 Assisted Reproductive Technology (ART) Techniques
Assisted Reproductive Technology (ART) Techniques
Introduction
Assisted reproductive technologies (ART), as defined by the Centers for Disease Control and Prevention (CDC), are fertility-related treatments in which eggs or embryos are manipulated. Procedures where only sperm are manipulated, such as intrauterine insemination, are not included under this definition. Additionally, procedures in which ovarian stimulation is performed without a plan for egg retrieval are also excluded by definition.
The first successful human in vitro fertilization (IVF) was performed in England in 1978—a woman had an unstimulated menstrual cycle, and physicians performed a laparoscopic retrieval of a single oocyte from the ovary. The oocyte was then fertilized in vitro and subsequently transferred as an embryo into her uterus.[1]
Since its inception, IVF has undergone significant technological advancements and has become widely accessible worldwide. IVF remains the most commonly utilized ART procedure. IVF remains the most commonly utilized ART procedure, and a clear understanding of IVF principles, related ART techniques, and their appropriate application is fundamental to clinicians’ practice.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Understanding ART requires a thorough comprehension of female reproductive anatomy, specifically the ovaries, fallopian tubes, and uterus. The ovaries are the female gonads, paired oval-shaped structures that embryologically derive from the mesonephric ridge before descending into the pelvis. Ovaries are the third component of the hypothalamic-pituitary-ovarian axis (HPO), a complex feedback loop that regulates the female menstrual cycle. The ovaries produce estradiol and progesterone, and they are the site where oocytes mature and develop. The ovaries have 2 peritoneal attachments: the ovarian ligament and the suspensory ligament of the ovary. The ovarian ligament attaches the ovary to the uterus. The suspensory ligament of the ovary attaches the ovary to the pelvic sidewall and contains the neurovascular supply for the ovary. The transvaginal approach to oocyte retrieval relies on an understanding of this anatomical relationship.
The uterus lies in the pelvis, between the bladder and rectum. It consists of the corpus (the body of the uterus) and the cervix, which connects the uterus to the vagina. The uterine body consists of 3 layers: the perimetrium, myometrium, and endometrium. The endometrium is composed of 2 layers: the functionalis and the basalis. With each menstrual cycle, the functionalis layer changes in response to hormones from the HPO axis to prepare for implantation. Increasing estrogen levels during the follicular phase of the menstrual cycle result in endometrial glandular proliferation. During the luteal phase, progesterone levels rise, causing the endometrium to undergo secretory changes. If an embryo does not implant during the cycle, estrogen and progesterone levels fall, leading to the degradation of the functionalis layer, which then sloughs off during menses.[2]
The fallopian tubes are muscular tubes that extend laterally from the uterus towards the ovaries on both sides. The fallopian tubes aid in the transfer of the ovum to the uterus, and fertilization often occurs within the tube itself. The tubes sweep up the ovum at their fimbriated ends, then smooth muscle contractions and ciliated columnar epithelial cells transport the ovum or embryo to the uterus, where it can implant if fertilized.
Indications
ART procedures are most frequently performed in the setting of infertility. In patients with tubal factor infertility, IVF directly bypasses the fallopian tubes. Other infertility indications for IVF include male factor infertility, diminished ovarian reserve, ovarian insufficiency (with donor eggs), ovulatory dysfunction, and unexplained infertility.[3] In patients with uterine factor infertility or for whom pregnancy is relatively contraindicated (discussed below), IVF can be used with a gestational carrier.
IVF is also used outside of infertility settings. The procedure can be used for patients desiring preimplantation genetic testing, such as those known to be carriers of certain genetic disorders, and for fertility preservation, including patients about to receive gonadotoxic therapy or those who wish to delay childbearing. These individuals may opt to freeze their eggs or embryos for future use.[4] Another common use for IVF is in patients who do not have a male partner or who wish to use a sperm donor, such as same-sex couples and single individuals.
Contraindications
Before initiation of ART modalities, the maternal risks associated with ART procedures and pregnancy are discussed with the patient. An active pelvic infection is a contraindication for invasive ART procedures, such as transvaginal oocyte retrieval. Certain maternal conditions, particularly cardiopulmonary conditions such as pulmonary hypertension and heart failure, are relative contraindications for pregnancy itself. Preconception counseling and an evaluation to screen for such conditions should be conducted. Gestational carrier options can be utilized in patients with such contraindications.[5]
Equipment
Based on the American Society of Reproductive Medicine (ASRM) guidelines for embryology/andrology labs, the basic equipment required for the management of oocytes and embryos is as follows:
- Incubator
- Microscope suitable for the handling and micromanipulation of oocytes and embryos
- Devices for pH and temperature monitoring and maintenance
- Warming blocks
- Laser for the biopsy of embryos
- Cryopreservation equipment (liquid nitrogen tanks)
- Laboratory centrifuge
- Laminar flow hood
- Culture media
- Refrigerator
- Air filtration system [6]
Personnel
Per ASRM, the minimum personnel required to appropriately offer ART are as follows:
- Medical director
- Physician licensed in reproductive endocrinology and infertility (REI)
- Physician with male reproduction expertise
- Nursing with training in reproductive medicine and ART
- Embryology laboratory director
- Andrologist with laboratory procedure experience
- Laboratory personnel to perform the necessary hormone assays
- Individual with expertise in gynecologic ultrasound (physician, technician, or nurse)
- Mental health professional with fertility counseling experience
- Genetic counselor [7]
Preparation
Preparation for ART procedures largely centers on the infertility workup. Infertility is defined as the inability to achieve a successful pregnancy after at least 1 year of unprotected intercourse. The infertility evaluation can also be initiated at 6 months of attempted conception when the female partner is older than 35 or in cases where there are known possible barriers, such as previously diagnosed uterine or tubal disease or male infertility.[8] Initial comprehensive history taking includes a menstrual history, pregnancy history, duration of infertility, prior infertility treatments, past medical and surgical history, family history, and social and environmental exposures and habits. The physical examination includes basic vital signs, body mass index (BMI), a pelvic examination, and an evaluation for signs of thyroid dysfunction and excess androgen levels (virilization).
