Introduction
Basivertebral nerve (BVN) ablation is a minimally invasive spinal procedure targeting the BVN, which carries nociceptive information from damaged vertebral endplates, structures that have recently been postulated as sources of chronic axial low back pain (LBP).[1][2][3] Since the initial randomized clinical trials, intraosseous basivertebral nerve ablation (BVNA) has evolved into an evidence-supported intervention, with multiple systematic reviews, pooled analyses, and long-term (up to 5 years) outcome data demonstrating durable improvements in pain, function, and healthcare utilization.[4][5][6] Historically, other structures were considered the primary contributors to the etiology of chronic axial LBP, including intervertebral disks, zygapophyseal facet joints, ligaments, sacroiliac joints, and muscles. However, the recent understanding that vertebral endplates are particularly susceptible to inflammatory changes, fissuring, posttraumatic degeneration, and intraosseous edema due to their highly vascularized and innervated terminals from the basivertebral nerve and venous plexus suggests that vertebral endplates are likely contributors to LBP symptomatology, in addition to other structures.[7][8][9][10][11][12]
Finding the source of chronic axial LBP is clinically challenging because 80% of diagnoses are nonspecific LBP, and an anatomical source can be identified in only 20% of cases.[13] This variability and uncertainty may contribute to the limited success rates and variable outcomes of many interventions for chronic axial LBP that directly target anatomical structures, including the intervertebral disk, muscles, facet joints, and ligaments. Results from several studies reported a high incidence of vertebral endplate damage in up to 43% of patients with chronic axial LBP symptoms, and vertebral endplate damage tends to manifest differently than pain arising from other structures.[1][2][3][14][15] Often, patients with vertebral endplate pain tend to present with significant functional impairment and debilitating pain while seated, standing, or during spinal flexion (in contrast to extension), with the pain reported as burning, deep, and achy, located in the midline region of the lumbar spine without radicular symptoms, and without motor weakness, numbness, or tingling. Vertebral endplate pain tends to present clinically differently from nonspecific etiologies, with reported greater frequency and longer duration of painful episodes, as well as worse outcomes with conservative treatment and surgical procedures.[16][17][18][19][20]
Treatment options for chronic axial LBP from damaged vertebral endplates begin with conservative care, similar to other treatment algorithms, including oral analgesics, opioids, and therapeutic exercises; however, conservative methods tend to be ineffective. Identification and diagnosis in patients with pathoanatomical vertebral endplate damage, using history, physical examination, and diagnostic imaging, are crucial for optimizing outcomes and offering effective treatment options, such as BVN ablation.[21][22][23] Since early randomized clinical trials established the efficacy of BVNA, subsequent systematic reviews and pooled analyses have demonstrated durable clinical benefits extending beyond 5 years, including sustained pain reduction, functional improvement, and reduced opioid use. Results from these studies support BVNA as a validated intervention for a specific subset of patients with chronic vertebrogenic low back pain.[24][25][26]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Chronic axial low back pain remains a global healthcare problem, affecting 30 million people in the United States and costing the healthcare system $90 billion annually.[18][27] Given the high financial burden, clinicians and researchers need to understand the pathoanatomical considerations and phenotypic profile of chronic axial LBP associated with vertebral endplate damage to target this source and optimize treatment options and success rates. Additionally, the sinuvertebral nerve arises from the ventral rami of the spinal nerves bilaterally, takes a recurrent course, and enters the spinal canal, traveling toward the posterior aspect of the vertebra, where it enters the vertebral body through the basivertebral foramen.
This foramen lies in the midline of the posterior vertebral body and is the entry point for the neurovascular bundle comprising the basivertebral nerve and the basivertebral vascular plexus. Although anatomical variability occurs along its course, the nerve travels anteriorly into the vertebral body by about 30% to 50%, where it forms a trunk cluster of fibers that migrate cranially and caudally toward the vertebral endplates, with nociceptive fibers implicated in endplate-mediated pain. This branching point is the anatomical site targeted for the ablative procedure (see Image. Anatomical Distribution of the Basivertebral Nerve Within the Vertebral Body).[2][7][28]
Vertebral endplates are the superior and inferior edges of the vertebral body. Vertebral endplates are highly susceptible to microfracture, inflammatory degeneration, fissuring, fibrovascular ingrowths, and intraosseous edema, which are visible on MRI and commonly correlate with vertebral pain; these changes are classified as vertebral endplate Modic changes.[29][30][31] Three types of Modic changes can occur: type 1, type 2, and type 3, and these differ based on MRI findings (see Image. Sagittal MRI of the Lumbar Spine Demonstrating Modic Type 1 and Type 2 Vertebral Endplate Changes).
- Type 1 Modic changes represent vertebral endplate disruption, fissuring, degeneration, and active inflammatory vertebral endplate changes and manifest as hypointense or decreased signal intensity findings from fibrovascular intraosseous bone marrow edema on T1-weighted MRI sequences and as hyperintense or increased signal intensity findings on T2-weighted MRI sequences.
- Type 2 Modic changes represent subacute or chronic fatty bone marrow infiltration or replacement and show increased signal intensity on both T1- and T2-weighted MRI sequences.
- Type 3 Modic changes are characterized by decreased signal intensity findings on both T1- and T2-weighted MRI sequences.[3][8][31][32]
Although Modic changes are radiological findings on MRI, they have been reported to be associated with a history and physical examination compatible with axial LBP in numerous clinical and basic science studies, suggesting a positive association with a specific vertebral etiology (vertebrogenic pain). Nociceptive input from these damaged vertebral endplates carried by the BVN is directly related to inflammatory cytokines, substance P, and calcitonin gene-related peptide, as confirmed by histology with protein gene product 9.5–positive staining, supporting the BVN as a key pain mediator. In particular, type 1 Modic changes have been reported to have a stronger direct association with more debilitating, severe LBP of longer duration, greater frequency, and worse functional impairments than patients with chronic axial LBP but without Modic changes, supporting the need to focus on a treatment intervention directly targeting this pain generator, such as ablation of the BVN.[3][7][30][31][33][34]
Indications
Results from clinical studies evaluating BVN ablation consistently include patients with chronic axial LBP lasting longer than 6 months that is refractory to at least 6 months of conservative treatment. MRI findings must demonstrate Modic type 1 or type 2 changes at 1 or more vertebral endplates between L3 and S1. Patients should have significant functional impairment attributable to vertebrogenic pain, and alternative primary pain generators, such as radiculopathy, instability, or infection, should be excluded.
