Introduction
Corneral Laceration Overview
Ocular injury is common, with an estimated 24 million people in the United States suffering an eye injury.[1] Injuries to the eye vary in severity, from a small scratch to the cornea (corneal abrasion) to a split in the external structure (globe rupture). Globe rupture can occur in various parts of the eye; for example, a corneal laceration (see Image. Normal Cornea). In a review of 890 eye injuries in Iraq and Afghanistan from 2001 to 2011, 20.7% involved a corneal laceration.[2] Corneal lacerations vary in size and shape, can be partial or full-thickness, and range from a simple linear pattern to a complex stellate formation. All lacerations require urgent repair to reduce the risk of infection, decrease tissue necrosis, and alleviate patient discomfort. The typical recommendation for a repair is within 24 hours.[3] The repair of a corneal laceration often requires suturing; however, tissue adhesives or contact lenses can close lacerations less than 2 mm.[4] The goal of any repair is a watertight closure, restoration of normal anatomy, and limitation of postoperative corneal scarring and astigmatism.[5][6]
Corneal laceration represents one of the most vision-threatening forms of anterior segment trauma and continues to be a major contributor to avoidable visual morbidity worldwide. While ocular trauma spans a wide clinical spectrum, injuries involving disruption of corneal integrity demand particular attention because of the cornea’s dual role in both structural protection and optical precision. Even minor alterations in corneal architecture can significantly affect refractive outcomes, making timely and meticulous repair essential not only for globe preservation but also for visual rehabilitation. Over the past decade, evolving surgical techniques, biomaterials, and imaging modalities have substantially refined the approach to corneal wound management, shifting the focus from mere closure to functional and anatomical restoration.[7]
The epidemiology of corneal lacerations reflects both environmental exposures and occupational risks, with a higher incidence reported among young males, industrial workers, agricultural settings, and conflict zones. In developing countries, delayed presentation, lack of access to specialized care, and higher rates of contaminated injuries further complicate outcomes. In contrast, developed settings are witnessing an increasing proportion of high-velocity and iatrogenic injuries, including those associated with refractive procedures and intraocular surgeries. These variations underscore the importance of tailoring management strategies to the mechanism, timing, and available resources.[8]
From a pathophysiological standpoint, corneal lacerations disrupt the highly organized stromal collagen lamellae, leading to loss of biomechanical strength and transparency. Full-thickness injuries additionally compromise intraocular pressure homeostasis and may be associated with prolapse of intraocular contents, increasing the risk of endophthalmitis. The wound-healing response is characterized by keratocyte apoptosis, activation of fibroblasts and myofibroblasts, and deposition of a disorganized extracellular matrix, all of which contribute to scar formation and irregular astigmatism. Contemporary research has emphasized the role of molecular mediators, eg, transforming growth factor-beta (TGF-β) and matrix metalloproteinases, in modulating this healing cascade, opening avenues for targeted therapeutic interventions.[9]
Corneal Laceration Assessment
Modern classification systems now go beyond simple descriptors of size and depth, incorporating factors, eg, wound configuration, location (central vs peripheral), associated ocular injuries, and presence of contamination. This has practical implications in surgical planning, prognostication, and selection of adjunctive therapies. For instance, central corneal lacerations carry a higher risk of visually significant scarring, whereas peripheral injuries may be complicated by limbal stem cell deficiency or secondary angle involvement.[10]
Advances in diagnostic imaging have significantly enhanced preoperative assessment. High-resolution anterior segment optical coherence tomography (AS-OCT) allows precise delineation of wound depth, configuration, and apposition, even in edematous or opaque corneas. Ultrasound biomicroscopy (UBM) serves as an adjunct in cases with suspected posterior extension or associated anterior segment trauma. These imaging modalities not only aid in surgical decision-making but also facilitate postoperative monitoring of wound integrity and healing dynamics.[11]
General Principles of Corneal Laceration Repair
The principles of corneal laceration repair have evolved from simple suturing techniques to a more nuanced, individualized approach. The primary objective remains the restoration of globe integrity; however, increasing emphasis is being placed on minimizing surgically induced astigmatism and optimizing visual outcomes. Microsurgical techniques using 10-0 or 11-0 nylon sutures remain the gold standard for full-thickness lacerations. Recent refinements include selective suture placement guided by intraoperative keratoscopy or microscope-integrated optical coherence tomography (MI-OCT), enabling real-time assessment of wound apposition and curvature.[12]
For smaller or partial-thickness lacerations, nonsuturing modalities have gained prominence. Cyanoacrylate and fibrin-based tissue adhesives are increasingly utilized, offering the advantages, eg, reduced surgical time, minimal tissue manipulation, and decreased postoperative inflammation. Bandage contact lenses, often used in conjunction with adhesives, provide additional mechanical support and promote epithelial healing. However, careful patient selection is critical, as these modalities may not be suitable for contaminated or irregular wounds.[13]
A notable recent development is the integration of biologic and regenerative therapies into corneal wound management. Amniotic membrane transplantation (AMT), with its anti-inflammatory, anti-fibrotic, and proepithelialization properties, has emerged as a valuable adjunct in selected cases. Both sutured and sutureless techniques (eg, ProKera devices) are being employed, particularly in cases with epithelial defects or high risk of scarring. Additionally, experimental approaches involving stem cell therapy and bioengineered corneal substitutes are being explored, although their routine clinical application remains limited at present.[14]
The perioperative management of corneal lacerations has also undergone significant refinement. Broad-spectrum antimicrobial prophylaxis remains a cornerstone, especially in high-risk or contaminated injuries. Recent trends favor the use of intracameral antibiotics in selected cases to reduce the risk of endophthalmitis. Anti-inflammatory therapy, including topical corticosteroids, is carefully titrated to balance the need for reducing inflammation against the risk of delayed healing or infection. The role of systemic therapy is guided by the extent of injury and associated ocular or adnexal involvement.[15]
Postoperative rehabilitation is increasingly recognized as a critical component of overall management. Early detection and management of complications, eg, wound leak, infection, and suture-related problems, are essential. Advances in corneal topography and tomography have enabled precise assessment of postrepair astigmatism, facilitating timely optical correction with spectacles, contact lenses, or refractive procedures. In selected cases, secondary interventions, eg, suture adjustment, selective suture removal, or even corneal transplantation, may be required to optimize visual outcomes.[16]
Evolving Advancements