For the female evaluation, day 3 follicle-stimulating hormone (FSH), estradiol (E2), antral follicle count, and anti-müllerian hormone (AMH) levels are determined via blood work, and a baseline transvaginal ultrasound is performed to assess ovarian reserve. Further medical evaluation of patients with ovulatory dysfunction includes measurement of thyroid-stimulating hormone (TSH), prolactin, dehydroepiandrosterone sulfate (DHEAS), testosterone, and 17-hydroxyprogesterone levels. This hormonal assessment helps determine the etiology of anovulation. Additionally, the uterus and pelvis are typically evaluated with a baseline transvaginal ultrasound, often in conjunction with a hysterosalpingogram or sonohysterogram. This ultrasound evaluation helps detect uterine anatomical factors that may affect fertility or pregnancy maintenance, such as polyps, submucosal fibroids, or uterine malformations, including uterine septa (see Image. Saline Infusion Sonohysterogram of Intracavitary Fibroid). Ultrasound can also help identify other causes of subfertility, such as hydrosalpinx or endometriosis.
The male infertility workup begins with a thorough medical, surgical, and reproductive history, along with a physical examination focused on the genitourinary system. The cornerstone of evaluation is a semen analysis assessing volume, concentration, motility, and morphology. Additional testing may include hormonal profiling (FSH, luteinizing hormone [LH], testosterone, prolactin), scrotal ultrasound, and genetic testing when indicated. In addition, both male and female evaluations usually involve a basic infectious disease workup, including syphilis, a hepatitis panel, and human immunodeficiency virus (HIV).
Technique or Treatment
IVF is the most commonly utilized ART. It involves the collection of oocytes from the ovary, followed by the fertilization of the oocytes in vitro, and ultimately the transfer of the resulting embryo into the uterus. The process outlined below comprises several steps: controlled ovarian stimulation, oocyte retrieval, fertilization, embryo culture, and embryo transfer. Additionally, preimplantation genetic testing (PGT) and intracytoplasmic sperm injection (ICSI) may be included in the process. Cryopreservation with vitrification is then used to freeze excess embryos or to preserve fertility by freezing eggs or embryos.
Controlled Ovarian Stimulation
The first cases of IVF utilized a natural menstrual cycle where a single oocyte was retrieved. Natural cycle IVF is still in practice. However, controlled ovarian stimulation is now more commonly performed to maximize the number of oocytes retrieved per cycle. The practice also offers a much higher chance of pregnancy success.
Multiple agents and regimens exist for controlled ovarian stimulation. Selective estrogen receptor modulators (SERMs), such as clomiphene citrate or tamoxifen, offer one avenue for this approach. The benefits of minimal stimulation protocols ("mini-IVF") utilizing SERMs include a decreased risk of ovarian hyperstimulation syndrome (OHSS) and multifetal gestation. However, these protocols also result in a lower live birth rate (49% versus 63% for mini-IVF and conventional IVF, respectively).[9]
Injection of exogenous gonadotropins, such as FSH and LH, is frequently used for controlled stimulation. This practice maximizes the number of developing follicles during a single cycle. The following gonadotropin protocols are currently the most popular.
Gonadotropin-Releasing Hormone (GnRH) Antagonist Cycles
Mixed gonadotropin medications use 2 types of injections: 1 with FSH activity (recombinant FSH) and 1 that has both FSH and LH activity. The premature LH surge is prevented by a GnRH antagonist such as cetrorelix or ganirelix, which competitively binds to GnRH receptors in the pituitary gland. After baseline parameters are confirmed by ultrasound and normal FSH and estradiol levels are established, the GnRH antagonist cycle can be initiated during menses. Two main approaches are used for the timing of GnRH antagonist administration. In fixed protocols, the GnRH antagonist is started on day 5 or 6 of stimulation.[10] In flexible protocols, the GnRH antagonist is initiated when the largest follicle reaches a specific size, typically 12 to 14 mm, or when the estradiol level is near 400 pg/mL. Hormonal pretreatment with oral contraceptive pills, estradiol (E2), or progestins may be used for 2 to 4 weeks before the cycle starts. Unlike GnRH agonists, a desensitization phase is not required for GnRH antagonist protocols, as the immediate downregulation with an antagonist eliminates the need for this phase. Thus, GnRH antagonist cycles involve a shorter duration of ovarian stimulation and may be associated with a lower risk of OHSS compared to GnRH agonist cycles.[11] As such, GnRH antagonist protocols are often preferred in patients with polycystic ovary syndrome (PCOS). In addition, when using a GnRH antagonist protocol, the trigger can be a GnRH agonist (eg, leuprolide acetate) instead of human chorionic gonadotropin (hCG), which has a much higher association with OHSS.
Gonadotropin-Releasing Hormone (GnRH) Agonist Cycles
Mixed gonadotropins are also used in GnRH agonist protocols, again with 2 types of injection: 1 with FSH activity (recombinant FSH) and 1 with both FSH and LH activity. However, in a GnRH agonist cycle, the premature LH surge is prevented by a GnRH agonist, which binds to the GnRH receptor to cause an initial increase in FSH and LH, followed by downregulation. Pretreatment with oral contraceptives can also be used in these cycles. The GnRH agonist is initiated either during the luteal phase of the menstrual cycle or while the patient is on combined oral contraceptive therapy before gonadotropin administration, thereby desensitizing the pituitary through downregulation and suppressing the endogenous LH surge. Once downregulation is confirmed, the dose of the GnRH agonist is halved until a trigger is given for final maturation, before egg retrieval. Transvaginal ultrasound monitoring is utilized to track the number and growth of follicles, starting at stimulation and repeated every few days. Serum laboratory testing is also performed, most frequently to measure E2 levels and track ovarian response, allowing for adjustments in dosing. Once ovarian follicles are mature (typically when 2 to 3 follicles reach 18 mm in size), final oocyte maturation is artificially triggered via exogenous human chorionic gonadotropin (hCG) and not with a GnRH agonist like leuprolide acetate (which is often used in GnRH antagonist cycles). There is no clear consensus on which is more efficacious between GnRH antagonist and agonist cycles; however, GnRH antagonists are commonly preferred due to their ease of use, cost-effectiveness, and shorter period of ovarian stimulation.[12]
Progestin Protocols
Progestin cycles are a newer alternative to traditional GnRH agonist and antagonist cycles. Oral progestins such as medroxyprogesterone are used to suppress the LH surge. The advantage of this technique is that oral medications are used instead of injections, which can reduce costs and improve patient comfort. Progestin cycles require frozen embryo transfer due to unfavorable endometrial receptivity with prolonged progesterone exposure.
Oocyte Retrieval
Today, oocyte retrieval is typically performed vaginally using ultrasound guidance under general anesthesia or conscious sedation.[13] A needle is inserted transvaginally and guided with ultrasound into each follicle to aspirate the follicular fluid, usually containing an oocyte. Retrieving more oocytes (up to 15) is associated with improved live birth rates.[14]
Before the ultrasound-guided transvaginal approach, laparoscopic or abdominal retrievals of oocytes were performed.[15] While they have largely fallen out of practice, laparoscopic and abdominal egg retrievals are still occasionally used to obtain oocytes in cases such as vaginal agenesis or when the ovaries are not in the pelvis (as in cases of ovarian transposition in advance of radiation therapy or with patients who have a large fibroid uterus).
