial angle closure [62]
- Intraoperative considerations
- Trypan blue for poor red reflex
- Controlled capsulorhexis
- Low-flow phaco settings
- Viscoelastic tamponade to deepen the AC
- Postoperative IOP
- Manage transient spikes with topical aqueous suppressants
- Preferred procedures
- Pupillary block (phacotopic) glaucoma (lens subluxation/dislocation)
- Surgical approach depends on the degree and direction of lens displacement
- Mild to moderate subluxation
- Phacoemulsification with capsular tension rings or sutured capsular segments
- Severe subluxation or anterior dislocation
- MSICS or intracapsular cataract extraction
- Posterior dislocation
- Pars plana lensectomy with vitrectomy
- Mild to moderate subluxation
- Intraocular lens (IOL) considerations
- Scleral-fixated IOL
- Iris-claw IOL
- Anterior chamber IOL, depending on residual support
(B3) - Surgical approach depends on the degree and direction of lens displacement
Special Intraoperative Challenges
- Ruptured anterior capsule
- Perform a continuous capsulorhexis incorporating central capsular tears.
- Avoid tension at peripheral tears to prevent extension to the equator or posterior capsule.
- Gentle aspiration is critical to avoid zonular stress.[32]
- Corneal edema
- Use hypertonic saline (NaCl 5%).
- Consider glycerol application intraoperatively.
- Preoperative mannitol improves corneal clarity.
- Small pupil
- Stretch pupilloplasty
- Iris hooks
- Malyugin ring
- Poor zonular support (PXF, trauma)
- Capsular tension ring
- Scleral fixation techniques [3]
(B3)
Table 11. Timing Recommendations (Guideline-Based)
|
Guideline |
Recommendation |
|
AAO (2022) |
Early lens removal is essential, ideally within 24 to 2 hours after medical stabilization. |
|
ICO (2021) |
Immediate IOP control should be followed by definitive lens extraction; delaying increases the risk of optic neuropathy. |
|
AIOS PPP (2023) |
Surgery should not be postponed beyond 48 hours once IOP is adequately controlled. |
AAO, American Academy of Ophthalmology; AIOS PPP, All India Ophthalmological Society Preferred Practice Pattern; ICO, International Council of Ophthalmology; IOP, intraocular pressure
Postoperative Management
Medications
- Topical steroids, tapered gradually (initially 6–8 times/day)
- Cycloplegics for comfort and prevention of posterior synechiae
- Topical aqueous suppressants, as needed
- Lubricants for corneal epithelial recovery
Monitoring
- IOP assessment on postoperative day 1, at 1 week, and at 1 month
- Gonioscopy at 2 to 4 weeks to assess for PAS
- Optic nerve evaluation once the corneal clarity permits
Complications to monitor
- Persistent intraocular inflammation
- Postoperative IOP spikes
- Cystoid macular edema
- Corneal endothelial decompensation
- Posterior capsular rupture or retained lens material [63]
Long-Term Considerations
Definitive surgical management addresses the inciting lens pathology; however, postoperative care and long-term rehabilitation are critical for achieving sustained intraocular pressure control, visual recovery, and prevention of secondary glaucoma (see Table 12). Please refer to the Postoperative and Rehabilitation Care section for more information on postoperative management strategies, visual rehabilitation, and long-term surveillance.
Table 12. Summary of Management by Subtype
|
Subtype |
Initial Management |
Definitive Management |
|
Phacolytic |
Steroids + IOP control |
Lens extraction |
|
Lens Particle |
Steroids + aqueous suppressants |
Removal of fragments, pars plana vitrectomy |
|
Phacoanaphylactic |
Intensive steroids |
Removal of antigenic lens material |
|
Phacomorphic |
IOP lowering + cycloplegia | Early cataract extraction |
|
Phacotopic |
IOP contvrol |
Lens reposition/removal |
IOP, intraocular pressure
Differential Diagnosis
Lens-induced glaucoma must be differentiated from other causes of acute ocular pain, inflammation, and elevated IOP. Accurate diagnosis relies on careful history, slit-lamp examination, gonioscopy, and adjunctive imaging such as B-scan ultrasonography when posterior segment visualization is limited (see Table 13, which shows key conditions that may mimic lens-induced glaucoma, with distinguishing clinical and examination features that aid in accurate diagnosis).
Key distinctions center on:
- Lens status (size, position, integrity)
- Angle configuration (open vs closed; appositional vs synechial)
- Degree and nature of inflammation
- Temporal relationship to surgery or trauma
Common Diagnostic Pitfalls
- Infectious endophthalmitis can resemble PAG or PLG glaucoma but is suggested by purulent hypopyon, vitritis, and rapid clinical deterioration.[6]
- Acute anterior uveitis typically presents with normal or low IOP; however, viral uveitis may cause IOP elevation and should be considered when inflammation is disproportionate to lens findings.[4][8]
- Primary acute angle-closure glaucoma may mimic PMG but is distinguished by a clear lens, absence of lens intumescence, and a shallow AC in the contralateral eye.[3]
- Malignant (ciliary block) glaucoma may be confused with PBG mechanisms but unlike PBG, it does not respond to laser peripheral iridotomy and demonstrates posterior aqueous misdirection on ultrasound biomicroscopy.[7]
- Suprachoroidal hemorrhage or effusion should be suspected in cases of flat AC with severe pain, particularly after surgery or trauma; B-scan ultrasonography is diagnostic.[5]
Table 13. Conditions Mimicking Lens-Induced Glaucoma
|
Condition |
Why Mimics Lens-Induced Glaucoma |
Key Distinguishing Features (Helps Rule Out) |
|
Infectious Endophthalmitis, Including Posttraumatic Cases (vs Phacolytic Glaucoma) |
Painful red eye, corneal edema, AC inflammatory material | Purulent hypopyon, severe vitritis, rapid deterioration, recent surgery or injection; B-scan shows dense vitreous echoes |
|
Uveitic Glaucoma (Acute Anterior Uveitis), including Fuchs Heterochromic Iridocyclitis (vs Phacolytic Glaucoma) |
Pain, redness, flare, possible IOP elevation | Typically normal or mildly elevated IOP; cells often exceed flare; no hypermature lens or milky AC |
|
Postoperative Uveitis (vs Lens Particle Glaucoma) |
Inflammation and IOP rise after cataract surgery | No visible lens fragments; inflammation predominates over particulate debris; IOP elevation usually less extreme |
|
Retained Viscoelastic–Induced IOP Rise (vs Lens Particle Glaucoma) |
Acute postoperative IOP spike | Occurs early (POD 0–1); no lens fragments; resolves with aspiration and topical therapy |
|
Granulomatous Uveitis (Sarcoidosis, TB) (vs Phacoanaphylactic Glaucoma) |
Granulomatous inflammation with elevated IOP | No history of lens rupture or surgery; systemic features present; inflammation not centered on lens proteins |
|
Primary Acute Angle-Closure Glaucoma (vs Phacomorphic Glaucoma) |
Acute painful red eye with high IOP and corneal edema | Clear lens without intumescence; shallow AC in fellow eye; no lens swelling or hypermaturity |
|
Plateau Iris Syndrome (vs Phacomorphic Glaucoma) |
Angle closure | Deep central AC, “double-hump” sign on gonioscopy, normal-sized lens, younger age |
|
Malignant Glaucoma (Ciliary Block/Aqueous Misdirection) (vs Phacomorphic or Pupillary Block/Phacotopic Glaucoma) |
Shallow AC with high IOP | Patent PI without IOP relief; posterior aqueous misdirection on UBM; normal lens size; often occurs after intraocular surgery |
|
Traumatic Hyphema with Angle Closure (vs Pupillary Block/Phacotopic Glaucoma) |
Sudden IOP rise after trauma | Visible hyphema or clot; lens not displaced; angle obstruction due to blood |
|
Pseudoexfoliation Glaucoma |
Elevated IOP with lens/zonular abnormalities |
Dandruff-like PXF deposits on lens and angle; chronic course; no lens hypermaturity or milky AC |
|
Suprachoroidal Hemorrhage/Effusion |
Flat AC with sudden pain and IOP elevation |
B-scan shows suprachoroidal blood or fluid; posterior segment pathology; normal lens |
|
Neovascular Glaucoma |
High IOP with corneal edema and pain |
Rubeosis iridis, fibrovascular angle membranes, retinal ischemia (eg, diabetes, CRVO), normal lens morphology |
|
Secondary Angle Closure from Posterior Uveitis or Scleritis |
Painful red eye with elevated IOP |
Severe deep scleral pain, thickened choroid, posterior segment inflammation on imaging; normal lens morphology |
AC, anterior chamber; CRVO, central retinal vein occlusion; IOP, intraocular pressure; POD, postoperative day; PXF, pseudoexfoliation; TB, tuberculosis; UBM, ultrasound biomicroscopy
Pertinent Studies and Ongoing Trials
Lens-induced glaucoma has been extensively studied in large observational cohorts, hospital-based prospective studies, and population-based cataract surveys. Although randomized controlled trials are limited given the ethical impossibility of withholding timely cataract surgery, the available evidence strongly supports early IOP reduction and definitive lens extraction as the optimal management strategy across all subtypes (see Table 12). Below is a synthesis of the most influential evidence.
Evidence Supporting Early Cataract Extraction (Definitive Treatment)
- The Aravind Eye Hospital Prospective Lens-Induced Glaucoma Study (India, n= 1200)
- One of the most extensive datasets on lens-induced glaucoma
- Outcome:
- Early cataract extraction (within 48 hours) resulted in:
- 94% IOP normalization
- Significant reduction in corneal edema within 72 hours
- Better postoperative best corrected visual acuitycompared to delayed surgery
- Early cataract extraction (within 48 hours) resulted in:
- Conclusion: Early surgery prevents irreversible damage to the angle and the optic nerve.[64]
- AIIMS New Delhi Lens-Induced Glaucoma Cohort (n= 450)
- Compared medical-only stabilization versus immediate surgery
- Outcome:
- Medical therapy alone was insufficient; IOP rebounded in 78%.
- Surgery within 24 to 48 hours improved outcomes and reduced the incidence of peripheral anterior synechiae.
- Conclusion: Surgery is mandatory, not optional.[3]
- Nepal Blindness and Cataract Study (World Health Organization-supported)
- Emphasized the high prevalence of phacolytic and phacomorphic glaucoma in rural populations.
- Outcome:
- MSICS demonstrated excellent results in the treatment of swollen cataracts.
- Phacoemulsification is recommended only for experienced surgeons due to capsular fragility.[65]
Evidence Supporting Medical Stabilization Before Surgery
- Mannitol Use Studies (AIOS–Glaucoma Society of India)
- Increased corneal clarity and AC depth with preoperative intravenous mannitol
- Enabled safer capsulorhexis
- Outcome: Lowered intraoperative complication rates [66]
- Topical Steroid Efficacy Trials (Phacolytic and Lens Particle–Induced Glaucoma)
- Prednisolone acetate reduced:
- Protein load
- Macrophage migration
- Anterior chamber flare
- Outcome: Improved surgical visibility and lower postoperative inflammation [67]
- Prednisolone acetate reduced:
Studies on Lens Particle Glaucoma
- Post-Phaco Retained Lens Matter Analysis (UCLA–Bascom Palmer)
- Lens fragments >2 mm significantly increased the risk of postoperative IOP spikes.
- Recommendation: Early removal (washout or pars plana vitrectomy) improves outcomes.[68]
- Indian Postoperative Lens-Induced Glaucoma Study (n= 320)
- Delayed removal (>7 days) led to:
- Higher chronic IOP
- Increased uveitis
- Higher incidence of secondary glaucoma needing long-term medication [69]
- Delayed removal (>7 days) led to:
Evidence for Management of Phacoanaphylactic Glaucoma
- Immune-Mediated Uveitis Studies
- Demonstrated type III hypersensitivity reaction to lens proteins.
- Outcome:
- Intensive steroids + lens removal resulted in rapid control.
- Steroid therapy alone cannot cure the condition.
Evidence Supporting MSICS versus Phacoemulsification
- Coimbatore MSICS versus Phaco Trial in Lens-Induced Glaucoma
- MSICS is favored for hypermature/white cataracts.
- Outcome:
- Shorter surgical time
- Less endothelial loss
- Easier nucleus delivery
- AAO and AIOS cite MSICS as the preferred technique in lens-induced glaucoma.[70]
- Global Cataract Outcomes Study
- In resource-limited settings:
- MSICS had comparable outcomes to phaco.
- MSICS was associated with lower cost and better safety for swollen lenses
- In resource-limited settings:
Epidemiologic Studies Driving Guidelines
- VISION 2020 India and Nepal Cataract Blindness Surveys
- Identified lens-induced glaucoma as a significant cause of avoidable blindness.
- Outcome, Strategies adopted globally:
- Early detection of mature cataracts
- Community outreach
- Immediate referral pathways [71]
- Nigerian & Ethiopian Glaucoma Registries
- Demonstrated high lens-induced glaucoma burden due to delayed cataract surgery.
- Outcome: Advocacy for early intervention incorporated into ICO policy.
Table 14. Key Clinical Practice Guidelines Influenced by These Studies
|
Guideline Issued By |
Recommendation Based on Evidence |
|
American Academy of Ophthalmology |
Early lens extraction is essential; medical therapy is temporary only |
|
International Council of Ophthalmology |
Gonioscopy + rapid IOP control + surgery within 24 to 72 hrs |
|
All India Ophthalmological Society |
MSICS preferred in phacomorphic/phacolytic eyes; endorsed early surgical management |
|
Glaucoma Society of India |
IV mannitol + topical therapy before surgery improves outcomes |
|
Nepal Ophthalmic Society |
Emphasis on rural cataract screening to prevent lens-induced glaucoma |
IOP, intraocular pressure; IV, intravenous; MSICS, manual small incision cataract surgery
Ongoing Studies and Research Trends
While randomized trials are rare, several prospective observational studies are underway:
- India (Aravind/AIIMS Multi-Centric Lens-Induced Glaucoma Registry Study: Ongoing)
- Aim: Understand long-term optic nerve outcomes after early versus delayed cataract extraction.[72]
- Nepal (Biratnagar Cataract Maturity Study: Ongoing)
- Aim: Predict risk of lens-induced glaucoma based on lens density and nuclear opalescence scores.[73]
- Ethiopia (World Health Organization-AFRO Cataract Barriers Project)
- Aim: To evaluate rural access barriers that contribute to the prevalence of lens-induced glaucoma.[74]
- Glaucoma Society of India: Phacolytic Protein Analysis Project
- Aim: Leverage proteomic analysis of leaked lens proteins to understand macrophage activation pathways.