One of the most significant paradigm shifts in recent years has been the emphasis on interprofessional and staged management of complex ocular trauma. Collaboration between cornea specialists, vitreoretinal surgeons, and oculoplastic surgeons is often necessary, particularly in cases involving posterior segment injury or adnexal damage. The concept of “damage control ophthalmology,” analogous to trauma surgery principles, advocates for initial stabilization followed by definitive reconstruction once the ocular environment is optimized.[17]
Technological innovations are also shaping the future of corneal laceration repair. Femtosecond laser-assisted corneal surgery, although primarily used in refractive and keratoplasty procedures, is being explored for its potential to create precise wound edges and facilitate customized repair. Similarly, the use of artificial intelligence (AI) in trauma assessment and surgical planning is an emerging field, with preliminary studies demonstrating its utility in predicting outcomes and guiding decision-making.[18]
Despite these advancements, several challenges remain. Access to specialized care continues to be a major limitation in low-resource settings, where the burden of ocular trauma is often highest. Training in microsurgical techniques, availability of appropriate instruments and materials, and timely referral systems are critical areas that require ongoing attention. Furthermore, standardized protocols and multicentric studies are needed to establish evidence-based guidelines for various aspects of corneal laceration management.[19]
Therefore, the management of corneal lacerations has evolved into a highly specialized and dynamic field that integrates principles of microsurgery, regenerative medicine, and advanced imaging. The focus has shifted from mere anatomical repair to achieving optimal functional outcomes, with an emphasis on preserving corneal transparency and minimizing refractive distortion. Continued research, technological innovation, and global efforts to improve access to care will be key to further improving outcomes in this challenging yet critical domain of ophthalmology.[20]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
A normal human cornea is transparent and avascular. The cornea provides structural support to the eye and acts as a barrier to infections. The average adult cornea is 12 mm horizontally by 11 mm vertically and 0.5 mm in thickness. The cornea has 5 distinct layers, starting from the outer surface: epithelium, Bowman membrane, stroma, Descemet membrane, and endothelium. In 2013, a sixth layer, called Dua’s layer, was reported, situated between the stroma and Descemet membrane. About 80% to 85% of the cornea is the stroma, which consists of type I and V collagen fibers arranged in specific parallel patterns to maintain transparency. The endothelial layer is monocellular and responsible for the cornea's optical clarity by maintaining its dehydration via the sodium-potassium pump.[21]
The corneal layers respond differently when injured. Injury to the epithelial layer leads to cell destruction and a subsequent defect in the layer. This defect will heal by migrating epithelial cells created at the limbus. About an hour after the injury, the epithelial wound healing starts.[22] Until the defect has healed, the cornea is at significant risk of infection. If the depth of the injury does not extend to the Bowman membrane, the cornea heals without scarring. An injury to the stroma heals with fibrotic deposition, which seals a wound but interferes with normal function. Excessive fibrotic tissue repair leads to increased scarring and contracture, limiting optical clarity.
Endothelial cells do not regenerate; therefore, when injured, the cornea may become edematous and cloudy due to loss of sodium-potassium pump function. The cornea is a highly innervated and sensitive tissue, which receives sensation from the nasociliary branch of the ophthalmic division of the trigeminal nerve.[23] Due to the dense innervation, a patient can feel extreme pain from a corneal injury.
Beyond its basic structural description, the cornea is a highly specialized, optically precise, and metabolically active tissue that contributes nearly two-thirds of the eye’s total refractive power (approximately +43 diopters). This refractive function is critically dependent on the smoothness of the anterior surface, the uniformity of stromal collagen architecture, and the maintenance of relative stromal dehydration. Even subtle disruptions in any of these parameters, eg, those induced by trauma, can result in significant visual degradation through irregular astigmatism and higher-order aberrations.[24]
Microstructural Organization and Transparency Mechanisms
Corneal transparency is not merely a passive property but the result of highly regulated ultrastructural organization. The stromal collagen fibrils are uniformly spaced at distances smaller than the wavelength of visible light, allowing destructive interference of scattered light (Maurice theory). Proteoglycans, eg, keratan sulfate and chondroitin sulfate, play a crucial role in maintaining this precise interfibrillar spacing. Additionally, the relative absence of blood vessels and the presence of crystallin proteins within keratocytes further enhance optical clarity.[12]
Recent insights have highlighted the biomechanical anisotropy of the cornea, in which collagen lamellae are preferentially oriented along the meridional axes, particularly in the central cornea. This organization confers tensile strength and resistance to deformation, which becomes clinically relevant in trauma, where wound configuration often follows these biomechanical lines.[7]
Corneal Metabolism and Oxygenation
Unlike many other tissues, the cornea relies on multiple sources for metabolic support. Oxygen is primarily derived from the atmosphere via diffusion through the tear film, while the aqueous humor supplies nutrients (eg, glucose). The peripheral cornea also receives limited support from the limbal vasculature. The epithelium exhibits high metabolic activity, relying on aerobic glycolysis, whereas the endothelium is more dependent on oxidative phosphorylation to sustain its intensive pump function.[25]
Tear film plays an essential physiological role beyond lubrication. The film provides oxygen, antimicrobial peptides (eg, lysozyme, lactoferrin), and growth factors that facilitate epithelial maintenance and repair. Disruption of the tear film, as seen in trauma or surface irregularity, can significantly delay healing and predispose to secondary infection.[26]
Limbal Stem Cell Niche and Regenerative Capacity
The limbus serves as a critical reservoir of epithelial stem cells located in the palisades of Vogt. These cells are responsible for continuous epithelial turnover and regeneration following injury. Damage extending to the limbal region can compromise this regenerative capacity, resulting in limbal stem cell deficiency (LSCD), characterized by conjunctivalization, persistent epithelial defects, and vascularization.
Recent advances have identified key molecular regulators of this niche, including Wnt signaling pathways, p63 transcription factor, and extracellular matrix components. Clinically, preservation of limbal integrity during trauma repair is crucial, and emerging therapies, eg, cultivated limbal epithelial transplantation (CLET) and simple limbal epithelial transplantation (SLET), are increasingly utilized in severe cases.[27]
Corneal Immune Privilege and Defense Mechanisms
The cornea is considered an immune-privileged site due to several protective adaptations. These include the absence of vasculature, the expression of anti-inflammatory cytokines (eg, TGF-β), and the presence of immune-modulating cells (eg, Langerhans cells) primarily in the peripheral cornea. However, trauma disrupts this delicate balance, leading to activation of innate immune pathways.