Results from several studies excluded patients with a history of spinal surgical procedures, spinal stenosis, and opioid use, whereas other studies' results included these patients, allowing for a more generalizable patient population more similar to daily clinical practice. Additional requirements when selecting patients for BVN ablation include documented evidence of significant functional impairment, debilitating pain unresponsive to conservative care, confirmed skeletal maturity on diagnostic imaging, and a history and physical examination excluding other potential primary sources of pain. Randomized trial criteria are consistent and reinforced by society guidelines from the International Society for the Advancement of Spine Surgery, American Society of Pain and Neuroscience, and North American Spine Society coverage recommendations. The Food and Drug Administration cleared the procedure in 2016 for patients who meet the preceding criteria.[7][22][24][26][35][36][37][38][39][40][41][42][43]
Contraindications
Contraindications to BVN ablation mirror those of other interventional spine procedures, such as systemic infections, spinal infections, pregnancy, incomplete skeletal maturity, implantable pulse generators (pacemakers, defibrillators), severe cardiopulmonary compromise, coagulopathy, patients in whom the targeted ablation zone is less than 10 mm away from a sensitive structure not intended to be ablated, including the vertebral foramen (spinal canal), and clinical situations in which unintended tissue damage may result based on the clinician’s assessment, such as spine surgical procedures at the treatment level when existing hardware is within the zone of the BVN ablation. Results from published studies reported additional exclusion criteria, including patients with severe obesity due to potential instrument length limitations when accessing the target with elevated levels of adipose tissue in the lumbar region; patients in whom symptomatic spinal stenosis or radicular pain is the primary pain source; and clinical situations in which injury may result from the procedure based on clinician assessment, such as osteoporosis (particularly in patients with prior vertebral compression fracture or who are actively taking hormonal therapy), metastatic disease or local malignant neoplasm, and bleeding risk, such as diagnosed thrombocytopenia or coagulopathy disorders.[36][37][38][44][45]
Equipment
Safe and accurate targeting of the BVN is critical to the success of the ablation procedure. The procedure is performed by a pain clinician, spine surgeon, or interventional radiologist with experience in image-guided spinal procedures, preferably with C-arm fluoroscopy or CT guidance. A combination of anteroposterior, lateral, and oblique C-arm fluoroscopic views is used to localize the pedicle and guide instrument placement.
A single C-arm is most often used; however, 2 C-arms may be used, with 1 for lateral images and 1 for anteroposterior and oblique images. In addition to CT or fluoroscopic imaging, equipment for BVN ablation includes an introducer diamond- or bevel-tipped trocar to access the vertebral body through a transpedicular approach; a curved cannula assembly with an accompanying straight stylet to create a channel in the vertebral body to the BVN terminus (target site); and a bipolar radiofrequency ablation probe and radiofrequency generator to create the ablative lesion in the nerve terminus (see Technique or Treatment section below for details). The next-generation access instruments with the EDGE J stylet (Boston Scientific) were released in 2025 and are purpose-built curved access tools intended to provide a more predictable and precise pathway to the BVN terminus. The OptaBlate system (Stryker Instruments), which recently received Food and Drug Administration clearance, offers 4 channels, allowing simultaneous ablation of up to 4 vertebral levels, a 7-minute ablation time, and a microinfuser, which is suggested to provide more consistent ablations. Additional supplies include standardized sterile surgical items, such as sterile gowns, gloves, sterile hats, shoe covers, masks, appropriate drapes, sponges, laparotomy pads, and other supplies to minimize the risk of infection.
Personnel
The procedure must be performed by a clinician experienced in image-guided spinal procedures, such as an interventional pain clinician, spine surgeon, or interventional radiologist. In addition to the clinician performing the procedure, the intraoperative personnel include a fluoroscopy technologist (radiology technologist), scrub technician, circulating nurse, and an anesthesiologist or nurse anesthetist to provide appropriate sedation and monitor the patient. Radiology support is important for confirming Modic type 1 or type 2 changes and excluding competing pathology. Device representatives may assist with equipment workflow.
Preparation
In addition to a detailed medical history and physical examination to support vertebral pain as the source of the patient's chronic axial LBP, the clinician must document radiological evidence of type 1 or type 2 Modic changes on MRI and a complete treatment history to support the rationale for the procedure, including longstanding debilitating LBP with functional impairment lasting longer than 6 months and unresponsive to at least 6 months of conservative care. The BVN ablation procedure uses a transpedicular approach similar to that used for vertebral augmentation procedures. Although no consensus exists on perioperative treatment before BVN ablation, clinicians may reasonably follow a standard of care similar to that used for other percutaneous spinal interventions. In preparation for the procedure, the following should be obtained: a complete metabolic profile, a complete blood count, and coagulation studies to assess bleeding risk and rule out underlying infection, severe thrombocytopenia, anemia, or metabolic disorders. Clinicians should also follow guidelines for blood transfusion, discontinuation of anticoagulation, and perioperative intravenous antibiotics, which vary based on the anticoagulant in question, including 2 g of cefazolin (or 600 mg of clindamycin if a patient has a penicillin allergy) 60 min before the procedure, as a prophylactic measure and standard of care for interventional spinal procedures. Based on the patient's comorbidities and the clinician's judgment, the procedure may be performed under general anesthesia or monitored anesthesia care sedation.
