Introduction
Bielschowsky coined the term dissociated vertical deviation (DVD). DVD has also been referred to as “alternating hyperphoria,” “double hyperphoria,” “occlusion hyperphoria,” “occlusion hypertropia,” “periodic vertical deviation,” “alternating sursum-duction,” “double dissociated hyperphoria,” “dissociated hypertropia,” and “dissociated vertical divergence.” DVD is classically defined as vertical drifting of one eye when the patient fixates at a target with the other eye.[1] The deviation is often bilateral and asymmetrical.[2]
This usually manifests when there is a mechanical, optical, or sensory interruption of the binocular visual input. The DVD syndrome encompasses 3 components: hyperdeviation, abduction, and excyclotorsion. The deviation may manifest spontaneously when the patient is fatigued, daydreaming, or latent, manifesting only on cover-uncover or alternate cover tests. An interesting finding is that as the uncovered/deviated eye shifts downwards to take up the fixation, the eye fixing earlier does not show a corresponding downward shift, thus violating the Herring law.[3]
Duane Retraction Syndrome (DRS) is a rare, congenital ocular motility disorder characterized by limitation or absence of horizontal eye movements, globe retraction, and palpebral fissure narrowing on attempted adduction. First described by Alexander Duane in 1905, this condition represents approximately 1% to 4% of all cases of strabismus. The pathophysiology is now understood to involve a congenital cranial dysinnervation disorder (CCDD) in which aberrant innervation of the lateral rectus muscle by branches of the oculomotor nerve leads to paradoxical co-contraction of horizontal recti. While classically unilateral, DRS may be bilateral in 10% to 20% of cases and is more commonly observed in females, with a predilection for the left eye.[4]
The etiology is linked to developmental anomalies of the abducens nerve (cranial nerve VI) or its nucleus, resulting in absent or hypoplastic innervation and compensatory miswiring from the oculomotor nerve. This neurogenic origin is supported by magnetic resonance imaging (MRI) studies demonstrating absent abducens nerve and electromyography findings of simultaneous lateral and medial rectus contraction during attempted adduction. In some cases, DRS is associated with systemic anomalies such as Goldenhar syndrome, Klippel–Feil anomaly, or other congenital malformations, reinforcing the notion of a broader embryologic insult affecting cranial nerve development.[5]
Clinically, DRS is classified into three primary types according to the Huber classification (1974):
- Type I: Marked limitation or absence of abduction, with relatively normal adduction and globe retraction on adduction
- Type II: Limitation or absence of adduction with relatively normal abduction
- Type III: Limitation of both abduction and adduction, often with significant globe retraction [6]
Patients may also exhibit upshoots or downshoots on adduction due to leash effects or mechanical factors within the extraocular muscle pulleys. Abnormal head posture is common as patients adopt compensatory face turns to maintain binocular single vision in primary gaze. The severity of motility restriction and retraction varies widely, influencing functional and cosmetic concerns. Epidemiologically, DRS accounts for a small fraction of strabismus cases worldwide but carries substantial clinical importance due to its distinct presentation, surgical challenges, and potential associations with systemic disorders. Population-based studies indicate prevalence rates ranging from 0.1 to 0.7 per 1000 live births, though true incidence may be underestimated due to underdiagnosis in mild cases. Awareness among pediatricians, ophthalmologists, and orthoptists is critical for early recognition and evaluation.[7]
From a diagnostic standpoint, DRS is primarily a clinical diagnosis supported by a detailed ocular motility examination. Key signs include narrowing of the palpebral fissure on adduction, globe retraction, and variable upshoots or downshoots. Forced duction testing may reveal mechanical restrictions, but the hallmark finding is paradoxical co-contraction of horizontal recti, confirmed by electromyography. Imaging with high-resolution orbital MRI or diffusion tensor imaging can delineate the absence of the abducens nerve, providing objective confirmation and aiding in surgical planning. Assessment should also include evaluation for associated systemic anomalies, as up to 30% of patients may have other congenital malformations.[8]
Management of DRS is individualized and guided by the severity of motility limitation, abnormal head posture, and patient symptoms. Mild cases with good primary gaze alignment may require only observation and periodic follow-up. Surgical intervention is indicated for significant misalignment in primary gaze, large abnormal head posture, or cosmetically disturbing globe retraction and upshoots/downshoots. Procedures may include recession of the medial rectus, lateral rectus, or a combination, and vertical rectus transpositions in select cases. The surgical approach is often more complex than other forms of strabismus due to the paradoxical innervation and risk of exacerbating retraction. Overcorrection, induced vertical deviations, and persistent limitation are recognized challenges.[9]
DRS is nonprogressive, but long-term follow-up is essential to monitor ocular alignment, binocular function, and amblyopia risk, particularly in children. Amblyopia occurs in up to 10% of cases, necessitating prompt detection and treatment. Orthoptic therapy supports maintaining binocular vision and managing mild head postures, although it does not correct the underlying innervational anomaly. Recent advances in understanding DRS pathogenesis have emerged from genetic and neuroimaging studies. Mutations in genes such as CHN1 (encoding alpha2-chimaerin) have been identified in familial cases, implicating axon guidance defects in cranial nerve development. These findings place DRS within the broader category of CCDDs, alongside Möbius syndrome and congenital fibrosis of the extraocular muscles. This reclassification has shifted the focus from purely mechanical explanations to neurodevelopmental mechanisms, fostering novel research avenues.[10]
The psychosocial impact of DRS should not be underestimated. Visible eye movement anomalies and abnormal head posture can affect self-esteem, social interactions, and quality of life, particularly in adolescents. Counseling, patient education, and appropriate referral for psychological support may be beneficial in selected cases. In pediatric patients, parental reassurance and guidance are critical to alleviate anxiety and ensure adherence to follow-up schedules.[11]
Interprofessional collaboration is central to optimal DRS management. Pediatric ophthalmologists, orthoptists, neurologists, radiologists, and genetic counselors contribute to comprehensive evaluation and care. For example, neurologists may assess for associated cranial nerve or central nervous system anomalies, while genetic counselors provide insight into inheritance patterns and recurrence risks. Radiologists skilled in high-resolution orbital imaging are important in confirming diagnosis and guiding surgical strategy. Orthoptists assist with functional assessment, prism adaptation, and postoperative rehabilitation, enhancing overall outcomes.
In conclusion, DRS represents a distinct, nonprogressive congenital ocular motility disorder with complex neurogenic and mechanical features. Advances in neuroimaging and genetics have enriched our understanding of its pathophysiology, while surgical and nonsurgical management strategies continue to evolve. Early recognition, thorough evaluation for systemic associations, individualized treatment planning, and long-term multidisciplinary follow-up are key pillars in optimizing patient functional and cosmetic outcomes. This educational activity equips learners with an evidence-based, clinically relevant framework for diagnosing and managing DRS, integrating current guidelines, expert consensus, and interprofessional care principles to improve patient-centered outcomes.[12]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of dissociated vertical deviation is not known. A few of the important points to consider include:
- An elastic preponderance of the elevator or depressor muscles, which imbalances the amount of innervation from each vestibular organ
- Abnormalities of the visual pathway
- Imbalance of binocular stimulation [3]
DVD is a unique ocular motility disorder, typically associated with early-onset strabismus, particularly infantile esotropia (see Tables 1 and 2). The etiology remains multifactorial and not fully understood, but several mechanisms have been proposed:
- Sensory theory (binocular maldevelopment):
- DVD is thought to arise from disrupting normal binocular development during infancy.
- Early loss of fusion (due to strabismus, anisometropia, or amblyopia) leads to defective cortical binocular interactions.
- This results in a dissociated response where one eye drifts upward when not fixating, independent of the Hering law.[13]
- Motor theory (vestibular imbalance):
- An imbalance in vertical vergence or vestibular pathways has been implicated.
- Bielschowsky suggested that latent nystagmus and abnormal vertical vergence mechanisms are linked.[14]
- Abnormal vertical vergence pathways:
- Some evidence suggests that DVD may represent an abnormal adaptive mechanism to suppress diplopia and confusion by elevating the nonfixing eye.
- This is thought to involve supranuclear control pathways for vertical vergence.[15]
- Neurophysiological basis:
- DVD is considered part of humans' “dorsal light reflex” abnormality, resembling compensatory eye movements in animals with binocular disruption.
- Functional MRI and electrophysiology studies support the role of subcortical (brainstem/vestibular) mechanisms.[12]
- Association with strabismus and amblyopia:
- Most cases occur in children with infantile esotropia, amblyopia, or other early binocular sensory deficits.
- DVD is rare in patients with normal binocular development.[16]
Table 1. Theories of DVD Etiology
|
Theory |
Proposed Mechanism |
Supporting Evidence |
|
Sensory Theory |
Early disruption of binocular fusion → abnormal cortical binocular interaction |
Common in infantile esotropia and amblyopia |
|
Motor Theory (Vestibular Imbalance) |
Defective vestibular/vertical vergence control → upward drift of nonfixing eye |
Linked with latent nystagmus |
|
Abnormal vertical vergence |
Supranuclear abnormality in vertical vergence pathways |
Explains dissociated nature (not obeying the Hering law) |
|
Dorsal Light Reflex Abnormality |
The primitive reflex is triggered due to abnormal binocular input |
Observed in primate models with binocular disruption |
Table 2. Clinical Associations of DVD
|
Associated Condition |
Relevance |
|
Infantile esotropia |
Most common association: The majority of DVD cases occur in this group |
|
Amblyopia |
Eyes with poorer vision are more likely to show greater DVD |
|
Latent nystagmus |
Frequently coexists; supports vestibular theory |
|
Intermittent strabismus |
Seen in children with early fusion disruption |
|
Other ocular motor anomalies |
Dissociated horizontal deviation, dissociated torsional deviation |
The etiology of DVD is multifactorial, with early sensory disruption of binocular vision considered the most widely accepted mechanism, possibly modulated by vestibular/vertical vergence pathway abnormalities. Associations with infantile esotropia, amblyopia, and latent nystagmus provide strong clinical support for these theories.[17]
Epidemiology
In the United States, about 3% to 5% of children have strabismus. The prevalence of DVD among the diagnosed cases of strabismus was estimated at 1.9%.[18] was found to be more frequently associated with sensory esotropia than exotropia.[19] Kutluk et al reported a DVD prevalence of 12.5% in patients with sensory hypertropia (see Image. Exotropia (20 degrees) and Hypertropia (10 degrees), Left Eye).[19] Cherfan et al reported that the common strabismus subtypes associated with DVD were congenital esotropia (53%), esotropia with a developmental deficit (25%), and accommodative esotropia (3.4%) in declining order.[18]
Kutluk et al reported a DVD prevalence of 12.5% in patients with sensory hypertropia.[19] Cherfan et al reported that the common strabismus subtypes associated with DVD were congenital esotropia (53%), esotropia with a developmental deficit (25%), and accommodative esotropia (3.4%) in declining order.[18] Dissociated vertical deviation (DVD) is an uncommon but clinically significant form of strabismus, typically manifesting in early childhood; this is strongly associated with infantile esotropia and other early-onset strabismic syndromes.
Frequency and Prevalence
- United States and Europe: DVD is reported in 50% to 90% of patients with infantile esotropia and in 60% to 80% of those with a history of infantile strabismus surgery. In the general population, the estimated prevalence is 1% to 1%, though precise figures are limited due to underdiagnosis in mild or latent cases.
- Worldwide: Studies from Asia, the Middle East, and South America suggest similar associations, though prevalence data vary widely, reflecting differences in study methodology and access to pediatric ophthalmology services. DVD is frequently reported in tertiary care centers as part of complex strabismus cases rather than in community-based surveys.
- Sex distribution: Most study results show no significant sex predilection. Male and female patients are affected equally.
- Age of onset: DVD usually manifests between 2 and 5 years of age, often after strabismus surgery, but can appear as early as infancy. This rarely presents in adolescence or adulthood unless long-standing childhood strabismus is present.
- Laterality: DVD is typically bilateral but asymmetric, with one eye more affected. Isolated unilateral cases are less common.[20]
Clinical Epidemiologic Associations
- Infantile esotropia is present in up to 70% to 80% of children with DVD.
- Latent nystagmus and oblique muscle overaction are commonly coexisting ocular motility disorders.
- Family history: Genetic and familial clustering have been suggested, but epidemiologic evidence remains limited.[21]
DVD is rare in the general population but common among children with infantile esotropia, with peak manifestation in early childhood and no sex predilection. The global frequency is underreported outside tertiary centers, but the condition carries consistent epidemiologic associations with early-onset strabismus syndromes.[22]
Pathophysiology
The exact mechanism underlying DVD remains incompletely understood. Still, several theories have been proposed, centering on abnormal binocular development, disruption of fusion, and aberrant vertical vergence control (see Image. Dissociated Vertical Deviation, Pathophysiology). A widely accepted belief is that DVD represents a disorder of binocular sensory processing that manifests as a motor imbalance. The exact cause of dissociated vertical deviation is not well understood. However, a few of the important theories explaining the underlying mechanism include:
- The Bielschowsky theory: Proposed alternating and intermittent excitation of subcortical vertical divergence centers as the cause of DVD.
- Later, it was thought of as a dorsal light reflex that modulates the central vestibular tone. Any fluctuations in the binocular visual input were supposed to stimulate the visual-vestibular reflex.[23]
- Guyton described it as a nystagmus blocking mechanism.[24]
- Spielmann suggested an imbalance of binocular stimulation.
- Few authors have also postulated an imbalance between the cortical input and subcortical pathways as the underlying pathology.[4][25]
Abnormal Binocular Development
- DVD is strongly associated with early-onset strabismus (especially infantile esotropia), suggesting that abnormal visual experience in the critical period disrupts the development of normal fusion.
- The absence of stable binocular input leads to dysfunction of the supranuclear fusion control centers, resulting in uncontrolled upward drifting of one eye when it is not fixating.[26]
Dissociated Nature of the Deviation
- Unlike comitant hypertropias, DVD is “dissociated,” meaning the deviation is not yoked to the Hering law of equal innervation.
- Each eye can drift upward independently, without a corresponding downward movement of the fellow eye. This reflects an abnormality in supranuclear ocular motor pathways controlling vertical vergence.[27]
Role of Fusion Maldevelopment Nystagmus Syndrome
- DVD often coexists with latent/manifest latent nystagmus and oblique overaction, leading some authors to consider it part of the “fusion maldevelopment nystagmus syndrome.”
- In this model, abnormal binocular control circuits in the brainstem and cerebellum development produce nystagmus and DVD.[16]
Neural Mechanisms
- Brainstem: Dysfunction within the interstitial nucleus of Cajal and posterior commissure is implicated in abnormal vertical vergence signals.