Epithelial cells express toll-like receptors (TLRs) that recognize microbial components and initiate inflammatory cascades. While this response is protective, excessive inflammation can exacerbate stromal damage and scarring. Understanding this balance is crucial in postoperative management, where inflammation is necessary for optimal healing.[28]
Corneal Hydration Control and Deturgescence
The concept of corneal deturgescence, the state of relative dehydration necessary for transparency, is tightly regulated by endothelial pump-leak mechanisms. The endothelium actively transports ions (primarily bicarbonate and chloride) out of the stroma, creating an osmotic gradient that draws water into the anterior chamber. Aquaporin channels facilitate this fluid movement. In the context of injury, even localized endothelial damage can disrupt this equilibrium, leading to stromal edema. Clinically, this manifests as corneal haze and reduced visual acuity. Persistent endothelial dysfunction may necessitate endothelial keratoplasty procedures, eg, DSEK or DMEK.[29]
Corneal Innervation and Biomechanical Properties
The cornea is among the most densely innervated tissues in the human body, with nerve endings forming a subbasal plexus beneath the epithelium. These nerves not only mediate sensation but also play a trophic role in maintaining epithelial health. Neurotrophic factors, eg, substance P and nerve growth factor, are essential for epithelial integrity and wound healing. Trauma can sever these nerve fibers, leading to reduced corneal sensitivity (hypoesthesia) and impaired healing, a condition termed neurotrophic keratopathy. Recent therapeutic advances include recombinant human nerve growth factor (cenegermin), which has shown promising results in restoring corneal integrity in such cases.[23]
Corneal biomechanics have gained increasing importance with the advent of diagnostic tools, eg, corneal hysteresis measurement and dynamic Scheimpflug imaging. The viscoelastic properties of the cornea influence how it responds to surgical manipulation. Thinner or structurally compromised corneas are more prone to deformation and poor wound apposition. In trauma settings, understanding these biomechanical principles aids in planning suture placement and tension distribution, and in predicting postoperative astigmatism. Modern surgical approaches aim to restore not only anatomical continuity but also biomechanical stability.[30]
Healing Modulation and Emerging Concepts
Recent research has focused on modulating corneal wound healing to minimize fibrosis. Anti-TGF-β therapies, matrix metalloproteinase inhibitors, and antifibrotic agents such as mitomycin-C are being explored for the treatment of stromal scarring. Additionally, corneal cross-linking (CXL), traditionally used in keratoconus, is being investigated for its role in stabilizing the cornea postinjury by enhancing collagen. Another emerging concept is the use of bioengineered scaffolds and nanofiber matrices that mimic stromal architecture, promoting organized healing rather than scar formation. Still largely experimental, these innovations represent the future of regenerative corneal therapy.[31]
Integrated Functional Perspective
In summary, the cornea is not merely a passive tissue but a dynamic, highly regulated structure that integrates structural, optical, neural, and immunological functions. Each layer contributes uniquely to maintaining vision, and disruption at any level, whether epithelial, stromal, or endothelial, has distinct clinical consequences. Modern understanding emphasizes that successful management of corneal injury requires not only anatomical repair but also preservation of these intricate physiological processes to ensure optimal visual recovery.[32]
Indications
A diagnosis of corneal laceration by slit-lamp examination is an indication for repair. Signs and symptoms of a corneal laceration after trauma are decreased vision, ocular pain, a positive Seidel test, an irregular pupil, eg, a peaked or teardrop pupil, an intraocular foreign body, and prolapse of intraocular contents. If a corneal laceration is suspected, but the view on examination is limited due to an uncooperative patient or eyelid edema, the patient should go to the operating room for an exam under anesthesia and globe exploration. A corneal laceration repair should be performed urgently to reduce the risk of infection, tissue necrosis, and peripheral anterior synechiae formation, and to alleviate patient discomfort. No specific time for repair has been reported in the literature, but standard practice is to complete it within 24 hours.
The diagnosis of a corneal laceration on slit-lamp biomicroscopy mandates prompt surgical consideration, as delay in intervention significantly increases the risk of irreversible visual loss. While classical clinical signs, eg, reduced visual acuity, ocular pain, a positive Seidel test, an irregular or peaked pupil, the presence of an intraocular foreign body, and prolapse of intraocular contents, remain the cornerstone of diagnosis, contemporary practice emphasizes a more comprehensive and stratified approach to identifying surgical indications.[12][15]
In modern ophthalmic trauma care, the decision to proceed with repair is based not only on the presence of a full-thickness defect but also on wound morphology, location, associated ocular injuries, and the risk of secondary complications (see Table 1). Central corneal lacerations, even if small, warrant urgent repair due to their profound impact on visual axis clarity and refractive integrity. Peripheral lacerations, although sometimes less visually significant, may predispose to anterior chamber instability, peripheral anterior synechiae, and secondary glaucoma if left untreated.
A critical but often underemphasized indication is wound leak without obvious tissue prolapse. Even micro-leaks, detectable only via Seidel testing or AS-OCT, can lead to hypotony, increased susceptibility to infection, and compromised wound healing. Similarly, stellate, ragged, or multiplanar lacerations require surgical intervention due to poor spontaneous apposition and a higher risk of irregular astigmatism.[17]
Another important consideration is the presence of associated anterior segment injuries, eg, traumatic cataract, iris incarceration, or hyphema. These conditions not only complicate the primary injury but also necessitate a controlled surgical environment for simultaneous or staged management. In pediatric patients, the threshold for intervention is even lower due to the heightened risk of amblyopia and the challenges in clinical assessment. When clinical examination is limited due to blepharospasm, lid edema, severe pain, or patient noncooperation, examination under anesthesia (EUA) with globe exploration becomes both a diagnostic and therapeutic step. This is particularly relevant in high-velocity injuries where occult globe penetration or intraocular foreign bodies may be missed on initial evaluation.[16]
Recent advancements have also introduced imaging-based indications. AS-OCT can identify partial-thickness versus full-thickness involvement, wound gape, and internal architecture, guiding the need for surgical repair. Similarly, computed tomography (CT) imaging is essential in suspected intraocular or intraorbital foreign bodies, which independently constitute an indication for surgical exploration. Timing remains a critical determinant of outcome. Although no universally fixed timeline exists, current best practices strongly advocate repair within 12 to 24 hours, especially for open-globe injuries, to minimize microbial contamination, prevent stromal necrosis, and reduce inflammatory sequelae. In contaminated or agricultural injuries, even earlier intervention is often recommended due to the high risk of fungal or atypical infections.[33]
Table 1. Indications for Corneal Laceration Repair
|
Category |
Specific Indication |
Clinical Significance |
Surgical Implication |
|
Structural Integrity |
Full-thickness corneal laceration |
Open globe with risk of collapse and infection |
Immediate surgical closure required |
|
Wound leak (positive Seidel test) |
Hypotony, infection risk |
Urgent repair to restore watertight integrity |
|
|
Stellate, irregular, or gaping wounds |
Poor self-sealing potential |
Requires suturing for proper apposition |
|
|
Visual Axis Involvement |
Central corneal laceration |
High risk of visual impairment |
Early, precise repair to minimize scarring |
|
Induced irregular astigmatism |
Optical distortion |
Structured suturing to restore curvature |
|
|
Intraocular Involvement |
Iris prolapse or incarceration |
Risk of necrosis, synechiae |
Surgical repositioning or excision |
|
Lens capsule violation / traumatic cataract |
Secondary inflammation, opacity |
Combined or staged lens management |
|
|
Vitreous prolapse |
Risk of retinal traction |
Anterior vitrectomy may be required |
|
|
Foreign Body |
Intraocular foreign body (IOFB) |
Infection, toxicity (eg, siderosis) |
Surgical removal with wound repair |
|
Organic/contaminated material |
High infection risk |
Urgent exploration and debridement |
|
|
Anterior Segment Complications |
Hyphema with wound instability |
Increased intraocular pressure (IOP), inflammation |
Surgical stabilization of the globe |
|
Peripheral anterior synechiae risk |
Secondary glaucoma |
Early repair to prevent angle closure |
|
|
Patient Factors |
Pediatric trauma |
Amblyopia risk, poor cooperation |
Early intervention is often under anesthesia |
|
Uncooperative patient/poor visualization |
Missed diagnosis risk |
EUA with globe exploration indicated |
|
|
Imaging-Based |
AS-OCT showing a full-thickness defect |
Confirms surgical necessity |
Guides surgical planning |
|
CT evidence of IOFB or globe rupture |
Hidden injury |
Mandates urgent surgical intervention |
|
|
Infective Risk |
Contaminated or agricultural injury |
High fungal/bacterial risk |
Emergency repair plus antimicrobial therapy |
|
Delayed presentation with inflammation |
Increased necrosis risk |
Aggressive surgical and medical management |
Additional Practical Considerations
The following management considerations should also be kept in mind:
- Microperforations and self-sealing wounds: Selected very small (<2 mm), well-apposed, nonleaking lacerations may be managed conservatively with bandage contact lenses or tissue adhesives. However, strict monitoring is essential, and any sign of leak or infection shifts the indication toward surgical repair.