Technique or Treatment
BVN ablation is performed in an outpatient setting by properly trained clinicians and surgeons. The procedure has technical similarities to vertebral augmentation because both use a transpedicular approach. However, an extrapedicular approach has been described for lumbar radiofrequency ablation, which uses an ablative lesion of the BVN to interrupt nociceptive signaling from damaged vertebral endplates. The first step in this procedure is to position the patient prone under general anesthesia or monitored anesthesia care, with continuous cardiac monitoring, pulse oximetry, and blood pressure monitoring. Next, using standardized sterile technique, the patient is prepared, and the target level and entry location are marked and confirmed with C-arm fluoroscopy or computed tomography guidance. Obtaining optimal image guidance is essential for this procedure, so the C-arm should first be rotated to obtain a true anteroposterior view of the pedicles at the level of entry, thereby optimizing a transpedicular approach.
The skin entry point and angle are marked with a sterile marker, the skin is anesthetized with 1% lidocaine, and a small incision is made with a scalpel. Next, a 22-gauge spinal needle may be used at the target entry position to anesthetize the pathway toward the periosteum. An introducer trocar is placed along the same trajectory and advanced through the pedicle starting at the superolateral aspect until it passes the posterior vertebral body wall.
Maintaining a trajectory superior to the inferior cortex and lateral to the medial cortex of the pedicle is important to prevent trocar entry into the spinal canal or near neural elements. As the trocar is slowly advanced using a mallet, multiple anterior-posterior and lateral C-arm views are obtained to ensure a safe trajectory. Once the vertebral body is breached, the trocar is removed from the introducer cannula.
A curved cannula assembly (curved cannula and curved stylet) is used to facilitate the creation of a curved channel toward the target site at the BVN terminus found in the midline, approximately 30% to 50% across the vertebral body width from posterior to anterior (see Image. Transpedicular Needle Positioning). Once the target site is confirmed with anterior-posterior and lateral C-arm views, the curved stylet is removed, and a bipolar radiofrequency probe is inserted. The probe is connected to a radiofrequency generator, and radiofrequency energy is used to create an approximately 1 cm spherical lesion at the BVN terminus (75 °C to 85 °C for 7 to 15 min).
While variations in ablation duration and generator design have emerged, most long-term outcome data supporting BVNA durability come from protocols that use longer ablation times (15 min at 85 °C). Shorter ablation protocols remain under investigation. Upon completion, the radiofrequency probe and the introducer cannula are removed, and the subcutaneous tissue and skin are closed in a standard sterile fashion with a pressure dressing and skin glue or Steri-Strips (3M Health Care). Sutures or staples are usually not necessary.
Patients are transferred to a postanesthesia care unit for monitoring. Vital signs and neurological function are reassessed after the procedure. Patients should be discharged the same day. After discharge, patients should be instructed to monitor the procedure site and to be educated on signs of infection, activity restrictions (no lifting more than 15 lb, twisting, or bending of the spine), and avoidance of water submersion for at least 48 hours after the procedure. The timing of follow-up postprocedure visits and the full return to activity is at each clinician's discretion.[4][46][47][48][49][50][51]
Complications
The procedure is generally considered safe, with a very low rate of adverse events reported across all clinical studies totaling 473 procedures. Temporary exacerbation of LBP symptoms and incisional pain were the most commonly reported self-limited adverse events after the procedure. Rare adverse events reported include transient radiculitis, which resolved after oral medication, and rare instances of nonpermanent lumbar or sacral radiculopathy, nerve root injury, and motor or sensory deficits.
Serious adverse events reported in the 473 clinical procedures included 1 case of vertebral compression fracture in a patient undergoing a sham crossover procedure who was taking hormonal therapy. In commercially treated patients, 2 serious adverse events were related to the device or procedure: 1 case of retroperitoneal hemorrhage and 1 case of vertebral compression fracture. No reports have described thermal injuries, spinal cord injury, avascular necrosis, or postprocedure infections. Among adverse events related to the device or procedure reported in the clinical studies, the median time to resolution was 66.5 days postoperatively.[4][35][44] Across pooled analyses and long-term follow-up, no serious device-related adverse events have been reported, and complication rates remain low.[46]
Clinical Significance
Results from randomized controlled trials, pooled long-term analyses, systematic reviews, and real-world utilization studies demonstrated that intraosseous basivertebral nerve ablation provides consistent, clinically meaningful, and durable benefit in carefully selected patients with vertebrogenic chronic low back pain, most commonly defined by Modic type 1 or type 2 vertebral endplate changes at L3 through S1.[48][52][53] Across studies, BVNA reliably meets established thresholds for clinical significance, including at least a 10-point improvement in the Oswestry Disability Index, at least a 2-point reduction in pain scores, at least 50% pain relief, and reductions in opioid use, often within 3 months of treatment.[16][54][55][56] Durability of benefit is supported by pooled intermediate- and long-term outcomes.
At 3 years, treated patients demonstrated mean reductions of approximately 30 points in the Oswestry Disability Index and approximately 4 points in pain scores, with responder rates of approximately 70% to 75% and approximately one-quarter reporting pain-free status.[46] At 5 years, results from pooled data showed sustained reductions in pain (4.3 points) and disability (28 points), approximately one-third of patients reporting complete pain resolution, and nearly two-thirds of baseline opioid users discontinuing opioids, alongside declining use of spinal injections and no serious device- or procedure-related adverse events.[4] Results from real-world data further supported the clinical and healthcare system impact of BVNA, demonstrating reductions in opioid use and subsequent spinal interventions within the first postprocedure year, with relatively low rates of subsequent spine surgical procedures.[47]
Results from narrative and economic reviews integrating randomized, observational, and use data emphasized that vertebrogenic pain represents a distinct anterior column pain phenotype best identified through concordant clinical features and MRI–confirmed Modic changes, and suggested that BVNA may be cost-effective compared with prolonged conservative treatment in appropriately selected patients.[48][57] Although broader radiofrequency denervation strategies targeting sinuvertebral pathways show overall improvements in discogenic and vertebrogenic pain populations, current evidence underscores the importance of distinguishing BVNA as a targeted intervention for endplate-mediated vertebrogenic pain.[58] Overall, literature spanning levels 1 to 4 evidence consistently supports BVNA as a safe, durable, and effective treatment option, and contemporary society guidelines recommend its use in a defined subset of patients with chronic axial low back pain refractory to conservative therapy and with imaging evidence of vertebral endplate pathology.