- Cerebellum: Aberrant output from the vestibulocerebellum (flocculus and nodulus) is believed to modulate the dissociated vertical drift.
- Cortical input: Deficient cortical binocular processing contributes to the loss of fusion and failure to suppress abnormal vergence signals.[28]
Clinical Correlates
- DVD is more prominent under inattention, fatigue, or monocular occlusion, consistent with its basis in disrupted fusional control.
- The association with early esotropia, latent nystagmus, and oblique dysfunction further supports the idea of a shared sensory-motor pathway disruption in infancy.
DVD arises from abnormal binocular sensory development in early childhood, leading to a supranuclear disorder of vertical vergence control. Brainstem and cerebellar dysfunction and loss of fusion cause one eye to drift upward independently when not fixating; this is best understood as part of the broader fusion maldevelopment spectrum rather than a simple motor imbalance.[29]
Histopathology
DVD is primarily a functional supranuclear disorder rather than a structural lesion. Unlike diseases with clear histopathologic tissue changes, DVD reflects abnormal neurophysiological control of ocular alignment due to defective development of binocular vision pathways in infancy (see Image. Dissociated Vertical Deviation (DVD), History and Physical Findings). However, correlates from neuropathology, animal models, and associated ocular changes help explain its basis.[4]
- Cortical and subcortical levels
- Visual Cortex: Abnormal development of binocular neurons in striate and extrastriate cortex, due to early disruption of fusion (commonly from infantile esotropia).
- Loss of normal cortical suppression mechanisms leads to unbalanced input into ocular motor nuclei.[4]
- Brainstem findings
- Dysfunction has been localized to the interstitial nucleus of Cajal and posterior commissure, which mediate vertical gaze and vergence.
- Abnormal output causes asymmetric innervation of vertical recti and oblique muscles, independent of the Hering law.[30]
- Cerebellar involvement
- Vestibulocerebellum (flocculus, nodulus) is implicated in adaptive control of eye movements.
- Histopathologic/functional studies suggest disinhibition of vertical vergence pathways, resulting in dissociated hypertropia.
- Cerebellar lesions in experimental primates can reproduce DVD-like phenomena.[27]
- Ocular and muscular correlates
- Extraocular muscles themselves show no primary histopathological abnormality in DVD.
- Secondary changes such as fibrosis or hypertrophy may be seen following long-standing strabismus or surgery, but these are nonspecific.[30]
- Neurophysiologic correlates
- Rather than true histopathology, DVD reflects a fusion maldevelopment nystagmus syndrome.
- Persistent abnormal neuronal firing in ocular motor integrators (brainstem + cerebellum) results in dissociated vertical drifts.[31]
Histopathology of DVD does not reveal local tissue damage but points to neurodevelopmental dysfunction within the visual cortex, brainstem vertical gaze centers, and cerebellar control circuits. The disorder arises from abnormal binocular development in infancy, leading to supranuclear dysregulation of vertical vergence pathways. No intrinsic disease of the extraocular muscles is found, making DVD a functional, centrally mediated condition rather than a peripheral structural pathology.[32]
Toxicokinetics
DVD is a neurodevelopmental strabismic disorder and not a toxin-mediated disease. Therefore, toxicokinetics in the classical sense (absorption, distribution, metabolism, excretion of toxins) does not apply directly to the pathogenesis. However, the concept becomes relevant when considering pharmacotherapy for the management of associated ocular motility or amblyopia-related complications, especially in children who may require prolonged therapy.[7]
Anticholinesterase Agents
- Refractory DVD/strabismus: Agents like echothiophate iodide were rarely historically used to induce miosis and augment accommodative effort.
- Absorption/metabolism: Topical absorption with systemic distribution; hydrolyzed by plasma cholinesterases
- Toxicity: Can cause iris cysts, prolonged paralysis with succinylcholine, and systemic cholinergic effects
- Clinical Relevance: Largely obsolete due to systemic adverse effects [3]
Botulinum Toxin, Botox
- Botox: Sometimes used in the nonsurgical management of DVD by injection into the superior rectus
- Absorption/distribution: Acts locally at the neuromuscular junction; blocks acetylcholine release with minimal systemic absorption
- Metabolism/Excretion: Degraded locally by proteolysis
- Toxicity: Local ptosis, overcorrection, and rare systemic weakness
- Kinetics: Onset within days, peak effect at 1 to 2 weeks, resolution in 3 to 4 months [12]
Corticosteroids (Adjunctive in Inflammatory Strabismus)
- Not a primary treatment for DVD; may be used when ocular inflammation coexists
- Absorption: Topical or systemic
- Metabolism: Hepatic
- Excretion: Renal
- Toxicity: Glaucoma, cataract, systemic effects with prolonged use [33]
Clinical Implications
- DVD is usually managed surgically (eg, superior rectus recession, inferior oblique weakening), but pharmacologic adjuncts require careful dosing and monitoring in children.
- Understanding the toxicokinetics of agents such as batrachotoxin and rare cholinesterase inhibitors is critical to balance efficacy with safety.
While DVD has no direct toxicokinetic basis, drugs occasionally used in its management (echothiophate iodide, botulinum toxin, corticosteroids) require awareness of their absorption, metabolism, and adverse effect profiles. The relevance of toxicokinetics in DVD lies in the safe use of adjunctive pharmacologic therapies, especially in pediatric and strabismus populations.[33]
History and Physical
Dissociated vertical deviation rarely presents in infancy, but is usually seen in patients between 2 and 5 years old. This condition can present as an isolated finding or be associated with other forms of strabismus, such as infantile esotropia, most commonly, or rarely, infantile exotropia, or Duane retraction syndrome.[34] This is usually bilateral and asymmetrical. The deviation is often more prominent in the amblyopic eye. The clinical features can be broadly divided into:
Deviation: This is defined as the upward drifting of the nonfixating eye when the patient fixates on the target with the other eye. This vertical deviation is often associated with extortion and slight abduction movement of the deviated eye. No movement is seen in the contralateral eye, as the uncovered eye takes up fixation. Thus, DVD is said to disobey the Herring law of ocular motility.
- Head posture: An abnormal head posture can be associated with one-third of the patients with DVDs. This is a motor adaptation to maintain binocular single vision. Patients presenting with this adaptation do not complain of double vision and tend to have good vision in both eyes.
- Sensory adaptations: Patients have binocular vision in the normal state, but fusion is lost when one eye deviates. The image from the deviated eye is suppressed, thus eliminating diplopia.[7]
Types of DVD
- Comitant: The vertical deviation is the same in abduction, primary position, and adduction.
- Incomitant: There is a significant difference in the deviation in abduction, primary position, and adduction.[22]
Types Based on Degrees of Deviation
This is defined based on the degrees of deviation measured in prism diopters (PD).
- Mild (0 to 9 PD)
- Moderate (10 to 19 PD)
- Severe (>20PD) [35]
History
Age of onset
- Most cases become evident between 2 and 5 years of age, coinciding with the development of visual attention and parental recognition of abnormal ocular movements.
- Rarely, a subtle DVD may be detectable in infancy but becomes clinically significant only after strabismus surgery (especially infantile esotropia surgery).[33]
Parental/patient observations
- Parents often describe the eye as "wandering upward" when the child is daydreaming, fatigued, or inattentive.
- DVD is intermittent, and parents may notice it more in photographs where one eye appears higher.
- Older children and adults may report awareness of eye drift in mirrors or may be teased about a cosmetic misalignment.[36]
Symptoms
- Diplopia is rare because the brain typically suppresses the deviating eye.
- Blurred vision is possible if the DVD is large and intermittent.
- Asthenopia: Some patients may report eye strain during near tasks due to intermittent ocular misalignment.
- Cosmesis is the most frequent complaint in adolescents and adults.[37]
Associated History
- This condition often coexists with infantile esotropia (present in 60%–80% of cases).
- This also may be associated with latent or manifest latent nystagmus.
- A history of strabismus surgery is common, with DVD often becoming more obvious postoperatively.
- A family history of strabismus, amblyopia, or nystagmus may be elicited.[32]
Physical Examination
General features
- Laterality: Typically bilateral but asymmetric; one eye may consistently demonstrate a larger deviation (see Image. Bilateral Exotropia)
- Character: A slow, spontaneous upward drift of the nonfixating eye, usually accompanied by excyclotorsion and abduction [36]
Cover-uncover test
- Hallmark finding: When one eye is covered, the nonfixing eye drifts upward; when uncovered, it slowly drifts back down without a corresponding downward movement of the other eye (violating the Hering law).
- The deviation may be more pronounced in distant fixation, inattention, or fatigue.[38]
Quantification
- Magnitude usually ranges from 8 to 15 prism diopters, but can be >20 PD in severe cases.
- The amplitude is often variable, even within the same patient at different examination times.[39]
Ocular motility
- Frequently associated with inferior oblique overaction
- May coexist with V-pattern strabismus
- No significant restriction of elevation or depression in versions, distinguishing DVD from restrictive or paretic causes [40]
Binocular sensory status
- Fusion: Poor or absent; fusional amplitudes are small
- Stereopsis: Usually reduced or absent (common in early-onset strabismus)
- Suppression: Deviating eye is typically suppressed during upward drift, preventing diplopia [41]
Associated ocular signs
- Latent or manifest latent nystagmus: Often present, especially in esotropic patients.
- Amblyopia: Frequently coexists in one eye due to strabismic amblyopia, requiring careful visual acuity assessment.
- Photophobia: Rare but reported in cases with large-amplitude DVD.[42]
Systemic/neurological exam
- No systemic abnormalities; DVD is an isolated ocular motility disorder
- Neurological exam is normal unless there is an associated secondary cause (rare)[43]
DVD typically presents in early childhood, most often in children with infantile esotropia or a history of strabismus surgery (see Table 3). Parents report an intermittent upward drift, often bilateral and asymmetric, worse with fatigue or inattention. On exam, the hallmark finding is a slow upward drift of the nonfixating eye with excyclotorsion, not following the Hering law (see Image. Evaluation Pattern of Dissociated Vertical Deviation). This is usually associated with latent nystagmus, inferior oblique overaction, reduced fusion, and poor stereopsis, but systemic and neurological findings are normal.[44]
Table 3. History and Physical Examination in Dissociated Vertical Deviation
|
Domain |
Findings |
|
Age of Onset |
Typically 2 to 5 years; occasionally after strabismus surgery; rarely in infancy |
|
Parental Observations |
Eye “drifts upward” when tired, daydreaming, or inattentive; noticed in photos |
|
Symptoms |
Usually asymptomatic; rarely diplopia; asthenopia in some; main concern is cosmesis |
|
Associated History |
Strongly linked with infantile esotropia (60%–80%); may follow strabismus surgery; associated with latent/manifest latent nystagmus; possible family history of strabismus |
|
Laterality |
Usually bilateral but asymmetric; one eye is more affected |
|
Characteristic Deviation |
Slow upward drift of non-fixating eye with excyclotorsion and abduction; returns slowly without reciprocal movement |
|
Cover-Uncover Test |
Eye drifts up under cover, drifts back down when uncovered; worsens with fatigue, inattention, distant fixation |
|
Magnitude |
Typically 8 to 15 prism diopters (can exceed 20 PD); variable amplitude |
|
Ocular Motility |
Frequently associated with inferior oblique overaction; may have V-pattern strabismus |
|
Binocular Sensory Status |
Fusion poor or absent; reduced/absent stereopsis; suppression of the deviating eye prevents diplopia |
|
Other Ocular Findings |
Latent/manifest latent nystagmus; amblyopia in the strabismic eye; rare photophobia |
|
Systemic Findings |
None; DVD is an isolated ocular motility disorder |
Evaluation
The diagnosis of dissociated vertical deviation is based on clinical examination alone. A few of the important tests include:
- Cover/uncover test: Spielmann translucent occluder is used.
- Manifest DVD: Once the fixating eye is covered, the deviated eye shows a downward movement to take up the fixation
- Latent DVD: The deviation manifests only once the eyes are dissociated. In this, no movement of the uncovered eye occurs; the eye is elevated and moves down once it is uncovered.[45]
- Head tilt test: The deviation of the eye increases on contralateral head tilt.[46]
- Bielschowsky graded density filter test: In this test, when one eye is covered, it elevates under the cover, and the other eye takes up the fixation. The filter bar, consisting of an increasing density of neutral density filters, is placed before the fixing eye. As the filter of gradually greater density is placed before the fixing eye, the elevated eye starts moving down. When the filters of lesser density are placed in front of the fixing eye, the other eye undercover will start elevating again.[47]
- Red filter test: This is also a dissociation test. Torchlight is shown as a target, and red glass is placed in front of one eye. The red glass dissociated the eyes. The eye behind the filter drifts up, and the patient localizes the red image of the fixation light. In the DVD, the red light is always seen below the fixation light, regardless of which eye the filter is placed in. This helps differentiate DVD from other cyclo-vertical deviations, in which red light position changes relative to the fixation light based on which eye fixates.[48]
- Measurement of DVD: This is done using a base-down prism. A prism is placed in front of the deviated eye first, and the patient is asked to fixate on a target located at a distance of 6 meters. The occluder is then shifted to the fixating eye, allowing the deviating eye to take up fixation. The alternate cover test is repeated with prisms of greater power until no downward movement of the deviated eye is noted. This test must be repeated for each eye in patients with bilateral DVDs.[49]
Grading of DVD
- 1+ deviation= a slight deviation
- 2+ deviation= a small deviation
- 3+ deviation= a moderate deviation
- 4+ deviation= a large deviation [50]
A DVD is primarily a clinical diagnosis, established through history and a detailed orthoptic/ocular motility examination. Investigations are directed toward quantifying the deviation, ruling out differential diagnoses, and planning management.
Clinical Examination
- History Taking:
- Age of onset, frequency, triggers (fatigue, inattention, occlusion)
- Previous strabismus surgery or history of infantile esotropia
- Family history of strabismus or amblyopia
- Visual acuity testing:
- To assess for amblyopia in one or both eyes, which is common in strabismic children
- Cover tests (mandatory):
- Cover-uncover test: Reveals slow, spontaneous upward drift of the covered (nonfixating) eye with excyclotorsion, a hallmark of DVD
- Alternate cover test: Helps quantify the deviation using the prism cover measurement
- Laterality assessment:
- Determine whether the DVD is bilateral but asymmetric or unilateral
- Measurement of deviation:
- Use prism diopters at distance and near fixation
- Note variability in amplitude depending on attention, fatigue, or fixation target
- Ocular motility evaluation:
- Assess for inferior oblique overaction or V-pattern strabismus.
- Check for coexistence of latent/manifest latent nystagmus.