- Role of tissue adhesives: Increasingly used in small linear lacerations, especially in noncentral locations. They reduce surgical time and avoid suture-induced astigmatism but are contraindicated in infected or irregular wounds.
- Endophthalmitis prophylaxis: Modern protocols emphasize early intravitreal or intracameral antibiotics in high-risk cases, making early repair even more critical.
- Combined surgical approach: In complex trauma, primary corneal repair is often combined with anterior vitrectomy, lens removal, or secondary procedures, following the principle of staged reconstruction.[34]
Indications for corneal laceration repair have evolved from a purely structural perspective to a comprehensive, function-oriented approach. Current practice integrates clinical findings, imaging modalities, wound characteristics, and patient-specific factors to guide timely intervention. The overarching principle remains early, meticulous, and individualized repair to preserve both the integrity of the globe and long-term visual function.[35]
Contraindications
The patient must be hemodynamically stable before the repair. In the setting of polytrauma, the risk of general anesthesia may make a corneal laceration repair unsafe.[36] While corneal laceration repair is typically an urgent, vision- and globe-saving intervention, immediate repair must be deferred or modified in specific clinical situations to avoid life-threatening complications or poor surgical outcomes (see Table 2). The fundamental principle is that systemic stabilization takes precedence over ocular intervention, particularly in polytrauma settings.
The requirement for hemodynamic stability before proceeding to surgery cannot be overemphasized. Patients with ongoing hemorrhage, shock, unstable vital parameters, or compromised airway are at significant risk during anesthesia. In such scenarios, attempting ophthalmic repair may worsen systemic outcomes. Therefore, the decision to delay surgery is not a contraindication to repair itself, but rather a temporary contraindication to immediate intervention under unsafe conditions.[33]
In addition to systemic factors, certain ocular and periocular conditions may necessitate postponement or modification of the repair strategy. These include overwhelming infection, extensive tissue necrosis, or situations where primary closure is not feasible due to tissue loss. Furthermore, logistical constraints, eg, a lack of surgical expertise, appropriate instrumentation, or a sterile environment, may necessitate temporary stabilization and referral.[37]
Table 2. Contraindications to Immediate Corneal Laceration Repair
|
Category |
Contraindication |
Clinical Rationale |
Recommended Approach |
|
Systemic (Absolute) |
Hemodynamic instability (shock, active bleeding) |
High perioperative mortality risk |
Stabilize first (ABCs), delay ocular surgery |
|
Severe head injury (raised ICP, GCS compromise) |
Anesthesia risk, poor neurological prognosis |
Neurosurgical priority, defer repair |
|
|
Unstable airway or respiratory compromise |
Risk of intraoperative hypoxia |
Secure the airway before considering surgery |
|
|
Systemic (Relative) |
Polytrauma requiring life-saving surgery |
Competing surgical priorities |
Perform ocular repair after stabilization |
|
Uncontrolled systemic infection/sepsis |
Increased surgical risk, poor healing |
Initiate systemic therapy first |
|
|
Coagulopathy/anticoagulation |
Risk of intraoperative hemorrhage |
Correct coagulation parameters |
|
|
Ocular (Absolute) |
Unsalvageable globe (e.g., complete disruption, no light perception with poor prognosis) |
No functional recovery expected |
Consider primary enucleation/evisceration |
|
Ocular (Relative) |
Extensive corneal tissue loss |
Inability to achieve watertight closure |
Temporary measures → tectonic graft later |
|
Severe ocular infection (e.g., fulminant keratitis/endophthalmitis) |
Risk of spreading infection |
Control infection before definitive repair |
|
|
Gross contamination (organic matter, soil) |
High risk of fungal/bacterial infection |
Debridement plus antimicrobial therapy first |
|
|
Marked lid edema is preventing access |
Poor visualization |
Delay or perform EUA when feasible |
|
|
Logistical/Practical |
Lack of surgical expertise |
Risk of suboptimal repair |
Stabilize and refer urgently |
|
Inadequate OT setup/instruments |
Compromised surgical quality |
Temporary closure (eg, glue) and transfer |
|
|
Patient does not consent (if conscious) |
Ethical/legal issue |
Counsel and proceed after consent |
Key Practical Insights
The following concepts should guide corneal laceration repair decisions:
- Damage control ophthalmology concept: Similar to trauma surgery, initial management may involve temporary globe stabilization (eg, tissue adhesive, shield, systemic antibiotics) followed by definitive repair once the patient is stable.
- Anesthesia considerations: General anesthesia is preferred in most cases, but in unstable patients, local or regional anesthesia may be considered cautiously in selected minor injuries, though rarely feasible in true lacerations.