Fertilization
Fertilization occurs in vitro by mixing oocytes obtained from the retrieval with spermatozoa in a culture medium. Spermatozoa are obtained via an ejaculation sample or surgical retrieval in cases of obstructive azoospermia and isolated via density centrifugation and washing in culture media. For patients with a history of fertilization failure or with male factor infertility, ICSI is considered, as it has been shown to improve fertilization rates.[16] ICSI uses a single sperm that is injected directly into the cytoplasm of the oocyte. Embryologists choose sperm for ICSI utilizing morphologic parameters.
Embryos are incubated for either a day 3 (cleavage stage) or day 5 (blastocyst stage) transfer. Day 5 transfers are more common and have a higher success rate; evaluation of the appearance of the embryos on day 5 at the blastocyst stage is more predictive of success compared to day 2 or 3 at the cleavage stage, in which the embryos are merely 4 or 8 cells, respectively.[17][18] See Image. Stages of Embryo Development.
Preimplantation Genetic Testing
Preimplantation genetic testing (PGT) involves various genetic assays performed on embryos before transfer to identify possible genetic disorders; it is commonly performed in conjunction with IVF. For example, preimplantation genetic testing for aneuploidies (PGT-A) screens for whole chromosome abnormalities. In contrast, preimplantation genetic testing for monogenic disorders (PGT-M) screens for single-gene disorders in high-risk patients.
PGT can be performed using polar bodies or an isolated blastomere from a cleavage-stage embryo, typically from a day 3 embryo. PGT can also be performed from a sample of cells from the trophectoderm of a blastocyst-stage embryo. The benefit of a trophectoderm sample is avoiding the need to biopsy the inner cell mass, which gives rise to the fetus (see Image. Trophectoderm Biopsy at the Blastocyst Stage). However, there is a possibility of false-positive results, and in the case of mosaicism, it may not fully represent the constitution of the fetal tissue.[19] For this reason, additional diagnostic testing, such as chorionic villous sampling, should be offered during pregnancy. PGT-A was initially performed using fluorescence in situ hybridization (FISH) analysis that utilizes selected chromosomes. Most evidence with this method does not show improvement in IVF outcomes.[20] Now, PGT-A is routinely performed on all 24 chromosomes, initially using array comparative genomic hybridization (aCGH) and now with the aid of more advanced technologies, such as next-generation sequencing.[21]
With 24-chromosome analysis, evidence for PGT-A is more mixed. A few randomized controlled trials (RCTs) comparing elective single-embryo transfer (eSET) of euploid embryos determined by PGT-A versus morphology grade-based selection of embryos found noninferior or improved pregnancy rates amongst the PGT-A group.[22][23] A 2011-2012 retrospective data analysis from a national ART database found a possible increase in the likelihood of live births in women older than 37 who utilized PGT-A.[24] These studies are limited by either their retrospective design or their use of patient cohorts with favorable prognoses. Additionally, these studies relied on genetic analysis methods that have since fallen out of practice, such as aCGH.
Given the mixed and limited data, ASRM does not advocate for or against the universal use of PGT-A. However, it acknowledges the potential benefits, particularly for eSET candidates, and the resulting decrease in multigestation pregnancies.[25]
While PGT is classically used for selection against aneuploidies and genetic disorders, it can also be used in more ethically controversial ways, such as sex selection. Additionally, individuals in specific communities, such as the Deaf community and people with dwarfism, have been reported to request selection for genetic deafness or dwarfism. A shared decision-making model is recommended in such circumstances.[26][27]
In Vitro Maturation
In vitro maturation (IVM) is an alternative to traditional IVF that can be used in select patients, such as those at risk of OHSS (eg, patients with PCOS) or biologically female patients with estrogen-sensitive cancers requiring time-sensitive gonadotoxic treatment. In IVM, immature follicles are collected with minimal to no exposure to hormonal stimulation during the germinal vesicle to metaphase II stage. Typically, a short course of FSH is administered, with or without hCG administration, for follicular priming.[28] Retrieval and culture need to be modified to obtain and mature the immature oocytes before fertilization. Candidates for IVM are typically those who have a relative contraindication to IVF, and patients should be counseled that the rate of achieving the blastocyst stage is lower with IVM. Likewise, pregnancy rates are also lower with this method.[29][30]
Embryo Transfer
The ASRM developed a standardized protocol for embryo transfer based on a task force that evaluated survey responses regarding individual practices amongst Society for Assisted Reproductive Technology (SART) medical directors.[31] The impetus for developing standardized practice guidelines was evidence of limited training in embryo transfer during fellowships and of varying IVF outcomes depending on the provider performing the transfer.
The standardized protocol based on the survey and existing evidence is as follows:
- The provider should first prepare for the embryo transfer by reviewing prior mock/transfer notes.
- Patient preparation for the procedure should include analgesics for patient comfort, although analgesics are not shown to improve pregnancy outcomes.
- A checklist-based time-out process is implemented to ensure accurate identification of patients and embryos.
- Transabdominal ultrasound guidance is used to visualize the endometrial cavity and pelvic anatomy, and to guide the transfer.
- Standard sterility preparation includes hand washing and the use of sterile gloves.
- After placement of the speculum, flushing of the vagina is recommended with either a cotton swab or gauze, utilizing saline or other media as the cleansing solution.
- Removal of mucus from the cervical-endocervical canal shows some evidence for improvement in clinical pregnancy rates.[32][33]
- A soft embryo transfer catheter should be used to pass through the cervix into the endometrial cavity. The transfer may occur directly, in which the catheter is loaded with the embryos before catheter placement, or with a trial transfer followed by the actual transfer (an empty catheter is passed through the cervix before loading the catheter with an embryo for transfer), or with an afterload transfer, in which the catheter is passed through the cervix. The inner catheter is removed, with the outer catheter left in place in the canal. The inner catheter is then loaded with the embryo(s) and replaced for the placement of the embryo(s) into the uterus.
- The catheter tip should be placed in the upper or middle third of the endometrial cavity. There is some evidence that this position improves pregnancy rates.[34][35]
- Confirm that the catheter does not have retained embryo(s).