Enhancing Healthcare Team Outcomes
Optimal outcomes require coordinated evaluation, shared decision-making, and follow-up across the interprofessional team. The treating clinician confirms the diagnosis, reviews MRI findings, excludes competing pain generators, discusses alternatives, obtains informed consent, performs the procedure, and treats complications. Advanced practice clinicians may support longitudinal assessment, documentation of conservative care failure, preprocedure optimization, and follow-up.
Radiologists help confirm Modic type 1 or type 2 changes and identify exclusionary pathology. Nurses coordinate preprocedure screening, medication reconciliation, education, recovery monitoring, and escalation of concerning symptoms. Pharmacists can assist with anticoagulant planning, analgesic optimization, and opioid tapering when clinically appropriate. Physical therapists help the patient transition from procedural recovery to graded activity- and function-based rehabilitation.
Nursing, Allied Health, and Interprofessional Team Interventions
Nursing and allied health professionals should verify that the patient has appropriate MRI documentation, a history of chronic axial low back pain refractory to conservative care, completed consent, medication reconciliation, allergy review, pregnancy screening when relevant, anticoagulant or antiplatelet planning, and transportation or postanesthesia instructions. The team should reinforce that BVNA is intended for vertebrogenic pain with concordant Modic type 1 or type 2 changes, not for nonspecific low back pain, radiculopathy, or untreated competing pain generators. Pharmacists may assist with perioperative medication safety, especially antithrombotic treatment and opioid stewardship. Physical therapists should tailor postoperative rehabilitation to gradual activity restoration rather than to immediate, aggressive strengthening.
Nursing, Allied Health, and Interprofessional Team Monitoring
Postprocedure monitoring should include vital signs, wound assessment, pain assessment, and a focused neurological evaluation before discharge. Patients should receive instructions to report fever, drainage, worsening back pain beyond the expected recovery course, new radicular pain, weakness, numbness, bowel or bladder dysfunction, syncope, signs of bleeding, or symptoms concerning for vertebral compression fracture. Follow-up should assess pain intensity, functional status, activity tolerance, analgesic and opioid use, adverse events, and need for additional evaluation of competing pain generators if response is incomplete. Patients with osteopenia, osteoporosis, prior compression fracture, or other fracture risk factors may require closer follow-up and coordination with primary care, endocrinology, or bone health specialists.
Media
(Click Image to Enlarge)
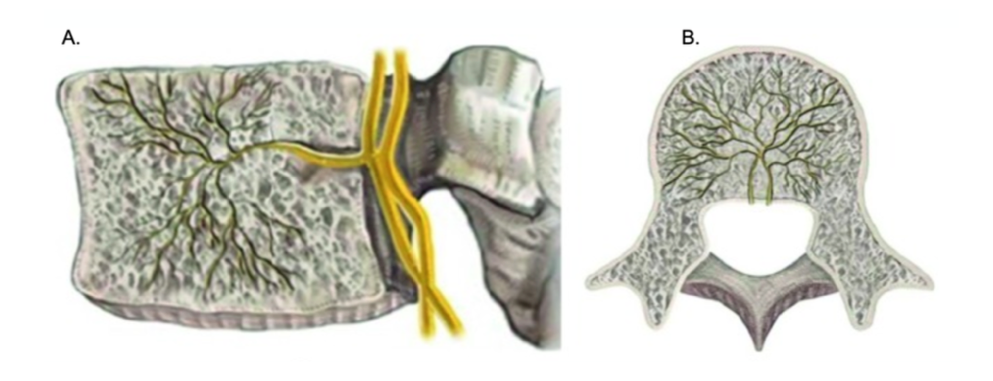
Anatomical Distribution of the Basivertebral Nerve Within the Vertebral Body. Sagittal (A) and axial views (B) of the basivertebral nerve as it enters the vertebral body through the basivertebral foramen, and the midline nerve tree, the anatomical target site for the ablative procedure.
Kim HS, Adsul N, Yudoyono F, et al. Transforaminal epiduroscopic basivertebral nerve laser ablation for chronic low back pain associated with modic changes: a preliminary open-label Study. Pain Res Manag. 2018;2018:6857983. doi: 10.1155/2018/6857983.
(Click Image to Enlarge)
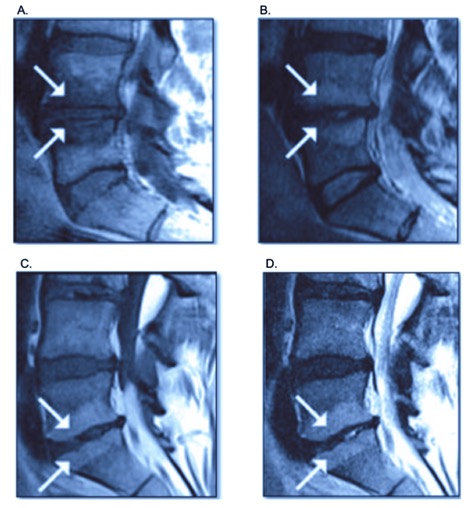
Sagittal MRI of the Lumbar Spine Demonstrating Modic Type 1 and Type 2 Vertebral Endplate Changes. The white arrows indicate the signaling changes across different MRI sequences. Modic changes type 1 (A, B) with hypodense or decreased signal intensity of fibrovascular intraosseous bone marrow edema on T1-weighted MRI sequence and as hyperintense or increased signal intensity on T2-weighted MRI sequence, while Modic type 2 (C,D) shows increased signal intensity in both T1 and T2 MRI sequence images.
Relievant Medsystems Inc.
(Click Image to Enlarge)
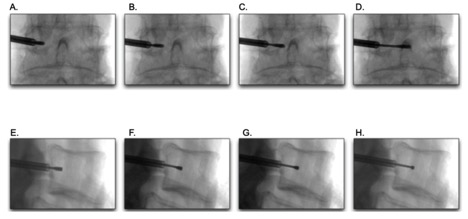
Transpedicular Needle Positioning. Transpedicular approach with safe needle advancement and placement visualized in an anterior-posterior (A-D) and lateral (E-H) fluoroscopy views towards the anatomical target.