- Binocular sensory testing:
- Worth 4-dot test and Bagolini striated lenses are used to evaluate fusion
- Stereopsis testing (Titmus Fly, Randot)–usually reduced or absent [51]
Ancillary Tests
- Cycloplegic refraction:
- Rule out associated refractive errors (hyperopia, astigmatism)
- Prescribe spectacles for amblyopia management
- Fundus examination:
- Evaluate for torsion (excyclotorsion often noted in DVD)
- Exclude structural anomalies
- Ocular imaging (optional):
- Not required for diagnosis, but optical coherence tomography may be used if coexisting amblyopia or structural causes are suspected [52]
Guidelines Perspective
- American Association for Pediatric Ophthalmology and Strabismus, AAPOS:Clinical evaluation with the prism cover test is recommended as the gold standard. Surgery is indicated only if the deviation is cosmetically significant or interferes with binocular function.
- American Academy of Ophthalmology, AAO:This organization emphasizes comprehensive strabismus workup, including ocular motility, binocular function, and refraction, with surgery tailored to functional/cosmetic needs.
- International Practice (UK, Europe, Asia):The guidelines are similar, stressing careful differentiation from true hypertropia, oblique dysfunction, and skew deviation.[53]
DVD evaluation relies on a detailed clinical assessment, especially covering testing and prism measurement, supported by binocular sensory testing and refraction. No specialized laboratory or radiographic test is required. International guidelines emphasize accurate diagnosis, quantification, and differentiation from other vertical strabismus for appropriate surgical planning.[49]
Treatment / Management
Treatment of dissociated vertical deviation can vary from observation to nonsurgical or surgical.
- Observation: This might be sufficient in patients with latent DVD, especially those older than 8, when the risk of amblyopia is not of concern, with small degrees of anomalous head postures, and not a significant cosmetic blemish.
- Nonsurgical: Conservative therapy, in the form of changing the fixation pattern or encouraging fusion, can be useful for small deviations. A slight optical blur induced in the fixating eye example by adding a +2D lens shifts the fixation preference to the other eye, and thus, DVD is avoided.[54] Injection of Botulinum toxin into the superior rectus has also been described.[55]
- Surgical: This is indicated when there is greater than +2 deviation; large DVD frequently manifests, anomalous head posture, or a significant cosmetic blemish. The literature describes several surgical options for DVD.
Important surgical options among these include:
- Inferior oblique weakening [56]
- Anteriorization of the inferior oblique [57]
- Anteriorization of the inferior oblique with resection [58]
- Superior rectus large recession (7 to 10 mm) [59][60]
- Faden operation with superior rectus recession of 3 to 5 mm [61]
- Inferior rectus resection: 4 mm for small deviations, 6 mm for intermediate deviations, and 8mm for large deviations [62]
- Anteronasal transposition of the inferior oblique [63]
- Inferior rectus tucking [64]
- Four-muscle oblique surgery [50][65] (A1)
The surgical treatment can be planned based on the DVD grade and the presence or absence of inferior oblique (IO) overaction.
- DVD with no IO overaction: Superior rectus recession + inferior rectus resection
- Moderate DVD with IO overaction: Recession with anteropositioning of IO
- Severe DVD with IO overaction: Recession with anteropositioning of IO + superior rectus recession (7 to 10 mm) [66]
The severity of deviation, cosmetic significance, functional impact, and association with other strabismic disorders guide DVD management. Most children are asymptomatic, and treatment is indicated primarily for cosmetic concerns, large-angle deviation, or when DVD interferes with fusion.
Observation and Nonsurgical Management
- Observation:
- A small, intermittent, and cosmetically insignificant DVD requires no active intervention.
- Parents should be reassured about the benign course.[50]
- Amblyopia therapy:
- If amblyopia coexists, treatment with occlusion therapy or optical correction is essential.
- Prisms/glasses:
- This is rarely useful for DVD correction, but may help address associated horizontal deviation or refractive error.[67]
Surgical Management (Mainstay of Treatment)
Surgery is considered when the DVD is large (>8–10 prism diopters), cosmetically disfiguring, or interferes with binocular vision.[66]
Superior rectus recession
- This is the most common surgery for DVD.
- Bilateral superior rectus recession is often performed in bilateral DVD.
- The amount of recession is titrated to the deviation magnitude.[68]
Inferior oblique weakening
- This is indicated when the DVD is associated with IO overaction.
- Procedures: IO recession, myectomy, or anterior transposition.
- IO anterior transposition has the dual benefit of reducing IO overaction and DVD.[69]
Combined procedures
- In large or asymmetric DVDs with IO overaction, SR recession + IO weakening may be combined.
- Unilateral DVD: This includes unilateral SR recession, occasionally combined with IO anterior transposition.
Posterior fixation sutures (Faden procedure)
- This is applied to the superior rectus in selected cases, especially when DVD is incomitant.[70]
Role of botulinum toxin
- Rarely used as a temporary measure for DVDp (particularly when surgery is contraindicated)
- Provides transient reduction but is not a definitive treatment
Prognosis after surgery
- Surgical success rates: A 60%–80% reduction in deviation has been shown.
- Residual DVD is common but usually less cosmetically significant.
- Repeat surgery may be needed in severe or recurrent cases.[71]
Guideline-based approach
- AAPOS/AAO Recommendations:
- Surgery is indicated only if the DVD is large, cosmetically unacceptable, or interferes with fusion.
- The choice of procedure depends on the presence/absence of IO overaction.
- The emphasis is on tailoring surgery to asymmetry (bilateral vs unilateral).
DVD is usually observed if mild, but for larger, cosmetically significant deviations, superior rectus recession with or without inferior oblique weakening is the treatment of choice. Combined procedures are often required in asymmetric or severe cases. Prognosis is generally favourable, though recurrence or residual deviation may occur.[66]
Differential Diagnosis
The closest and most important differentials to consider are inferior oblique overaction (IOOA) and acquired skew deviations; this is important to differentiate, as the surgical approach differs for these conditions.
The important differentiating points between IOOA and DVD include:
- Hyperdeviation is greatest in adduction in cases of IOOA. In contrast, in DVD, the hyperdeviation remains similar in primary, adducted, and abducted gaze positions.
- The V pattern is associated with IOOA but is absent in the DVD.
- Superior oblique under action is usually associated with IOOA.
- An extorted macula can be seen in IOOA, but it is absent in DVD patients.
- The Bielschowsky phenomenon is present in DVD, while it is absent in true hypertropia.[72]
The important differentiating points between acquired skew deviation and DVD (see Table 4) include:
- Skew deviations can present at any age, but the most common age of presentation among those with DVDs is around 2-4 years.
- In skew deviations, there is intortion of the higher eye and extortion of the lower eye, while vice versa in DVD.
- A brainstem or cerebellar region lesion can be associated with skew deviation.
- Vertical diplopia is associated with skew deviation, while DVD is not associated with similar complaints.
- Seesaw or hemi-seesaw nystagmus is associated with skew deviation, while DVD is associated with latent nystagmus.[73]
Table 4. Differential Diagnosis of DVD
|
Condition |
Distinguishing Features |
Key Points to Differentiate from DVD |
|
Superior Oblique Palsy |
Hypertropia increases on contralateral gaze and ipsilateral head tilt (positive Bielschowsky head tilt test). This is often associated with excyclotorsion. |
DVD is dissociated (not following the Hering law), often bilateral/asymmetric, and not limited to specific gaze/head tilt. |
|
Inferior Oblique Overaction |
Overelevation of the eye in adduction is usually symmetric and comitant with horizontal gaze changes. |
DVD occurs in primary gaze or during dissociation (cover test), not just in adduction. |
|
Skew Deviation |
Vertical misalignment due to brainstem/vestibular lesions; may be associated with head tilt, ataxia, or neurologic signs. |
DVD is usually seen in children with strabismus/amblyopia; skew deviation has an acute onset and neurologic features. |
|
Comitant Hypertropia |
Constant vertical deviation, equal in all gazes; follows the Hering law. |
DVD is variable, manifests only on dissociation, and does not obey the Hering law. |
|
Monocular Elevation Deficiency (Double Elevator Palsy) |
Limitation of elevation in all positions of gaze in one eye; true restriction or paresis. |
DVD shows free elevation, but with dissociated vertical drift when fixing eye changes. |
|
Latent Nystagmus With Vertical Component |
Vertical movements may accompany latent nystagmus; it occurs on monocular occlusion. |
DVD shows a slow upward drift, not rhythmic oscillations. |
|
Ocular Tilt Reaction |
Triad: skew deviation, head tilt, ocular torsion, typically from brainstem lesions. |
DVD is not associated with torsional shifts or neurologic tilt reaction. |
DVD should be distinguished from superior oblique palsy, inferior oblique overaction, skew deviation, comitant hypertropia, monocular elevation deficiency, latent nystagmus, and ocular tilt reaction. Careful evaluation of gaze dependency, torsional changes, compliance with the Hering law, and associated neurologic/systemic findings helps establish the correct diagnosis.[74]
Pertinent Studies and Ongoing Trials
Pertinent studies and ongoing trials include the following:
- Most evidence for DVD management comes from retrospective case series and small prospective cohorts; randomized trials are rare.
- Common surgical options include bilateral superior rectus (SR) recession (± posterior fixation), IO anteriorization/anterior-nasal transposition, and combined SR + IO procedures for mixed DVD/IO overaction.
- Across series, surgery typically reduces DVD by ~60% to 80% and improves head posture/manifestation of dissociation; undercorrection and asymmetry remain the main limitations.
- Risk of iatrogenic hypotropia and anti-elevation syndrome is higher with aggressive SR weakening or IO anteriorization—careful titration and symmetry are key.
- Nonsurgical measures (occlusion, optical penalization, amblyopia therapy) help in mild or intermittent DVD, especially in children (see Table 5).[74]
Table 5. Representative DVD Studies
|
Study Type |
Intervention(s) |
Sample Size (Typical) |
Main Findings |
|
Retrospective Series |
Bilateral SR recession (6–10 mm) ± posterior fixation |
20–80 |
This means a meaningful reduction of DVD, recurrence/undercorrection in a minority, and risk of hypotropia if over-recessed. |
|
Retrospective/Prospective Cohorts |
IO anteriorization / anterior-nasal transposition (when DVD + IO overaction) |
15–60 |
Good control of DVD in adduction and primary gaze; watch for anti-elevation syndrome if placed too anterior. |
|
Comparative Case Series |
SR recession vs IO anteriorization |
30–60 |
Similar overall control; choice guided by IO overaction and dissociation pattern. |
|
Combined Procedures |
SR recession + IO weakening |
20–50 |
Useful in large, asymmetric DVDs with IOOA; higher risk of vertical incomitance if asymmetrically dosed. |
DVD, dissociated vertical deviation; IO, inferior oblique; IOOA, inferior oblique overaction; SR, superior rectus
Evidence Gaps
Standardized dose–response tables, long-term (>5 years) outcomes, and validated patient-reported measures (cosmesis, asthenopia).
Ongoing/Needed Trials
- Prospective multicenter registry tracking pre-/postoperative angle, incomitance, stereopsis, and patient-reported outcome measures.
- Randomized/controlled trials comparing SR recession vs IO anteriorization in DVD with IO overaction, and evaluating posterior fixation augmentation.
- Technique refinements (graded anterior-nasal transposition vs classic IO anteriorization) to minimize anti-elevation.
- Nonsurgical protocols (standardized amblyopia/penalization pathways) for intermittent or small-angle DVD.[75]
Treatment Planning
Initial Assessment
- Severity of deviation: Angle of DVD (mild <10 PD, moderate 10–15 PD, severe >15 PD)
- Laterality: Bilateral (most common) vs unilateral or asymmetric presentation
- Associated anomalies: IOOA, latent nystagmus, amblyopia, or dissociated horizontal deviation
- Functional impact: Cosmesis, abnormal head posture, asthenopia, or suppression
- Age and visual potential: Younger children may require amblyopia management first [4]
Nonsurgical Management
- Observation: Mild, intermittent, or cosmetically insignificant cases can be monitored
- Amblyopia therapy: Occlusion or penalization to equalize fixation preference
- Prisms: Limited role due to dissociated nature (not comitant)
- Orthoptic therapy: Minimal efficacy, but may help in binocular stabilization [76]
Indications for Surgery
- Large DVD (>12–15 PD) affecting cosmesis
- Asymmetrical DVD with marked cosmetic disfigurement
- Frequent manifest DVD interfering with binocularity
- Associated IO overaction producing V-pattern or overelevation in adduction [77]
Surgical Options
|
Procedure |
Indication |
Advantages |
Limitations/Complications |
|
Bilateral Superior Rectus Recession |
Large, symmetrical DVD |
Standard procedure reduces elevation drift |
Risk of iatrogenic hypotropia, asymmetry if under-/over-corrected |
|
SR Recession with Posterior Fixation (Faden) |
Large DVD with risk of recurrence |
Enhances stability, reduces overaction |
Technically more demanding |
|
Unilateral SR Recession |
Asymmetrical DVD |
Targeted correction |
May unmask a latent DVD in the fellow eye |
|
IO Anteriorization/ Anterior-Nasal Transposition |
DVD with IO overaction |
Corrects both IOOA and DVD in abduction |
Risk of anti-elevation syndrome |
|
Combined SR + IO procedures |
Severe or mixed cases |
Comprehensive correction |
Higher risk of vertical incomitance |
|
Graded IO Anteriorization |
Moderate asymmetric DVD with IOOA |
Stepwise titration |
Requires surgical expertise |
DVD, dissociated vertical deviation; IO, inferior oblique; IOOA, inferior oblique overaction; SR, superior rectus
Postoperative Care and Follow-Up
- Follow up regularly for residual/recurrent DVD.
- Monitor for iatrogenic hypotropia, anti-elevation syndrome, or induced vertical incomitance.
- Continue amblyopia management if needed.
- Counsel parents regarding variable outcomes and the possibility of staged surgery.[78]
Treatment Strategy
- Mild/asymptomatic DVD: Observation + amblyopia therapy
- Moderate DVD or asymmetry: Targeted SR or IO procedure
- Severe/bilateral DVD (>15–20 PD): Bilateral SR recessions (± posterior fixation)
- DVD with IO overaction: IO anteriorization or anterior-nasal transposition ± SR surgery
- Residual/recurrent cases: Secondary procedures or combined surgery [21]
Treatment must be individualized based on severity, symmetry, cosmesis, presence of IOOA, and binocular potential. Surgery aims at reducing the manifest deviation to a cosmetically and functionally acceptable level rather than complete elimination.
Toxicity and Adverse Effect Management
Adverse effects and surgical complications can occur with DVD. See Table 6 below for more information.