- There is no evidence for bed rest after embryo transfer.[36]
While the vast majority of embryo transfers are performed transvaginally, for patients with uterine anomalies or difficult trans-cervical access, intrafallopian transfer via gamete intrafallopian transfer (GIFT) or zygote intrafallopian transfer (ZIFT) is a possible alternative to laparoscopic transfer techniques.
Current ASRM guidelines recommend single-embryo transfer for patients with a favorable prognosis and a maximum of 2 or 3 blastocyst embryos transferred at once in the 38- to 40-year-old and 41- to 42-year-old age groups, respectively.[37] These guidelines are made to reduce multifetal gestation. Following embryo transfer, the luteal phase is typically supported with progesterone and estrogen supplementation to promote implantation and maintain pregnancy.
Frozen versus Fresh Embryo Transfers
Embryos can be transferred during the same cycle as egg retrieval and fertilization, or during a later cycle. Fresh embryo transfer involves transferring the embryo into the uterus, typically 3-5 days after ovarian stimulation and egg retrieval (ie, during the same cycle). Alternatively, embryos can be cryopreserved, thawed, and transferred in a subsequent cycle. Although fresh embryo transfer involves only one cycle and thus has a shorter time to potential pregnancy, frozen embryo transfer has become more common due to improved clinical outcomes, including higher implantation and pregnancy rates, as well as improved perinatal outcomes.[38][39] Controlled ovarian stimulation may lead to decreased endometrial receptivity and thus impaired implantation of fresh embryo transfers. When using frozen embryos, embryo transfer can be performed at a time when endometrial receptivity is higher. Frozen embryo transfer also eliminates the risk of OHSS compared to fresh embryo transfer. However, frozen transfer can be a more costly and lengthy process for patients, given that it requires cryopreservation of the embryos for at least one additional cycle. Lower-quality embryos are typically not frozen, and embryos must survive the thawing process, resulting in potentially fewer embryos available for frozen transfers.
Cryopreservation
Embryos not used in the current cycle can be cryopreserved for future use. Cryopreservation is typically achieved through vitrification, a rapid-freezing process. Vitrification is believed to prevent cryoinjury by inhibiting the formation of intracellular crystals.[40] All embryos can also be frozen for patients at risk for OHSS. The embryos from these "freeze-all" cycles can then be used in a future cycle that is not associated with controlled ovarian stimulation. Freeze-all cycles are also utilized in some clinics routinely, as frozen-thawed embryos have been associated with improved pregnancy rates and obstetric outcomes, such as a decreased risk of perinatal mortality and preterm birth.[41][42]
Complications
While ART has significantly improved outcomes for individuals and couples facing infertility, the procedures are not without risks. Understanding the potential complications associated with ART is crucial for making informed clinical decisions and providing comprehensive patient counseling.
Ovarian Hyperstimulation Syndrome
OHSS is a potentially fatal complication of controlled ovarian stimulation. The reported incidence of OHSS, based on diagnostic criteria, is estimated to range from 1% to 5% for moderate-to-severe cases.[14]
OHSS develops from the exogenous administration of gonadotropins followed by the administration of hCG. In this process, many follicles are recruited and develop within a single cycle, resulting in the excessive production of various growth factors, such as vascular endothelial growth factor (VEGF), and subsequent neovascularization. The combination of excessive follicular growth and fluid and vascular development leads to significant fluid shifts to the third compartment, resulting in ascites, edema, pleural effusion, renal injury, pericardial effusion, and thromboembolism. Patients at particular risk of OHSS include those with a diagnosis of PCOS, multi-follicular development, a large number of oocytes retrieved (>24), and elevated estradiol levels (>3500 pg/mL).[43][44]
For patients diagnosed with moderate to severe OHSS, treatment involves supportive care with fluid resuscitation, therapeutic paracentesis, and prophylactic anticoagulation. Patients at risk for OHSS must not have a fresh transfer and must freeze all embryos until their ovarian stimulation has subsided. The final maturation trigger should be changed from hCG to a GnRH agonist if possible. In addition, cabergoline can be administered daily for 8 days after oocyte retrieval or after trigger administration to protect the patient from OHSS further. Then, 1 to 2 months later, when the ovarian stimulation has resolved, the patient can safely proceed with a frozen embryo transfer.
Antenatal and Neonatal Complications
The most common complication of ART is the risk of multifetal gestation. In 2009, 41.1% of infants conceived via ART were of multifetal pregnancies (compared to 3.5% of infants in the general population).[45] The effort to reduce multifetal gestation via reducing the number of embryos transferred at once has resulted in a significant reduction—by 2017, 73.6% of ART-conceived infants were from singleton pregnancies.[37][46]
Multifetal gestations have both maternal and fetal consequences. These pregnancies have a higher likelihood of various antenatal complications, including hyperemesis gravidarum, gestational diabetes, and hypertensive diseases of pregnancy.[47][48] Multifetal pregnancies also have worse fetal and neonatal outcomes than singleton pregnancies, with a significant increase in preterm birth and an associated increase in the risk of stillbirth (5-fold) and neonatal death (7-fold).[49][50]
IVF providers limit multifetal pregnancies through several avenues, including low-dose stimulation regimens, close hormonal and follicular monitoring during stimulated cycles, and limiting the number of embryos transferred per cycle.[51][52] Once a multifetal gestation is diagnosed, appropriate counseling regarding the increased risks should be discussed with the patient, and the option of multifetal reduction, when appropriate, should be offered.[53]
Beyond multifetal gestation, singleton IVF pregnancies are also possibly associated with increased risks of various complications compared to naturally conceived singleton pregnancies. These complications include perinatal mortality, preterm delivery, low birth weight, cesarean delivery, placenta previa, placental abruption, and preeclampsia. These potential risks should be discussed with patients, but with caution, as the designs of existing studies limit data quality. Standardizing the tracking of outcomes of ART pregnancies to include these complications would improve the strength of evidence for or against these potentially elevated risks associated with IVF-conceived singleton pregnancies.[54][55] There is also limited evidence of a slightly increased risk of birth defects in pregnancies conceived via IVF, particularly with ICSI—though again, the quality of the data is low.[56][57] It is reasonable to offer ultrasonographic surveillance during IVF-conceived pregnancies, such as with fetal echocardiography, to screen for congenital anomalies.
Clinical Significance
ART enables individuals and couples to achieve pregnancy in circumstances where natural conception may be unlikely or impossible, including cases of infertility, prior exposure to gonadotoxic treatments, and the presence of heritable genetic disorders.