Treatment Planning
Treatment planning for lens-induced glaucoma requires a stepwise, individualized, and subtype-specific approach that integrates:
- Urgency of IOP reduction
- Subtype of lens-induced glaucoma
- Degree of corneal edema
- Lens morphology (mature, hypermature, intumescent, fragmented, dislocated)
- Presence of inflammation
- Zonular integrity
- Surgeon experience and available technology
- Patient comorbidities and ocular status of the fellow eye [3]
Because definitive therapy is early lens extraction, the treatment plan (see Table 15) must prepare the eye for safe surgery while minimizing optic nerve damage. Planning begins by identifying the mechanism causing aqueous outflow obstruction (trabecular obstruction versus pupillary block).
Table 15. Determination of the Subtype Directs the Treatment Plan
|
Subtype |
Primary Treatment Goal |
|
Phacolytic |
Reduce inflammation and IOP → Remove hypermature lens |
|
Lens Particle Glaucoma |
Remove retained lens fragments (AC/IOL/PPV) |
|
Phacoanaphylactic |
Immunosuppression + removal of antigenic lens matter |
|
Phacomorphic |
Reduce IOP → Deepen AC → Extract swollen lens |
|
Phacotopic Glaucoma |
Control IOP → Reposition or remove dislocated lens |
AC, anterior chamber; IOL, intraocular lens; IOP, intraocular pressure; PPV, pars plana vitrectomy
Phase I: Immediate Stabilization (Preoperative)
Objectives
- Lower IOP rapidly
- Clear cornea sufficiently to allow safe surgery
- Reduce anterior chamber inflammation
- Prevent further TM dysfunction
- Avoid permanent optic nerve injury [2]
Components
- IOP reduction
- Begin with triple topical therapy (beta-blocker, carbonic anhydrase inhibitor, alpha-agonist).
- Add oral acetazolamide if no contraindications.
- Start intravenous mannitol (1–2 g/kg) if IOP >40 mm Hg or the cornea is too hazy for surgery.[5]
- Inflammation Control
- Topical steroids (prednisolone acetate 1%, 6–8 times/day)
- Cycloplegics to stabilize the blood–aqueous barrier
- Avoid prostaglandin analogues
- They exacerbate inflammation and are not included in the planning of acute lens-induced glaucoma.[21]
Phase II: Decide the Type and Timing of Surgery
AAO, AIOS, and ICO guidelines recommend surgery within 24 to 72 hours once IOP is controlled and corneal clarity allows safe entry.
- Phacolytic glaucoma
- Preferred: MSICS or phacoemulsification (expert hands)
- Careful aspiration of liquefied cortex and proteinaceous material
- Avoid sudden decompression to prevent capsular blowout [52]
- Lens particle glaucoma
- Small lens particles: AC washout
- Retained cortex/nucleus: I/A or vitrectomy
- Posterior nuclear fragments: pars plana vitrectomy + phacofragmentation by vitreoretinal surgeon
- Phacoanaphylactic glaucoma
- Topical ± systemic steroids for 24 to 48 hrs
- Surgery once the eye is quiet
- Removal of inciting lens material and inflammatory membranes [7]
- Phacomorphic glaucoma
- Preferred: MSICS or phacoemulsification (expert hands)
- Planning a large capsulorhexis is essential due to the intumescent cortex
- Use trypan blue routinely
- Pupillary block (phacotopic) glaucoma
- Surgery depends on displacement:
- Anterior dislocation: AC extraction/MSICS
- Posterior dislocation: PPV + lensectomy
- Decide IOL plan (anterior chamber intraocular lens, scleral-fixated, iris-claw, or aphakia initially) [5]
Phase III: Perioperative Planning
Key considerations during surgical planning
- Corneal edema
- Use pre-operative mannitol
- Endothelial protection with dispersive ophthalmic viscosurgical device
- Gentle fluidics
- Capsulorhexis planning
- Intumescent/Morgagnian:
- Two-stage continuous curvilinear capsulorhexis or capsular staining
- Controlled decompression after needle puncture [9]
- Intumescent/Morgagnian:
- Zonular weakness
- Suspect in trauma, PXF, hypermature cataract
- Prepare capsular tension ring, Cionni ring, and capsular hooks
- Have scleral fixation instruments available
- Small pupil
- Trypan blue
- Iris hooks or Malyugin ring
- Stretch pupilloplasty [2]
- Intraoperative IOP stability
- Low bottle height
- Minimize turbulence
- Avoid over-deepening the AC
Phase IV: Postoperative Planning
Goals:
- Prevent IOP spikes
- Control inflammation
- Protect cornea
- Prevent synechiae
- Monitor optic nerve recovery [3]
Postoperative medications:
- Topical steroids (6–8 times/day, slow taper over 4–6 weeks)
- Cycloplegics
- Aqueous suppressants for the first 1 to 2 weeks
- Avoid prostaglandin analogues initially
- Antibiotics for infection prophylaxis
Follow-up schedule:
- Day 1: IOP, AC reaction, corneal status
- 1 week: IOP, check for peripheral anterior synechiae (PAS)
- 2 to 4 weeks: Gonioscopy, optic nerve evaluation
- 1 to 3 months: Final intraocular lens position, visual recovery, nerve function [6]
Long-term plan:
- Assess for chronic angle closure (phacomorphic)
- Manage steroid response
- Treat residual glaucoma if present
- Consider laser or surgery if PAS is significant
Patient- and System-Level Planning
Patient education
- Explain urgency and the need for early surgery.
- Emphasize lifelong monitoring given the optic nerve's vulnerability.
- Address cataract neglect (common in rural/older populations).
System-level strategies: AIOS, ICO recommendations
- Prioritize lens-induced glaucoma cases in surgical scheduling.
- Strengthen rural cataract screening.
- Develop expedited referral pathways.
- Use MSICS infrastructure in low-resource settings.
Summary Treatment Planning Algorithm
Step 1: Identify lens-induced glaucoma subtype → Step 2: Lower IOP immediately → Step 3: Control inflammation → Step 4: Plan definitive lens surgery → Step 5: Customize surgical technique to lens morphology and zonules → Step 6: Manage post-op IOP and inflammation → Step 7: Long-term optic nerve follow-up [75]
Toxicity and Adverse Effect Management
Management of lens-induced glaucoma involves aggressive IOP reduction, anti-inflammatory therapy, hyperosmotic agents, and definitive surgical removal of the lens. Each therapeutic intervention carries potential toxicities and adverse effects. Safe and effective care requires understanding these risks and establishing preventive and corrective strategies.
Toxicities Related to Medical Therapy
Hyperosmotic agents (mannitol 20%/glycerol)
- Potential toxicities:
- Acute kidney injury
- Electrolyte imbalance (hyponatremia)
- Pulmonary edema
- Cardiac decompensation in congestive heart failure (CHF)
- Severe dehydration
- Nausea/vomiting
- Headache, altered sensorium (rare) [2]
- Management and prevention:
- Avoid in renal failure or CHF.
- Pre-treat serum electrolytes in high-risk patients.
- Infuse slowly over 30 to 45 minutes.
- Monitor urine output.
- Stop infusion if respiratory distress occurs.[8]
Carbonic anhydrase inhibitors (acetazolamide/dorzolamide/brinzolamide)
- Potential toxicities:
- Metabolic acidosis
- Hypokalemia
- Paresthesias, fatigue
- Gastrointestinal upset
- Kidney stones
- Stevens-Johnson syndrome (rare but serious)
- Contraindicated in sulfa allergy [4]
- Management:
- Provide oral potassium supplementation as needed.
- Avoid in sickle cell disease (risk of induced sickling).
- Monitor electrolytes in prolonged therapy.
Beta-blockers (timolol)
- Potential toxicities:
- Bradycardia
- Bronchospasm
- Hypotension
- Atrioventricular block
- Depression, fatigue
- Masking of hypoglycemia (eg, diabetes mellitus) [5]
- Management:
- Avoid use in asthma/chronic obstructive pulmonary disease and heart block (contraindicated).
- Use betaxolol (β1-selective) as needed in reactive airway disease.
- Monitor pulse and blood pressure.
Alpha-2 agonists (brimonidine)
- Potential toxicities:
- Allergic follicular conjunctivitis
- Dry mouth
- Fatigue, sedation
- Hypotension
- Central nervous system depression in infants (contraindicated <2 years)
- Management:
- Discontinue if allergic conjunctivitis occurs.[76]
- Avoid in children.
Topical steroids (prednisolone/dexamethasone)
- Potential toxicities:
- Steroid-induced ocular hypertension
- Steroid-responsive glaucoma
- Delayed wound healing
- Increased risk of infection
- Cataract progression (not relevant in lens-induced glaucoma)
- Management:
- Check IOP regularly.
- Plan a step-down taper.
- Switch to “soft” steroid (loteprednol) if needed.[77]
Cycloplegics (atropine/homatropine)
- Potential toxicities:
- Angle closure in narrow angles (use cautiously presurgery)
- Dry mouth
- Flushing
- Delirium in older adults (rare)
- Management:
- Use the minimal effective dose.
- Avoid known angle closure unless treating lens-induced glaucoma with block relief.[78]
Toxicities and Adverse Events Related to Surgical Management
Definitive management of lens-induced glaucoma involves cataract extraction (MSICS, phacoemulsification), removal of lens fragments, or lensectomy. Each carries potential intraoperative and postoperative complications.
Intraoperative surgical complications
- Capsular rupture
- Common in hypermature or intumescent lenses
- Leads to vitreous loss or retained lens fragments
- Management:
- Anterior vitrectomy
- Sulcus intraocular lens (IOL) or delayed secondary IOL placement [79]
- Zonular dialysis/dialysis extension
- Especially common in phacotopic glaucoma and pseudoexfoliation
- Management:
- Capsular tension ring or Cionni ring
- Iris hooks for capsular fixation
- Scleral-fixated IOL
- Endothelial toxicity
- Caused by ultrasound energy, prolonged phaco time, or manipulation in swollen lenses
- Management:
- Use dispersive viscoelastic.
- Ensure low-flow, low-energy phaco settings.
- Convert to MSICS if phaco visibility is poor.[80]
- Intraoperative hemorrhage
- Iris bleeding during minor pupil manipulation
- Rare expulsive hemorrhage in high IOP settings
- Management:
- Establish good IOP control preoperatively.
- Maintain gentle iris handling.
Early postoperative complications
- Acute pressure rise (IOP spike)
- Most common in lens-induced glaucoma, especially phacolytic and lens particle glaucoma
- Management:
- Aqueous suppressants
- Burping wound if AC is shallow
- AC washout if retained viscoelastic/lens matter
- Corneal edema
- Due to endothelial stress from high IOP
- Management:
- Hypertonic saline
- Steroids
- IOP control
- Bandage contact lens if epithelial compromise [80]
- Severe inflammation/fibrin membrane
- More common in phacoanaphylactic or lens particle glaucoma
- Management:
- Intensive steroids
- Cycloplegics
- Tissue plasminogen activator if fibrin severe
- Wound leak/hypotony
- Management:
- Bandage contact lens
- Resuturing if needed
- Management:
- Endophthalmitis (rare)
- Management:
- Intravitreal antibiotics (vancomycin + ceftazidime)
- Vitrectomy if indicated
- Management:
Late postoperative complications and toxicity
- Chronic glaucoma/peripheral anterior synechiae
- Particularly after phacomorphic glaucoma
- Occurs if angle closure persists longer than 48 to 72 hours [8]
- Management:
- Long-term IOP-lowering therapy
- Laser iridoplasty or filtering surgery if needed
- Cystoid macular edema
- Especially in hypermature cataracts or high inflammation states [8]
- Management:
- Nonsteroidal anti-inflammatory drugs
- Steroids (topical/periocular)
- Secondary IOL issues
- Dislocation
- Tilt
- Sulcus-IOL–related complications [8]
- Management:
- Reposition or refixate
- Exchange for scleral-fixated IOL if necessary
- Corneal endothelial decompensation
- From surgical trauma or prolonged high IOP [8]
- Management:
- Hypertonics
- Descemet stripping endothelial keratoplasty or descemet membrane endothelial keratoplasty for irreversible cases
General Preventive Strategies (Guideline-Based)
AIOS, AAO, ICO recommendations include:
- Adequate preoperative IOP control to prevent corneal toxicity
- Early surgery (<48–72 hrs) to reduce angle and TM damage
- Use of dispersive ophthalmic viscosurgical device to protect the endothelium
- Avoidance of pre-operative prostaglandins
- Adequate dilatation or mechanical pupil expansion
- Appropriate IOL choice based on zonular status
- Judicious steroid taper to avoid steroid-induced glaucoma [2]
Summary
Toxicity and adverse effect management in lens-induced glaucoma requires:
- Identifying drug-related toxicities early
- Anticipating intraoperative and postoperative complications
- Providing prompt correction and preventive strategies
- Long-term monitoring for optic nerve and corneal consequences
By recognizing toxicities upfront, clinicians can safely navigate the intense inflammatory and anatomical challenges posed by lens-induced glaucoma.[3]
Staging
Lens-induced glaucoma is traditionally classified by mechanism-based subtype, which provides etiologic insight but does not reliably convey clinical severity, necessitating a complementary staging approach. Functional staging helps guide urgency, prognosis, and postoperative expectations. The following staging system integrates the severity of IOP, inflammation, angle compromise, optic nerve head damage, and chronicity—all of which influence surgical planning and visual outcomes (see Table 16).[29]
Functional Severity Staging of Lens-Induced Glaucoma
Stage 0: Pre-glaucomatous/impending lens-induced glaucoma
- IOP: Normal
- Lens: Mature, hypermature, Morgagnian, or intumescent cataract
- Cornea: Clear
- AC reaction: None
- Angle: Open, or shallow AC in eyes at risk for phacomorphic subtype
- Optic nerve: Normal
- Symptoms: Asymptomatic or gradual visual decline from cataract [81]
Implication: High risk of progression; surgery should not be delayed.
Stage 1: Mild/early lens-induced glaucoma
- IOP: 25 to 35 mm Hg
- Lens: Mature or hypermature cataract; early intumescence or capsular leak
- Cornea: Clear or mild stromal edema
- AC reaction: Mild cells and flare; early protein leakage or particulate material
- Angle: Angle configuration varies by mechanism; descriptors below reflect the dominant pattern at this stage.[82]
- Phacolytic → Open, with early protein and macrophage accumulation
- Lens particle → Open, with limited particulate lens debris
- Phacoanaphylactic → Open, with mild inflammatory trabeculitis
- Phacomorphic → Partially narrow, without PAS
- Pupillary block (phacotopic) → Intermittent angle narrowing related to lens subluxation
- Optic nerve: Normal
- Symptoms: Occular pain, haloes, headache, blurred vision [83]
Implication: IOP elevation is rapidly reversible; excellent prognosis with timely surgery.