Table 6. Surgical Complications and Their Management
|
Complication |
Cause/Mechanism |
Management |
|
Iatrogenic Hypotropia |
Excessive superior rectus (SR) weakening |
Mild: observation (often improves) Severe: surgical revision (advancement of SR or recession of antagonist inferior rectus) |
|
Anti-Elevation Syndrome |
Over-anteriorization of inferior oblique (IO) (esp. anterior-nasal placement) |
Avoid aggressive anteriorization; if symptomatic, surgical repositioning of the IO |
|
Asymmetry/Residual DVD |
Under- or over-correction in bilateral cases |
Secondary surgery on the contralateral eye or augmentation of the previous procedure |
|
Vertical Incomitance |
Asymmetric or excessive surgery |
Prism therapy for mild cases; reoperation for severe incomitance |
|
Overcorrection Leading to Hypotropia in Downgaze |
Large SR recession |
Stepwise graded recession recommended; surgical adjustment if disabling |
|
Scarring and Motility Restriction |
Excessive dissection or reoperations |
Preventive gentle technique; surgical adhesiolysis if significant |
Nonsurgical Risks
- Amblyopia progression: Persistent suppression in the deviating eye; managed with occlusion or penalization therapy.
- Cosmetic dissatisfaction: Parents/patients may perceive residual updrift postop; preoperative counseling is required to set realistic expectations.
- Loss of fusion potential: Rare, but can occur in late or incomplete correction cases.[79]
Preventive Strategies
- Graded and symmetric surgical dosages to minimize overcorrection/undercorrection
- Tailoring surgery to the associated IO overaction (SR vs IO approach)
- Preoperative counseling regarding the possibility of recurrence or staged procedures
- Regular follow-up for early detection of complications [7]
DVD management is aimed at functional improvement and cosmesis, not complete elimination of deviation. Complications like hypotropia, anti-elevation, and residual asymmetry are best prevented with careful planning, conservative dosages, and stepwise surgical approaches. When they occur, most can be managed with observation, prism therapy, or revision surgery.[66]
Staging
The following details the DVD staging; please see Table 6 below for a complete summary.
Based on the Magnitude of Deviation
- Mild DVD: <10 PD; often intermittent, cosmetically insignificant, rarely requires surgery
- Moderate DVD: 10–15 PD; frequently noticeable, may cause cosmetic concern, surgical consideration if persistent
- Severe DVD: >15–20 PD; manifests most of the time, cosmetically disfiguring, usually a surgical candidate [49]
Based on Laterality
- Unilateral DVD: Rare; usually in the amblyopic eye
- Bilateral symmetrical DVD: Common in infantile esotropia; both eyes drift equally
- Bilateral asymmetrical DVD: One eye shows greater elevation than the other, often requiring an asymmetric surgical approach [80]
Based on the Frequency of Manifestation
- Latent DVD: Manifests only on dissociation (cover test)
- Intermittent DVD: Appears when fatigued, daydreaming, or under stress
- Manifest DVD: Constantly present; cosmetically significant [81]
Based on Associated Findings
- DVD with IOOA: Requires a combined approach (IO anteriorization)
- DVD without IOOA: Best managed with SR weakening procedures
- DVD with amblyopia/latent nystagmus: Indicates broader sensory disruption and may impact management [82]
Table 6. Practical Staging of DVD Summary
|
Stage |
Criteria |
Clinical Significance |
|
Stage I, Mild |
<10 prism diopters (PD), latent or intermittent, minimal cosmetic impact |
Observation ± amblyopia therapy |
|
Stage II, Moderate |
10–15 PD, frequent, cosmetically noticeable |
Consider surgery if symptomatic |
|
Stage III, Severe |
>15–20 PD, manifest most of the time, often asymmetric |
Surgical correction is usually indicated |
DVD is not formally staged in the way cancers or systemic diseases are, but clinicians commonly describe it in terms of severity, laterality, frequency, and associated anomalies. This practical staging helps guide treatment planning (eg, observation vs surgery and unilateral vs bilateral procedures).[22]
Prognosis
Depending on the frequency or degrees of deviation, the dissociated vertical deviation can be observed, or nonsurgical or surgical treatment might be needed. No major studies have compared nonsurgical versus surgical management options. The most frequently performed procedures include inferior oblique anteriorization or superior rectus weakening. The choice of surgical procedure depends on the degree of deviation, the degree of anomalous head posture, and the surgeon's preference.[72]
Natural History
Dissociated Vertical Deviation is generally non-progressive and persists throughout life once it develops. It often becomes apparent in early childhood, especially in those with infantile esotropia, amblyopia, or latent nystagmus. In many cases, the deviation may appear more noticeable with fatigue, inattention, or loss of fixation.[83]
Visual Prognosis
Visual acuity and long-term ocular health are usually unaffected if amblyopia is appropriately managed. However, untreated amblyopia can worsen outcomes, particularly in unilateral or asymmetric cases. Binocular vision potential is limited in most children with DVD, as it reflects early sensory disruption, but some patients may retain fusion in primary gaze.[84]
Cosmetic and Functional Outcomes
Mild DVD may be tolerated well, with minimal cosmetic impact. Moderate to severe cases can cause significant cosmetic disfigurement due to frequent upward drifting of one eye, which is often the main reason for surgical intervention.[50]
Surgical prognosis
Surgery (superior rectus recession, inferior oblique anteriorization, or combined procedures) typically reduces DVD magnitude by 60% to 80%. However:
- Residual DVD is common, and complete elimination is rare.
- Recurrence can occur, particularly in young children and asymmetric cases.
- Complications such as hypotropia or anti-elevation syndrome may affect long-term outcomes if surgical dosing is excessive.[85]
Quality of life
With appropriate treatment, most patients achieve cosmetically acceptable alignment and functional improvement. Residual DVD is often small enough to be socially inconspicuous. Early diagnosis and amblyopia management improve visual outcomes and reduce psychosocial impact. DVD has a benign visual prognosis but a variable cosmetic prognosis. Most patients achieve satisfactory long-term outcomes with observation or surgery, but recurrence and incomplete correction are common, requiring realistic expectations and, occasionally, staged procedures.[86]
Complications
The complications can be divided into those related to the disease, anesthesia, or those related to the surgical process (intraoperative or postoperative)
- Related to disease: Amblyopia, torticollis, and contracture of the sternocleidomastoid muscle.
- Anesthesia-related: Oculocardiac reflex, malignant hyperthermia, cardiac arrest, hepatic porphyria, or succinylcholine–induced apnoea
- Surgical complications:
- Intraoperative: Hemorrhage, Lost or slipped muscle, eyeball perforation, inadvertent injury to surrounding structures/muscles, operation of the wrong muscle or eye
- Postoperative complications include suture reaction, conjunctival granuloma, anterior segment ischemia, diplopia, retinal detachment, under- or overcorrections, and adhesive syndrome.[87]
Although the DVD is not vision-threatening, complications arise mainly from its clinical course, associated conditions, and surgical management (see Table 7).
Natural/Functional Complications
- Amblyopia: Common in unilateral or markedly asymmetric cases due to suppression of the deviating eye
- Loss of Binocular Function: Poor fusion and stereopsis (result from early binocular disruption)
- Cosmetic Impact: Visible updrift of one eye causes social/psychological distress
- Abnormal Head Posture: Rare, but may be adopted to minimize the cosmetic impact or maintain fusion [88]
Table 7. Surgical Complications of DVD
|
Complication |
Cause |
Notes/Management |
|
Residual or Recurrent DVD |
Under-correction or progression of dissociation |
Common; often managed with secondary procedures |
|
Overcorrection → Hypotropia |
Excessive superior rectus (SR) recession |
Requires revision (SR advancement or antagonist weakening) |
|
Anti-Elevation Syndrome |
Anteriorization/anterior-nasal transposition of inferior oblique (IO) |
Prevent with careful placement; if severe, IO repositioning may be required |
|
Vertical Incomitance |
Asymmetric surgery or scarring |
Can produce diplopia in eccentric gaze |
|
Scarring/Adhesions |
Multiple surgeries or excessive dissection |
May restrict motility; surgical adhesiolysis if needed |
Psychosocial/Quality-of-Life Complications
- Cosmetic disfigurement: Persistent visible updrift can impact confidence and social interactions even after surgery.
- Parental anxiety: In pediatrics, visible eye movements often cause parental concern, requiring counseling.[89]
DVD complications are most often cosmetic and functional rather than vision-threatening. Long-term outcomes are generally good with careful amblyopia management, surgical planning, and parental counseling. The main risks relate to residual asymmetry, hypotropia, or anti-elevation syndrome after surgery.[84]
Postoperative and Rehabilitation Care
Postoperatively, the patient should be started on low-dose surface-acting topical steroids in the form of 0.5% loteprednol 4 times per day for 1 week and then tapered over weekly intervals along with topical antibiotics 0.5% moxifloxacin 4 times per day for 20 days. The patient can also be started on oral analgesics, 50 mg diclofenac twice daily for the initial 3 to 5 days to reduce the pain. The patient should be followed up at 1 month and reassessed for head posture and ocular deviation with a prism bar cover test.
The parents and patient should receive explanations regarding the need for regular follow-up and the use of postprocedure medication. To prevent amblyopia, parents must understand the importance of patching or occlusion therapy, particularly in children younger 8, in cases of residual deviation. The patient can be followed up at 3 months and 6-monthly intervals thereafter until the critical age for amblyopia has passed.[4] DVD management does not end with surgery; comprehensive postoperative care is essential to optimizing outcomes, preventing complications, and maximizing binocular function.
- Immediate Postoperative Care
- Topical medications:
- Antibiotic-steroid combination drops for 2 to 3 weeks to prevent infection and reduce inflammation
- Lubricating eye drops to improve comfort
- Pain management:
- Mild oral analgesics (acetaminophen or nonsteroidal anti-inflammatory drugs) as needed
- Activity restrictions:
- Avoid swimming, dusty environments, and eye rubbing for at least 2–3 weeks.[7]
- Topical medications:
- Early follow-up (first 6 weeks)
- Examination schedule:
- Typically at 1 week, 1 month, and 6 weeks post-surgery
- Assessment:
- Wound healing, residual deviation, ocular motility, and presence of inflammation
- Monitor overcorrection/undercorrection
- Complication surveillance:
- Watch for conjunctival scarring, infection, anterior segment inflammation, or slipped muscle.[16]
- Examination schedule:
- Visual rehabilitation
- Amblyopia therapy:
- Postoperative occlusion therapy if amblyopia persists
- Optical correction:
- Ensure accurate refractive correction with glasses.
- Prism therapy:
- Occasionally prescribed for small residual deviations [22]
- Amblyopia therapy:
- Orthoptic and binocular vision therapy
- Postsurgery, some patients may benefit from orthoptic exercises to enhance binocular coordination.
- Though stereopsis recovery is limited in infantile strabismus, fusion potential should be maximized.[90]
- Long-term care
- Recurrence monitoring:
- DVD may recur or persist at reduced magnitude; long-term follow-up every 6–12 months is recommended.
- Reoperation:
- Considered significant residual or recurrent (this DVD is cosmetically disturbing)
- Recurrence monitoring:
- Psychosocial support:
- Address cosmetic concerns, especially in adolescents.[91]
- Guideline perspective
- AAPOS/AAO:
- Stress the importance of postoperative amblyopia management, accurate refraction, and counseling families about possible residual DVD even after surgery.
- AAPOS/AAO:
Postoperative care for DVD involves topical therapy, wound healing surveillance, amblyopia treatment, and orthoptic support. Long-term follow-up is crucial, as recurrence or residual DVD is common. Rehabilitation focuses on maximizing fusion, correcting amblyopia, and addressing cosmetic or psychosocial concerns.[4]
Consultations
Any patient visiting the outpatient department with a DVD to any general ophthalmologist must be referred to an expert pediatric ophthalmologist for a higher opinion and further management. The pediatric ophthalmologist is critical in deciding on conservative or surgical management in these cases. The pediatric ophthalmologists' skill and expertise will help decide the need for spectacles, patching or occlusion therapy, fusion exercises, or surgical management.[92]
Initial Point of Contact
- Patients with DVD often present first to a general ophthalmologist or an optometrist for complaints of strabismus, abnormal ocular movements, or cosmetic concerns.
- Since DVD is a specialized form of strabismus, diagnosis may be missed or confused with hypertropia or oblique dysfunction in a general practice.
- Early recognition and referral to a pediatric ophthalmologist or strabismus specialist is crucial for timely and appropriate management.[93]
Role of the Pediatric Ophthalmologist/Strabismus Specialist
The pediatric ophthalmologist plays a central role in the continuum of care:
- Diagnostic accuracy:
- Differentiates DVD from true hypertropia, oblique overaction, skew deviation, thyroid eye disease, or paresis.
- Uses specialized strabismus tests (cover-uncover, prism quantification, binocular function assessment).
- Evaluation of associated conditions:
- Screens for infantile esotropia, latent nystagmus, amblyopia, inferior oblique overaction, and V-pattern strabismus.
- Identifies patients requiring amblyopia therapy in parallel with DVD treatment.[94]
- Conservative management planning:
- Decides on optical correction for refractive errors.
- Prescribes patching or occlusion therapy for amblyopia.
- Recommends fusion or orthoptic exercises in selected cases to enhance binocular function.[95]
- Surgical decision-making:
- Evaluates the magnitude of DVD, asymmetry, and coexisting oblique dysfunction.
- Selects appropriate procedure: superior rectus recession, inferior oblique weakening (recession, myectomy, anterior transposition), or combined approaches.
- Tailor surgery (unilateral vs bilateral) depends on the deviation and cosmesis.[96]
Multidisciplinary Collaboration
DVD management often requires input from multiple professionals:
- Optometrists/orthoptists: Assist in measuring deviations, prism testing, and orthoptic exercises.
- Vision therapists: Provide fusion training and binocular therapy where potential exists.
- Counselors/psychologists: Support children and adolescents with cosmetic concerns or psychosocial distress due to visible ocular misalignment.[97]
Timing and Follow-up Consultations
- Preoperative consultation: This is meant to confirm diagnosis, quantify deviation, and plan an individualized surgical approach.
- Postoperative follow-up: Pediatric ophthalmologists guide wound healing, amblyopia therapy, prism correction (if required), and long-term monitoring.
- Long-term monitoring: As DVD may persist, fluctuate, or recur, ongoing specialist review ensures timely reoperation if necessary.[98]
Guideline Perspective
- AAPOS and AAO recommend that a strabismus-trained pediatric ophthalmologist evaluate all suspected DVD patients for accurate diagnosis and tailored management.
- International practice standards emphasize team-based care, with pediatric ophthalmologists supported by orthoptists and optometrists to optimize outcomes.