Relievant Medsystems Inc.
References
Mok FP, Samartzis D, Karppinen J, Fong DY, Luk KD, Cheung KM. Modic changes of the lumbar spine: prevalence, risk factors, and association with disc degeneration and low back pain in a large-scale population-based cohort. The spine journal : official journal of the North American Spine Society. 2016 Jan 1:16(1):32-41. doi: 10.1016/j.spinee.2015.09.060. Epub 2015 Oct 8 [PubMed PMID: 26456851]
Tzika M, Paraskevas GK, Piagkou M, Papatolios AK, Natsis K. Basivertebral foramina of true vertebrae: morphometry, topography and clinical considerations. Surgical and radiologic anatomy : SRA. 2021 Jun:43(6):889-907. doi: 10.1007/s00276-021-02690-0. Epub 2021 Feb 17 [PubMed PMID: 33598754]
Kjaer P, Korsholm L, Bendix T, Sorensen JS, Leboeuf-Yde C. Modic changes and their associations with clinical findings. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2006 Sep:15(9):1312-9 [PubMed PMID: 16896838]
Level 2 (mid-level) evidenceKhalil JG, Truumees E, Macadaeg K, Nguyen DTD, Moore GA, Lukes D, Fischgrund J. Intraosseous basivertebral nerve ablation: A 5-year pooled analysis from three prospective clinical trials. Interventional pain medicine. 2024 Dec:3(4):100529. doi: 10.1016/j.inpm.2024.100529. Epub 2024 Dec 13 [PubMed PMID: 39758714]
Mekhail N, Eldabe S, Templeton E, Costandi S, Rosenquist R. Pain Management Interventions for the Treatment of Chronic Low Back Pain: A Systematic Review and Meta-Analysis. The Clinical journal of pain. 2023 Jul 1:39(7):349-364. doi: 10.1097/AJP.0000000000001116. Epub 2023 Jul 1 [PubMed PMID: 37104694]
Level 1 (high-level) evidenceMcCormick ZL, Fogarty AE, Conger A, Burnham T, Kendall R, Dickenson BA, Kanjanapanang N, Curtis TM, Sen H, Glinka Przybysz A, Clark T, Smolinski K, Wagner G, Teramoto M, Cooper AN. The effectiveness of basivertebral nerve radiofrequency ablation for the treatment of vertebrogenic low back pain: 1-year results of a prospective real-world cohort study. Pain medicine (Malden, Mass.). 2026 Mar 1:27(3):254-261. doi: 10.1093/pm/pnaf122. Epub [PubMed PMID: 40891888]
Kim HS, Wu PH, Jang IT. Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature. International journal of molecular sciences. 2020 Feb 21:21(4):. doi: 10.3390/ijms21041483. Epub 2020 Feb 21 [PubMed PMID: 32098249]
Level 2 (mid-level) evidenceWeishaupt D, Zanetti M, Hodler J, Min K, Fuchs B, Pfirrmann CW, Boos N. Painful Lumbar Disk Derangement: Relevance of Endplate Abnormalities at MR Imaging. Radiology. 2001 Feb:218(2):420-7 [PubMed PMID: 11161156]
Fras C, Kravetz P, Mody DR, Heggeness MH. Substance P-containing nerves within the human vertebral body. an immunohistochemical study of the basivertebral nerve. The spine journal : official journal of the North American Spine Society. 2003 Jan-Feb:3(1):63-7 [PubMed PMID: 14589248]
Kuisma M, Karppinen J, Niinimäki J, Ojala R, Haapea M, Heliövaara M, Korpelainen R, Taimela S, Natri A, Tervonen O. Modic changes in endplates of lumbar vertebral bodies: prevalence and association with low back and sciatic pain among middle-aged male workers. Spine. 2007 May 1:32(10):1116-22 [PubMed PMID: 17471095]
Bailey JF, Liebenberg E, Degmetich S, Lotz JC. Innervation patterns of PGP 9.5-positive nerve fibers within the human lumbar vertebra. Journal of anatomy. 2011 Mar:218(3):263-70. doi: 10.1111/j.1469-7580.2010.01332.x. Epub 2011 Jan 12 [PubMed PMID: 21223256]
Lotz JC, Fields AJ, Liebenberg EC. The role of the vertebral end plate in low back pain. Global spine journal. 2013 Jun:3(3):153-64. doi: 10.1055/s-0033-1347298. Epub 2013 May 23 [PubMed PMID: 24436866]
Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002. Spine. 2006 Nov 1:31(23):2724-7 [PubMed PMID: 17077742]
Level 3 (low-level) evidencePacella G, Natella R, Bruno F, Fischetti M, Bruno M, Brunese MC, Brunese M, Forte A, Forte F, Apollonio B, Romano DG, Zappia M. Subacute and Chronic Low-Back Pain: From MRI Phenotype to Imaging-Guided Interventions. Diagnostics (Basel, Switzerland). 2026 Jan 12:16(2):. doi: 10.3390/diagnostics16020240. Epub 2026 Jan 12 [PubMed PMID: 41594216]
Jensen RK, Leboeuf-Yde C, Wedderkopp N, Sorensen JS, Manniche C. Rest versus exercise as treatment for patients with low back pain and Modic changes. A randomized controlled clinical trial. BMC medicine. 2012 Feb 29:10():22. doi: 10.1186/1741-7015-10-22. Epub 2012 Feb 29 [PubMed PMID: 22376791]
Level 1 (high-level) evidenceOdonkor CA, Oghenesume O, Yoo S, Mosquera Limas S, Yeung J, Doherty P, Kadian S, Rosenberg J, Kadian SK, Whang PG. Timing and trajectory of pain and functional outcomes after basivertebral nerve ablation: a prospective cohort study. Interventional pain medicine. 2025 Dec:4(4):100652. doi: 10.1016/j.inpm.2025.100652. Epub 2025 Nov 28 [PubMed PMID: 41399736]