Stage 2: Moderate lens-induced glaucoma
- IOP: 35 tp 45 mm Hg
- Lens: Hypermature, intumescent, or capsular disruption with protein leakage
- Cornea: Moderate edema with reduced visualization
- AC reaction: Moderate to severe flare; visible proteinaceous material and macrophages
- Angle:
- Phacolytic → Open, with heavy protein and macrophage obstruction of the TM
- Lens particle → Open, with significant particulate debris obstructing trabecular outflow
- Phacoanaphylactic → Open, with active granulomatous trabeculitis
- Phacomorphic → Significant appositional angle closure
- Pupillary block (phacotopic) → Sustained angle narrowing or closure due to lens displacement
- Optic nerve: Early glaucomatous damage; increased cup-to-disc ratio, early retinal nerve fiber layer loss
- Symptoms: Severe pain, photophobia, marked visual reduction
Implication: Urgent IOP control and early lens extraction required (within 24–48 hrs) to prevent irreversible lens damage.[84]
Stage 3: Severe/decompensated lens-induced glaucoma
- IOP: 45 to 55+ mm Hg
- Lens: Hypermature cataract with liquefied cortex or extensive capsular compromise
- Cornea: Marked stromal and epithelial edema, often obscuring the view
- AC reaction: Intense inflammation with dense flare, fibrin, or pseudohypopyon
- Angle:
- Phacolytic → Open, with dense proteinaceous and cellular obstruction, reduced trabecular function
- Lens particle → Open, with persistent particulate blockage and secondary trabecular damage
- Phacoanaphylactic → Open, with chronic inflammatory damage, early synechial closure possible
- Phacomorphic → Appositional closure with developing PAS
- Pupillary block (phacotopic) → Fixed angle closure or structural angle distortion from lens entrapment
- Optic nerve: Definite glaucomatous damage
- Symptoms: Severe pain, nausea/vomiting, profound vision loss
Implication: High risk of intra- and postoperative surgical complications; postoperative IOP control is often difficult.[85]
Stage 4: Chronic/advanced lens-induced glaucoma
- IOP: Persistently elevated or fluctuating despite medical therapy
- Lens: Long-standing hypermature or previously removed cataract with secondary damage
- Cornea: Chronic edema or bullous keratopathy
- AC reaction: Low-grade or burnt-out inflammation
- Angle: Peripheral anterior synechiae involving >180°
- Optic nerve: Advanced glaucomatous cupping with severe field loss
- Symptoms: prolonged duration (>2–4 weeks), severe visual impairment (counting fingers to hand motion)
Implication: Lens extraction alone is insufficient; long-term IOP-lowering therapy or glaucoma surgery (trabeculectomy or tube shunt) is frequently required.[86]
Table 16. Prognostic Staging (Postoperative Expectation)
|
Stage |
Postoperative Recovery |
|
0–1 |
Excellent; intraocular pressure normalizes quickly |
|
2 |
Good, but monitor for steroid response and early peripheral anterior synechiae |
|
3 |
Limited; frequent need for long-term intraocular pressure control |
|
4 |
Poor; high chance of chronic glaucoma despite surgery |
Summary
Lens-induced glaucoma staging is multidimensional, incorporating:
- IOP severity
- Lens condition
- Inflammation intensity
- Angle status
- Optic nerve health
- Chronicity
This structured approach helps:
- Predict prognosis
- Guide surgical timing
- Inform patient counseling
- Identify the need for adjunct glaucoma therapy [3]
Prognosis
Lens-induced glaucoma carries a highly variable prognosis, primarily determined by time to presentation, the severity of IOP elevation, the degree of optic nerve compromise, and the presence of permanent angle damage. Because lens-induced glaucoma is typically a consequence of a long-standing, mature, or hypermature cataract, many patients present late, often with significantly elevated IOP and inflammatory changes. The single most important prognostic factor is the speed with which definitive lens extraction is performed after IOP elevation begins.
The following sections describe the expected outcomes based on disease severity at presentation.
Early Diagnosis and Prompt Surgical Intervention
When lens-induced glaucoma is recognized early (ie, before peripheral anterior synechiae, severe inflammation, or optic nerve damage occurs), the prognosis is excellent.
- IOP usually normalizes within hours to days after lens removal.
- Corneal edema resolves quickly.
- Visual acuity commonly improves dramatically, depending on preexisting cataract density.
- Very few patients require long-term glaucoma medications.
- The angle structure reverses if appositional closure is short-lived.[87]
Outcome: Patients presenting within 24 to 72 hours of symptom onset have the best visual and pressure outcomes.
Moderate Disease/Delayed Presentation
Outcomes decline progressively after 7 to 10 days of uncontrolled IOP elevation. In patients presenting after several days of symptoms:
- IOP may take longer to normalize.
- Corneal edema may persist for several days due to endothelial dysfunction.
- Inflammation may be more intense, requiring prolonged steroids.
- Early optic nerve damage may already be detectable.[88]
While many cases still achieve good visual outcomes, a significant proportion require ongoing medical therapy to maintain target pressure.
Outcome: Functional vision often improves, but long-term follow-up is essential.
Advanced or Chronic Disease
Patients presenting late (often weeks after symptom onset) face significantly worse outcomes.
Common predictors of poor prognosis:
- Peripheral anterior synechiae (peripheral anterior synechiae ≥180°)
- Very high IOP (>45–50 mm Hg) for prolonged duration
- Severe corneal edema or endothelial decompensation
- Optic nerve cupping at presentation
- Prolonged inflammatory attack (phacolytic, phacoanaphylactic)
- Lens dislocation with chronic angle damage (pupillary block/phacotopic) [89]
In these patients:
- Visual recovery may be limited.
- Chronic secondary glaucoma is common.
- Many require long-term IOP-lowering medications.
- Some require trabeculectomy or glaucoma drainage devices post-cataract surgery.
- Combined cataract extraction and trabeculectomy may achieve early IOP control; however, long-term trabeculectomy failure rates remain high in these cases.
Outcome: Late presentation considerably worsens prognosis; optic nerve and angle changes are often irreversible.[2]
Subtype-Specific Prognostic Considerations
- Phacolytic glaucoma
- Usually excellent visual and pressure recovery after timely lens extraction
- Worse prognosis with prolonged inflammation [90]
- Lens particle glaucoma
- Excellent prognosis if retained fragments are removed early
- Risk of trabeculitis and persistent IOP elevation with delayed clearance
- Phacoanaphylactic glaucoma (lens-induced uveitis)
- Prognosis dependent on severity of granulomatous inflammation
- Increased risk of postoperative cystoid macular edema and chronic uveitic glaucoma
- Phacomorphic glaucoma
- Best prognosis with early intervention
- Risk of permanent peripheral anterior synechiae (PAS) and chronic angle closure with delayed treatment
- Pupillary block (phacotopic) glaucoma
- Prognosis dependent on the angle status, lens position, and duration
- Irreversible TM damage with long-standing dislocation [70]
Prognostic Indicators
Good prognostic indicators
- Early intervention (<3 days)
- No optic nerve damage at presentation
- No vitreous involvement or posterior segment disturbance
- Minimal corneal edema
- Open angles without PAS
- Mild inflammation
Poor prognostic indicators
- Delayed presentation (>1–2 weeks)
- Optic disc cupping
- Severe corneal edema or endothelial compromise
- Extensive PAS
- Recurrent IOP spikes
- Secondary glaucomatous optic neuropathy
- Poor pupillary dilation (suggesting chronic inflammation or PXF)
- Absent or severely impaired light projection [91]
Long-Term Prognosis
Even after successful cataract extraction:
- Approximately 10% to 30% of patients may develop chronic glaucoma, depending on the severity at presentation.
- Visual prognosis may remain guarded if the optic nerve or macula was compromised.
- Regular follow-up is critical, especially in Stage 3 to 4 disease.
Most important: When cataract surgery is done promptly, and angle/nerve damage has not yet occurred, lens-induced glaucoma is one of the most recoverable glaucomas.
Public Health Relevance
In many developing regions, lens-induced glaucoma remains a significant cause of avoidable blindness. Earlier cataract detection, timely surgery, and community outreach substantially improve overall prognosis at the population level.[92]
Complications
Complications of lens-induced glaucoma reflect the effects of prolonged IOP elevation, inflammation, surgical complexity, and irreversible ocular damage (see Tables 17–20).[2] The following tables summarize complications across mechanisms, clinical subtypes, timing relative to surgery, and disease stage.
Table 17. Complications of Lens-Induced Glaucoma by Pathophysiologic Mechanism
|
Category |
Complication |
Description/Clinical Significance |
|
Ocular Structural Damage |
Corneal edema/endothelial Decompensation |
Elevated intraocular pressure (IOP) and inflammation can cause stromal/epithelial edema and permanent endothelial loss → persistent visual impairment |
|
Peripheral anterior synechiae (PAS) |
Prolonged pupillary block or angle closure results in the formation of PAS → chronic angle closure glaucoma |
|
|
Shallow/flat anterior chamber |
Forward displacement of lens in phacomorphic glaucoma → risk of iridocorneal contact |
|
|
Optic Nerve Damage |
Acute glaucomatous optic neuropathy |
Severe IOP spikes cause rapid optic nerve injury → permanent vision loss |
|
Chronic secondary glaucoma |
Permanent trabecular dysfunction → persistent or lifelong need for IOP-lowering therapy |
|
|
Inflammation-Related Complications |
Severe anterior uveitis |
Lens protein leakage → intense anterior chamber inflammation, flare, and photophobia |
|
Fibrin membrane formation |
Seen in phacoanaphylactic or phacolytic glaucoma → may obstruct pupil/visual axis |
|
|
Cystoid macular edema (CME) |
Postoperative inflammatory complication → central vision impairment |
|
|
Intraocular lens (IOL) surface deposits (pigment/proteinaceous) |
Seen after phacolytic, lens particle, or phacoanaphylactic glaucoma; may cause visual disturbance and persistent inflammation | |
|
Lens and Capsule–Related |
Capsular bag compromise |
Hypermature cataract → increased risk of capsular rupture and zonular dialysis |
|
Phacodonesis/lens subluxation |
Weak zonules in hypermature cataract → unstable lens, risk of phacotopic glaucoma |
|
|
Aphakia |
Results from inadequate capsular or zonular support; may require secondary IOL implantation | |
|
Infection-Related |
Endophthalmitis |
Rare; occurs in cases of severe surgical wound contamination or preexisting inflammation |
|
Surgical Complications |
Posterior capsular rupture |
Occurs during the extraction of swollen or liquefied lenses → need for pars plana vitrectomy (PPV) |
|
Retained lens fragments |
Retained cortical or nuclear lens fragments → persistent inflammation and elevated IOP |
|
|
IOL decentration/subluxation |
Zonular compromise → need for capsular support devices or secondary IOL fixation |
|
|
Dropped nucleus/posterior dislocation of lens fragments |
Occurs during the extraction of hypermature or intumescent cataracts; often requires PPV | |
|
Corneal Complications |
Bullous keratopathy |
Chronic high IOP and endothelial injury → painful edema requiring keratoplasty |
|
Postoperative IOP Issues |
IOP spikes |
Common due to retained viscoelastic, inflammation, or trabecular meshwork dysfunction |
|
Steroid-induced ocular hypertension |
Occurs due to prolonged postoperative steroid use |
|
|
Posterior Segment Complications |
Vitreous loss |
Intraoperative complication requiring PPV; increases the risk of CME |
|
Retinal detachment (rare) |
More common if the capsule is compromised or high myopia is present |
|
| End-Stage Complications |
Painful blind eye |
Result of uncontrolled IOP, corneal decompensation, or phthisis; may require cyclodestructive procedures or enucleation |
Table 18. Complications of Lens-Induced Glaucoma by Clinical Subtype
|
Subtype |
Key Complications |
Clinical Notes |
|
Phacolytic Glaucoma |
|
Caused by the leakage of high-molecular-weight proteins from the hypermature lens |
|
Lens Particle Glaucoma |
|
Retained cortical/nuclear fragments cause inflammation; good prognosis if removed early |
|
Phacoanaphylactic (Lens-Induced Uveitis) |
|
Immune-mediated; risk of postoperative inflammation and macular edema |
|
Phacomorphic Glaucoma |
|
Pupillary block and forward lens movement; permanent angle closure if untreated |
|
Phacotopic Glaucoma (Lens Dislocation) |
|
Occurs in trauma, Marfan, pseudoexfoliation; may require lensectomy/PPV |
AC, anterior chamber; CME, cystoid macular edema; IOP, intraocular pressure; PPV, pars plana vitrectomy; TM, trabecular meshwork
Table 19. Complications of Lens-Induced Glaucoma by Timing Relative to Surgery
|
Category |
Complication |
Clinical Relevance |
|
Early Postoperative |
IOP spikes |
Common; occurs due to retained viscoelastic, TM dysfunction, and inflammation |
|
Corneal edema |
May persist in cases with preoperative endothelial damage |
|
|
Severe uveitis/fibrin reaction |
Especially in phacolytic and phacoanaphylactic eyes |
|
|
Wound leak/hypotony |
Leads to shallow AC and risk of choroidal detachment |
|
|
Retained lens fragments |
Require AC washout or vitrectomy |
|
|
Hyphema |
Caused by iris manipulation or high preoperative pressure |
|
|
Intermediate Postoperative |
Steroid-induced ocular hypertension |
Must monitor IOP closely |
|
PAS progression |
Especially in delayed phacomorphic cases |
|
|
CME |
Common in inflammatory subtypes (phacoanaphylactic/phacolytic) |
|
|
IOL decentration or subluxation |
Occurs with zonular weakness or capsular compromise |
|
|
Late Postoperative |
Chronic secondary glaucoma |
Due to permanent TM damage or PAS |
|
Bullous keratopathy |
From significant endothelial loss |
|
|
Chronic uveitis |
Particularly in autoimmune-mediated cases | |
|
Retinal detachment (rare) |
More likely in phacotopic cases or posterior capsular rupture |
AC, anterior chamber; CME, cystoid macular edema; IOL, intraocular lens; IOP, intraocular pressure; PAS, peripheral anterior synechiae; TM, trabecular meshwork
Table 20. Complications of Lens-Induced Glaucoma by Disease Stage and Mechanism
|
Stage |
Associated Complications |
Pathophysiology |
|
Stage 1 (Early) |
Reversible corneal edema, mild uveitis |
Acute IOP rise, protein leakage |
|
Stage 2 (Moderate) |
Endothelial stress, early optic nerve damage, TM inflammation |
Persistent IOP elevation, macrophage load |
|
Stage 3 (Severe) |
Permanent PAS, severe corneal edema, optic neuropathy |
Long-standing inflammation + angle closure |
|
Stage 4 (Chronic) |
Chronic glaucoma, bullous keratopathy, CME, poor visual recovery |
Irreversible TM and optic nerve injury |
CME, cystoid macular edema; IOP, intraocular pressure; PAS, peripheral anterior synechiae; TM, trabecular meshwork
Postoperative and Rehabilitation Care
The postoperative and rehabilitation phases following surgery for lens-induced glaucoma are essential for visual recovery and long-term IOP control. Management focuses on mitigating the consequences of prolonged IOP elevation, preexisting inflammation, endothelial compromise, and possible optic nerve injury.[2] Many patients require systemic corticosteroids, osmotic agents, and analgesics in the perioperative and early postoperative periods. Close early monitoring of IOP and anterior chamber inflammation is crucial to preserve corneal clarity, optimize surgical outcomes, and reduce the risk of persistent glaucoma. During the rehabilitation period, regular assessment of IOP, optic nerve status, and visual function is recommended, with refractive correction typically performed 4 to 6 weeks after surgery to support visual rehabilitation.[4] Postoperative care can be conceptualized in three phases: immediate, intermediate, and long-term, each with distinct priorities and management goals.