Consultations for DVD require a tiered referral system. General ophthalmologists serve as the entry point but should promptly refer to pediatric ophthalmologists or strabismus specialists for definitive diagnosis and management. These specialists are uniquely trained to balance conservative therapy, amblyopia care, and surgical planning, while collaborating with orthoptists, optometrists, and vision therapists. Long-term follow-up under specialist care is essential, as DVD often requires continued monitoring and sometimes repeat intervention.[99]
Deterrence and Patient Education
Patient education and involvement of parents/guardians in management decision-making are important. Observation or patching with close follow-ups might be sufficient in patients with minimal head postures or latent deviations. Parents can be reassured and informed about the natural course of the disease. If surgery is indicated, a detailed discussion about the risks and benefits should be conducted with the parents. They should also be informed about the possible psychological impact of strabismus on the child and directed to support groups, which can benefit the child’s well-being and outcome.
Patient and Family Education
- Families should be counseled that DVD is a benign but chronic ocular motility disorder, usually linked to early strabismus such as infantile esotropia.
- Parents should understand that DVD often appears intermittent, becoming more noticeable when the child is tired, daydreaming, or when one eye is covered.
- Emphasize that DVDs do not usually cause double vision because the brain suppresses the deviating eye, but they may reduce binocular function and stereopsis.[100]
Role of Regular Follow-up
- Routine monitoring is essential to assess the progression of deviation, the development of amblyopia, and the need for surgery.
- Families should be educated on the importance of regular pediatric ophthalmology visits, even if symptoms appear stable.[10]
Preventing Secondary Effects
- Amblyopia prevention: Early detection and treatment with patching or occlusion therapy is essential to maintain visual acuity.
- Spectacle compliance: Ensure proper correction of refractive errors to reduce associated strabismic amblyopia.
- Psychosocial support: Parents should be counseled that large, untreated DVDs may cause cosmetic concerns, leading to low self-esteem in children; timely intervention prevents social difficulties.[101]
Indications for Surgical Referral
- Parents should be informed that not all cases require surgery, and small-angle DVD can often be observed.
- Surgery is considered if the deviation is large, cosmetically disturbing, asymmetric, or interferes with fusion.
- Families should understand that the expected outcomes typically improve, but do not eliminate the deviation.[66]
Lifestyle and Home Guidance
- Encourage adequate visual hygiene (proper reading posture, breaks during near work).
- Explain that fatigue and inattention may exacerbate DVD, so ensuring rest and healthy routines may help reduce its appearance.
- Parents should avoid excessive self-imposed patching without medical advice, as inappropriate occlusion may worsen amblyopia or imbalance.[102]
Empowering Parents
- Educate caregivers to observe the frequency and severity of eye drifting and report during follow-up.
- Ensure that DVD is a known entity with effective management strategies, preventing unnecessary anxiety.
- Share credible resources (AAPOS patient guides, trusted ophthalmology society websites) for further understanding.
Deterrence and patient education in DVD focus on early recognition, regular follow-up, amblyopia prevention, and reassurance. Parents should be empowered with knowledge about when intervention is necessary, while being counseled on the cosmetic and psychosocial impact. Proper education prevents neglect, reduces anxiety, and ensures timely treatment for optimal visual and social outcomes.[103]
Pearls and Other Issues
The dissociated vertical deviation is a rare form of squint, and it might be challenging for the evaluating optometrist/ophthalmologist to choose the best suitable management option. A thorough history, visual acuity, examination details, and parents' concerns related to the condition will help choose the best customized treatment plan for each patient. Observation with or without patching, along with refractive correction, can be sufficient for most of the patients. Surgery can be reserved for patients with frequent deviations, large degrees of deviation, large degrees of anomalous head posture, or apprehensive parents.
Clinical Pearls
- Characteristic drift:
- DVD manifests as a slow, spontaneous upward drift of the nonfixating eye, often with excyclotorsion and abduction, distinguishing it from hypertropia or paresis.
- Dissociated nature:
- Unlike comitant hypertropias, DVD does not follow the Hering law; the fellow eye does not show a reciprocal movement.
- Association with infantile esotropia:
- Most cases occur in children with infantile esotropia or after surgery for esotropia, highlighting the shared sensory pathway disruption.
- Bilateral but asymmetric:
- Always look for asymmetry; many cases labeled “unilateral DVD” are bilateral with a subtle contralateral component.[50]
Disposition
- Most cases are benign and primarily a cosmetic issue.
- Observation is appropriate for a small-angle, intermittent DVD with no functional disturbance.
- Surgery is indicated for large, cosmetically disturbing deviations or when DVD interferes with binocular vision.[72]
Common Pitfalls
- Misdiagnosis:
- Confusing DVD with superior oblique palsy, skew deviation, thyroid-related hypertropia, or restrictive strabismus.
- Careful cover testing and binocular function assessment prevent errors.
- Over-treatment:
- Not all DVDs require surgery; unnecessary procedures may risk overcorrection or induce vertical imbalance.
- Ignoring amblyopia:
- Failure to address coexisting amblyopia may compromise visual outcomes.
- Underestimating psychosocial impact:
- Even if vision is preserved, visible ocular drift can affect childhood self-esteem and social interactions, necessitating timely counseling or surgical correction.[4]
Prevention and Early Recognition
- Early detection of infantile esotropia and proper management (spectacles, strabismus surgery, amblyopia therapy) may reduce the severity of DVD later in life.
- Regular follow-up after esotropia surgery is essential, as DVD often emerges or becomes more obvious postoperatively.
- Parental education helps in early reporting and monitoring of eye drifting behavior.[104]
Other Considerations
- Surgical outcomes: Even after superior rectus recession or inferior oblique anterior transposition, residual or recurrent DVD is common but usually milder.
- Fusion maldevelopment nystagmus syndrome: DVD should be considered part of this broader syndrome, which often coexists with latent nystagmus.
- Long-term outlook: DVD rarely causes functional disability but requires attention for cosmetic, psychosocial, and amblyopia-related concerns.[35]
DVD is a distinctive strabismus entity characterized by dissociated, slow upward drift. While benign in most cases, careful diagnosis prevents confusion with other vertical deviations, and management must balance observation with surgical intervention when warranted. Addressing amblyopia, psychosocial impact, and long-term follow-up are equally important in achieving comprehensive care.[104]
Enhancing Healthcare Team Outcomes
Evaluating the patient with DVS requires an interprofessional approach, involving clinicians, orthoptists, nurses, pharmacists, and ophthalmic technicians. The interprofessional health staff will be able to guide the patient and help them through the choice of management, ensure compliance with patching, monitor them regularly, and make better decisions for surgical intervention. They will be well-versed in postoperative care and have instructions on correctly administering eye drops. They will also explain to the patient/parents about the red-flag symptoms to be aware of and the need to contact the team should they develop them. They will be part of the patient follow-up in an outpatient setting, assisting with visual acuity and orthoptic assessments on regular follow-up visits.[4]
Role of the Clinician/Pediatric Ophthalmologist
- The team leader is responsible for diagnosis, clinical decision-making, and overall care planning.
- They differentiate DVD from other vertical strabismus conditions and determine the need for conservative versus surgical intervention.
- They provide surgical expertise when indicated (superior rectus recession, inferior oblique weakening, or combined procedures).
- They coordinate with allied health staff for amblyopia therapy, orthoptic support, and postoperative monitoring.[104]
Orthoptists
- These specialists play a crucial role in clinical evaluation and functional testing: cover tests, prism measurements, ocular motility assessment, binocular function, and stereopsis testing.
- They guide amblyopia therapy, patching regimens, and monitor adherence.
- They provide orthoptic exercises where applicable to maximize fusional amplitudes.
- They assist in long-term follow-up and early detection of residual or recurrent DVD.[33]
Nurses
- Nurses provide perioperative and postoperative support.
- They educate families on eye drop instillation techniques, wound hygiene, and activity restrictions.
- They reinforce the importance of follow-up visits and ensure medication adherence.
- They act as a first point of contact for parental queries regarding eye redness, pain, or unexpected ocular drift after surgery [30]
Pharmacists
- Pharmacists are important in ensuring safe dispensing and counseling of topical and systemic medications (antibiotics, steroids, lubricants)
- They review potential drug interactions and side effects, particularly in children on systemic therapy for other comorbidities.
- They also reinforce compliance by explaining dosing schedules and storage instructions in parent-friendly language.[4]
Ophthalmic Technicians/Optometrists
- These specialists perform visual acuity testing, refraction, and fundus photography when needed.
- They support orthoptists in prism cover testing and motility charting.
- They provide technical assistance in diagnostic imaging (optical coherence tomography, fundus torsion documentation).[105]
Interprofessional Communication and Coordination
- Regular team meetings and shared documentation ensure continuity of care.
- Electronic health records facilitate shared notes and treatment updates.
- Parents are actively included as partners in care, reinforcing home-based amblyopia therapy and monitoring red-flag symptoms (sudden increase in deviation, diplopia, persistent redness).[4]
Patient Safety and Outcomes
- Early amblyopia treatment improves visual prognosis.
- Multidisciplinary postoperative care reduces the risk of complications, improves healing, and enhances satisfaction.
- Coordinated team-based management ensures timely surgical intervention, prevents unnecessary delays, and addresses psychosocial concerns.
Management of DVD benefits from a well-coordinated interprofessional team involving pediatric ophthalmologists, orthoptists, nurses, pharmacists, optometrists, and technicians. Each member contributes unique skills—from diagnostic precision and amblyopia therapy to safe medication use and family education. This team-based model enhances patient-centered care, safety, adherence, and long-term outcomes, ensuring functional and cosmetic success.[106]
Media
(Click Image to Enlarge)

Exotropia (20 degrees) and Hypertropia (10 degrees), Left Eye. This image shows a patient with 20-degree exotropia and 10-degree hypertropia in the left eye in primary gaze. Additionally, the alternate cover test revealed right eye 20-degree exotropia with no vertical deviation, suggesting an alternate exotropia in both eyes, with left eye dissociated vertical deviation.
Contributed by K Kaur, MD
(Click Image to Enlarge)
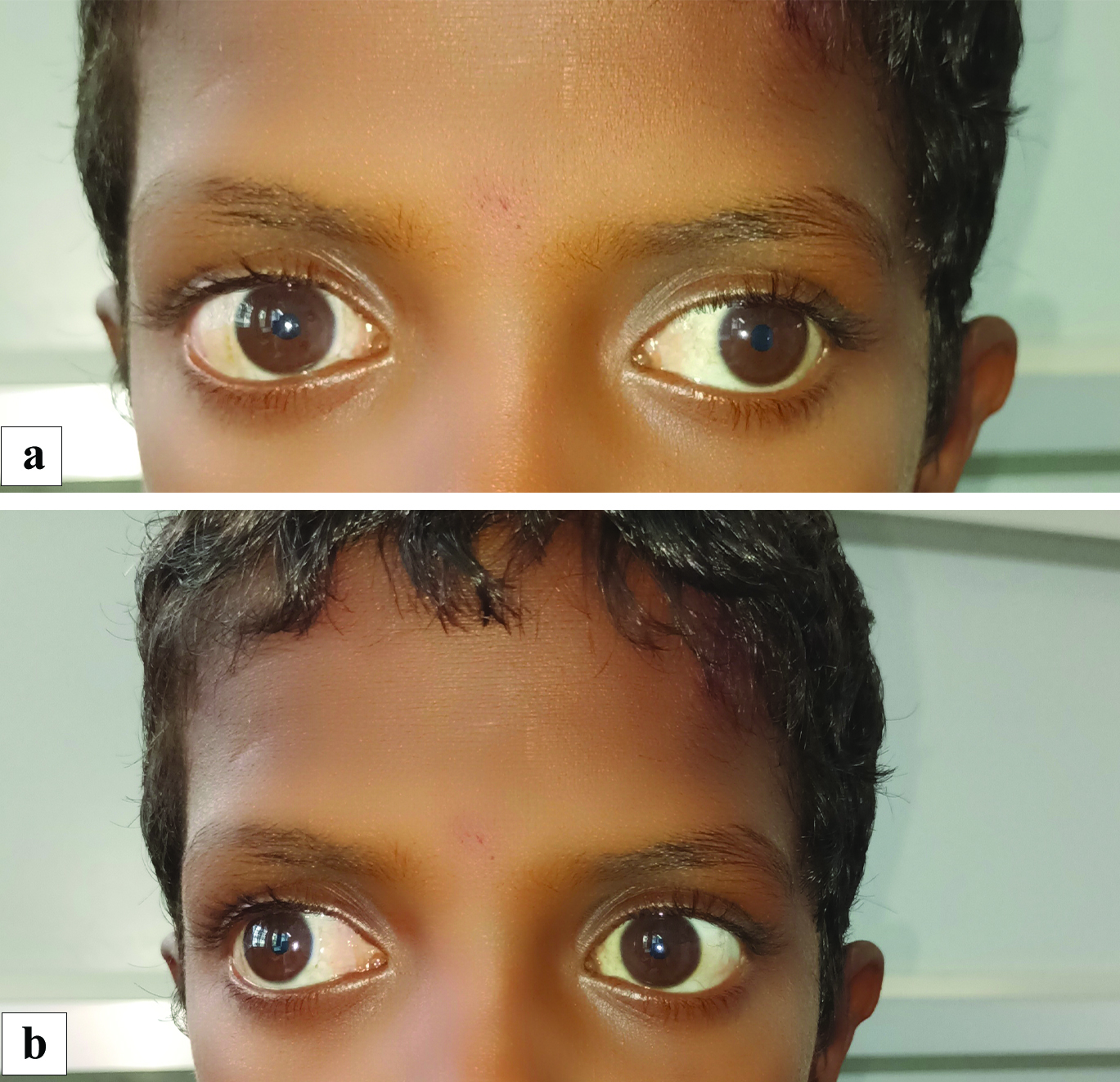
Bilateral Exotropia. This image shows: (a) a child depicting a 30° exotropia in the left eye while fixating with the right eye in primary gaze, and (b) a child showing a 30° exotropia with minimal 5° hypertropia of the right eye while fixating with the left eye in primary gaze, suggestive of an alternate exotropia with right eye dissociated vertical deviation.