According to the CDC, as of 2017, 1.9% of US-born infants were conceived with ART. In 2017, approximately 200,000 ART cycles with embryo transfer were performed, resulting in 78,052 live births.[46] As rates of delayed childbearing and insurance coverage for ART increase, these numbers are likely to rise. As such, women’s health and reproductive healthcare providers need to have a working knowledge of indications for ART and appropriate timing for referral to a reproductive endocrinology and infertility (REI) specialist.
Enhancing Healthcare Team Outcomes
Effective, patient-centered care with ART requires a coordinated, interprofessional approach involving physicians, advanced practitioners, nurses, pharmacists, and other allied health professionals. Each team member brings specialized skills and knowledge. Physicians and advanced practitioners lead the diagnostic evaluation and treatment planning, while nurses provide patient education, emotional support, and cycle coordination. Pharmacists ensure safe and accurate medication management. An andrologist with laboratory experience is essential for the evaluation and preparation of sperm for ART procedures, including semen analysis, sperm retrieval, and processing. Laboratory personnel execute precise technical procedures and perform vital hormone assays that inform clinical decision-making and ensure accurate timing of interventions. A clinician or technician skilled in gynecologic ultrasound plays a key role in follicular monitoring, endometrial assessment, and procedural guidance during egg retrieval and embryo transfer. The inclusion of a mental health professional with experience in fertility counseling supports patients and couples in managing the emotional, ethical, and psychological challenges associated with ART. Genetic counselors further enhance care by assessing hereditary risks, guiding decisions on preimplantation genetic testing, and supporting informed consent.
Clear, respectful communication among team members is essential for aligning goals, minimizing errors, and enhancing patient safety. Ethical responsibilities include respecting patient autonomy, handling sensitive genetic and reproductive information with discretion, and ensuring equitable access to care. Strategies such as shared decision-making, standardized protocols, and regular case conferences improve team performance and clinical outcomes. Through collaborative practice and diligent care coordination, the interprofessional team can deliver high-quality, individualized ART services that prioritize both patient well-being and successful reproductive outcomes.
Media
(Click Image to Enlarge)

Stages of Embryo Development. (A) Depicts an embryo 16-18 hours following insemination. (B) Depicts a 4-cell embryo 40-50 hours after insemination. (C) Depicts an 8-cell cleavage-stage embryo 64-67 hours following insemination. (D) Depicts a blastocyst-stage embryo 120 hours following insemination.
Einstein/Montefiore Medical Library
(Click Image to Enlarge)

Trophectoderm Biopsy at the Blastocyst Stage. Five to 10 cells are removed from the outer layer of the embryo (trophectoderm), which forms the placenta. The inner cell mass, which develops into the fetus, remains intact. These cells are then analyzed for genetic testing.
Einstein/Montefiore Medical Library
(Click Image to Enlarge)
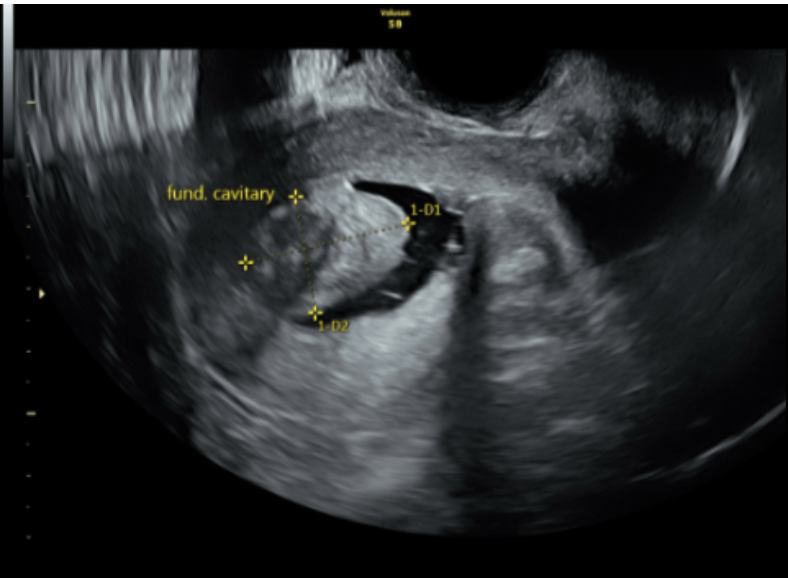
Saline Infusion Sonohysterogram of Intracavitary Fibroid. Preparation for in vitro fertilization includes evaluation for etiologies of infertility as well as potential barriers to success for in vitro fertilization. This figure is an example of a saline infusion sonohysterogram, in which a saline infusion is introduced into the uterine cavity during transvaginal ultrasound to identify intracavitary abnormalities. A fundal cavitary fibroid is noted, which, if left untreated, may reduce implantation success rates and increase miscarriage rates in achieved pregnancies.