Immediate Postoperative Care (First 24–72 Hours)
Monitoring
- Measure IOP every 4 to 6 hours on day 1 in high-risk cases.
- Check for corneal clarity, AC depth, pupil shape, wound integrity, and presence of fibrin or hyphema.[8]
- Evaluate for retained lens fragments.
Medications
- Topical corticosteroids (prednisolone acetate 1% or dexamethasone)
- Frequency: 6 to 8 times/day initially
- Purpose: Controls severe postoperative inflammation, especially in phacolytic and phacoanaphylactic glaucoma [2]
- Cycloplegics (atropine or homatropine)
- Reduces pain, stabilizes the blood-aqueous barrier, and prevents synechiae [5]
- Topical antibiotics
- Frequency: 4 times/day for 1 week
- IOP-lowering agents
- Beta-blockers, alpha-agonists, carbonic anhydrase inhibitors
- Avoid prostaglandin analogs early due to inflammation
- Hypertonic saline if corneal edema persists
Addressing early complications
- Retained viscoelastic–related IOP spikes
- Managed with topical therapy or wound burping
- Severe inflammation or retained lens material
- May require anterior chamber washout
- Fibrin membrane formation
- Treated with intensive topical steroids or intracameral tPA[3]
Intermediate Postoperative Care (1–4 Weeks)
Goals:
- Control inflammation
- Achieve stable IOP
- Promote corneal and macular recovery
- Detect chronic angle changes
Follow-up schedule
- Day 1
- Week 1
- Weeks 3 to 4 [6]
Tasks at each visit
- IOP measurement
- Corneal status evaluation
- Gonioscopy (at week 3–4) to assess for PAS
- Optic nerve evaluation (cup-to-disc ratio, retinal nerve fiber layer, optical coherence tomography [OCT] if view allows)
Medication adjustments
- Gradually taper topical steroids over 4 to 6 weeks.
- Continue aqueous suppressants if IOP remains borderline.
- Treat steroid-induced IOP elevation, if present.[4]
Monitoring for complications
- Cystoid macular edema: Perform OCT if visual recovery is delayed.
- Persistent corneal edema: Consider endothelial assessment.
- IOL centration: Evaluate for zonular compromise.
Long-Term Rehabilitation (1–6 Months+)
Visual rehabilitation
- Refraction
- Provided at 4 to 6 weeks after complete corneal stabilization
- Spectacle correction or bifocals for pseudophakia
- Low-vision support (if optic neuropathy is severe)
- Magnifiers, contrast-enhancing lenses, and orientation training
Glaucoma surveillance
- Long-term follow-up is mandatory because chronic glaucoma can develop even after successful surgery.[6]
- Monitoring includes:
- IOP every 1 to 3 months initially
- Optic nerve OCT
- Visual fields (if fixation stable)
- Gonioscopy annually or earlier with symptoms
Management of chronic glaucoma
- Long-term aqueous suppressants if TM damage persists
- Trabeculectomy or glaucoma drainage implants in non-responsive cases
- Laser iridoplasty or goniosynechiolysis in selected phacomorphic cases with persistent PAS [21]
Rehabilitation Considerations in Special Populations
- Older or cognitively impaired individuals
- These patients often require caregiver involvement to ensure medication adherence. Simplified treatment regimens are preferred, and education for the patient and caregivers should focus on recognizing symptoms of IOP elevation or recurrent inflammation.
- Patients with markedly delayed presentation
- These individuals are at higher risk of optic nerve damage and may require early or additional glaucoma surgery. Visual prognosis may be guarded, and early counseling regarding expectations is essential.[3]
- Unilateral severe lens-induced glaucoma with fellow-eye dense cataract
- The fellow eye should be evaluated promptly due to the risk of recurrent lens-induced glaucoma. Early cataract surgery in the fellow eye may be considered as a preventive strategy.
Patient Education and Lifestyle Guidance
- Postoperative care instructions: Hygiene, medications, and follow-up schedule
- Activity restrictions: Avoid eye rubbing, heavy lifting, or water exposure for the first week
- Warning symptoms: Prompt reporting of redness, pain, halos, or sudden vision loss
- Expectations: Lens pathology is corrected, but ongoing glaucoma risk may persist [2]
Outcome Measures
Patients with early intervention often achieve:
- Rapid IOP normalization
- Good visual recovery
- Minimal long-term therapy
Patients with late-stage lens-induced glaucoma may experience:
- Chronic glaucoma
- Permanent visual field loss
- Persistent corneal changes
- Dependence on long-term medical and/or surgical glaucoma therapy
Postoperative and rehabilitation care following lens-induced glaucoma surgery requires intensive early management, close intermediate monitoring, and long-term glaucoma surveillance. Successful visual and functional rehabilitation hinges on controlling inflammation, ensuring IOP stability, monitoring for complications, and providing tailored support based on optic nerve status and patient-specific factors.[3]
Consultations
Management of lens-induced glaucoma often requires targeted specialty consultations, particularly in acute presentations, moderate-to-severe disease, or patients with significant systemic comorbidities. Conditions such as diabetes mellitus, hypertension, renal disease, and cardiovascular disease may influence medical therapy choices and perioperative planning, necessitating coordination with treating physicians to optimize patients for surgical intervention. Timely consultation with appropriate ophthalmic subspecialists enhances patient safety, facilitates definitive management, and improves visual and pressure-related outcomes.[93]
Ophthalmology Subspecialty Consultations
Glaucoma specialist
A glaucoma specialist should be involved when:
- IOP remains uncontrolled despite maximal therapy
- Extensive peripheral anterior synechiae are present
- Advanced optic nerve damage is suspected
- Combined cataract–glaucoma surgery may be beneficial
- Secondary surgical interventions (trabeculectomy, glaucoma drainage device) are anticipated
They provide expertise in gonioscopy interpretation, glaucoma risk stratification, and long-term management strategies.[94]
Cornea specialist
Consultation is recommended in cases with:
- Severe corneal edema
- Endothelial compromise
- Bullous keratopathy following surgery
- Irreversible endothelial failure requiring consideration of keratoplasty (descemet stripping endothelial keratoplasty, descemet membrane endothelial keratoplasty)
- Poor visualization due to corneal haze during cataract surgery
Cornea specialists assist in preoperative planning and postoperative rehabilitation.[95]
Vitreoretinal surgeon
Consultation is recommended in cases with:
- Retained lens fragments requiring posterior segment removal
- Posterior dislocation of the lens or nucleus (pupillary block/phacotopic glaucoma)
- Dense vitreous inflammation obscuring fundus visualization
- Suspected or confirmed retinal tears or detachment [96]
Deterrence and Patient Education
Lens-induced glaucoma is a largely avoidable cause of ocular morbidity, and effective prevention relies on patient awareness, timely cataract intervention, and community-level education. Because lens-induced glaucoma frequently arises from long-standing mature or hypermature cataracts, especially in underserved populations, patient education plays a vital role in reducing avoidable blindness.[3]
Educating Patients on Cataract Progression and Risks
Patients should be counseled that:
- Cataracts do not need to become “white” or “ripe” before surgery.
- Long-standing cataracts can cause dangerous spikes in IOP, leading to irreversible optic nerve damage.
- Early cataract surgery is safe and effective, and it prevents lens-induced glaucoma entirely.
- Sudden pain, redness, headache, or vision loss in a cataract-bearing eye requires emergency evaluation.
Clear explanations help dispel common myths, especially in rural and older populations.[2]
Warning Signs Requiring Urgent Attention
Patients and caregivers must recognize symptoms of impending lens-induced glaucoma, which may include the following:
- Sudden decrease in vision
- Eye pain or headache
- Marked redness
- Seeing halos around lights
- Nausea or vomiting associated with eye discomfort [8]
Immediate reporting of these symptoms can prevent optic nerve injury.
Preventive Measures for At-Risk Groups
Older individuals
Encourage:
- Annual eye examinations beginning at age 60
- Earlier assessments in cases of reduced vision or functional decline
- Timely cataract intervention to prevent progression [4]
Patients with diabetes or hypertension
Encourage:
- Regular ophthalmic follow-up is provided to monitor accelerated cataract progression.
- Prompt cataract surgery once the cataract becomes visually significant.
Patients with limited access to care or low health literacy
Encourage:
- Community-based screening programs (eg, village outreach, mobile clinics)
- Use of simple, culturally appropriate educational materials
- Engagement of community health workers to facilitate follow-up and referral [5]
Children with ectopia lentis–associated syndromes (eg, Marfan syndrome, homocystinuria, Weill-Marchesani syndrome)
Encourage:
- Early ophthalmic screening for lens subluxation or dislocation
- Regular IOP monitoring to detect secondary glaucoma
- Periodic refraction assessment to support visual development
Postoperative Education to Prevent Recurrent Issues
Following treatment for lens-induced glaucoma, clinicians should:
- Stress the importance of follow-up visits for IOP monitoring.
- Educate patients about medication adherence (steroids, IOP-lowering drops).
- Demonstrate correct eye-drop instillation.
- Inform patients about the possibility of chronic glaucoma.
- Provide instructions about protecting the operated eye during rehabilitation.
- Discuss the need for cataract surgery in the fellow eye before it becomes hypermature.[6]
Role of Family and Caregivers
Given that lens-induced glaucoma often affects older individuals:
- Families should encourage cataract screening for all older relatives.
- Family members should accompany patients to appointments to support informed decision-making.
- Caregivers should help monitor symptoms before and after surgery.
- Care partners should assist with adherence to postoperative medication schedules.
Family involvement improves outcomes dramatically.[21]
Community and Public Health Education
To prevent lens-induced glaucoma at the population level:
- Conduct cataract screening camps, especially in rural and underserved areas.
- Promote awareness among local leaders through posters and via radio/social media messages.
- Encourage early referral from primary health centers.
- Train front-line workers (auxiliary nurse midwives, accredited social health activists, optometrists) to identify mature cataracts.
- Emphasize the fact that cataract surgery is typically painless, affordable, and widely available.
Public health education encourages timely intervention and prevents advanced disease.[12]
Addressing Barriers to Care
Educate patients about:
- Affordable options: government systems, insurance, nongovernment organization-supported surgeries
- Transport assistance: community programs, mobile vans
- Safety: Modern cataract surgery has excellent outcomes
- Myths: Cataract does NOT need to “ripen”; surgery is not risky if done early
Addressing misconceptions improves surgical acceptance.
Empowering Patients After Treatment
Patients should understand:
- Vision may continue to improve over the weeks.
- New symptoms should be reported immediately.
- Long-term glaucoma surveillance is crucial.
- Protective eyewear should be used outdoors.
- Spectacle correction will be given at 4 to 6 weeks.[12]
Summary
Deterrence of lens-induced glaucoma relies on:
- Early detection of cataracts
- Strong patient education
- Caregiver involvement
- Community awareness programs
Effective patient and public education can virtually eliminate lens-induced glaucoma, making it one of the most preventable causes of secondary glaucoma and blindness worldwide.[52]
Pearls and Other Issues
The following pearls and practical considerations emphasize high-yield concepts and common pitfalls in the care of patients with lens-induced glaucoma, from early recognition and subtype differentiation to surgical preparedness and postoperative vigilance.
Clinical Pearls
- Lens-induced glaucoma is completely preventable.
- The single most crucial pearl is that lens-induced glaucoma rarely occurs when cataracts are detected and treated early. Mature and hypermature lenses (still common in underserved populations) remain the primary modifiable risk factor.[3]
- The cure is early cataract surgery, not prolonged medical therapy.
- IOP-lowering medications are only a temporary bridge. Definitive treatment requires removal of the offending lens; delays increase the risk of irreversible angle closure and optic nerve damage.[2]
- Corneal clarity determines surgical timing—not IOP alone.
- Even after IOP is lowered, corneal edema may prevent safe surgery. Hyperosmolar agents, such as mannitol, and topical therapy must be optimized to create a clear surgical window. Attempting surgery too early can compromise visualization and increase complications.[4]
- Phacolytic and phacomorphic subtypes behave differently.
- Recognizing the mechanism guides appropriate management and helps avoid common pitfalls, such as unnecessary iridotomy in phacolytic cases.[7]
- Phacolytic glaucoma: primarily inflammatory, open-angle obstruction
- Phacomorphic glaucoma: primarily mechanical, angle-closure mechanism
- Recognizing the mechanism guides appropriate management and helps avoid common pitfalls, such as unnecessary iridotomy in phacolytic cases.[7]
- Long-term glaucoma monitoring is essential.
- Even when surgery is successful and pressure normalizes, some patients develop chronic glaucoma due to preoperative trabecular injury or PAS formation. Scheduled follow-up for IOP, gonioscopy, optical coherence tomography, retinal nerve fiber layer, and visual fields is mandatory.[21]
- MSICS is often safer than phacoemulsification in lens-induced glaucoma.
- Unless phaco can be performed by a highly experienced surgeon, MSICS provides safer nucleus delivery, less endothelial insult, and lower intraoperative complication rates for intumescent, hypermature, or Morgagnian cataracts.
- Screen the fellow eye.
- Many patients presenting with lens-induced glaucoma have a similarly advanced cataract in the fellow eye. Early elective surgery in the non-glaucomatous eye helps prevent recurrence of lens-induced mechanisms.
- Optic nerve damage can occur even in a short duration.
- IOP spikes in phacomorphic glaucoma, even for a few days, can cause rapid axonal injury, underscoring the urgency of timely intervention.
- Community education is as crucial as surgery.