Contributed by K Kaur, MD
(Click Image to Enlarge)
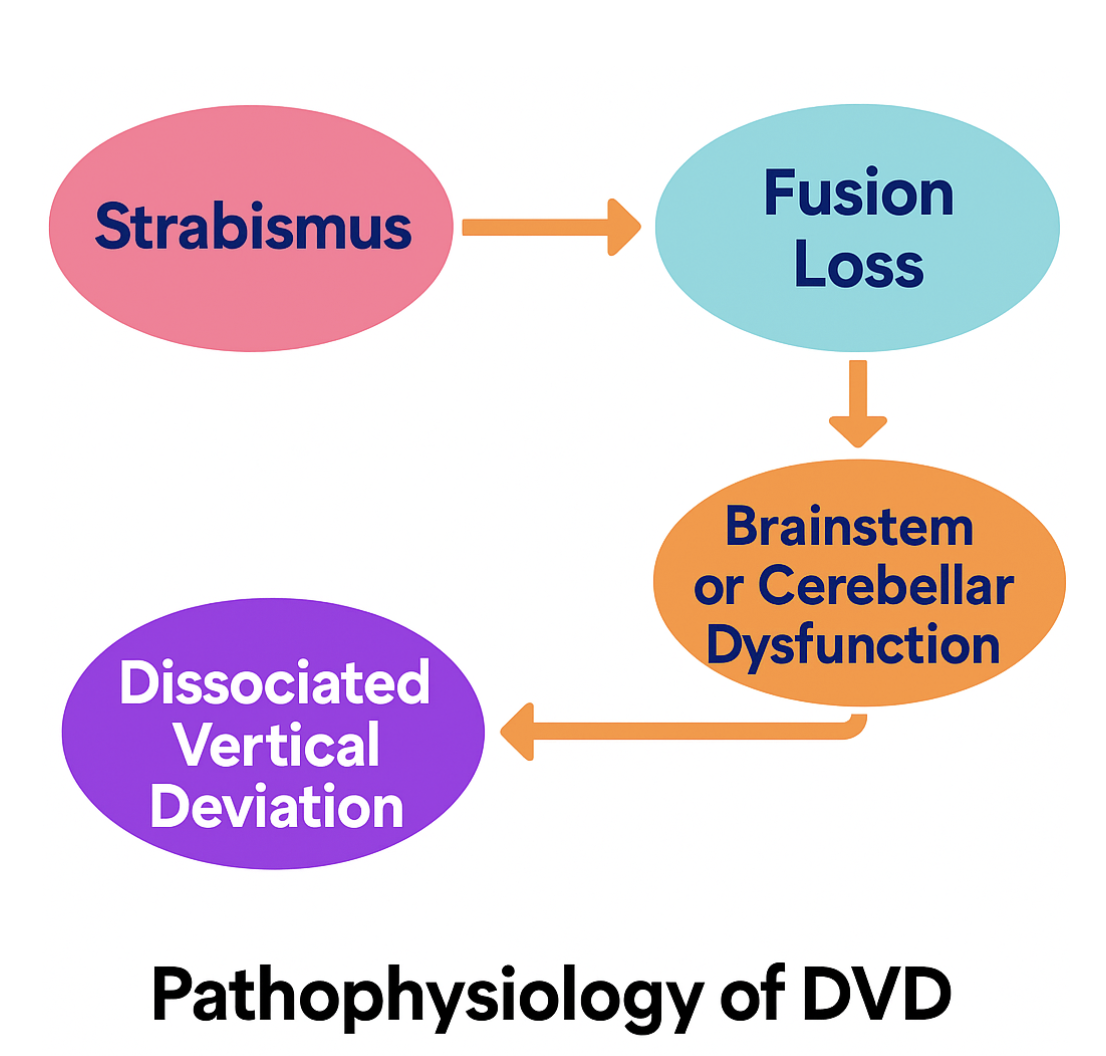
Dissociated Vertical Deviation, Pathophysiology. The exact mechanism of this condition remains incompletely understood; however, several theories have been proposed, focusing on abnormal binocular development, disruption of fusion, and aberrant vertical vergence control.
Contributed by K Kaur, MD
(Click Image to Enlarge)
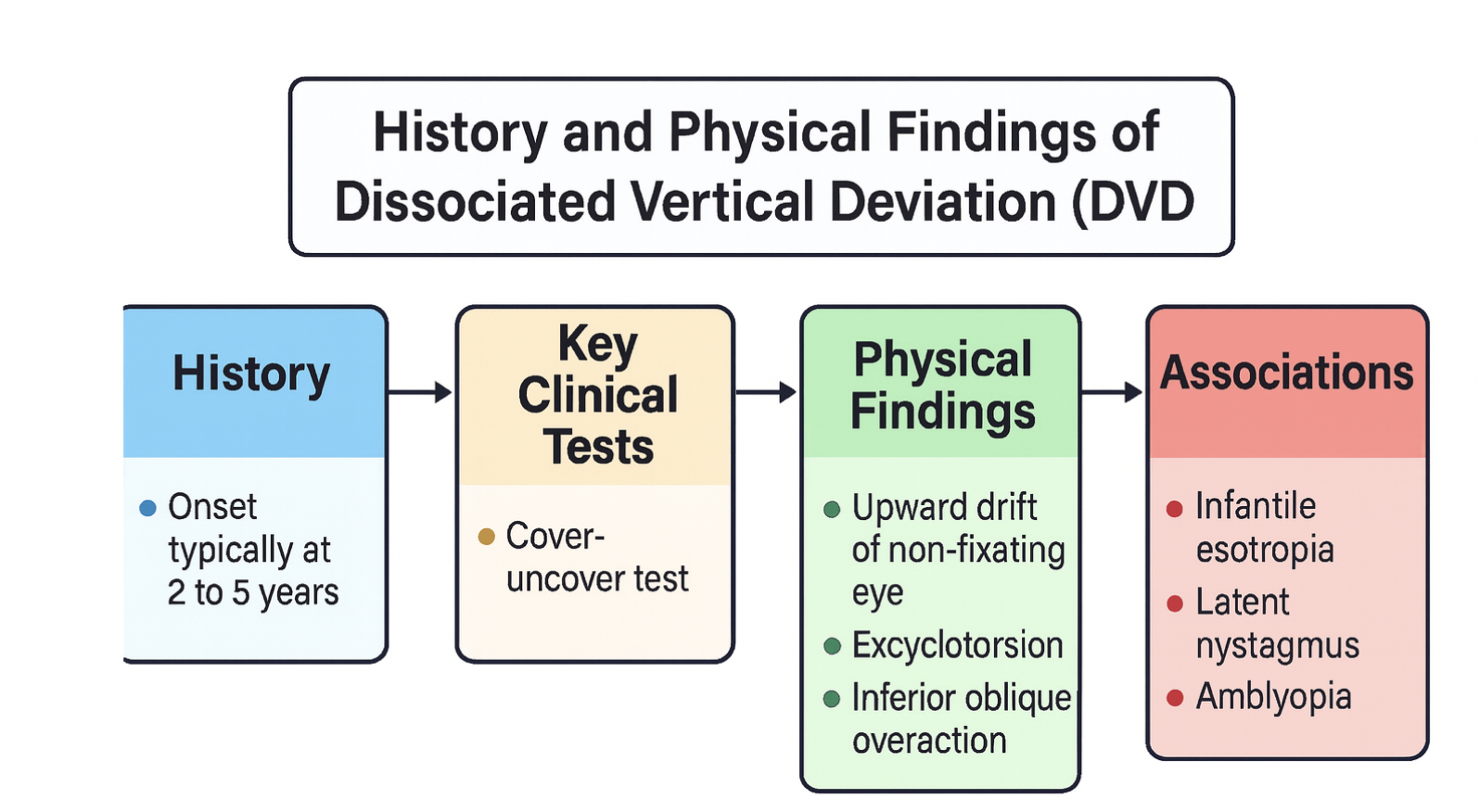
Dissociated Vertical Deviation, History and Physical Findings. This condition is primarily a functional supranuclear disorder rather than a structural lesion. Unlike diseases with clear histopathologic tissue changes, DVD reflects abnormal neurophysiological control of ocular alignment resulting from the defective development of binocular vision pathways in infancy.
Contributed by K Kaur, MD
(Click Image to Enlarge)
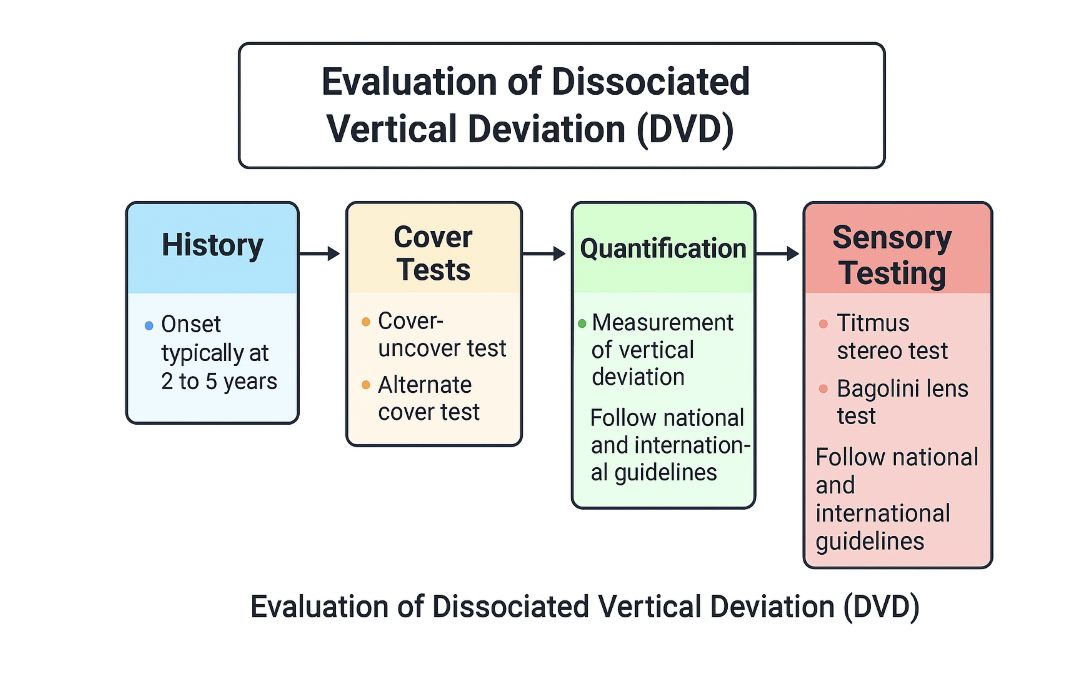
Evaluation Pattern of Dissociated Vertical Deviation. This image is a schematic drawing of the dissociated vertical deviation evaluation pattern, which includes history, cover tests, quantification, and sensory testing.
Contributed by B Gurnani, MD
References
Brodsky MC. DVD remains a moving target! Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 1999 Dec:3(6):325-7 [PubMed PMID: 10613573]
Level 3 (low-level) evidenceHelveston EM. Dissociated vertical deviation-a clinical and laboratory study. Transactions of the American Ophthalmological Society. 1980:78():734-79 [PubMed PMID: 7020216]
Level 3 (low-level) evidenceManta AI, Demer JL, Goldberg RA. Magnetic Resonance Imaging Demonstrates Differences in Brow and Upper Eyelid Fat and Muscle Layers Between East Asians and Caucasians. Ophthalmic plastic and reconstructive surgery. 2025 Sep-Oct 01:41(5):535-538. doi: 10.1097/IOP.0000000000002904. Epub 2025 Jan 16 [PubMed PMID: 40919988]
Shamsher E, Saccaro L, Pungirum VB, Tran NB, Alghaith OAHA, Khabazianzadeh F, Bridge H, Ip IB. Selective serotonin reuptake inhibitors for amblyopia treatment: a systematic review and meta-analysis of randomized controlled trials. Frontiers in neurology. 2025:16():1639913. doi: 10.3389/fneur.2025.1639913. Epub 2025 Aug 21 [PubMed PMID: 40917656]
Level 1 (high-level) evidenceGraham C, Gurnani B, Mohseni M. Abducens Nerve Palsy. StatPearls. 2026 Jan:(): [PubMed PMID: 29489275]
Lee YJ, Lee HJ, Kim SJ. Clinical Features of Duane Retraction Syndrome: A New Classification. Korean journal of ophthalmology : KJO. 2020 Apr:34(2):158-165. doi: 10.3341/kjo.2019.0100. Epub [PubMed PMID: 32233150]
Feyissa M, Bowman R, Theodorou M. Trends in paediatric visual impairment in England and Wales: a retrospective study (2009-2022). Eye (London, England). 2025 Oct:39(15):2815-2821. doi: 10.1038/s41433-025-03979-9. Epub 2025 Sep 5 [PubMed PMID: 40913077]
Level 2 (mid-level) evidenceKocamaz M, Aygit ED, Inal A, Ocak OB, Cicek U, Gokyigit B. Duane Retraction Syndrome and Accompanying Ocular Abnormalities. Beyoglu eye journal. 2019:4(1):28-31. doi: 10.14744/bej.2019.36854. Epub 2019 Feb 20 [PubMed PMID: 35187428]
Akbari MR, Manouchehri V, Mirmohammadsadeghi A. Surgical treatment of Duane retraction syndrome. Journal of current ophthalmology. 2017 Dec:29(4):248-257. doi: 10.1016/j.joco.2017.08.008. Epub 2017 Sep 11 [PubMed PMID: 29270470]
Sen S, Singh P, Saxena R. Management of amblyopia in pediatric patients: Current insights. Eye (London, England). 2022 Jan:36(1):44-56. doi: 10.1038/s41433-021-01669-w. Epub 2021 Jul 7 [PubMed PMID: 34234293]
Kelly KR, Jost RM, Wang YZ, Dao L, Beauchamp CL, Leffler JN, Birch EE. Improved Binocular Outcomes Following Binocular Treatment for Childhood Amblyopia. Investigative ophthalmology & visual science. 2018 Mar 1:59(3):1221-1228. doi: 10.1167/iovs.17-23235. Epub [PubMed PMID: 29625442]
March de Ribot F, March de Ribot A, Visa J. Marcus Gunn jaw winking associated with Duane's retraction syndrome. Strabismus. 2026 Jun:34(2):223-226. doi: 10.1080/09273972.2025.2557260. Epub 2025 Sep 5 [PubMed PMID: 40908837]
Cotter SA, Varma R, Tarczy-Hornoch K, McKean-Cowdin R, Lin J, Wen G, Wei J, Borchert M, Azen SP, Torres M, Tielsch JM, Friedman DS, Repka MX, Katz J, Ibironke J, Giordano L, Joint Writing Committee for the Multi-Ethnic Pediatric Eye Disease Study and the Baltimore Pediatric Eye Disease Study Groups. Risk factors associated with childhood strabismus: the multi-ethnic pediatric eye disease and Baltimore pediatric eye disease studies. Ophthalmology. 2011 Nov:118(11):2251-61. doi: 10.1016/j.ophtha.2011.06.032. Epub 2011 Aug 19 [PubMed PMID: 21856012]
Eggers SDZ, Bisdorff A, von Brevern M, Zee DS, Kim JS, Perez-Fernandez N, Welgampola MS, Della Santina CC, Newman-Toker DE. Classification of vestibular signs and examination techniques: Nystagmus and nystagmus-like movements. Journal of vestibular research : equilibrium & orientation. 2019:29(2-3):57-87. doi: 10.3233/VES-190658. Epub [PubMed PMID: 31256095]
Irsch K, Guyton DL, Ramey NA, Adyanthaya RS, Ying HS. Vertical vergence adaptation produces an objective vertical deviation that changes with head tilt. Investigative ophthalmology & visual science. 2013 May 3:54(5):3108-14. doi: 10.1167/iovs.12-11368. Epub 2013 May 3 [PubMed PMID: 23572100]
Shinde A, Warkad VU. Esotropia-hypertropia complex in myopic strabismus fixus managed with an unconventional loop myopexy. BMJ case reports. 2025 Sep 3:18(9):. pii: e263663. doi: 10.1136/bcr-2024-263663. Epub 2025 Sep 3 [PubMed PMID: 40903093]
Level 3 (low-level) evidenceGuyton DL. Dissociated vertical deviation: etiology, mechanism, and associated phenomena. Costenbader Lecture. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2000 Jun:4(3):131-44 [PubMed PMID: 10849388]
Cherfan CG, Diehl NN, Mohney BG. Prevalence of dissociated strabismus in children with ocular misalignment: a population-based study. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2014 Aug:18(4):374-7. doi: 10.1016/j.jaapos.2014.04.002. Epub 2014 Aug 1 [PubMed PMID: 25087642]
Level 2 (mid-level) evidenceKutluk S, Avilla CW, von Noorden GK. The prevalence of dissociated vertical deviation in patients with sensory heterotropia. American journal of ophthalmology. 1995 Jun:119(6):744-7 [PubMed PMID: 7785688]
Level 2 (mid-level) evidenceKrahenbuhl GS, Constable SH, Darst PW, Marett JR, Reid GB, Reuther LC. Catecholamine excretion in A-10 pilots. Aviation, space, and environmental medicine. 1980 Jul:51(7):661-4 [PubMed PMID: 7417130]
Level 3 (low-level) evidenceRepka MX, Lum F, Li C, Saseendrakumar BR. Strabismus and Strabismus Surgery Reoperation Rates at 1, 3, and 5 years: Analyses from the IRIS® Registry (Intelligent Research in Sight). Ophthalmology. 2025 Sep 2:():. pii: S0161-6420(25)00538-X. doi: 10.1016/j.ophtha.2025.08.028. Epub 2025 Sep 2 [PubMed PMID: 40907579]
Lee JJ, Patil N, Schimmel T, Benson MD, DeSerres JJ. Acquired Brown Syndrome as a Postoperative Complication of Orbital Wall Fracture Repair with Metallic Mesh. Plastic surgery (Oakville, Ont.). 2025 Aug 29:():22925503251371048. doi: 10.1177/22925503251371048. Epub 2025 Aug 29 [PubMed PMID: 40895464]
Brodsky MC. Dissociated vertical divergence: a righting reflex gone wrong. Archives of ophthalmology (Chicago, Ill. : 1960). 1999 Sep:117(9):1216-22 [PubMed PMID: 10496394]
Level 3 (low-level) evidenceGuyton DL. Dissociated vertical deviation: an acquired nystagmus-blockage phenomenon. The American orthoptic journal. 2004:54():77-87. doi: 10.3368/aoj.54.1.77. Epub [PubMed PMID: 21149089]
ten Tusscher MP, van Rijn RJ. A hypothetical mechanism for DVD: unbalanced cortical input to subcortical pathways. Strabismus. 2010 Sep:18(3):98-103. doi: 10.3109/09273972.2010.502956. Epub [PubMed PMID: 20843186]
Level 3 (low-level) evidenceBui Quoc E, Milleret C. Origins of strabismus and loss of binocular vision. Frontiers in integrative neuroscience. 2014:8():71. doi: 10.3389/fnint.2014.00071. Epub 2014 Sep 25 [PubMed PMID: 25309358]
Rickels KL, Chauhan MZ, Dagi LR, Rageh A, Oke I, Phillips PH, Elhusseiny AM. Incidence of Strabismus in Childhood Glaucoma. Ophthalmology science. 2025 Nov-Dec:5(6):100892. doi: 10.1016/j.xops.2025.100892. Epub 2025 Jul 23 [PubMed PMID: 40893618]
Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, Ballout RA, El-Hattab AW, Schaaf CP, Cheung SW. Xq28 Duplication Syndrome, Int22h1/Int22h2 Mediated. GeneReviews(®). 1993:(): [PubMed PMID: 26962617]
Mouhcine Y, Lahjouji O, Ouazzani H, Chaouche I, Akammar A, Bouardi NE, Alami B, Lamrani YA, Maaroufi M, Boubbou M. Pituitary apoplexy within a prolactin-secreting macroadenoma in a child: A rare clinical entity with radiological correlation. Radiology case reports. 2025 Nov:20(11):5583-5589. doi: 10.1016/j.radcr.2025.07.066. Epub 2025 Aug 16 [PubMed PMID: 40895003]
Level 3 (low-level) evidenceWang YM, Liu J, Chen WW, Jiang MX, Liu XX, Fu J. Accuracy of a system combining virtual reality and artificial intelligence for screening pediatric strabismus. Digital health. 2025 Jan-Dec:11():20552076251374129. doi: 10.1177/20552076251374129. Epub 2025 Aug 26 [PubMed PMID: 40881061]
Lino P, de Aguiar PV, Cunha JP. Success of Strabismus Surgery in Intermittent Exotropia. Journal of personalized medicine. 2025 Jul 30:15(8):. doi: 10.3390/jpm15080333. Epub 2025 Jul 30 [PubMed PMID: 40863395]
Meng Q, Parunakian E, Yehezkeli V, Demer JL. Surgical Dosing for Correction of Consecutive Exotropia. American journal of ophthalmology. 2025 Aug 25:280():176-181. doi: 10.1016/j.ajo.2025.08.025. Epub 2025 Aug 25 [PubMed PMID: 40865896]