- Temporary measures: In cases where immediate surgery is contraindicated, these temporary measures help bridge the gap until definitive repair
- Eye shield placement
- Broad-spectrum IV antibiotics
- Tetanus prophylaxis
- Avoidance of pressure on the globe
- Polytrauma priority principle: “Life over sight”; systemic survival always takes precedence over ocular salvage.[38]
Contraindications to corneal laceration repair are primarily contextual rather than absolute, with systemic instability being the most critical limiting factor. The decision to delay surgery should be strategic and temporary, aimed at optimizing patient survival and eventual surgical success. Modern management emphasizes an interprofessional, staged approach, ensuring that once conditions permit, definitive repair is performed under the safest and most controlled circumstances possible.[15]
Equipment
Equipment that may be utilized with corneal laceration repair procedures includes:
- Microscope or surgical loupes
- Surgical preparation kit (sponges, 5% povidone-iodine)
- Surgical eye drapes
- Suture: 10-0 nylon (if limbus or scleral involved: 9-0 and 8-0) on a prime reverse cutting or spatulated needle (see Table 3)
- Eyelid speculum (Jaffe or Schott prevents pressure on the globe); eyelid sutures can be an alternative to the speculum
- Needle holders
- 0.12 forceps (+/- Colibri forceps)
- Surgical tying forceps
- Tenotomy and fine scissors
- Surgical blade (1.0 to 1.2 mm)
- Ophthalmic viscoelastic
- Balanced salt solution
- 3 mL syringe
- 27 or 30 gauge cannula
- Eye spears
- Cyclodialysis spatula (used to displace the iris from the corneal wound)
- Fluorescein strip
- Cyanoacrylate glue
- Bandage contact lens
- Irradiated corneal tissue or pericardium allograft (needed if tissue is missing from trauma)
- Rigid eye shield
- Eye pads
- Postoperative antibiotics (intracameral, subconjunctival, or topical)
Table 3. Recommended Sutures for Parts of the Eye
| Suture Size | Part of the Eye |
| 10-0 | Cornea |
| 9-0 | Limbus |
| 8-0 | Sclera |
The standard suture for a corneal laceration repair is 10-0 nylon with a fine spatulated needle. If a surgical needle has a high radius of curvature, it will result in longer passes; a smaller radius of curvature will result in shorter passes.[3]
Expanded Instrumentation and Materials
The following equipment is used for each component of corneal repair procedures:
- Visualization and magnification
- Operating microscope with coaxial illumination (preferred over loupes for precision)
- Microscope-integrated OCT (MI-OCT), recent advancement for real-time wound assessment
- Adjustable zoom and red reflex enhancement for depth perception [39]
- Basic surgical setup
- Sterile draping with adhesive isolation sheets
- 5%–10% povidone-iodine for periocular prep (including conjunctival sac irrigation)
- Lash isolation (important in contaminated injuries)
- Core microsurgical instruments
- Needle holders (Castroviejo preferred for fine control)
- 0.12 forceps / Colibri forceps (toothed vs nontoothed depending on tissue)
- Tying forceps (McPherson or Hoskins)
- Vannas or Westcott scissors (more precise than standard tenotomy in microsurgery)
- Crescent blade (useful for lamellar dissection if needed)
- Sutures and needles (see Table 4)
- Spatulated needles minimize tissue trauma and allow lamellar passage
- Shorter curvature needles (3/8 circle) provide better control in small wounds
- Needle geometry directly affects bite depth and astigmatism induction
- Anterior chamber and wound management
- Ophthalmic viscoelastic device (cohesive preferred for chamber maintenance)
- Balanced salt solution (BSS) or BSS Plus
- 1–3 mL syringe with 27 or 30 gauge cannula
- Anterior chamber maintainer (advanced setup) [40]
- Tissue handling and reconstruction
- Cyclodialysis spatula (for iris repositioning)
- Iris repositor/Kuglen hook (alternative tool)
- Fine nontoothed forceps for endothelial protection
- Vitreous cutter (if anterior vitrectomy required) (modern addition) [41]
- Adjunctive materials
- Fluorescein strip (for Seidel test intraoperatively)
- Cyanoacrylate glue (for micro-leaks or adjunct closure)
- Fibrin glue (less inflammatory alternative)
- Bandage contact lens (protective and stabilizing role) [11]
- Graft and patch materials
- Irradiated corneal tissue (tectonic graft)
- Amniotic membrane (modern addition for epithelial healing)
- Pericardium or scleral patch graft (for structural support) [42]
- Infection control and medications
- Intracameral antibiotics (eg, cefuroxime, moxifloxacin)
- Subconjunctival antibiotics and steroids
- Antifungal agents in high-risk trauma (recent emphasis)
- Tetanus prophylaxis [43]
- Protective and postoperative materials
- Rigid eye shield (mandatory postop)
- Eye pads and sterile dressing
- Protective goggles (long-term advice) [44]
Table 4. Recommended Sutures for Corneal Repair
|
Suture Size |
Anatomical Use |
Preferred Needle Type |
Clinical Note |
|
10-0 Nylon |
Cornea |
Spatulated (microsurgical) |
Standard for corneal closure |
|
9-0 Nylon |
Limbus |
Spatulated |
Better tensile strength |
|
8-0 Nylon |
Sclera |
Reverse cutting |
For thicker tissues |
|
11-0 Nylon (optional) |
Pediatric/very fine wounds |
Spatulated |
Reduces scarring |
Additional Advanced Practical Points
Careful evaluation of wound architecture remains essential during corneal laceration repair. Surgeons should assess whether the laceration demonstrates a linear, stellate, or ragged configuration, as well as whether the injury involves the central or peripheral cornea. These characteristics directly influence the required number of sutures, stromal bite depth, and suture spacing (see Table 5).[45]
Refinements in suture technique focus on achieving approximately 90% stromal depth with equal bite sizes on both sides of the wound. Suturing commonly begins centrally and progresses toward the periphery to improve wound alignment and structural symmetry. Excessive suture tension should be avoided because over-tightening may induce postoperative astigmatism, whereas loose sutures increase the risk of wound leakage.[46]
Modern approaches to astigmatism control incorporate selective suture tightening, intraoperative keratoscopy, and symmetric suture placement to reduce postoperative irregular astigmatism and improve refractive outcomes.[47] Maintenance of anterior chamber stability remains critical throughout surgical repair. Ophthalmic viscosurgical devices (OVDs) or balanced salt solution (BSS) help preserve chamber depth, prevent iris or lens prolapse, and reduce repeated chamber collapse, which may contribute to endothelial damage.[48] Principles of tissue preservation emphasize minimal manipulation, avoidance of endothelial contact, selective excision of only nonviable tissue, and preservation of limbal structures whenever feasible.[49]
Special intraoperative situations require individualized management strategies. Surgeons should reposition viable prolapsed iris tissue while excising necrotic tissue when necessary. Lens involvement may warrant delayed intervention unless inflammation develops, whereas vitreous prolapse generally requires anterior vitrectomy.[50] Emerging surgical innovations include microscope-integrated optical coherence tomography-guided suturing to improve intraoperative precision, femtosecond-assisted wound preparation, and the development of biologic scaffolds and regenerative materials for enhanced tissue repair and visual rehabilitation.[51]
Table 5. Summary of Essential Versus Advanced Additions
|
Category |
Essential |
Advanced/Optional |
|
Visualization |
Microscope |
MI-OCT |
|
Sutures |
10-0 nylon |
11-0 nylon |
|
Instruments |
Forceps, needle holder |
Vitrectomy cutter |
|
Closure |
Sutures |
Tissue glue |
|
Support |
BSS, ophthalmic viscoelastic device |
AC maintainer |
|
Grafts |
Corneal patch |
Amniotic membrane |
Key Takeaway
Modern corneal laceration repair is no longer just about closing a wound; current techniques focus on restoring anatomy, preserving optics, and minimizing long-term refractive distortion. The addition of advanced instruments, refined suture techniques, and adjunctive biomaterials has significantly improved surgical precision and patient outcomes.