- Lens-induced glaucoma often arises from delayed presentation due to:
- Fear of surgery
- Misbelief: Cataracts must “ripen”
- Limited access
- Low literacy
- Lack of family support
- Public health outreach, routine screening, and early referral drastically reduce the incidence of lens-induced glaucoma.[52]
- Lens-induced glaucoma often arises from delayed presentation due to:
Common Pitfalls
- Misdiagnosis as primary angle-closure glaucoma
- Older adults with a white, mature cataract may present with a shallow AC, high IOP, and corneal edema. Failure to recognize the enlarged lens as the cause can delay appropriate treatment and worsen prognosis.[7]
- Underestimation of zonular weakness
- Chronic hypermaturity and pseudoexfoliation can severely weaken zonules. Anticipating the need for capsular tension rings, iris hooks, or conversion to manual small-incision cataract surgery helps prevent intraoperative complications.[5]
- Failure to identify retained lens fragments after surgery
- Persistent postoperative inflammation or spikes in IOP often indicate retained cortical or nuclear material. Early AC washout or posterior segment cleanup prevents long-term trabecular damage.[21]
- Unrecognized steroid-induced IOP elevation
- Eyes with lens-induced glaucoma are already prone to IOP instability. Prolonged corticosteroid use may precipitate further pressure elevation, necessitating cautious tapering and frequent IOP monitoring.[12]
Social and System-Level Issues
- Lens-induced glaucoma disproportionately affects older, socioeconomically disadvantaged, and rural populations.
- Enhancing access to and affordability of cataract surgery remain public health priorities.
- Training primary care and community health workers to detect mature cataracts helps prevent late-stage presentations.
In summary, lens-induced glaucoma is a highly preventable condition in which timely intervention profoundly influences visual outcomes, underscoring the importance of education, system-level awareness, and multidisciplinary planning.[97]
Enhancing Healthcare Team Outcomes
Effective management of lens-induced glaucoma requires a coordinated, interprofessional team approach, as patients often present late, in severe pain, or with limited visual capacity. Optimizing outcomes depends on the seamless integration of skills across ophthalmologists, optometrists, nurses, pharmacists, primary care providers, community health workers, and social support personnel. Collaborative practice improves patient safety, ensures timely surgical intervention, reduces postoperative complications, and enhances long-term visual rehabilitation.[93]
Professional Roles
Ophthalmologist/cataract surgeon
- Diagnoses the specific subtype of lens-induced glaucoma (phacomorphic, phacolytic, lens particle).
- Coordinates acute management, including IOP lowering, inflammation control, and surgical planning.
- Communicates clearly with anesthesia, nursing, and pharmacy staff regarding perioperative needs.
- Performs cataract extraction or refers to subspecialists when needed (glaucoma, retina, cornea).
- Ensures ethical decision-making, particularly for older or cognitively impaired patients who require support with consent.[87]
Glaucoma specialist
- Assists with complex IOP management, gonioscopic interpretation, and angle assessment.
- Performs or advises on combined cataract–glaucoma procedures when indicated.
- Provides long-term monitoring for chronic glaucoma.
- Enhances patient outcomes by preventing irreversible optic nerve damage.[98]
Optometrist/vision specialist
- Performs refraction, visual rehabilitation, and postoperative optical correction.
- Screens for potential complications, such as persistent corneal edema or reduced best-corrected vision.
- Reinforces patient education about protective eyewear, medication adherence, and early warning signs.[6]
Nursing team
Nurses play a central role in patient-centered care for lens-induced glaucoma:
- Triages patients presenting with acute pain or reduced vision.
- Measures IOP, assesses ocular surface, and monitors corneal clarity.
- Provides preoperative counseling, postoperative instruction, and drop administration teaching.
- Identifies early signs of complications such as IOP spikes or severe uveitis.
- Ensures the implementation of infection-control protocols and safe perioperative preparation.[21]
Pharmacist
- Ensures appropriate dispensing of IOP-lowering medications, steroids, cycloplegics, and antibiotics.
- Screens for drug interactions, contraindications (eg, mannitol in congestive heart failure, acetazolamide in renal disease), and allergies.
- Reinforces correct dosing, tapering schedules, and adherence, which is particularly critical in older adults.
- Provides culturally appropriate guidance on medication safety.[95]
Anesthesiologist
- Manages patients with:
- Severe hypertension due to pain
- Comorbid systemic conditions
- Anxiety or agitation
- Ensures safe anesthesia selection for cataract surgery (topical, peribulbar, or general).[55]
Community health workers/social workers
Social support personnel are particularly important in rural and low-literacy populations.
- Facilitates early detection of cataracts before they become hypermature.
- Coordinates transportation, financial assistance, and follow-up reminders.
- Provides culturally sensitive explanations to dispel myths about cataract surgery.
- Helps ensure medication adherence in older or dependent individuals.[99]
Interprofessional Communication Strategies
To enhance outcomes:
- Use SBAR (situation–background–assessment–recommendation) for handoffs.
- Maintain shared treatment plans accessible to all team members.
- Conduct brief preoperative team huddles to anticipate intraoperative challenges (poor dilation, zonular weakness, corneal edema).
- Document and clearly communicate postoperative instructions, especially steroid taper schedules and IOP check timing.[100]
Ethical and Patient-Centered Care Considerations
- Obtain informed consent, taking into account cognitive status and the need for family involvement.
- Address disparities in access to care by offering guidance on affordable options.
- Maintain respect, privacy, and dignity—especially in anxious or older patients.
- Provide a transparent discussion about visual prognosis and long-term glaucoma risk.
Improving Patient Safety and Team Performance
Interprofessional collaboration reduces:
- Delays in surgical intervention
- Medication errors
- Failure-to-follow-up events
- Postoperative complications (IOP spikes, corneal edema, uveitis)
Team-based debriefing after complex lens-induced glaucoma surgeries enhances learning and improves system processes.
Optimal outcomes in lens-induced glaucoma depend on a cohesive healthcare team working with coordinated precision: early triage by nurses, accurate diagnosis by ophthalmologists, medical optimization by pharmacists, visual rehabilitation by optometrists, and community support by outreach workers. Strong communication, ethical care, shared decision-making, and patient-centered strategies significantly reduce preventable blindness and enhance overall treatment success.[101]
Media
(Click Image to Enlarge)
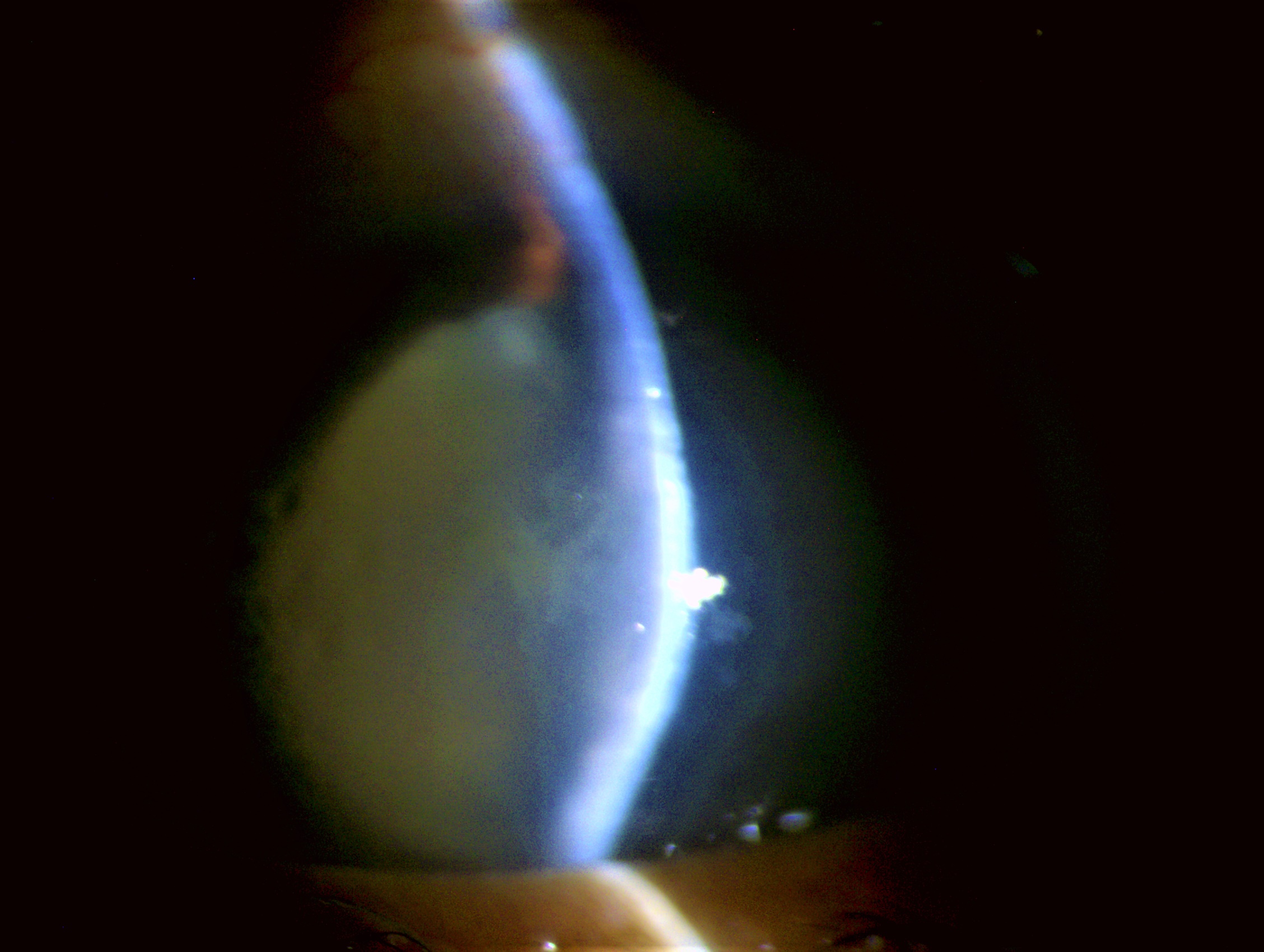
Phacomorphic Glaucoma. As a cataract matures, osmotic changes cause the lens to swell. The increased lens volume pushes the iris anteriorly, narrows the anterior chamber angle, and produces a relative pupillary block. This culminates in acute angle-closure glaucoma, often associated with severe pain, corneal edema, and markedly elevated intraocular pressure.
Contributed by S Shah, MBBS, MRCS
(Click Image to Enlarge)
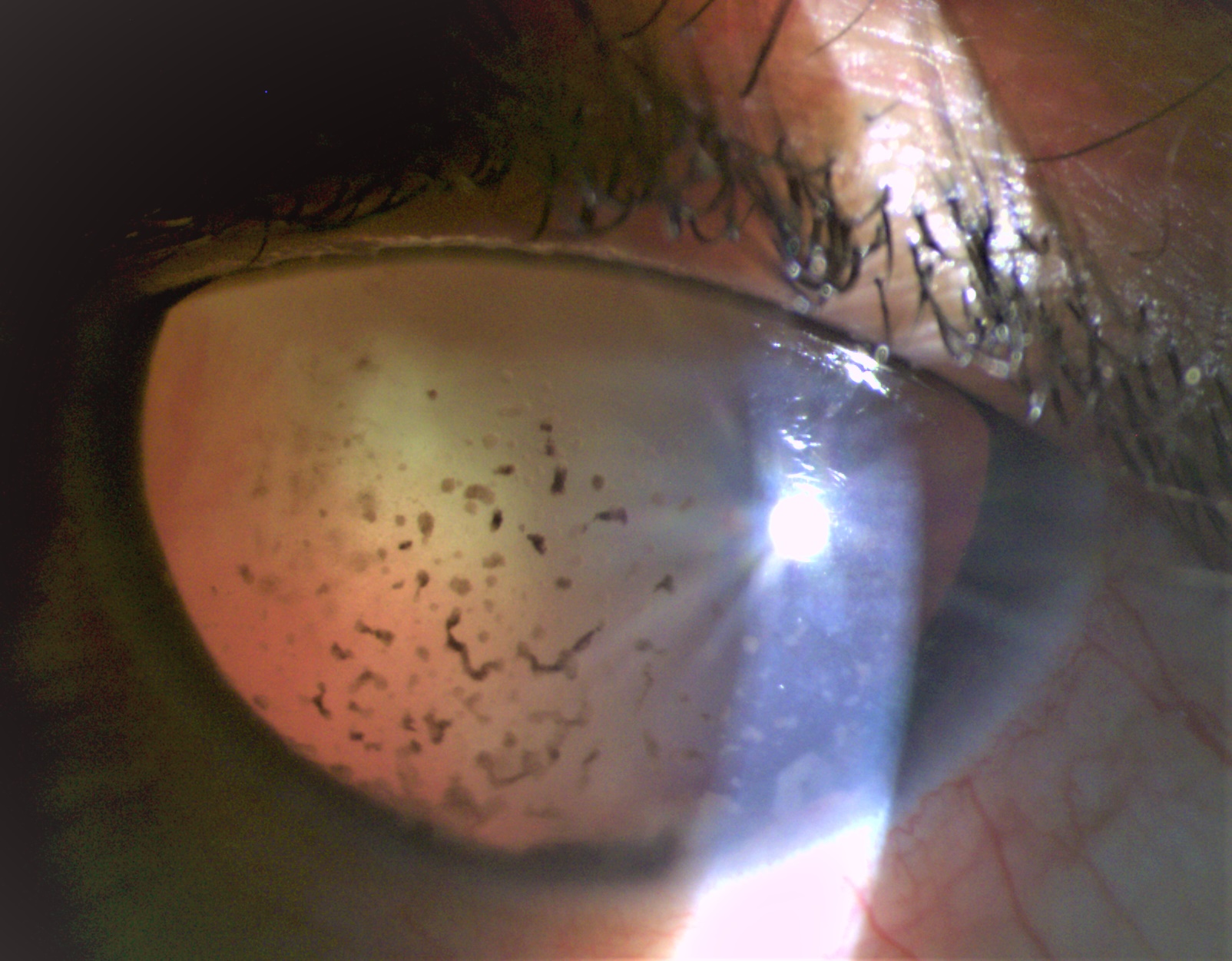
Phacoanaphylactic Glaucoma. This subtype is an immune-mediated granulomatous reaction to exposed lens proteins after surgery or trauma, resulting in intense anterior uveitis. Fibrin and inflammatory cells, particularly macrophages, clog the trabecular meshwork, dramatically reducing aqueous outflow.