Amorim Filho AV, Silva AF, Lemos GA, da Silva IB, D'Angelo ER, Alvares Barbosa LM, Melo L, Moretti E. Effectiveness of interventions for the treatment of non-specific chronic low back pain in adults: An overview of systematic reviews. Journal of bodywork and movement therapies. 2025 Dec:45():894-945. doi: 10.1016/j.jbmt.2025.10.001. Epub 2025 Oct 18 [PubMed PMID: 41316666]
Level 1 (high-level) evidenceHoy D, Bain C, Williams G, March L, Brooks P, Blyth F, Woolf A, Vos T, Buchbinder R. A systematic review of the global prevalence of low back pain. Arthritis and rheumatism. 2012 Jun:64(6):2028-37. doi: 10.1002/art.34347. Epub 2012 Jan 9 [PubMed PMID: 22231424]
Level 1 (high-level) evidenceWen J, Kou M, Abed I, Park D, Muttalib Z, Alam A, Elahi F. Modic changes and their role in vertebrogenic back pain: a literature review. Skeletal radiology. 2026 Feb:55(2):249-261. doi: 10.1007/s00256-025-05065-3. Epub 2025 Nov 3 [PubMed PMID: 41177782]
Lee E, Kim J, Rahman S, Daksla N, Caldwell W, Bergese S. Basivertebral Nerve Ablation for Treatment of Lower Back Pain. Biomedicines. 2024 Sep 9:12(9):. doi: 10.3390/biomedicines12092046. Epub 2024 Sep 9 [PubMed PMID: 39335559]
Yang D, Hoehl BU, Schönnagel L, Mödl L, Zhang T, Liu S, Reitmaier S, Fleig L, Pumberger M, Schmidt H. Modic Changes Are Associated With Increased Pain Intensity, Greater Disability, and Reduced Quality of Life in Low Back Pain: A Cross-Sectional Study. Clinical orthopaedics and related research. 2025 Dec 1:483(12):2353-2363. doi: 10.1097/CORR.0000000000003565. Epub 2025 Jun 5 [PubMed PMID: 40478213]
Level 2 (mid-level) evidenceSayed D, Naidu RK, Patel KV, Strand NH, Mehta P, Lam CM, Tieppo Francio V, Sheth S, Giuffrida A, Durkin B, Khatri N, Vodapally S, James CO, Westerhaus BD, Rupp A, Abdullah NM, Amirdelfan K, Petersen EA, Beall DP, Deer TR. Best Practice Guidelines on the Diagnosis and Treatment of Vertebrogenic Pain with Basivertebral Nerve Ablation from the American Society of Pain and Neuroscience. Journal of pain research. 2022:15():2801-2819. doi: 10.2147/JPR.S378544. Epub 2022 Sep 14 [PubMed PMID: 36128549]
Level 1 (high-level) evidenceGrider JS, Deer TR, Beall DP, Murphy MZ, Fleming JW, Falowski SM, Mallard CJ, Ramawad HA, Garcia RA, Latif U, Vu CM, Christopher A, Harned ME, Patel RG, Shah AJ, Cowan IM, Jarzombek K, Tate JL, Khatri N, Graca MJ, Karcz MK, Davis TT, Barkoh K, Clerk-Lamalice O, Durkin B, Malinowski MN, Gross DK, Hedman T, Green M, Dorsi MJ, Amirdelfan K, Sayed D. A Primer on Anatomy, Biophysics, Pathology, Imaging and Treatment of the Intervertebral Disc and the Anterior Spinal Column: The Discogenic, Intervertebral, Spinal Column (DISC) ASPN Workgroup. Journal of pain research. 2025:18():6651-6698. doi: 10.2147/JPR.S553033. Epub 2025 Dec 11 [PubMed PMID: 41415801]
Fischgrund JS, Rhyne A, Franke J, Sasso R, Kitchel S, Bae H, Yeung C, Truumees E, Schaufele M, Yuan P, Vajkoczy P, Depalma M, Anderson DG, Thibodeau L, Meyer B. Intraosseous Basivertebral Nerve Ablation for the Treatment of Chronic Low Back Pain: 2-Year Results From a Prospective Randomized Double-Blind Sham-Controlled Multicenter Study. International journal of spine surgery. 2019 Apr:13(2):110-119. doi: 10.14444/6015. Epub 2019 Apr 30 [PubMed PMID: 31131209]
Level 2 (mid-level) evidenceBellow E, Johnson D, Bajrami S, Caldwell W. Safety and effectiveness of basivertebral nerve ablation in patients with osteoporosis and osteopenia: A real-world study. Interventional pain medicine. 2025 Sep:4(3):100624. doi: 10.1016/j.inpm.2025.100624. Epub 2025 Aug 14 [PubMed PMID: 40896550]
Markman JD, Rhyne AL, Sasso RC, Patel AA, Hsu WK, Fischgrund JS, Edidin AA, Vajkoczy P. Association Between Opioid Use and Patient-Reported Outcomes in a Randomized Trial Evaluating Basivertebral Nerve Ablation for the Relief of Chronic Low Back Pain. Neurosurgery. 2020 Mar 1:86(3):343-347. doi: 10.1093/neuros/nyz093. Epub [PubMed PMID: 31034561]
Level 1 (high-level) evidenceDagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. The spine journal : official journal of the North American Spine Society. 2008 Jan-Feb:8(1):8-20. doi: 10.1016/j.spinee.2007.10.005. Epub [PubMed PMID: 18164449]
Level 1 (high-level) evidenceShayota B, Wong TL, Fru D, David G, Iwanaga J, Loukas M, Tubbs RS. A comprehensive review of the sinuvertebral nerve with clinical applications. Anatomy & cell biology. 2019 Jun:52(2):128-133. doi: 10.5115/acb.2019.52.2.128. Epub 2019 Jun 30 [PubMed PMID: 31338228]
Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology. 1988 Jan:166(1 Pt 1):193-9 [PubMed PMID: 3336678]
Level 2 (mid-level) evidenceAlbert HB, Kjaer P, Jensen TS, Sorensen JS, Bendix T, Manniche C. Modic changes, possible causes and relation to low back pain. Medical hypotheses. 2008:70(2):361-8 [PubMed PMID: 17624684]