Einstein/Montefiore Medical Library
References
Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet (London, England). 1978 Aug 12:2(8085):366 [PubMed PMID: 79723]
Level 3 (low-level) evidenceCritchley HO, Saunders PT. Hormone receptor dynamics in a receptive human endometrium. Reproductive sciences (Thousand Oaks, Calif.). 2009 Feb:16(2):191-9. doi: 10.1177/1933719108331121. Epub [PubMed PMID: 19208787]
Level 3 (low-level) evidencevan Eekelen R, van Geloven N, van Wely M, Bhattacharya S, van der Veen F, Eijkemans MJ, McLernon DJ. IVF for unexplained subfertility; whom should we treat? Human reproduction (Oxford, England). 2019 Jul 8:34(7):1249-1259. doi: 10.1093/humrep/dez072. Epub [PubMed PMID: 31194864]
Noyes N, Labella PA, Grifo J, Knopman JM. Oocyte cryopreservation: a feasible fertility preservation option for reproductive age cancer survivors. Journal of assisted reproduction and genetics. 2010 Aug:27(8):495-9. doi: 10.1007/s10815-010-9434-3. Epub 2010 May 18 [PubMed PMID: 20480389]
Practice Committee of the American Society for Reproductive Medicine and Practice Committee of the Society for Assisted Reproductive Technology. Electronic address: ASRM@asrm.org, Practice Committee of the American Society for Reproductive Medicine and Practice Committee of the Society for Assisted Reproductive Technology. Recommendations for practices utilizing gestational carriers: a committee opinion. Fertility and sterility. 2017 Feb:107(2):e3-e10. doi: 10.1016/j.fertnstert.2016.11.007. Epub 2017 Jan 6 [PubMed PMID: 28069181]
Level 3 (low-level) evidencePractice Committee of American Society for Reproductive Medicine, Practice Committee of Society for Assisted Reproductive Technology. Revised guidelines for human embryology and andrology laboratories. Fertility and sterility. 2008 Nov:90(5 Suppl):S45-59. doi: 10.1016/j.fertnstert.2008.08.099. Epub [PubMed PMID: 19007646]
Practice Committee of the American Society for Reproductive Medicine, Practice Committee of the Society for Assisted Reproductive Technology, and Practice Committee of the Society of Reproductive Biologists and Technologists. Electronic address: asrm@asrm.org. Minimum standards for practices offering assisted reproductive technologies: a committee opinion. Fertility and sterility. 2021 Mar:115(3):578-582. doi: 10.1016/j.fertnstert.2020.12.036. Epub 2021 Feb 7 [PubMed PMID: 33568271]
Level 3 (low-level) evidencePractice Committee of the American Society for Reproductive Medicine. Electronic address: asrm@asrm.org. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertility and sterility. 2020 Mar:113(3):533-535. doi: 10.1016/j.fertnstert.2019.11.025. Epub 2020 Feb 27 [PubMed PMID: 32115183]
Level 3 (low-level) evidenceZhang JJ, Merhi Z, Yang M, Bodri D, Chavez-Badiola A, Repping S, van Wely M. Minimal stimulation IVF vs conventional IVF: a randomized controlled trial. American journal of obstetrics and gynecology. 2016 Jan:214(1):96.e1-8. doi: 10.1016/j.ajog.2015.08.009. Epub 2015 Aug 8 [PubMed PMID: 26259908]
Level 1 (high-level) evidenceVenetis CA, Storr A, Chua SJ, Mol BW, Longobardi S, Yin X, D'Hooghe T. What is the optimal GnRH antagonist protocol for ovarian stimulation during ART treatment? A systematic review and network meta-analysis. Human reproduction update. 2023 May 2:29(3):307-326. doi: 10.1093/humupd/dmac040. Epub [PubMed PMID: 36594696]
Level 1 (high-level) evidenceTarlatzis BC, Fauser BC, Kolibianakis EM, Diedrich K, Rombauts L, Devroey P. GnRH antagonists in ovarian stimulation for IVF. Human reproduction update. 2006 Jul-Aug:12(4):333-40 [PubMed PMID: 16567347]
Tarlatzis BC, Kolibianakis EM. GnRH agonists vs antagonists. Best practice & research. Clinical obstetrics & gynaecology. 2007 Feb:21(1):57-65 [PubMed PMID: 17049460]
Kwan I, Wang R, Pearce E, Bhattacharya S. Pain relief for women undergoing oocyte retrieval for assisted reproduction. The Cochrane database of systematic reviews. 2018 May 15:5(5):CD004829. doi: 10.1002/14651858.CD004829.pub4. Epub 2018 May 15 [PubMed PMID: 29761478]
Level 1 (high-level) evidenceSteward RG, Lan L, Shah AA, Yeh JS, Price TM, Goldfarb JM, Muasher SJ. Oocyte number as a predictor for ovarian hyperstimulation syndrome and live birth: an analysis of 256,381 in vitro fertilization cycles. Fertility and sterility. 2014 Apr:101(4):967-73. doi: 10.1016/j.fertnstert.2013.12.026. Epub 2014 Jan 23 [PubMed PMID: 24462057]
Level 2 (mid-level) evidenceWikland M, Enk L, Hamberger L. Transvesical and transvaginal approaches for the aspiration of follicles by use of ultrasound. Annals of the New York Academy of Sciences. 1985:442():182-94 [PubMed PMID: 3893266]
van der Westerlaken L, Helmerhorst F, Dieben S, Naaktgeboren N. Intracytoplasmic sperm injection as a treatment for unexplained total fertilization failure or low fertilization after conventional in vitro fertilization. Fertility and sterility. 2005 Mar:83(3):612-7 [PubMed PMID: 15749489]
Level 1 (high-level) evidenceGardner DK, Schoolcraft WB, Wagley L, Schlenker T, Stevens J, Hesla J. A prospective randomized trial of blastocyst culture and transfer in in-vitro fertilization. Human reproduction (Oxford, England). 1998 Dec:13(12):3434-40 [PubMed PMID: 9886530]
Level 1 (high-level) evidenceGlujovsky D, Farquhar C, Quinteiro Retamar AM, Alvarez Sedo CR, Blake D. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. The Cochrane database of systematic reviews. 2016 Jun 30:(6):CD002118. doi: 10.1002/14651858.CD002118.pub5. Epub 2016 Jun 30 [PubMed PMID: 27357126]
Level 1 (high-level) evidenceCapalbo A, Rienzi L. Mosaicism between trophectoderm and inner cell mass. Fertility and sterility. 2017 May:107(5):1098-1106. doi: 10.1016/j.fertnstert.2017.03.023. Epub 2017 Apr 19 [PubMed PMID: 28433375]
Mastenbroek S, Twisk M, van der Veen F, Repping S. Preimplantation genetic screening: a systematic review and meta-analysis of RCTs. Human reproduction update. 2011 Jul-Aug:17(4):454-66. doi: 10.1093/humupd/dmr003. Epub 2011 Apr 29 [PubMed PMID: 21531751]