Contributed by S Shah, MBBS, MRCS
(Click Image to Enlarge)
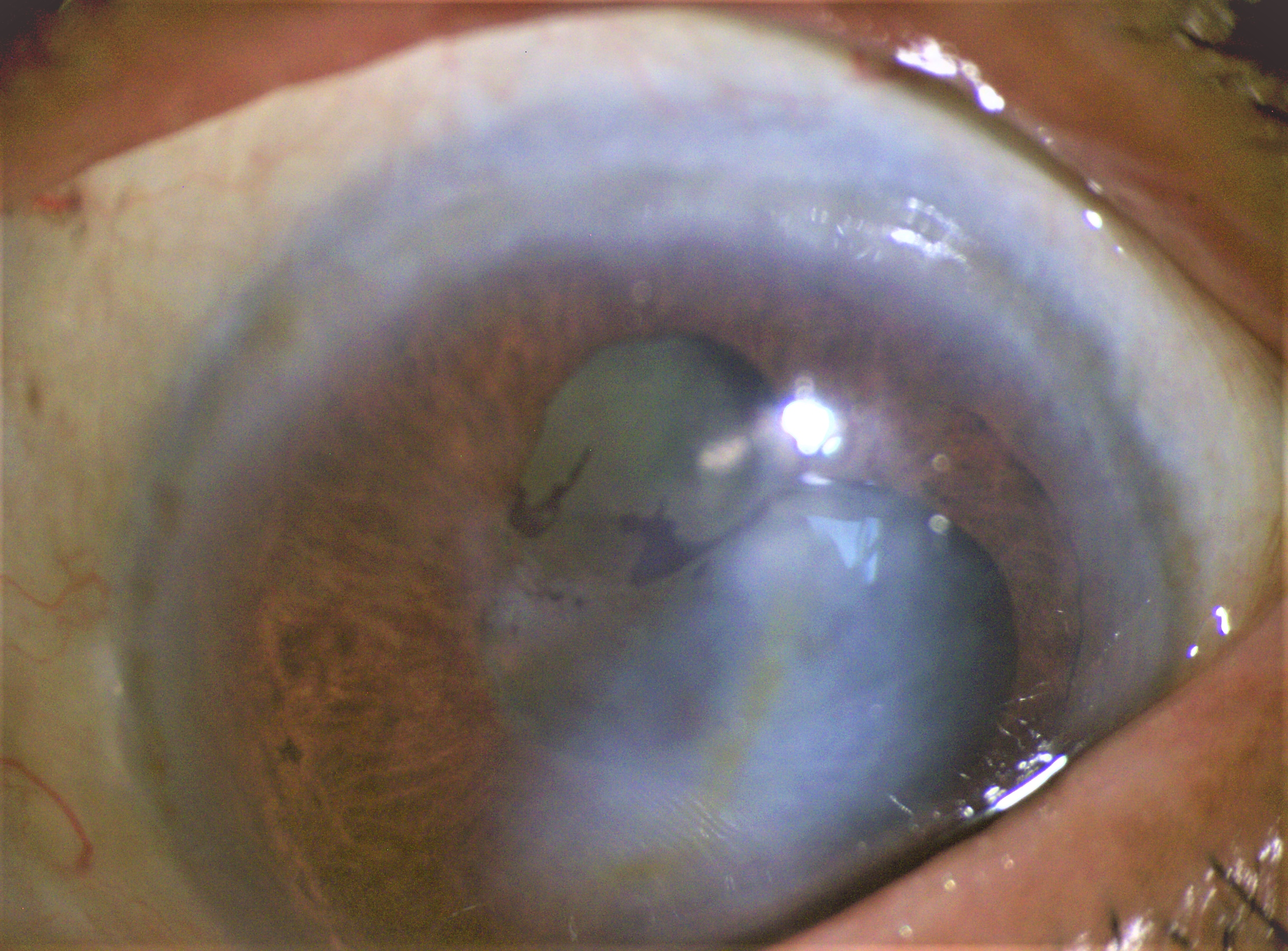
Phacolytic Glaucoma. High-molecular-weight lens proteins leak into the anterior chamber, triggering macrophage recruitment. Swollen macrophages then obstruct the trabecular meshwork, reducing aqueous outflow and sharply elevating intraocular pressure; the chamber depth remains regular or deep.
Contributed by S Shah, MBBS, MRCSEd
(Click Image to Enlarge)
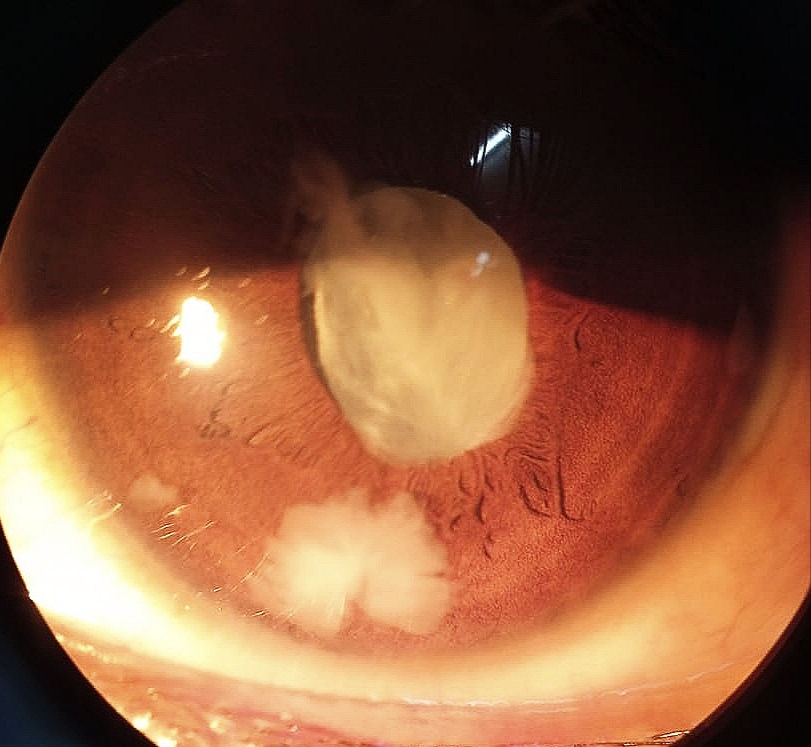
Lens Particle Glaucoma. Following cataract surgery, trauma, or spontaneous capsular rupture, cortical or nuclear lens fragments may enter the anterior chamber. These particles directly obstruct trabecular outflow and induce secondary inflammatory trabeculitis, thereby elevating intraocular pressure.
Contributed by S Shah, MBBS, MRCSEd
(Click Image to Enlarge)
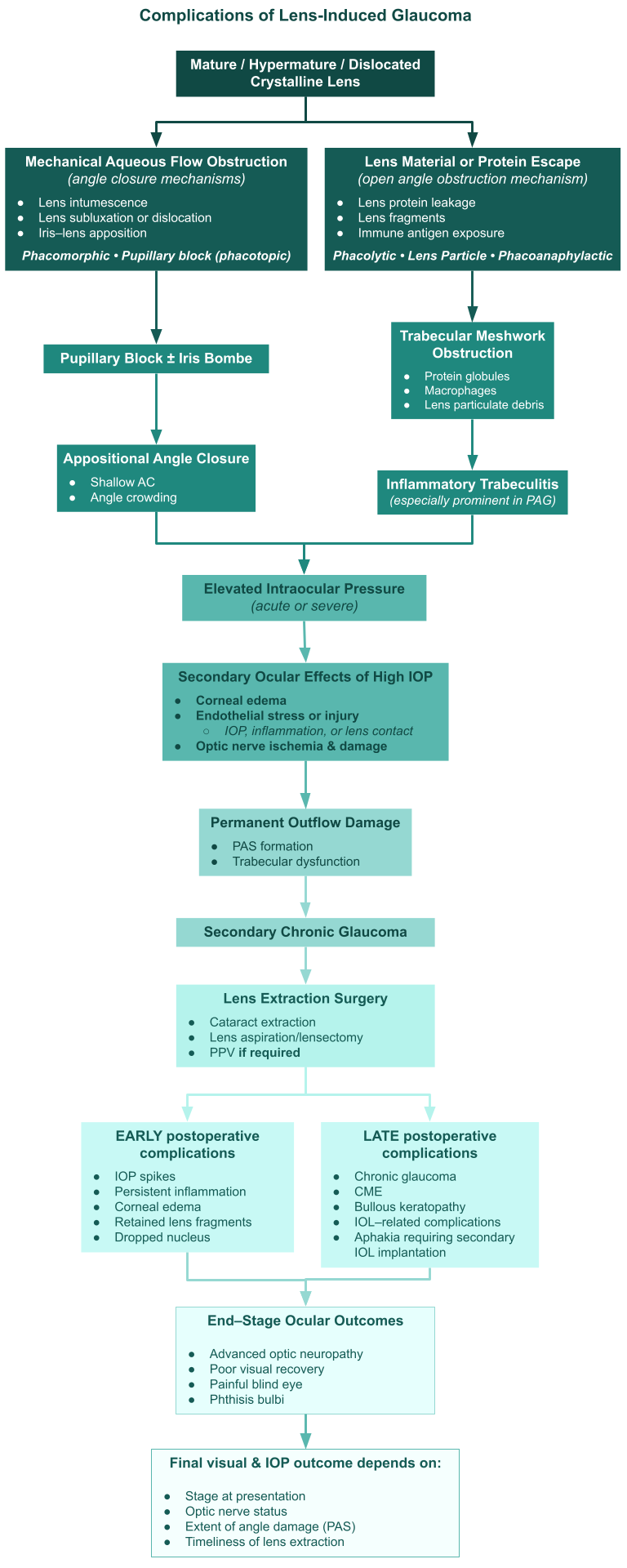
Complications of Lens-Induced Glaucoma. Mechanistic pathways and complications of lens-induced glaucoma, showing inflammatory and mechanical routes to intraocular pressure elevation, shared secondary ocular damage, postoperative outcomes, and end-stage sequelae.
Contributed by MH Kerekes, MD
References
Kothari R, Tathe S, Gogri P, Bhandari A. Lens-Induced Glaucoma: The Need to Spread Awareness about Early Management of Cataract among Rural Population. ISRN ophthalmology. 2013:2013():581727. doi: 10.1155/2013/581727. Epub 2013 Jun 25 [PubMed PMID: 24555131]
Morita S, Fujii T, Sakanishi Y, Usui-Ouchi A, Nakao S, Ebihara N. Surgical outcomes of interventions for treating intraocular lens-induced secondary pigment dispersion syndrome: a retrospective study. International ophthalmology. 2025 Oct 23:45(1):430. doi: 10.1007/s10792-025-03799-6. Epub 2025 Oct 23 [PubMed PMID: 41128808]
Level 2 (mid-level) evidenceRamakrishnan M, Singh P, Shetye R. Study of clinical profile in cases of secondary glaucoma at a tertiary hospital. Oman journal of ophthalmology. 2025 Sep-Dec:18(3):336-340. doi: 10.4103/ojo.ojo_408_24. Epub 2025 Oct 28 [PubMed PMID: 41230064]
Level 3 (low-level) evidenceAhn J, Jeong D. The Clinical Efficacy of a Topical Selective EP2 Receptor Agonist Against Feline Glaucoma That Is Not Responsive to Conventional Anti-Glaucoma Eyedrops. Veterinary ophthalmology. 2026 Jan:29(1):e70047. doi: 10.1111/vop.70047. Epub 2025 Jul 26 [PubMed PMID: 40714849]
Nur Faizah H, Nurul Hafizah MN, Juliana J, Wan-Hazabbah WH. A decade of intracapsular cataract extraction: Clinical profile and visual outcomes at Hospital Melaka, Malaysia. The Medical journal of Malaysia. 2025 Jan:80(1):68-71 [PubMed PMID: 39812431]
Zulaikha AR, Fhun LC, Ng SL, Shahidatul-Adha M. Two-year retrospective review of lens-induced glaucoma in Hospital Taiping, Perak, Malaysia. The Medical journal of Malaysia. 2024 Jul:79(4):452-456 [PubMed PMID: 39086343]
Level 2 (mid-level) evidenceIkeda SI, Sone K, Takai Y, Miyano T, Negishi K, Tsubota K, Kurihara T. Dose-dependent myopia-suppressing effect of 4-phenlybutyric acid eye drops in a mouse myopia model under masked condition. BMC ophthalmology. 2025 Jul 1:25(1):383. doi: 10.1186/s12886-025-04213-6. Epub 2025 Jul 1 [PubMed PMID: 40598091]
Angwatcharaprakan R, Lee EJ, Kim KH, Woo KI. Angle-Closure Glaucoma due to Lens Subluxation Associated With Orbital Arteriovenous Malformation. Ophthalmic plastic and reconstructive surgery. 2025 Sep 11:():. doi: 10.1097/IOP.0000000000003016. Epub 2025 Sep 11 [PubMed PMID: 40934899]
Ali KM, Mostafa AA. Lens-related ocular emergencies (LROE) in dogs: treatment and visual outcome after late presentation of 90 eyes. Irish veterinary journal. 2023 Jul 18:76(1):12. doi: 10.1186/s13620-023-00240-1. Epub 2023 Jul 18 [PubMed PMID: 37464438]
Zhang Y, Zhang H, Song X, Liu M, Wang N, Qiao C. Proportion and risk factors of zonulopathy in patients with age-related cataract. Heliyon. 2024 Apr 15:10(7):e28644. doi: 10.1016/j.heliyon.2024.e28644. Epub 2024 Mar 27 [PubMed PMID: 38586387]
Level 2 (mid-level) evidenceKrishna U, Odayappan A, Venkatesh R, Kavitha S. Changes in emergency glaucoma care during the COVID-19 pandemic in South India. Indian journal of ophthalmology. 2023 Mar:71(3):864-868. doi: 10.4103/ijo.IJO_1883_22. Epub [PubMed PMID: 36872695]
Jeong H, Lee D, Jiang X, Negishi K, Tsubota K, Kurihara T. Topical Application of Bunazosin Hydrochloride Suppresses Myopia Progression With an Increase in Choroidal Blood Perfusion. Investigative ophthalmology & visual science. 2023 Nov 1:64(14):15. doi: 10.1167/iovs.64.14.15. Epub [PubMed PMID: 37955611]
El Hamichi S, Aguilar RJ, Kon Graversen V, Gold AS, Berrocal AM, Murray TG. Lens-Induced Uveitis Triggered by Intravitreal Injection 40 Years after Primary Congenital Cataract Surgery with Aphakia. Case reports in ophthalmology. 2020 May-Aug:11(2):293-298. doi: 10.1159/000508390. Epub 2020 Jul 6 [PubMed PMID: 32774295]
Level 3 (low-level) evidenceChalla P, Hauser MA, Luna CC, Freedman SF, Pericak-Vance M, Yang J, McDonald MT, Allingham RR. Juvenile bilateral lens dislocation and glaucoma associated with a novel mutation in the fibrillin 1 gene. Molecular vision. 2006 Aug 28:12():1009-15 [PubMed PMID: 16971892]
Harrison DA, Mullaney PB, Mesfer SA, Awad AH, Dhindsa H. Management of ophthalmic complications of homocystinuria. Ophthalmology. 1998 Oct:105(10):1886-90 [PubMed PMID: 9787359]
Level 2 (mid-level) evidenceErkayhan GE, Dogan S. Cataract Surgery and Possible Complications in Patients with Pseudoexfoliation Syndrome. The Eurasian journal of medicine. 2017 Feb:49(1):22-25. doi: 10.5152/eurasianjmed.2016.0060. Epub 2016 Aug 18 [PubMed PMID: 28416927]
Fuchs J, Rosenberg T. Congenital ectopia lentis. A Danish national survey. Acta ophthalmologica Scandinavica. 1998 Feb:76(1):20-6 [PubMed PMID: 9541430]
Level 2 (mid-level) evidenceSingh S, Pardhan S, Kulothungan V, Swaminathan G, Ravichandran JS, Ganesan S, Sharma T, Raman R. The prevalence and risk factors for cataract in rural and urban India. Indian journal of ophthalmology. 2019 Apr:67(4):477-483. doi: 10.4103/ijo.IJO_1127_17. Epub [PubMed PMID: 30900578]
Tegegn MT, Assaye AK, Belete GT, Munaw MB. Visually significant cataract and associated factors among older people attending a community ophthalmic service in central Gondar Zone, Northwest Ethiopia: a cross-sectional study. The Journal of international medical research. 2022 Jun:50(6):3000605221104761. doi: 10.1177/03000605221104761. Epub [PubMed PMID: 35698450]
Level 2 (mid-level) evidenceYüksel N, Yılmaz Tuğan B. Pseudoexfoliation Glaucoma: Clinical Presentation and Therapeutic Options. Turkish journal of ophthalmology. 2023 Aug 19:53(4):247-256. doi: 10.4274/tjo.galenos.2023.76300. Epub [PubMed PMID: 37602651]
Hsu E, Nguyen A, Sanjiv N, Desai M, Blaney D, Rowe SG. A case of accommodation-induced lens subluxation with iris displacement causing intermittent angle closure. American journal of ophthalmology case reports. 2024 Jun:34():102014. doi: 10.1016/j.ajoc.2024.102014. Epub 2024 Feb 13 [PubMed PMID: 38389701]
Level 3 (low-level) evidenceFLOCKS M, LITTWIN CS, ZIMMERMAN LE. Phacolytic glaucoma; a clinicopathologic study of one hundred thirty-eight cases of glaucoma associated with hypermature cataract. A.M.A. archives of ophthalmology. 1955 Jul:54(1):37-45 [PubMed PMID: 14375459]
Level 3 (low-level) evidenceEpstein DL, Jedziniak JA, Grant WM. Obstruction of aqueous outflow by lens particles and by heavy-molecular-weight soluble lens proteins. Investigative ophthalmology & visual science. 1978 Mar:17(3):272-7 [PubMed PMID: 627464]
Epstein DL, Jedziniak JA, Grant WM. Identification of heavy-molecular-weight soluble protein in aqueous humor in human phacolytic glaucoma. Investigative ophthalmology & visual science. 1978 May:17(5):398-402 [PubMed PMID: 640786]
Thach AB, Marak GE Jr, McLean IW, Green WR. Phacoanaphylactic endophthalmitis: a clinicopathologic review. International ophthalmology. 1991 Jul:15(4):271-9 [PubMed PMID: 1917323]
Level 2 (mid-level) evidenceEllant JP, Obstbaum SA. Lens-induced glaucoma. Documenta ophthalmologica. Advances in ophthalmology. 1992:81(3):317-38 [PubMed PMID: 1483374]
Level 3 (low-level) evidencePerlman EM, Albert DM. Clinically unsuspected phacoanaphylaxis after ocular trauma. Archives of ophthalmology (Chicago, Ill. : 1960). 1977 Feb:95(2):244-6 [PubMed PMID: 836209]
Level 3 (low-level) evidenceTan RKY, Ng GY, Tun TA, Braeu FA, Nongpiur ME, Aung T, Girard MJA. Iris Morphological and Biomechanical Factors Influencing Angle Closure During Pupil Dilation. Investigative ophthalmology & visual science. 2024 Sep 3:65(11):7. doi: 10.1167/iovs.65.11.7. Epub [PubMed PMID: 39230993]
Papaconstantinou D, Georgalas I, Kourtis N, Krassas A, Diagourtas A, Koutsandrea C, Georgopoulos G. Lens-induced glaucoma in the elderly. Clinical interventions in aging. 2009:4():331-6 [PubMed PMID: 19696897]
Chan AX, Yeh K, Bakhoum M, Do JL. Pseudophakic glaucoma and angle closure in a patient with an anterior chamber intraocular lens. American journal of ophthalmology case reports. 2020 Dec:20():100877. doi: 10.1016/j.ajoc.2020.100877. Epub 2020 Aug 16 [PubMed PMID: 32875158]
Level 3 (low-level) evidenceMacovei ML, Canache M, Neagoe BM. Phacolytic glaucoma - case report. Romanian journal of ophthalmology. 2021 Apr-Jun:65(2):191-195. doi: 10.22336/rjo.2021.38. Epub [PubMed PMID: 34179587]
Level 3 (low-level) evidenceShah SS, Gurnani B. Lens-Induced Glaucoma. StatPearls. 2026 Jan:(): [PubMed PMID: 34662038]