Applebaum A, Nessim A, Cho W. Modic Change: An Emerging Complication in the Aging Population. Clinical spine surgery. 2022 Feb 1:35(1):12-17. doi: 10.1097/BSD.0000000000001168. Epub [PubMed PMID: 33769981]
Jensen TS, Karppinen J, Sorensen JS, Niinimäki J, Leboeuf-Yde C. Vertebral endplate signal changes (Modic change): a systematic literature review of prevalence and association with non-specific low back pain. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2008 Nov:17(11):1407-22. doi: 10.1007/s00586-008-0770-2. Epub 2008 Sep 12 [PubMed PMID: 18787845]
Level 2 (mid-level) evidenceHerlin C, Kjaer P, Espeland A, Skouen JS, Leboeuf-Yde C, Karppinen J, Niinimäki J, Sørensen JS, Storheim K, Jensen TS. Modic changes-Their associations with low back pain and activity limitation: A systematic literature review and meta-analysis. PloS one. 2018:13(8):e0200677. doi: 10.1371/journal.pone.0200677. Epub 2018 Aug 1 [PubMed PMID: 30067777]
Level 1 (high-level) evidenceAbel F, Altorfer FCS, Rohatgi V, Gibbs W, Chazen JL. Imaging of Discogenic and Vertebrogenic Pain. Neurosurgery clinics of North America. 2025 Oct:36(4):485-496. doi: 10.1016/j.nec.2025.04.011. Epub [PubMed PMID: 41167820]
Lorio M, Clerk-Lamalice O, Beall DP, Julien T. International Society for the Advancement of Spine Surgery Guideline-Intraosseous Ablation of the Basivertebral Nerve for the Relief of Chronic Low Back Pain. International journal of spine surgery. 2020 Feb:14(1):18-25. doi: 10.14444/7002. Epub 2020 Feb 29 [PubMed PMID: 32128298]
Becker S, Hadjipavlou A, Heggeness MH. Ablation of the basivertebral nerve for treatment of back pain: a clinical study. The spine journal : official journal of the North American Spine Society. 2017 Feb:17(2):218-223. doi: 10.1016/j.spinee.2016.08.032. Epub 2016 Sep 1 [PubMed PMID: 27592808]
Fischgrund JS, Rhyne A, Franke J, Sasso R, Kitchel S, Bae H, Yeung C, Truumees E, Schaufele M, Yuan P, Vajkoczy P, DePalma M, Anderson DG, Thibodeau L, Meyer B. Intraosseous basivertebral nerve ablation for the treatment of chronic low back pain: a prospective randomized double-blind sham-controlled multi-center study. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2018 May:27(5):1146-1156. doi: 10.1007/s00586-018-5496-1. Epub 2018 Feb 8 [PubMed PMID: 29423885]
Level 1 (high-level) evidenceKim HS, Adsul N, Yudoyono F, Paudel B, Kim KJ, Choi SH, Kim JH, Chung SK, Choi JH, Jang JS, Jang IT, Oh SH. Transforaminal Epiduroscopic Basivertebral Nerve Laser Ablation for Chronic Low Back Pain Associated with Modic Changes: A Preliminary Open-Label Study. Pain research & management. 2018:2018():6857983. doi: 10.1155/2018/6857983. Epub 2018 Aug 14 [PubMed PMID: 30186540]
Khalil JG, Smuck M, Koreckij T, Keel J, Beall D, Goodman B, Kalapos P, Nguyen D, Garfin S, INTRACEPT Trial Investigators. A prospective, randomized, multicenter study of intraosseous basivertebral nerve ablation for the treatment of chronic low back pain. The spine journal : official journal of the North American Spine Society. 2019 Oct:19(10):1620-1632. doi: 10.1016/j.spinee.2019.05.598. Epub 2019 Jun 20 [PubMed PMID: 31229663]
Level 2 (mid-level) evidenceTruumees E, Macadaeg K, Pena E, Arbuckle J 2nd, Gentile J 2nd, Funk R, Singh D, Vinayek S. A prospective, open-label, single-arm, multi-center study of intraosseous basivertebral nerve ablation for the treatment of chronic low back pain. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2019 Jul:28(7):1594-1602. doi: 10.1007/s00586-019-05995-2. Epub 2019 May 21 [PubMed PMID: 31115683]
Fischgrund JS, Rhyne A, Macadaeg K, Moore G, Kamrava E, Yeung C, Truumees E, Schaufele M, Yuan P, DePalma M, Anderson DG, Buxton D, Reynolds J, Sikorsky M. Long-term outcomes following intraosseous basivertebral nerve ablation for the treatment of chronic low back pain: 5-year treatment arm results from a prospective randomized double-blind sham-controlled multi-center study. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2020 Aug:29(8):1925-1934. doi: 10.1007/s00586-020-06448-x. Epub 2020 May 25 [PubMed PMID: 32451777]
Level 1 (high-level) evidenceDe Vivo AE, D'Agostino G, D'Anna G, Al Qatami H, Gil I, Ventura F, Manfrè L. Intra-osseous basivertebral nerve radiofrequency ablation (BVA) for the treatment of vertebrogenic chronic low back pain. Neuroradiology. 2021 May:63(5):809-815. doi: 10.1007/s00234-020-02577-8. Epub 2020 Oct 13 [PubMed PMID: 33051706]
Smuck M, Khalil J, Barrette K, Hirsch JA, Kreiner S, Koreckij T, Garfin S, Mekhail N, INTRACEPT Trial Investigators. Prospective, randomized, multicenter study of intraosseous basivertebral nerve ablation for the treatment of chronic low back pain: 12-month results. Regional anesthesia and pain medicine. 2021 Aug:46(8):683-693. doi: 10.1136/rapm-2020-102259. Epub 2021 May 24 [PubMed PMID: 34031220]