Yang Y, Hou J, Huang H, Wei C, Chen J, Wu T, Liu J, Deng D, Ling S, Yang W, Yan J, Chang S, Yu X. Reading ability in children with intermittent exotropia and its association with binocular visual function and visual information processing capability. BMC ophthalmology. 2025 Sep 1:25(1):497. doi: 10.1186/s12886-025-04326-y. Epub 2025 Sep 1 [PubMed PMID: 40890623]
Arslan U, Atilla H, Erkam N. Dissociated vertical deviation and its relationship with time and type of surgery in infantile esotropia. The British journal of ophthalmology. 2010 Jun:94(6):740-2. doi: 10.1136/bjo.2008.157016. Epub [PubMed PMID: 20508049]
Level 2 (mid-level) evidenceMarra KV, Chen JS, Nudleman E, Robbins SL. Review of Retinopathy of Prematurity Management in the Anti-VEGF Era: Evolving Global Paradigms, Persistent Challenges and Our AI-Assisted Future. Clinical & experimental ophthalmology. 2025 Sep 4:():. doi: 10.1111/ceo.14598. Epub 2025 Sep 4 [PubMed PMID: 40908574]
Alagha P, Akhtarkhavari T, Shokouhian E, Ghodratpour F, Arzhangi S, Najmabadi H, Kahrizi K. Investigation of the Clinical and Genetic Spectrum of PMM2-CDG: Insights from a Family with a Novel Variant and Previous Studies. Archives of Iranian medicine. 2025 Jul 1:28(7):387-397. doi: 10.34172/aim.34187. Epub 2025 Jul 1 [PubMed PMID: 40886090]
Sachdeva V, Vepakomma T, Chandrasekharan A, Kekunnaya R. Clinical profile and surgical outcomes of Duane syndrome with primary position hypertropia with or without coexisting horizontal deviation. Strabismus. 2025 Aug 28:():1-8. doi: 10.1080/09273972.2025.2527960. Epub 2025 Aug 28 [PubMed PMID: 40874383]
Peli E, McCormack G. Dynamics of cover test eye movements. American journal of optometry and physiological optics. 1983 Aug:60(8):712-24 [PubMed PMID: 6624871]
Lee T, Leung M, van Boxtel JJA, Boon MY. The Effects of Refractive Imbalance on Binocular Vision Status, Reading Performance, and Vision-Related Reading Difficulty Symptoms in Expert Readers. Investigative ophthalmology & visual science. 2025 Jul 1:66(9):15. doi: 10.1167/iovs.66.9.15. Epub [PubMed PMID: 40622213]
Ozsoy E, Gunduz A, Ozturk E. Inferior Oblique Muscle Overaction: Clinical Features and Surgical Management. Journal of ophthalmology. 2019:2019():9713189. doi: 10.1155/2019/9713189. Epub 2019 Jul 17 [PubMed PMID: 31396413]
Wright KW, Matsumoto E, Edelman PM. Binocular fusion and stereopsis associated with early surgery for monocular congenital cataracts. Archives of ophthalmology (Chicago, Ill. : 1960). 1992 Nov:110(11):1607-9 [PubMed PMID: 1444921]
von Noorden GK, Avilla C, Sidikaro Y, LaRoche R. Latent nystagmus and strabismic amblyopia. American journal of ophthalmology. 1987 Jan 15:103(1):87-9 [PubMed PMID: 3799793]
Kassavetis P, Kaski D, Anderson T, Hallett M. Eye Movement Disorders in Movement Disorders. Movement disorders clinical practice. 2022 Apr:9(3):284-295. doi: 10.1002/mdc3.13413. Epub 2022 Feb 16 [PubMed PMID: 35402641]
Kaur K, Gurnani B. Esotropia. StatPearls. 2026 Jan:(): [PubMed PMID: 35201735]
Hull S, Tailor V, Balduzzi S, Rahi J, Schmucker C, Virgili G, Dahlmann-Noor A. Tests for detecting strabismus in children aged 1 to 6 years in the community. The Cochrane database of systematic reviews. 2017 Nov 6:11(11):CD011221. doi: 10.1002/14651858.CD011221.pub2. Epub 2017 Nov 6 [PubMed PMID: 29105728]
Level 1 (high-level) evidenceWong AM. Understanding skew deviation and a new clinical test to differentiate it from trochlear nerve palsy. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2010 Feb:14(1):61-7. doi: 10.1016/j.jaapos.2009.11.019. Epub [PubMed PMID: 20227626]
Level 3 (low-level) evidenceElghonemy AM, Attia FS, Brodsky MC. Mechanisms for Positive Bielschowsky Head Tilt Testing in Horizontal Strabismus. Journal of binocular vision and ocular motility. 2024 Apr-Jun:74(2):69-74. doi: 10.1080/2576117X.2024.2325919. Epub 2024 Apr 24 [PubMed PMID: 38656210]
Yoo HS, Park E, Rhiu S, Chang HJ, Kim K, Yoo J, Heo JH, Nam HS. A computerized red glass test for quantifying diplopia. BMC ophthalmology. 2017 May 17:17(1):71. doi: 10.1186/s12886-017-0465-8. Epub 2017 May 17 [PubMed PMID: 28514951]
Klaehn LD, Hatt SR, Leske DA, Holmes JM. Role of a Standardized Prism Under Cover Test in the Assessment of Dissociated Vertical Deviation. Strabismus. 2018 Mar:26(1):1-5. doi: 10.1080/09273972.2017.1391850. Epub 2018 Feb 2 [PubMed PMID: 29393712]
Hatt SR, Wang X, Holmes JM. Interventions for dissociated vertical deviation. The Cochrane database of systematic reviews. 2015 Nov 20:2015(11):CD010868. doi: 10.1002/14651858.CD010868.pub2. Epub 2015 Nov 20 [PubMed PMID: 26587695]
Level 1 (high-level) evidenceSharma M, Ganjoo S, Ganesh S. Occurrence and subsequent development of vertical deviations in patients treated surgically for infantile esotropia. Indian journal of ophthalmology. 2023 Jul:71(7):2835-2840. doi: 10.4103/IJO.IJO_2777_22. Epub [PubMed PMID: 37417130]
Li T, Zhou X, Zhu J, Tang X, Gu X. Effect of cycloplegia on the measurement of refractive error in Chinese children. Clinical & experimental optometry. 2019 Mar:102(2):160-165. doi: 10.1111/cxo.12829. Epub 2018 Aug 22 [PubMed PMID: 30136309]
Arnold RW, Donahue SP, Silbert DI, Longmuir SQ, Bradford GE, Peterseim MMW, Hutchinson AK, O'Neil JW, de Alba Campomanes AG, Pineles SL, AAPOS Vision Screening and Research Committees. AAPOS uniform guidelines for instrument-based pediatric vision screen validation 2021. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2022 Feb:26(1):1.e1-1.e6. doi: 10.1016/j.jaapos.2021.09.009. Epub 2022 Jan 20 [PubMed PMID: 35066152]
Level 1 (high-level) evidenceYue YY, Zhao KX, Ma HZ, Hua N, Wang LJ. [Treatment of dissociated vertical deviation by shifting fixating eye]. [Zhonghua yan ke za zhi] Chinese journal of ophthalmology. 2003 Dec:39(12):724-6 [PubMed PMID: 14769222]
McNeer KW. Botulinum toxin injection into the superior rectus muscle of the non-dominant eye for dissociated vertical deviation. Journal of pediatric ophthalmology and strabismus. 1989 Jul-Aug:26(4):162-4 [PubMed PMID: 2760787]
Strominger MB, Rogers GL, Wagner RS. Dissociated vertical deviation and inferior oblique overaction. Journal of pediatric ophthalmology and strabismus. 2009 May-Jun:46(3):132-6 [PubMed PMID: 19496491]
Nelson LB. Anterior transposition of the inferior oblique for dissociated vertical deviation. Journal of pediatric ophthalmology and strabismus. 2007 May-Jun:44(3):152 [PubMed PMID: 17542435]
Wong CY, Ng JS, Goh TY. Combined resection and anterior transposition of the inferior oblique muscle for the treatment of moderate to large dissociated vertical deviation associated with inferior oblique muscle overaction. Journal of pediatric ophthalmology and strabismus. 2003 Jul-Aug:40(4):194-5 [PubMed PMID: 12908529]
Level 3 (low-level) evidenceBroniarczyk-Loba A, Nowakowska O, Loba P. [Difficulties in diagnosis and treatment of dissociated vertical deviation (DVD). Part II--own experiences]. Klinika oczna. 2007:109(7-9):292-6 [PubMed PMID: 18260282]
Schwartz T, Scott W. Unilateral superior rectus recession for the treatment of dissociated vertical deviation. Journal of pediatric ophthalmology and strabismus. 1991 Jul-Aug:28(4):219-22 [PubMed PMID: 1919970]
Kii T, Ogasawara K, Ohba M, Hotsubo M, Sakai N, Nakagawa T. [The effectiveness of the Faden operation on the superior rectus muscle combined with recession of the muscle for the treatment of dissociated vertical deviation]. Nippon Ganka Gakkai zasshi. 1994 Jan:98(1):98-102 [PubMed PMID: 8109453]
Level 2 (mid-level) evidenceNoel LP, Parks MM. Dissociated vertical deviation: associated findings and results of surgical treatment. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 1982 Feb:17(1):10-2 [PubMed PMID: 7083051]
Stager DR Sr, Beauchamp GR, Stager DR Jr. Anterior and nasal transposition of the inferior oblique muscle: a preliminary case report on a new procedure. Binocular vision & strabismus quarterly. 2001:16(1):43-4 [PubMed PMID: 11240936]
Level 3 (low-level) evidenceArroyo-Yllanes ME, Escanio-Cortés ME, Pérez-Pérez JF, Murillo-Murillo L. [Unilateral tucking of the inferior rectus muscle for dissociated vertical deviation]. Cirugia y cirujanos. 2007 Jan-Feb:75(1):7-12 [PubMed PMID: 17470318]
Gamio S. A surgical alternative for dissociated vertical deviation based on new pathologic concepts: weakening all four oblique eye muscles. Outcome and results in 9 cases. Binocular vision & strabismus quarterly. 2002:17(1):15-24 [PubMed PMID: 11874379]
Level 3 (low-level) evidenceMravicic I, Gulic MP, Barisic A, Biscevic A, Pjano MA, Pidro A. Different Surgical Approaches for Treatment of Dissociated Vertical Deviation (DVD). Medical archives (Sarajevo, Bosnia and Herzegovina). 2019 Dec:73(6):386-390. doi: 10.5455/medarh.2019.73.386-390. Epub [PubMed PMID: 32082005]
Yen MY. Therapy for Amblyopia: A newer perspective. Taiwan journal of ophthalmology. 2017 Apr-Jun:7(2):59-61. doi: 10.4103/tjo.tjo_56_17. Epub [PubMed PMID: 29018758]
Level 3 (low-level) evidenceTibrewal S, Nguyen PTT, Ganesh S, Molinari A. Bilateral Symmetric and Asymmetric Superior Rectus Recession for Patients with Dissociated Vertical Deviation. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2019 May-Jun:8(3):218-223. doi: 10.22608/APO.2018415. Epub 2019 May 15 [PubMed PMID: 31090282]
Aghdam KA, Asadi R, Sanjari MS, Sadeghi A, Razavi M. Comparing Two Inferior Oblique Weakening Procedures: Disinsertion versus Myectomy. Journal of ophthalmic & vision research. 2021 Apr-Jun:16(2):212-218. doi: 10.18502/jovr.v16i2.9085. Epub 2021 Apr 29 [PubMed PMID: 34055259]