Yoo WS, Kim BJ, Chung IY, Seo SW, Yoo JM, Kim SJ. A case of phacolytic glaucoma with anterior lens capsule disruption identified by scanning electron microscopy. BMC ophthalmology. 2014 Nov 19:14():133. doi: 10.1186/1471-2415-14-133. Epub 2014 Nov 19 [PubMed PMID: 25407294]
Level 3 (low-level) evidenceRosenbaum JT, Samples JR, Seymour B, Langlois L, David L. Chemotactic activity of lens proteins and the pathogenesis of phacolytic glaucoma. Archives of ophthalmology (Chicago, Ill. : 1960). 1987 Nov:105(11):1582-4 [PubMed PMID: 3675292]
Mavrakanas N, Axmann S, Issum CV, Schutz JS, Shaarawy T. Phacolytic glaucoma: are there 2 forms? Journal of glaucoma. 2012 Apr-May:21(4):248-9. doi: 10.1097/IJG.0b013e31820d7d2e. Epub [PubMed PMID: 21423037]
Level 3 (low-level) evidenceKase S, Chin S, Hamanaka T, Shinmei Y, Ohguchi T, Kijima R, Matsuda A, Ishida S. Histological Findings in the Trabecular Meshwork of a Patient with Atopic Glaucoma. The open ophthalmology journal. 2017:11():103-106. doi: 10.2174/1874364101711010103. Epub 2017 May 29 [PubMed PMID: 28660005]
Goit RK. Exploring Glaucoma: From Pathogenesis to Emerging Diagnostic and Management Strategies. Journal of ophthalmology. 2025:2025():8476785. doi: 10.1155/joph/8476785. Epub 2025 Jul 31 [PubMed PMID: 40964175]
Abu-Hassan DW, Acott TS, Kelley MJ. The Trabecular Meshwork: A Basic Review of Form and Function. Journal of ocular biology. 2014 May:2(1):. pii: http://fulltextarticles.avensonline.org/JOCB-2334-2838-02-0017.html. Epub [PubMed PMID: 25356439]
Ramya MG, Lokanathan LM, Shekhar M, Murali N, Waghamare SR. Intraocular lens scaffolding technique in hypermature/Morgagnian cataract in manual small-incision cataract surgery. Journal of cataract and refractive surgery. 2023 Apr 1:49(4):405-408. doi: 10.1097/j.jcrs.0000000000001119. Epub [PubMed PMID: 36729596]
De Andres J, Hayek S, Perruchoud C, Lawrence MM, Reina MA, De Andres-Serrano C, Rubio-Haro R, Hunt M, Yaksh TL. Intrathecal Drug Delivery: Advances and Applications in the Management of Chronic Pain Patient. Frontiers in pain research (Lausanne, Switzerland). 2022:3():900566. doi: 10.3389/fpain.2022.900566. Epub 2022 Jun 16 [PubMed PMID: 35782225]
Level 3 (low-level) evidenceMcKee CT, Wood JA, Shah NM, Fischer ME, Reilly CM, Murphy CJ, Russell P. The effect of biophysical attributes of the ocular trabecular meshwork associated with glaucoma on the cell response to therapeutic agents. Biomaterials. 2011 Mar:32(9):2417-23. doi: 10.1016/j.biomaterials.2010.11.071. Epub 2011 Jan 8 [PubMed PMID: 21220171]
Chandrashekharan S, Chakrabarty S, Tanwar M, Madhuvarasu B, Uduman MS, Ramakrishnan R. Outcomes and favourable prognostic factors in patients of phacomorphic and phacolytic glaucoma managed by manual small-incision cataract surgery: A retrospective study. Indian journal of ophthalmology. 2022 Apr:70(4):1216-1221. doi: 10.4103/ijo.IJO_2371_21. Epub [PubMed PMID: 35326019]
Level 2 (mid-level) evidenceSoleimani M, Cheraqpour K, Salari F, Fadakar K, Habeel S, Baharnoori SM, Banz S, Tabatabaei SA, Woreta FA, Djalilian AR. All about traumatic cataracts: narrative review. Journal of cataract and refractive surgery. 2024 Jul 1:50(7):760-766. doi: 10.1097/j.jcrs.0000000000001424. Epub [PubMed PMID: 38350230]
Level 3 (low-level) evidenceDíez-Ajenjo MA, Luque-Cobija MJ, Peris-Martínez C, Ortí-Navarro S, García-Domene MC. Refractive changes and visual quality in patients with corneal edema after cataract surgery. BMC ophthalmology. 2022 Jun 2:22(1):242. doi: 10.1186/s12886-022-02452-5. Epub 2022 Jun 2 [PubMed PMID: 35655163]
Level 2 (mid-level) evidencePeracha-Riyaz MH, Peracha ZH, Spaulding J, Baciu P, Ahmed S, Imami NR, Darnley-Fisch D, Desai U. First Described Case of Anterior and Posterior Segment Crystals in Phacolytic Glaucoma. Journal of glaucoma. 2017 May:26(5):e171-e173. doi: 10.1097/IJG.0000000000000642. Epub [PubMed PMID: 28234682]
Level 3 (low-level) evidenceVu AT, Bui VA, Vu HL, Quyet D, Thai TV, Nga VT, Dinh TC, Bac ND. Evaluation of Anterior Chamber Depth and Anterior Chamber Angle Changing After Phacoemulsification in the Primary Angle Close Suspect Eyes. Open access Macedonian journal of medical sciences. 2019 Dec 30:7(24):4297-4300. doi: 10.3889/oamjms.2019.378. Epub 2019 Dec 20 [PubMed PMID: 32215081]
Filipe JC, Palmares J, Delgado L, Lopes JM, Borges J, Castro-Correia J. Phacolytic glaucoma and lens-induced uveitis. International ophthalmology. 1993 Oct:17(5):289-93 [PubMed PMID: 8132409]
Sidhu T, Desai A, Gagrani M, Dada T. Phacomorphic glaucoma in a high myope with phakic intraocular lens. BMJ case reports. 2019 Feb 25:12(2):. doi: 10.1136/bcr-2018-227096. Epub 2019 Feb 25 [PubMed PMID: 30804159]
Level 3 (low-level) evidenceRazeghinejad MR. Gonioscopic features in patients with acute and chronic angle-closure glaucoma. Iranian journal of medical sciences. 2011 Mar:36(1):7-13 [PubMed PMID: 23365471]
Ng JK, Lau O. Traumatic Glaucoma. StatPearls. 2025 Jan:(): [PubMed PMID: 36251842]
Guan JY, Ma YC, Zhu YT, Xie LL, Aizezi M, Zhuo YH, Wumaier A. Lens nucleus dislocation in hypermature cataract: Case report and literature review. Medicine. 2022 Sep 2:101(35):e30428. doi: 10.1097/MD.0000000000030428. Epub [PubMed PMID: 36107580]
Level 3 (low-level) evidenceFarooq S, Khan NA, Meena R, Kochar A. Phacoemulsification in phacomorphic angle closure: Our experience. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2023 Apr-Jun:37(2):90-93. doi: 10.4103/sjopt.sjopt_38_22. Epub 2023 Jan 16 [PubMed PMID: 37492207]
Zhumageldiyeva FE, Dzhumataeva Z, Dauletbekov D, Suleymenov M, Utelbayeva Z, Meyermanova Z, Teleuova T. A-Scan Parameters and the Risk of Phacomorphic Glaucoma in the Kazakh Population. Medicina (Kaunas, Lithuania). 2022 Oct 28:58(11):. doi: 10.3390/medicina58111544. Epub 2022 Oct 28 [PubMed PMID: 36363501]
Karmiris E, Papakonstantinou E, Tsiripidis K, Stavrakas P, Giannakis I, Chalkiadaki E. Atypical phacolytic glaucoma diagnosed by biometry and anterior segment optical coherence tomography (OCT) in a patient with CMV anterior uveitis. European journal of ophthalmology. 2024 Jul:34(4):NP29-NP32. doi: 10.1177/11206721241246816. Epub 2024 Apr 11 [PubMed PMID: 38602030]
Gurnani B, Kaur K. Comment on: Surgeon adoption of immediate sequential bilateral cataract surgery in the United States from 2018 to 2022. Journal of cataract and refractive surgery. 2025 Aug 1:51(8):747. doi: 10.1097/j.jcrs.0000000000001704. Epub [PubMed PMID: 41060140]
Level 3 (low-level) evidenceBartlett KJ, Vo AP, Rueckert J, Wojewoda C, Steckel EH, Stinnett-Donnelly J, Repp AB. Promoting appropriate utilisation of laboratory tests for inflammation at an academic medical centre. BMJ open quality. 2020 Feb:9(1):. doi: 10.1136/bmjoq-2019-000788. Epub [PubMed PMID: 32098777]
Level 2 (mid-level) evidenceYang WH, Xu YW, Sun XH, Expert Workgroup of Guidelines for Glaucoma Imaging Classification, Annotation, and Quality Control for Artificial Intelligence Applications. Guidelines for glaucoma imaging classification, annotation, and quality control for artificial intelligence applications. International journal of ophthalmology. 2025:18(7):1181-1196. doi: 10.18240/ijo.2025.07.01. Epub 2025 Jul 18 [PubMed PMID: 40688788]
Level 2 (mid-level) evidenceBojikian KD, Leveque TK, McEvoy A, Hopkin B, Popovici N, Hopkin H, Howell G, Kim ME, Yu JT, Chen A, Ding L, Taravati P, Tarczy-Hornoch K, Feng S. Assessment of Emergency Department Intraocular Pressure and Visual Acuity Assessment as a Screening Exam. Clinical ophthalmology (Auckland, N.Z.). 2025:19():683-690. doi: 10.2147/OPTH.S511327. Epub 2025 Feb 25 [PubMed PMID: 40026816]
Tuteja S, Zeppieri M, Chawla H. Pseudoexfoliation Syndrome and Glaucoma. StatPearls. 2025 Jan:(): [PubMed PMID: 34662036]
Jiang Y, Chang DS, Foster PJ, He M, Huang S, Aung T, Friedman DS. Immediate changes in intraocular pressure after laser peripheral iridotomy in primary angle-closure suspects. Ophthalmology. 2012 Feb:119(2):283-8. doi: 10.1016/j.ophtha.2011.08.014. Epub 2011 Oct 29 [PubMed PMID: 22036632]
Ziakas NG, Boboridis K, Nakos E, Mikropoulos D, Margaritis V, Konstas AG. Does the use of trypan blue during phacoemulsification affect the intraocular pressure? Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2009 Jun:44(3):293-6. doi: 10.3129/i09-055. Epub [PubMed PMID: 19491985]
Rajkumari V, Singh Kaminibabu K, Bhabanisana RD, Victor R. Manual Small Incision Cataract Surgery in Phacomorphic Glaucoma: Surgical Technique and Outcome in North-eastern India. Journal of current glaucoma practice. 2013 May-Aug:7(2):43-8. doi: 10.5005/jp-journals-10008-1136. Epub 2013 May 9 [PubMed PMID: 26997781]
Pleyer U, Ursell PG, Rama P. Intraocular pressure effects of common topical steroids for post-cataract inflammation: are they all the same? Ophthalmology and therapy. 2013 Dec:2(2):55-72. doi: 10.1007/s40123-013-0020-5. Epub 2013 Sep 17 [PubMed PMID: 25135807]
Balu GS, Gupta S, Ravilla RD, Ravilla TD, Mertens H, Webers C, Vasudeva Rao S, van Merode F. Impact of practicing internal benchmarking on continuous improvement of cataract surgery outcomes: a retrospective observational study at Aravind Eye Hospitals, India. BMJ open. 2023 Jun 22:13(6):e071860. doi: 10.1136/bmjopen-2023-071860. Epub 2023 Jun 22 [PubMed PMID: 37349104]
Level 2 (mid-level) evidenceThapa SS, Berg RV, Khanal S, Paudyal I, Pandey P, Maharjan N, Twyana SN, Paudyal G, Gurung R, Ruit S, Rens GH. Prevalence of visual impairment, cataract surgery and awareness of cataract and glaucoma in Bhaktapur district of Nepal: the Bhaktapur Glaucoma Study. BMC ophthalmology. 2011 Jan 21:11():2. doi: 10.1186/1471-2415-11-2. Epub 2011 Jan 21 [PubMed PMID: 21255382]