Personnel
Interprofessional team members that may be involved with corneal laceration cases include:
- Ophthalmologist (surgeon): Performs the corneal repair and ensures anatomical and visual restoration.[52]
- Surgical technician: Prepares instruments and maintains the sterile field during surgery.[11]
- Operating room nurse: Assists with patient care and monitoring and ensures that surgical safety protocols are followed.[53]
- Anesthesiologist/CRNA: Manages anesthesia and maintains patient stability throughout the procedure.[54]
- Ophthalmic assistant/technician: Assists in preoperative evaluation, visual acuity assessment, and postoperative follow-up testing. They also support imaging and documentation.[55]
- Emergency physician: Often the first to evaluate the patient, initiate stabilization, and coordinate urgent ophthalmology referral.[56]
- Pharmacist: Ensures appropriate antibiotic selection, dosing, and drug safety, particularly in complex trauma cases requiring systemic therapy.[57]
- Optometrist/contact lens specialist: Plays a major role in postoperative visual rehabilitation, especially in fitting rigid gas permeable or scleral lenses for irregular corneas.[58]
- Vitreoretinal surgeon (if required): In cases with posterior segment involvement, they manage retinal complications, eg, vitreous hemorrhage or retinal detachment.[59]
Successful management of corneal laceration depends not solely on surgical skill but on a well-coordinated interprofessional team, in which each member contributes to patient stabilization, precise surgical execution, and optimal postoperative recovery.[60]
Preparation
While awaiting corneal laceration repair, clinicians should immediately protect the injured eye with a rigid eye shield and maintain continuous shielding until surgery.[61] Manipulation of the eye, patching, and application of pressure dressings should be avoided because patches may exert harmful pressure on the globe. Patients should receive strict instructions to avoid eye rubbing, eyelid squeezing, coughing, straining, or other Valsalva maneuvers that may increase intraocular pressure and precipitate extrusion of intraocular contents.[62] Elevation of the head to approximately 30° may help reduce intraocular pressure and decrease the risk of prolapse. Pain and nausea require prompt control with analgesics and antiemetics, while mild anxiolysis may benefit selected patients.[63] Intravenous opioids, including fentanyl, commonly serve as preferred analgesics, whereas ondansetron or metoclopramide may reduce nausea and vomiting that could otherwise produce sudden increases in intraocular pressure.[63]
Modern trauma management follows Advanced Trauma Life Support (ATLS) principles, prioritizing airway, breathing, and circulation before definitive ocular intervention.[64] Clinicians should evaluate associated injuries, including head trauma, orbital fractures, and facial lacerations, while ensuring hemodynamic stability and adequate oxygenation.[64] Patients should remain nil per os in preparation for surgery because general anesthesia remains preferred in most corneal laceration repairs.[65] Preanesthetic evaluation should include assessment of cardiac status, airway anatomy, and medication allergies (see Table 6).[65]
CT of the face and orbits before repair frequently identifies intraocular or orbital foreign bodies and commonly represents the standard of care for ocular trauma at multiple institutions.[66][67] Indications for CT include suspected intraocular foreign body (IOFB), high-velocity trauma involving metal, glass, or blast injuries, and poor visualization caused by edema or hyphema.[68] Best practices favor noncontrast orbital CT with thin slices measuring approximately 1 to 2 mm.[68] MRI should be avoided when a metallic foreign body is suspected. Additional advanced imaging modalities may include AS-OCT for assessment of wound depth in stable, cooperative patients and B-scan ultrasonography only after exclusion of globe rupture.[69]
Early infection prevention remains critical in ocular trauma management. Broad-spectrum intravenous antibiotics should be initiated promptly, with common regimens including vancomycin plus ceftazidime.[70] Agricultural injuries may warrant antifungal coverage due to an increased risk of fungal contamination.[70] Clinicians should administer tetanus prophylaxis according to the patient’s immunization status.[66][67][70]
Clinicians should perform a cautious but essential ocular examination to avoid worsening the injury or causing additional distress to the patient.[71] Although examination may prove difficult, the evaluation should include visual acuity testing with a Snellen chart or near-vision card, pupillary reflex assessment with attention to a relative afferent pupillary defect, and gross anterior segment evaluation using a penlight or slit lamp.[71][72] Additional clinical findings requiring assessment include a shallow anterior chamber, hyphema, lens displacement, and a circumferential subconjunctival hemorrhage, as a 360-degree subconjunctival hemorrhage may suggest globe rupture.[72] Tonometry should not be performed when a full-thickness laceration or open globe injury remains present or suspected.[73] Gonioscopy and excessive eyelid manipulation should also be avoided.[72]
When the depth of the laceration is uncertain, clinicians should gently perform a Seidel test under slit-lamp visualization with fluorescein to identify aqueous leakage.[73] Excessive manipulation should be avoided in obvious open-globe injuries because additional pressure may worsen tissue extrusion.
Before corneal laceration repair, clinicians should instill 5% povidone-iodine ophthalmic solution into the conjunctival sac because this solution remains highly effective in reducing bacterial contamination.[74] Preparation of the periocular skin should include cleansing with 10% povidone-iodine and maintenance of a contact time of at least 2 to 3 minutes to maximize bactericidal activity.[75] Repeated irrigation should be avoided because excessive fluid manipulation may worsen wound leakage.[75] Throughout examination and surgical preparation, clinicians should avoid all digital pressure and eyelid squeezing to prevent protrusion of intraocular contents. When eyelid retraction becomes necessary, careful use of a speculum, preferably a Jaffe or Schott design, or placement of eyelid sutures may reduce pressure-related complications.