Bothun ED, Summers CG. Unilateral inferior oblique anterior transposition for dissociated vertical deviation. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2004 Jun:8(3):259-63 [PubMed PMID: 15226728]
Witmanowski H, Błochowiak K. The whole truth about botulinum toxin - a review. Postepy dermatologii i alergologii. 2020 Dec:37(6):853-861. doi: 10.5114/ada.2019.82795. Epub 2019 Feb 5 [PubMed PMID: 33603602]
Loba P, Broniarczyk-Loba A. [Difficulties in diagnosis and treatment of dissociated vertical deviation (DVD). Part I]. Klinika oczna. 2007:109(7-9):356-8 [PubMed PMID: 18260298]
Brodsky MC, Donahue SP, Vaphiades M, Brandt T. Skew deviation revisited. Survey of ophthalmology. 2006 Mar-Apr:51(2):105-28 [PubMed PMID: 16500212]
Level 3 (low-level) evidenceDonahue SP, Lavin PJ, Mohney B, Hamed L. Skew deviation and inferior oblique palsy. American journal of ophthalmology. 2001 Nov:132(5):751-6 [PubMed PMID: 11704037]
Cruz Rivera S, McMullan C, Jones L, Kyte D, Slade A, Calvert M. The impact of patient-reported outcome data from clinical trials: perspectives from international stakeholders. Journal of patient-reported outcomes. 2020 Jul 2:4(1):51. doi: 10.1186/s41687-020-00219-4. Epub 2020 Jul 2 [PubMed PMID: 32617713]
Level 3 (low-level) evidenceHeydarian S, Hashemi H, Jafarzadehpour E, Ostadi A, Yekta A, Aghamirsalim M, Dadbin N, Ostadimoghaddam H, Khoshhal F, Khabazkhoob M. Non-surgical Management Options of Intermittent Exotropia: A Literature Review. Journal of current ophthalmology. 2020 Jul-Sep:32(3):217-225. doi: 10.4103/JOCO.JOCO_81_20. Epub 2020 Jul 4 [PubMed PMID: 32775794]
Can D, Ozkan SB, Kasim R, Duman S. Surgical results in highly asymmetric dissociated vertical deviations. Strabismus. 1997:5(1):21-6. doi: 10.3109/09273979709055055. Epub [PubMed PMID: 21314390]
Parkash RO, Gurnani B, Kaur K, Parkash TO, Sharma T. Assessing the validity of flap motility sign in predicting the extent of anterior capsular tears in phacoemulsification. Indian journal of ophthalmology. 2023 Aug:71(8):3095-3099. doi: 10.4103/IJO.IJO_2552_22. Epub [PubMed PMID: 37530287]
Younan MH, Youssef YT, Erum U, Nasir MT, Ismaeil M, Aziz M, Fawzy VN, Mourad N, Ismaiel M, Ahmed MSA, Melad L, Abdelglil M. Evolving Strategies in Amblyopia Management: From Traditional Therapies to Cutting-Edge Innovations. Cureus. 2025 Jul:17(7):e88012. doi: 10.7759/cureus.88012. Epub 2025 Jul 15 [PubMed PMID: 40821151]
Lembo A, Serafino M, Villani E, Nucci P. Unilateral Surgery in Bilateral Asymmetrical Dissociated Vertical Deviation With Strong Preferential Fixation. Journal of pediatric ophthalmology and strabismus. 2022 Jan-Feb:59(1):60-64. doi: 10.3928/01913913-20210708-06. Epub 2021 Sep 30 [PubMed PMID: 34592873]
Kaur K, Gurnani B. Dissociated Vertical Deviation. StatPearls. 2026 Jan:(): [PubMed PMID: 34424634]
Osama G, Elhilali H, Salah M, Fouad HM. Anteriorization of the inferior oblique muscle versus anteriorization and resection for asymmetrical dissociated vertical deviation. Strabismus. 2025 Mar:33(1):28-35. doi: 10.1080/09273972.2024.2402925. Epub 2024 Sep 19 [PubMed PMID: 39295544]
Zubcov AA, Goldstein HP, Reinecke RD. Dissociated vertical deviation (DVD): The saccadic and slow eye movements. Strabismus. 1994:2(1):1-11. doi: 10.3109/09273979409105048. Epub [PubMed PMID: 21314545]
Ohlsson J, Baumann M, Sjöstrand J, Abrahamsson M. Long term visual outcome in amblyopia treatment. The British journal of ophthalmology. 2002 Oct:86(10):1148-51 [PubMed PMID: 12234897]
Varn MM, Saunders RA, Wilson ME. Combined bilateral superior rectus muscle recession and inferior oblique muscle weakening for dissociated vertical deviation. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 1997 Sep:1(3):134-7 [PubMed PMID: 10532773]
Gurnani B, Kaur K. Quality of life in patients with keratoconus. Indian journal of ophthalmology. 2022 Aug:70(8):3155. doi: 10.4103/ijo.IJO_927_22. Epub [PubMed PMID: 35919000]
Level 2 (mid-level) evidenceOlitsky SE, Coats DK. Complications of Strabismus Surgery. Middle East African journal of ophthalmology. 2015 Jul-Sep:22(3):271-8. doi: 10.4103/0974-9233.159692. Epub [PubMed PMID: 26180463]
Maconachie GD, Gottlob I. The challenges of amblyopia treatment. Biomedical journal. 2015 Dec:38(6):510-6. doi: 10.1016/j.bj.2015.06.001. Epub 2016 Feb 28 [PubMed PMID: 27013450]
Honigman RJ, Phillips KA, Castle DJ. A review of psychosocial outcomes for patients seeking cosmetic surgery. Plastic and reconstructive surgery. 2004 Apr 1:113(4):1229-37 [PubMed PMID: 15083026]
Abildgaard U, Amtorp O, Hansø S, Rosenkilde P, Sejrsen P. The local xenon washout method applied to the study of blood flow in subcapsular cortex of the canine kidney. Pflugers Archiv : European journal of physiology. 1983 Feb:396(2):182-3 [PubMed PMID: 6835820]
Olteanu AO, Klimko A, Tieranu EN, Bota AD, Preda CM, Tieranu I, Pavel C, Pahomeanu MR, Toma CV, Saftoiu A, Ionescu EM, Tieranu CG. Managing Crohn's Disease Postoperative Recurrence Beyond Prophylaxis: A Comprehensive Review with Meta-Analysis. Biomedicines. 2024 Oct 23:12(11):. doi: 10.3390/biomedicines12112434. Epub 2024 Oct 23 [PubMed PMID: 39595001]
Level 1 (high-level) evidenceMezad-Koursh D, Skaat A, Davidov B, Manaim T, Leshno A. Qualification of non-pediatric ophthalmologists in examining children. European journal of ophthalmology. 2023 Jan:33(1):123-128. doi: 10.1177/11206721221111885. Epub 2022 Jul 6 [PubMed PMID: 35795924]
Wan LQ, Wan XM, Gong HQ, Xie LX. The effects of simultaneous operation on dissociated vertical deviation with horizontal and torsional strabismus. International journal of ophthalmology. 2020:13(4):637-642. doi: 10.18240/ijo.2020.04.17. Epub 2020 Apr 18 [PubMed PMID: 32399417]
Sprunger DT, Lambert SR, Hercinovic A, Morse CL, Repka MX, Hutchinson AK, Cruz OA, Wallace DK, American Academy of Ophthalmology Preferred Practice Pattern Pediatric Ophthalmology/Strabismus Panel. Esotropia and Exotropia Preferred Practice Pattern®. Ophthalmology. 2023 Mar:130(3):P179-P221. doi: 10.1016/j.ophtha.2022.11.002. Epub 2022 Dec 14 [PubMed PMID: 36526451]
Chaturvedi I, Jamil R, Sharma P. Binocular vision therapy for the treatment of Amblyopia-A review. Indian journal of ophthalmology. 2023 May:71(5):1797-1803. doi: 10.4103/IJO.IJO_3098_22. Epub [PubMed PMID: 37203032]
Vijittrakarnrung T, Lekskul A, Preechaharn P, Aramrungroj S, Wuthisiri W. Surgical Outcome of Inferior Oblique Myectomy versus Recession-Anteriorization in the Treatment of Inferior Oblique Overaction. Clinical ophthalmology (Auckland, N.Z.). 2024:18():819-824. doi: 10.2147/OPTH.S454260. Epub 2024 Mar 13 [PubMed PMID: 38504932]
Shainberg MJ. Vision therapy and orthoptics. The American orthoptic journal. 2010:60():28-32 [PubMed PMID: 21061881]
Hailaiti A, Yu X, Yao K, Shentu X. Postoperative amblyopia in children with congenital cataracts: a systematic review and meta-analysis. Italian journal of pediatrics. 2025 May 19:51(1):141. doi: 10.1186/s13052-025-02010-x. Epub 2025 May 19 [PubMed PMID: 40390126]
Level 1 (high-level) evidenceHutchinson AK, Morse CL, Hercinovic A, Cruz OA, Sprunger DT, Repka MX, Lambert SR, Wallace DK, American Academy of Ophthalmology Preferred Practice Pattern Pediatric Ophthalmology/Strabismus Panel. Pediatric Eye Evaluations Preferred Practice Pattern. Ophthalmology. 2023 Mar:130(3):P222-P270. doi: 10.1016/j.ophtha.2022.10.030. Epub 2022 Dec 19 [PubMed PMID: 36543602]
Thokar MA, Malla N, Wattal C. Serological study of patients clinically suspected to have toxoplasmosis in Kashmir. The Indian journal of medical research. 1988 Jul:88():29-34 [PubMed PMID: 3053439]
Shrestha M, Bhandari G, Rathi SK, Gudlavalleti AG, Pandey B, Ghimire R, Ale D, Kayastha S, Chaudhary DS, Byanju R, Operational Research Capacity Building Study Group. Improving the Follow-up Rate for Pediatric Patients (0-16 years) of an Eye Hospital in Nepal: Protocol for a Public Health Intervention Study. JMIR research protocols. 2021 Oct 8:10(10):e31578. doi: 10.2196/31578. Epub 2021 Oct 8 [PubMed PMID: 34521615]
Feng D, Lu C, Cai Q, Lu J. A Study on the Design of Vision Protection Products Based on Children's Visual Fatigue under Online Learning Scenarios. Healthcare (Basel, Switzerland). 2022 Mar 25:10(4):. doi: 10.3390/healthcare10040621. Epub 2022 Mar 25 [PubMed PMID: 35455799]
Mo Y, Xu Z, Xiao H, Yu X, Zhang H, Huang W, Gao L, Wang Y. Caregiver competence in pediatric eye drop administration: An observational study. Journal of pediatric nursing. 2025 Sep-Oct:84():261-267. doi: 10.1016/j.pedn.2025.06.023. Epub 2025 Jun 20 [PubMed PMID: 40543350]
Level 2 (mid-level) evidenceHirota A, Goseki T, Kunimi K, Kimijima M, Ichibe Y. A Case of Highly Myopic Strabismus That Showed Temporary Large Exotropia After the Yokoyama Procedure. Cureus. 2025 Jul:17(7):e88932. doi: 10.7759/cureus.88932. Epub 2025 Jul 28 [PubMed PMID: 40895942]
Level 3 (low-level) evidenceAlrefaie SM, Afandi RA, Alhaimi FM. The outcome of lateral rectus extirpation in a case of traumatic third cranial nerve palsy: A case report. International journal of surgery case reports. 2025 Oct:135():111887. doi: 10.1016/j.ijscr.2025.111887. Epub 2025 Sep 2 [PubMed PMID: 40925303]
Level 3 (low-level) evidenceChen AM, Cotter SA. The Amblyopia Treatment Studies: Implications for Clinical Practice. Advances in ophthalmology and optometry. 2016 Aug:1(1):287-305. doi: 10.1016/j.yaoo.2016.03.007. Epub [PubMed PMID: 28435934]
Level 3 (low-level) evidence