Liang Z, Li H, Hou X, Yang K, Lv K, Ma Y, Lu Y, Wu K, Wu H. Prospective study on the role of preoperative mannitol in capsulorhexis and reducing intraoperative complications in primary angle-closure disease surgery. The Journal of international medical research. 2025 Jan:53(1):3000605241310106. doi: 10.1177/03000605241310106. Epub [PubMed PMID: 39817367]
Gayton JL. A clinical comparison of two different prednisolone acetate formulations in patients undergoing cataract surgery. Current medical research and opinion. 2005 Aug:21(8):1291-5 [PubMed PMID: 16083539]
Level 3 (low-level) evidenceRothman AL, Persad LS, Paranjpe VR, Chang TC, Lum F, Vanner EA, O'Brien RC. Intraocular Pressure after Phacoemulsification with Retained Lens Fragments in the IRIS® Registry (Intelligent Research in Sight). Ophthalmology. 2025 Oct 14:():. pii: S0161-6420(25)00643-8. doi: 10.1016/j.ophtha.2025.10.008. Epub 2025 Oct 14 [PubMed PMID: 41101529]
Evereklioglu C, Karacan Erşekerci T, Sönmez HK, Sener H, Gulmez Sevim D, Polat OA, Arda H, Horozoglu F. The Frequency of Intraocular Pressure Elevation, Incidence of Secondary Glaucoma, and Surgical Treatment With Postoperative Complications in Pediatric and Adult Patients With Uveitis. Cureus. 2024 Mar:16(3):e55734. doi: 10.7759/cureus.55734. Epub 2024 Mar 7 [PubMed PMID: 38586631]
Nche EN, Amer R. Lens-induced uveitis: an update. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2020 Jul:258(7):1359-1365. doi: 10.1007/s00417-019-04598-3. Epub 2020 Jan 6 [PubMed PMID: 31907641]
Luitel P, Pandey M, Karn RR, Dev MK, Rajbanshi L, Sitoula RP. Visual and Surgical Outcomes of Outreach Cataract Surgeries in Ilam District of Nepal: An Observational Study. JNMA; journal of the Nepal Medical Association. 2024 Nov:62(279):739-743. doi: 10.31729/jnma.8798. Epub 2024 Nov 30 [PubMed PMID: 40656808]
Level 2 (mid-level) evidenceWang B, Zheng Y, Han X, Kong L, Xiao G, Xiao Z, Chen S. A systematic literature review on integrating AI-powered smart glasses into digital health management for proactive healthcare solutions. NPJ digital medicine. 2025 Jul 5:8(1):410. doi: 10.1038/s41746-025-01715-x. Epub 2025 Jul 5 [PubMed PMID: 40617964]
Level 1 (high-level) evidenceMachado S, Paes F, Ferreira-Garcia R, Gonçalves LL, Carta MG, Appolinario JC, Nardi AE. Virtual Reality: Challenges and Perspectives in Mental Health. Alpha psychiatry. 2025 Oct:26(5):47536. doi: 10.31083/AP47536. Epub 2025 Oct 21 [PubMed PMID: 41209496]
Level 3 (low-level) evidenceMehari ZA, Zewedu RT, Gulilat FB. Barriers to cataract surgical uptake in central ethiopia. Middle East African journal of ophthalmology. 2013 Jul-Sep:20(3):229-33. doi: 10.4103/0974-9233.114798. Epub [PubMed PMID: 24014987]
See JL, Aquino MC, Aduan J, Chew PT. Management of angle closure glaucoma. Indian journal of ophthalmology. 2011 Jan:59 Suppl(Suppl1):S82-7. doi: 10.4103/0301-4738.73690. Epub [PubMed PMID: 21150039]
Aftab OM, Khan H, Bargoud A, Khouri AS. Are Alpha-2 Adrenergic Agonists Being Used in Infants? Journal of ocular pharmacology and therapeutics : the official journal of the Association for Ocular Pharmacology and Therapeutics. 2025 Mar:41(2):75-78. doi: 10.1089/jop.2024.0095. Epub 2024 Aug 22 [PubMed PMID: 39172558]
Feroze KB, Zeppieri M, Khazaeni L. Steroid-Induced Glaucoma. StatPearls. 2025 Jan:(): [PubMed PMID: 28613653]
Ah-Kee EY, Egong E, Shafi A, Lim LT, Yim JL. A review of drug-induced acute angle closure glaucoma for non-ophthalmologists. Qatar medical journal. 2015:2015(1):6. doi: 10.5339/qmj.2015.6. Epub 2015 May 10 [PubMed PMID: 26535174]
Helayel HB, Alyahya AA, Al Owaifeer AM, Khan AM, Al Zahrani AT, Badawi AH, Khandekar R, Al-Swailem SA. Risk factors, complications, and outcomes of phacoemulsification cataract surgery complicated by retained lens fragments in Asian eyes: A 10-year retrospective study. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2022 Apr-Jun:36(2):171-176. doi: 10.4103/sjopt.sjopt_122_22. Epub 2022 Aug 29 [PubMed PMID: 36211313]
Level 2 (mid-level) evidenceCionni RJ, Osher RH. Management of profound zonular dialysis or weakness with a new endocapsular ring designed for scleral fixation. Journal of cataract and refractive surgery. 1998 Oct:24(10):1299-306 [PubMed PMID: 9795841]
Huang X, Saki F, Wang M, Elze T, Boland MV, Pasquale LR, Johnson CA, Yousefi S. An Objective and Easy-to-Use Glaucoma Functional Severity Staging System Based on Artificial Intelligence. Journal of glaucoma. 2022 Aug 1:31(8):626-633. doi: 10.1097/IJG.0000000000002059. Epub 2022 Jun 3 [PubMed PMID: 35658070]
Ong AY, Ng SM, Vedula SS, Friedman DS. Lens extraction for chronic angle-closure glaucoma. The Cochrane database of systematic reviews. 2021 Mar 24:3(3):CD005555. doi: 10.1002/14651858.CD005555.pub3. Epub 2021 Mar 24 [PubMed PMID: 33759192]
Level 1 (high-level) evidenceLee CK, Lee NE, Hong S, Kang E, Rho SS, Seong GJ, Hong YJ, Kim CY. Risk Factors of Disease Progression After Cataract Surgery in Chronic Angle-closure Glaucoma Patients. Journal of glaucoma. 2016 Apr:25(4):e372-6. doi: 10.1097/IJG.0000000000000350. Epub [PubMed PMID: 26550967]
Cabuk KS, Cekic O. Intraocular Pressure Change and Sustained Intraocular Pressure Elevation After Pars Plana Vitrectomy. Beyoglu eye journal. 2021:6(2):96-101. doi: 10.14744/bej.2021.92408. Epub 2021 Jun 8 [PubMed PMID: 35005501]
Ostovic M, Hofmann C, Klaproth OK, Kohnen T. Corneal decompensation and angle-closure glaucoma after upside-down implantation of an angle-supported anterior chamber phakic intraocular lens. Journal of cataract and refractive surgery. 2013 May:39(5):806-9. doi: 10.1016/j.jcrs.2013.02.005. Epub 2013 Mar 26 [PubMed PMID: 23540572]
Supakontanasan W, Suwan Y, Nilphatanakorn S, Teekhasaenee C, Tantraworasin A, Petpiroon P. Twenty-Four-Hour Intraocular Pressure in Chronic Primary Angle-Closure Disease. Journal of glaucoma. 2023 Oct 1:32(10):854-859. doi: 10.1097/IJG.0000000000002280. Epub 2023 Aug 1 [PubMed PMID: 37566875]
Gurnani B, Kaur K. Post-market surveillance of ophthalmic implants: role of real-world evidence. Expert review of medical devices. 2025 Dec:22(12):1303-1308. doi: 10.1080/17434440.2025.2579578. Epub 2025 Oct 24 [PubMed PMID: 41123186]
Kaur K, Zeppieri M, Gurnani B. Primary Congenital Glaucoma. StatPearls. 2026 Jan:(): [PubMed PMID: 34662067]
Gessesse GW, Damji KF. Advanced glaucoma: management pearls. Middle East African journal of ophthalmology. 2013 Apr-Jun:20(2):131-41. doi: 10.4103/0974-9233.110610. Epub [PubMed PMID: 23741132]
Kyari F. Managing cataract surgery in patients with glaucoma. Community eye health. 2019:31(104):88-90 [PubMed PMID: 31086439]
Kodali S, Khan B, Zong AM, Moon JY, Shrivastava A, Daily JP, Gibralter RP. Prognostic indicators of corneal ulcer clinical outcomes at a tertiary care center in the Bronx, New York. Journal of ophthalmic inflammation and infection. 2024 Apr 24:14(1):18. doi: 10.1186/s12348-024-00392-3. Epub 2024 Apr 24 [PubMed PMID: 38656674]
Level 2 (mid-level) evidenceLing JD, Bell NP. Role of Cataract Surgery in the Management of Glaucoma. International ophthalmology clinics. 2018 Summer:58(3):87-100. doi: 10.1097/IIO.0000000000000234. Epub [PubMed PMID: 29870412]
Gurnani B, Kaur K. Corneal cross-linking for keratoconus: a global economic and clinical perspective. Journal of medical economics. 2025 Dec:28(1):2119-2124. doi: 10.1080/13696998.2025.2587416. Epub 2025 Nov 30 [PubMed PMID: 41320236]
Level 3 (low-level) evidenceMurugan SB, Sunil Kumar, Gurnani B, Kaur K. Assessment of Subjective Visual Experiences During Intraocular Surgery and Intravitreal Injection Among Uveitis Patients at a Tertiary Eye Hospital: A Cross-Sectional Observational Study. Ophthalmology and therapy. 2026 Jan:15(1):173-191. doi: 10.1007/s40123-025-01264-2. Epub 2025 Nov 6 [PubMed PMID: 41196490]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert review of medical devices. 2025 Dec:22(12):1287-1292. doi: 10.1080/17434440.2025.2582616. Epub 2025 Nov 2 [PubMed PMID: 41147335]
Nishant P, Gurnani B, Singh P, Sinha S, Kaur K, Kumar A, Sinha RK. Current concepts and recent trends in endothelial keratoplasty. World journal of transplantation. 2025 Jun 18:15(2):102507. doi: 10.5500/wjt.v15.i2.102507. Epub [PubMed PMID: 40535500]
Laroche D, Madu CT. Preventing Blindness with Early Cataract Surgery and Micro-Invasive Glaucoma Surgery in Patients Over 50: Guidance for Patients, Physicians and World Governments in Dealing with Glaucoma. Clinical ophthalmology (Auckland, N.Z.). 2023:17():2929-2938. doi: 10.2147/OPTH.S422415. Epub 2023 Oct 4 [PubMed PMID: 37814637]
Tripathi M, Markan A, Gurnani B. Cytomegalovirus Corneal Endotheliitis. StatPearls. 2026 Jan:(): [PubMed PMID: 35201702]
Kumar A, Sahu V, Misra S, Rathore V, Gurnani B, Kaur K. Changes in various ocular parameters of patients undergoing hemodialysis. European journal of ophthalmology. 2025 Nov:35(6):2235-2243. doi: 10.1177/11206721251349681. Epub 2025 Jun 18 [PubMed PMID: 40530962]
Davis BP, Mitchell SA, Weston J, Dragon C, Luthra M, Kim J, Stoddard H, Ander D. Situation, Background, Assessment, Recommendation (SBAR) Education for Health Care Students: Assessment of a Training Program. MedEdPORTAL : the journal of teaching and learning resources. 2023:19():11293. doi: 10.15766/mep_2374-8265.11293. Epub 2023 Jan 3 [PubMed PMID: 36655140]
Varkey B. Principles of Clinical Ethics and Their Application to Practice. Medical principles and practice : international journal of the Kuwait University, Health Science Centre. 2021:30(1):17-28. doi: 10.1159/000509119. Epub 2020 Jun 4 [PubMed PMID: 32498071]