Level 1 (high-level) evidenceBrezina PR, Anchan R, Kearns WG. Preimplantation genetic testing for aneuploidy: what technology should you use and what are the differences? Journal of assisted reproduction and genetics. 2016 Jul:33(7):823-32. doi: 10.1007/s10815-016-0740-2. Epub 2016 Jun 14 [PubMed PMID: 27299602]
Forman EJ, Hong KH, Ferry KM, Tao X, Taylor D, Levy B, Treff NR, Scott RT Jr. In vitro fertilization with single euploid blastocyst transfer: a randomized controlled trial. Fertility and sterility. 2013 Jul:100(1):100-7.e1. doi: 10.1016/j.fertnstert.2013.02.056. Epub 2013 Mar 30 [PubMed PMID: 23548942]
Level 1 (high-level) evidenceYang Z, Liu J, Collins GS, Salem SA, Liu X, Lyle SS, Peck AC, Sills ES, Salem RD. Selection of single blastocysts for fresh transfer via standard morphology assessment alone and with array CGH for good prognosis IVF patients: results from a randomized pilot study. Molecular cytogenetics. 2012 May 2:5(1):24. doi: 10.1186/1755-8166-5-24. Epub 2012 May 2 [PubMed PMID: 22551456]
Level 3 (low-level) evidenceKushnir VA, Darmon SK, Albertini DF, Barad DH, Gleicher N. Effectiveness of in vitro fertilization with preimplantation genetic screening: a reanalysis of United States assisted reproductive technology data 2011-2012. Fertility and sterility. 2016 Jul:106(1):75-79. doi: 10.1016/j.fertnstert.2016.02.026. Epub 2016 Mar 4 [PubMed PMID: 26952783]
Practice Committees of the American Society for Reproductive Medicine and the Society for Assisted Reproductive Technology. Electronic address: ASRM@asrm.org, Practice Committees of the American Society for Reproductive Medicine and the Society for Assisted Reproductive Technology. The use of preimplantation genetic testing for aneuploidy (PGT-A): a committee opinion. Fertility and sterility. 2018 Mar:109(3):429-436. doi: 10.1016/j.fertnstert.2018.01.002. Epub [PubMed PMID: 29566854]
Level 3 (low-level) evidenceEthics Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org, Ethics Committee of the American Society for Reproductive Medicine. Transferring embryos with genetic anomalies detected in preimplantation testing: an Ethics Committee Opinion. Fertility and sterility. 2017 May:107(5):1130-1135. doi: 10.1016/j.fertnstert.2017.02.121. Epub [PubMed PMID: 28476180]
Level 3 (low-level) evidenceWallis JM. Is it ever morally permissible to select for deafness in one's child? Medicine, health care, and philosophy. 2020 Mar:23(1):3-15. doi: 10.1007/s11019-019-09922-6. Epub [PubMed PMID: 31542873]
Ho VNA, Pham TD, Le AH, Ho TM, Vuong LN. Live birth rate after human chorionic gonadotropin priming in vitro maturation in women with polycystic ovary syndrome. Journal of ovarian research. 2018 Aug 27:11(1):70. doi: 10.1186/s13048-018-0445-5. Epub 2018 Aug 27 [PubMed PMID: 30149808]
Ortega-Hrepich C, Stoop D, Guzmán L, Van Landuyt L, Tournaye H, Smitz J, De Vos M. A "freeze-all" embryo strategy after in vitro maturation: a novel approach in women with polycystic ovary syndrome? Fertility and sterility. 2013 Oct:100(4):1002-7. doi: 10.1016/j.fertnstert.2013.06.018. Epub 2013 Jul 11 [PubMed PMID: 23850301]
Level 2 (mid-level) evidenceHo VNA, Braam SC, Pham TD, Mol BW, Vuong LN. The effectiveness and safety of in vitro maturation of oocytes versus in vitro fertilization in women with a high antral follicle count. Human reproduction (Oxford, England). 2019 Jun 4:34(6):1055-1064. doi: 10.1093/humrep/dez060. Epub [PubMed PMID: 31111879]
Practice Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org, Penzias A, Bendikson K, Butts S, Coutifaris C, Falcone T, Fossum G, Gitlin S, Gracia C, Hansen K, Mersereau J, Odem R, Rebar R, Reindollar R, Rosen M, Sandlow J, Vernon M. ASRM standard embryo transfer protocol template: a committee opinion. Fertility and sterility. 2017 Apr:107(4):897-900. doi: 10.1016/j.fertnstert.2017.02.108. Epub 2017 Mar 11 [PubMed PMID: 28292611]
Level 3 (low-level) evidenceMoini A, Kiani K, Bahmanabadi A, Akhoond M, Akhlaghi A. Improvement in pregnancy rate by removal of cervical discharge prior to embryo transfer in ICSI cycles: a randomised clinical trial. The Australian & New Zealand journal of obstetrics & gynaecology. 2011 Aug:51(4):315-20. doi: 10.1111/j.1479-828X.2011.01318.x. Epub 2011 Jun 9 [PubMed PMID: 21806579]
Level 1 (high-level) evidenceEskandar MA, Abou-Setta AM, El-Amin M, Almushait MA, Sobande AA. Removal of cervical mucus prior to embryo transfer improves pregnancy rates in women undergoing assisted reproduction. Reproductive biomedicine online. 2007 Mar:14(3):308-13 [PubMed PMID: 17359583]
Franco JG Jr, Martins AM, Baruffi RL, Mauri AL, Petersen CG, Felipe V, Contart P, Pontes A, Oliveira JB. Best site for embryo transfer: the upper or lower half of endometrial cavity? Human reproduction (Oxford, England). 2004 Aug:19(8):1785-90 [PubMed PMID: 15218006]
Level 1 (high-level) evidenceCoroleu B, Barri PN, Carreras O, Martínez F, Parriego M, Hereter L, Parera N, Veiga A, Balasch J. The influence of the depth of embryo replacement into the uterine cavity on implantation rates after IVF: a controlled, ultrasound-guided study. Human reproduction (Oxford, England). 2002 Feb:17(2):341-6 [PubMed PMID: 11821275]
Level 1 (high-level) evidenceCraciunas L, Tsampras N. Bed rest following embryo transfer might negatively affect the outcome of IVF/ICSI: a systematic review and meta-analysis. Human fertility (Cambridge, England). 2016 Apr:19(1):16-22. doi: 10.3109/14647273.2016.1148272. Epub 2016 Mar 17 [PubMed PMID: 26986834]
Level 1 (high-level) evidencePractice Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org, Practice Committee of the Society for Assisted Reproductive Technology. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertility and sterility. 2017 Apr:107(4):901-903. doi: 10.1016/j.fertnstert.2017.02.107. Epub 2017 Mar 11 [PubMed PMID: 28292618]