Temporary stabilization measures should continue throughout the preoperative period and may include maintenance of the rigid eye shield, continuation of intravenous antibiotics, use of cyanoacrylate glue for microleaks, and placement of a bandage contact lens in selected cases.[76]
Comprehensive counseling and informed consent remain essential before surgery. Clinicians should explain the nature of the injury, the risk of permanent vision loss, the urgency of surgical intervention, and the possibility that multiple procedures may become necessary.[77] Documentation should include baseline visual acuity findings and a discussion of the anticipated prognosis.[77]
Table 6. Preoperative Checklist
|
Step |
Action |
Purpose |
|
Protection |
Eye shield |
Prevent extrusion |
|
Stabilization |
ATLS protocol |
Life-saving priority |
|
Pain control |
Analgesics and antiemetics |
Prevent IOP spikes |
|
Imaging |
CT orbit |
Detect IOFB |
|
Infection control |
IV antibiotics and tetanus |
Prevent endophthalmitis |
|
Examination |
Minimal essential exam |
Baseline assessment |
|
Surface prep |
Povidone-iodine |
Reduce microbial load |
|
Fasting |
NPO |
Anesthesia readiness |
Recent Practical Updates
Recent practical updates in corneal laceration management emphasize earlier intervention, structured stabilization, and integration of advanced diagnostic strategies. Administration of systemic antibiotics within 1 hour of injury has demonstrated improved clinical outcomes by reducing the risk of infection and limiting progression to severe ocular complications. Intraoperative use of intracameral antibiotics has also become increasingly common as part of comprehensive antimicrobial prophylaxis.
The damage-control approach continues to gain importance in modern ocular trauma care, prioritizing rapid stabilization of the patient and globe before definitive surgical repair. This staged strategy supports safer operative planning and improved preservation of ocular structures in complex trauma settings. Contemporary practice also incorporates expanded use of point-of-care imaging modalities to facilitate rapid assessment of wound characteristics and associated injuries. In parallel, standardized trauma protocols increasingly guide clinical management, promoting consistent evaluation, timely intervention, and improved coordination among interprofessional trauma teams.[60]
Key Clinical Pearls
Factors that should be kept in mind with corneal laceration repair include:
- “Do no harm before surgery”, avoid unnecessary manipulation
- Never measure IOP in suspected open globe
- CT scan is standard in high-risk trauma
- Vomiting = emergency risk → always control nausea
- Time to repair matters, but stability matters more
Preoperative preparation in corneal laceration is not merely a routine step but a critical determinant of surgical success and visual prognosis. A structured approach integrating systemic stabilization, infection control, careful examination, and meticulous ocular protection ensures that the patient reaches the operating table in the safest possible condition, thereby optimizing both anatomical and functional outcomes.[78]
Technique or Treatment
Corneal lacerations present uniquely in each patient, resulting in a wide range of repair strategies. Each injury requires individualized assessment and surgical problem-solving, challenging the surgeon to restore structural integrity while minimizing long-term visual impairment. Some surgeons view this complexity as intellectually rewarding, whereas others regard such repairs as technically demanding. Regardless of surgical perspective or technique, the primary objective remains the creation of a watertight corneal closure without incarceration of intraocular contents, thereby restoring globe integrity and preventing additional damage to the cornea and surrounding ocular structures.[5] Adherence to fundamental corneal suturing principles reduces the risk of excessive postoperative corneal scarring and high residual astigmatism.
Anesthesia Management
Anesthesia management for corneal laceration repair ranges from topical anesthesia to general anesthesia, depending on the severity and complexity of the injury.[79] Small lacerations managed in the clinic may respond adequately to topical anesthesia or a peribulbar block. Complex lacerations or injuries accompanied by tissue prolapse generally require general anesthesia to facilitate controlled surgical repair while reducing patient pain and anxiety. Full-thickness corneal lacerations particularly benefit from smooth anesthetic induction because coughing, straining, or sudden movement may precipitate prolapse of intraocular contents.[80]
Laceration Specific Management
Suspected corneal laceration
When clinicians cannot definitively confirm a corneal laceration in the emergency department or clinic setting, transport to the operating room for examination under anesthesia and possible globe exploration becomes appropriate.
Partial-thickness corneal laceration
Careful management of partial-thickness corneal lacerations includes gentle debridement followed by Seidel testing to confirm preservation of partial-thickness integrity. A positive Seidel test indicates conversion to or presence of a full-thickness laceration, requiring management according to open-globe repair principles. Negative Seidel testing supports conservative treatment with a bandage contact lens or fibrin glue, similar to management strategies used for corneal abrasions.
Wound cultures should be obtained carefully to avoid pressure on the globe or prolapse of intraocular tissue. Culture results may later guide treatment if infection develops. Only the operating surgeon should perform tissue debridement because improper manipulation may worsen ocular damage. Necrotic tissue requires excision, while viable tissue should be repositioned into the eye. Surgeons should also remove all visible debris and foreign bodies during wound preparation.
Full-thickness corneal laceration less than 2 mm
Management of full-thickness corneal lacerations measuring less than 2 mm may involve cyanoacrylate glue, fibrin glue, amniotic membrane placement, or bandage contact lenses.[81][82][83] Failure to achieve a watertight seal with these modalities necessitates suturing. Cooperative patients may undergo these procedures in the clinic setting. Despite the small size of certain lacerations, many surgeons still prefer primary suturing because bedside evaluation may underestimate wound extent, whereas operative assessment allows more accurate characterization of the injury.
Full-thickness corneal laceration greater than 2 mm
Full-thickness corneal lacerations greater than 2 mm generally require sutured repair in the operating room. Before placing sutures, surgeons should carefully evaluate the wound and formulate a structured repair plan. Sketching the anticipated repair may help organize the surgical approach. During suturing, the needle should enter the cornea perpendicular to the tissue surface. One technique involves holding 1 side of the corneal wound at a 45-degree angle and entering the tissue at the same angle, then rotating the wrist along the natural curvature of the needle until exiting perpendicular to the tissue on the opposite side. Surgeons may secure sutures using a slip knot, 2-1-1 knot, or 3-1-1 knot configuration before trimming the ends. Smaller knots facilitate easier burial within the corneal stroma.
Optimal stromal suture placement occurs at approximately 90% depth because shallow sutures may produce posterior wound gape. Full-thickness suture passes should be avoided because they may create a conduit for microbial entry into the eye. Placement of subsequent sutures should account for triangular compression zones extending from each suture to ensure complete wound closure without gaps.[84]
Longer sutures generate larger zones of compression than shorter sutures. Peripheral placement of long sutures may steepen the central cornea and improve wound sealing. Central sutures lie within the visual axis; therefore, surgeons should favor shorter central sutures with minimal tension to reduce postoperative astigmatism and minimize excessive corneal scarring.