Level 2 (mid-level) evidenceNguyen KML, Nguyen DTD. Minimally Invasive Treatment for Degenerative Lumbar Spine. Techniques in vascular and interventional radiology. 2020 Dec:23(4):100700. doi: 10.1016/j.tvir.2020.100700. Epub 2020 Oct 5 [PubMed PMID: 33308584]
Urits I, Noor N, Johal AS, Leider J, Brinkman J, Fackler N, Vij N, An D, Cornett EM, Kaye AD, Viswanath O. Basivertebral Nerve Ablation for the Treatment of Vertebrogenic Pain. Pain and therapy. 2021 Jun:10(1):39-53. doi: 10.1007/s40122-020-00211-2. Epub 2020 Oct 31 [PubMed PMID: 33128702]
Smuck M, Truumees E, Macadaeg K, Jaini AM, Chatterjee S, Levin J. Intraosseous basivertebral nerve ablation: Pooled long-term outcomes from two prospective clinical trials. Interventional pain medicine. 2023 Jun:2(2):100256. doi: 10.1016/j.inpm.2023.100256. Epub 2023 Jun 10 [PubMed PMID: 39238665]
Stephens AR, Aktas AF, El-Hassan R. Decrease in opioid use and spinal interventions after basivertebral nerve ablation. Interventional pain medicine. 2025 Jun:4(2):100594. doi: 10.1016/j.inpm.2025.100594. Epub 2025 May 30 [PubMed PMID: 40519794]
Mahendram S, Christo PJ. Advances in Basivertebral Nerve Ablation for Chronic Low Back Pain: A Narrative Review. Journal of personalized medicine. 2025 Mar 19:15(3):. doi: 10.3390/jpm15030119. Epub 2025 Mar 19 [PubMed PMID: 40137435]
Level 3 (low-level) evidenceKhan M, Choi R, Manupipatpong S, Schick J, Gad M. Basi-Vertebral Nerve Ablation (BVNA): Part 1. AJNR. American journal of neuroradiology. 2026 Feb 16:():. pii: ajnr.A9242. doi: 10.3174/ajnr.A9242. Epub 2026 Feb 16 [PubMed PMID: 41698818]
Khan M, Foote C, Choi R, Manupipatpong S, Schick J, Gad M. Basi-Vertebral Nerve Ablation (BVNA): Part 2. AJNR. American journal of neuroradiology. 2026 Feb 16:():. pii: ajnr.A9241. doi: 10.3174/ajnr.A9241. Epub 2026 Feb 16 [PubMed PMID: 41698821]
Tieppo Francio V, Sherwood D, Twohey E, Barndt B, Pagan-Rosado R, Eubanks J, Sayed D. Developments in Minimally Invasive Surgical Options for Vertebral Pain: Basivertebral Nerve Ablation - A Narrative Review. Journal of pain research. 2021:14():1887-1907. doi: 10.2147/JPR.S287275. Epub 2021 Jun 23 [PubMed PMID: 34188535]
Level 3 (low-level) evidenceConger A, Schuster NM, Cheng DS, Sperry BP, Joshi AB, Haring RS, Duszynski B, McCormick ZL. The Effectiveness of Intraosseous Basivertebral Nerve Radiofrequency Neurotomy for the Treatment of Chronic Low Back Pain in Patients with Modic Changes: A Systematic Review. Pain medicine (Malden, Mass.). 2021 May 21:22(5):1039-1054. doi: 10.1093/pm/pnab040. Epub [PubMed PMID: 33544851]
Level 1 (high-level) evidenceNwosu M, Agyeman WY, Bisht A, Gopinath A, Cheema AH, Chaludiya K, Khalid M, Yu AK. The Effectiveness of Intraosseous Basivertebral Nerve Ablation in the Treatment of Nonradiating Vertebrogenic Pain: A Systematic Review. Cureus. 2023 Apr:15(4):e37114. doi: 10.7759/cureus.37114. Epub 2023 Apr 4 [PubMed PMID: 37034146]
Level 1 (high-level) evidenceBaker P, Pal D, Kendall C, Avula LV, Papanikitas J, Yanny S, Hughes R, McKean D. Recent Advances and Immediate Future of Spinal Intervention. Seminars in musculoskeletal radiology. 2026 Mar 30:():. doi: 10.1055/a-2820-0900. Epub 2026 Mar 30 [PubMed PMID: 41911690]
Level 3 (low-level) evidenceBellow E, Bae J, Zhang J, Bajrami S, Johnson D, Caldwell W. Basivertebral nerve ablation provides comparable early pain relief in patients with psychiatric conditions: A real-world study. Interventional pain medicine. 2026 Mar:5(1):100743. doi: 10.1016/j.inpm.2026.100743. Epub 2026 Feb 24 [PubMed PMID: 41777429]
Stephens AR, Wozniak GH, El-Hassan R, Aktas AF. Evaluating the effectiveness of 7-min basivertebral nerve ablation in treating vertebrogenic low back pain. Interventional pain medicine. 2025 Dec:4(4):100714. doi: 10.1016/j.inpm.2025.100714. Epub 2025 Dec 3 [PubMed PMID: 41438936]
Smuck M, McCormick ZL, Gilligan C, Hailey MK, Quinn ML, Bentley A, Metcalfe K, Bradbury B, Lukes DJ, Taylor RS. A cost-effectiveness analysis of intraosseous basivertebral nerve ablation for the treatment of chronic low back pain. The spine journal : official journal of the North American Spine Society. 2025 Feb:25(2):201-210. doi: 10.1016/j.spinee.2024.09.016. Epub 2024 Sep 25 [PubMed PMID: 39332685]
Moneim MA, Nathani KR, Michalopoulos GD, Johnson SE, Jarrah R, Ibrahim S, Pittelkow TP, Olatoye DO, Brinjikji W, Bydon M. Radiofrequency ablation of basivertebral and sinuvertebral nerves for chronic discogenic low back pain: a systematic review and meta-analysis. Neurosurgical review. 2025 Apr 14:48(1):364. doi: 10.1007/s10143-025-03527-9. Epub 2025 Apr 14 [PubMed PMID: 40229490]
Level 1 (high-level) evidence