Level 3 (low-level) evidenceShi Y, Sun Y, Hao C, Zhang H, Wei D, Zhang Y, Zhu Y, Deng X, Qi X, Li H, Ma X, Ren H, Wang Y, Zhang D, Wang B, Liu F, Wu Q, Wang Z, Bai H, Li Y, Zhou Y, Sun M, Liu H, Li J, Zhang L, Chen X, Zhang S, Sun X, Legro RS, Chen ZJ. Transfer of Fresh versus Frozen Embryos in Ovulatory Women. The New England journal of medicine. 2018 Jan 11:378(2):126-136. doi: 10.1056/NEJMoa1705334. Epub [PubMed PMID: 29320646]
Level 2 (mid-level) evidenceShapiro BS, Daneshmand ST, Restrepo H, Garner FC, Aguirre M, Hudson C. Matched-cohort comparison of single-embryo transfers in fresh and frozen-thawed embryo transfer cycles. Fertility and sterility. 2013 Feb:99(2):389-92. doi: 10.1016/j.fertnstert.2012.09.044. Epub 2012 Oct 11 [PubMed PMID: 23062733]
Li Z, Wang YA, Ledger W, Edgar DH, Sullivan EA. Clinical outcomes following cryopreservation of blastocysts by vitrification or slow freezing: a population-based cohort study. Human reproduction (Oxford, England). 2014 Dec:29(12):2794-801. doi: 10.1093/humrep/deu246. Epub 2014 Oct 14 [PubMed PMID: 25316444]
Level 2 (mid-level) evidenceRoque M, Valle M, Sampaio M, Geber S. Obstetric outcomes after fresh versus frozen-thawed embryo transfers: A systematic review and meta-analysis. JBRA assisted reproduction. 2018 Sep 1:22(3):253-260. doi: 10.5935/1518-0557.20180049. Epub 2018 Sep 1 [PubMed PMID: 29782139]
Level 1 (high-level) evidenceMaheshwari A, Pandey S, Shetty A, Hamilton M, Bhattacharya S. Obstetric and perinatal outcomes in singleton pregnancies resulting from the transfer of frozen thawed versus fresh embryos generated through in vitro fertilization treatment: a systematic review and meta-analysis. Fertility and sterility. 2012 Aug:98(2):368-77.e1-9. doi: 10.1016/j.fertnstert.2012.05.019. Epub 2012 Jun 13 [PubMed PMID: 22698643]
Level 1 (high-level) evidenceKahnberg A, Enskog A, Brännström M, Lundin K, Bergh C. Prediction of ovarian hyperstimulation syndrome in women undergoing in vitro fertilization. Acta obstetricia et gynecologica Scandinavica. 2009:88(12):1373-81. doi: 10.3109/00016340903287482. Epub [PubMed PMID: 19878052]
Ashrafi M, Bahmanabadi A, Akhond MR, Arabipoor A. Predictive factors of early moderate/severe ovarian hyperstimulation syndrome in non-polycystic ovarian syndrome patients: a statistical model. Archives of gynecology and obstetrics. 2015 Nov:292(5):1145-52. doi: 10.1007/s00404-015-3723-0. Epub 2015 Apr 29 [PubMed PMID: 25920524]
Sunderam S, Kissin DM, Crawford SB, Folger SG, Jamieson DJ, Warner L, Barfield WD, Centers for Disease Control and Prevention (CDC). Assisted Reproductive Technology Surveillance - United States, 2013. Morbidity and mortality weekly report. Surveillance summaries (Washington, D.C. : 2002). 2015 Dec 4:64(11):1-25. doi: 10.15585/mmwr.ss6411a1. Epub 2015 Dec 4 [PubMed PMID: 26633040]
Sunderam S, Kissin DM, Zhang Y, Jewett A, Boulet SL, Warner L, Kroelinger CD, Barfield WD. Assisted Reproductive Technology Surveillance - United States, 2017. Morbidity and mortality weekly report. Surveillance summaries (Washington, D.C. : 2002). 2020 Dec 18:69(9):1-20. doi: 10.15585/mmwr.ss6909a1. Epub 2020 Dec 18 [PubMed PMID: 33332294]
Bailit JL. Hyperemesis gravidarium: Epidemiologic findings from a large cohort. American journal of obstetrics and gynecology. 2005 Sep:193(3 Pt 1):811-4 [PubMed PMID: 16150279]
Level 2 (mid-level) evidenceDay MC, Barton JR, O'Brien JM, Istwan NB, Sibai BM. The effect of fetal number on the development of hypertensive conditions of pregnancy. Obstetrics and gynecology. 2005 Nov:106(5 Pt 1):927-31 [PubMed PMID: 16260508]
Level 2 (mid-level) evidenceScher AI, Petterson B, Blair E, Ellenberg JH, Grether JK, Haan E, Reddihough DS, Yeargin-Allsopp M, Nelson KB. The risk of mortality or cerebral palsy in twins: a collaborative population-based study. Pediatric research. 2002 Nov:52(5):671-81 [PubMed PMID: 12409512]
Level 2 (mid-level) evidenceMcDonald SD, Han Z, Mulla S, Ohlsson A, Beyene J, Murphy KE, Knowledge Synthesis Group. Preterm birth and low birth weight among in vitro fertilization twins: a systematic review and meta-analyses. European journal of obstetrics, gynecology, and reproductive biology. 2010 Feb:148(2):105-13. doi: 10.1016/j.ejogrb.2009.09.019. Epub [PubMed PMID: 19833428]
Level 1 (high-level) evidenceJain T, Missmer SA, Hornstein MD. Trends in embryo-transfer practice and in outcomes of the use of assisted reproductive technology in the United States. The New England journal of medicine. 2004 Apr 15:350(16):1639-45 [PubMed PMID: 15084696]
Gleicher N, Oleske DM, Tur-Kaspa I, Vidali A, Karande V. Reducing the risk of high-order multiple pregnancy after ovarian stimulation with gonadotropins. The New England journal of medicine. 2000 Jul 6:343(1):2-7 [PubMed PMID: 10882762]
Wimalasundera RC. Selective reduction and termination of multiple pregnancies. Seminars in fetal & neonatal medicine. 2010 Dec:15(6):327-35. doi: 10.1016/j.siny.2010.08.002. Epub 2010 Sep 22 [PubMed PMID: 20863776]
Jackson RA, Gibson KA, Wu YW, Croughan MS. Perinatal outcomes in singletons following in vitro fertilization: a meta-analysis. Obstetrics and gynecology. 2004 Mar:103(3):551-63 [PubMed PMID: 14990421]
Level 1 (high-level) evidenceShevell T, Malone FD, Vidaver J, Porter TF, Luthy DA, Comstock CH, Hankins GD, Eddleman K, Dolan S, Dugoff L, Craigo S, Timor IE, Carr SR, Wolfe HM, Bianchi DW, D'Alton ME. Assisted reproductive technology and pregnancy outcome. Obstetrics and gynecology. 2005 Nov:106(5 Pt 1):1039-45 [PubMed PMID: 16260523]
Level 2 (mid-level) evidenceDavies MJ, Moore VM, Willson KJ, Van Essen P, Priest K, Scott H, Haan EA, Chan A. Reproductive technologies and the risk of birth defects. The New England journal of medicine. 2012 May 10:366(19):1803-13. doi: 10.1056/NEJMoa1008095. Epub 2012 May 5 [PubMed PMID: 22559061]
Level 2 (mid-level) evidenceHansen M, Kurinczuk JJ, Milne E, de Klerk N, Bower C. Assisted reproductive technology and birth defects: a systematic review and meta-analysis. Human reproduction update. 2013 Jul-Aug:19(4):330-53. doi: 10.1093/humupd/dmt006. Epub 2013 Feb 28 [PubMed PMID: 23449641]
Level 1 (high-level) evidence