Managing Tissue Prolapse
The iris and vitreous commonly prolapse through a corneal laceration in response to the existing pressure gradient and may continue to extrude until adequate wound closure occurs. Successful repair requires meticulous avoidance of incorporating prolapsed intraocular tissue into the wound closure, as tissue incarceration may worsen inflammation, compromise healing, and increase the risk of postoperative complications.
Several techniques may assist in managing prolapsed tissue during repair. One commonly used strategy involves creating a paracentesis away from the primary wound with a surgical blade, followed by injection of a viscoelastic agent to help maintain anterior chamber stability. A cyclodialysis spatula may then reposition the iris into the eye using a gentle sweeping motion. Repeated repositioning of intraocular tissue may become necessary throughout the suturing process because accidental globe pressure during suture passage or excessive wound manipulation with surgical instruments frequently promotes further tissue prolapse.
Special attention should be given to preventing further extrusion of intraocular contents at every stage of repair. In phakic patients, preservation of the crystalline lens remains particularly important, and surgeons should carefully avoid capsular violation during tissue manipulation and wound closure. The following are general guidelines for various types of corneal lacerations (see Image. Corneal Laceration Suture Techniques):
- Oblique laceration: The suture will be an equal distance at the posterior part of the wound, but anteriorly will look displaced to 1 side. Avoid tension over the shallow side of the wound when tying the suture.
- Linear laceration: Start suture placement in the center of the laceration and then bisect the halves until sealed.
- Gaping laceration: Place the initial sutures at the ends of the wound, then zip it up, keeping tissue out of the closure.
- Angled laceration: The initial suture can be placed at the apex, then suture the sides as separate linear lacerations.
- Stellate laceration: These closures can be challenging. A purse-string suture is placed centrally, either at the beginning or end of the closure, to help seal it. Interrupted sutures close the remaining aspects of the laceration.[85]
- Corneoscleral laceration: Place the initial suture at the limbus. This alignment is critical to repairing the cornea and scleral aspects. The limbus is usually the most identifiable tissue during the repair because of the contrast between the cornea and sclera. After closing the limbus, focus on the corneal aspect first and then the sclera to avoid tissue prolapse (see Image. Corneoscleral Laceration).
Corneal tissue loss
Corneal tissue loss poses a significant challenge to repair because successful closure requires restoring globe integrity despite the absence of native tissue. In such cases, a patch graft may provide a watertight closure and help preserve the structural stability of the eye. Multiple patch graft techniques are available and may incorporate amniotic membrane, allograft tissue, or gamma-irradiated corneal tissue, depending on the size, location, and characteristics of the defect.[86][87][88]
Final steps following repair
After completion of the corneal laceration repair, the surgeon should carefully assess the wound for leakage using surgical spears or a fluorescein strip. Detection of a persistent leak warrants additional intervention to achieve complete wound closure. Further suturing may be necessary, or adjunctive measures, eg, cyanoacrylate glue, fibrin glue, amniotic membrane, or a bandage contact lens may be applied to reinforce the repair and establish a watertight seal.
All suture knots should remain securely buried, preferably away from the visual axis, to reduce patient discomfort, minimize epithelial disruption, and limit visual disturbance. Careful knot placement also helps reduce the risk of postoperative complications associated with exposed sutures. Postoperative infection prevention requires comprehensive antimicrobial coverage. A combination of intracameral, subconjunctival, topical, intravenous, and oral antibiotics may reduce the risk of postoperative infection and support favorable healing outcomes.
Following completion of the procedure, the eye should be covered with surgical eye pads and protected with a rigid eye shield to safeguard the repair and minimize the risk of inadvertent trauma during the immediate postoperative period.
Advanced Corneal Laceration Repair Techniques
Modern corneal laceration repair extends beyond basic suturing techniques to include detailed optimization of wound architecture, refined intraoperative decision-making, and strategies to preserve refractive outcomes.[89] Contemporary surgical approaches emphasize not only restoration of globe integrity but also minimization of postoperative scarring, astigmatism, and visual distortion.
Presuturing strategic planning
Before placing the initial suture, experienced surgeons mentally reconstruct the corneal curvature and visualize the anticipated final corneal contour, rather than focusing solely on wound closure. Careful assessment should identify the highest points of corneal distortion as well as areas of tissue mismatch or override. In complex injuries, marking the wound edges with a gentian violet marker may assist with surgical planning and orientation. Thorough preoperative planning remains critical because inadequate planning may result in irregular astigmatism despite technically successful wound closure.[90]
Depth control and lamellar alignment refinement
Optimal suture bites generally engage approximately 85% to 95% of stromal depth. In wounds with uneven architecture, deeper bites on the shorter or steeper side and shallower bites on the longer or more sloping side may improve tissue alignment. This approach promotes accurate posterior surface apposition, which carries greater optical significance than alignment of the anterior corneal surface.[40]
Posterior wound apposition
Accurate anterior wound alignment does not necessarily guarantee proper posterior wound closure. Posterior wound gape may persist despite a satisfactory anterior appearance and can contribute to persistent wound leakage and irregular healing. Surgeons may initially apply slight over-tightening of sutures and subsequently adjust tension as needed. Intraoperative reformation of the anterior chamber can assist in assessing internal wound sealing and confirming adequate posterior apposition.[91]
Suture tension modulation strategy
Uniform suture tightening may not provide optimal outcomes. Central sutures generally require minimal tension to reduce postoperative scarring, whereas peripheral sutures may benefit from slightly greater tension to improve wound sealing. Surgeons should adjust tension according to corneal curvature and wound geometry. Sequential tightening of sutures rather than immediate final tightening of each suture may enhance wound symmetry and improve overall tissue alignment.[92]
Intraoperative astigmatism control
Modern corneal repair incorporates refractive principles throughout the procedure. Long, tightly secured central sutures should generally be avoided because they may induce significant postoperative astigmatism. Short, evenly spaced sutures positioned centrally help maintain corneal contour and reduce refractive distortion. Symmetrical spacing and mirror-image suture placement further support favorable optical outcomes. Intraoperative assessment with a handheld keratoscope or surgical microscope may assist in identifying and correcting corneal irregularities during repair.[93]
Anterior chamber dynamics management
Maintenance of anterior chamber stability requires continuous adjustment throughout surgery. Surgeons commonly alternate between ophthalmic viscosurgical device injection and balanced salt solution hydration to preserve chamber depth and support tissue positioning. Overfilling the chamber may promote iris prolapse, whereas underfilling may contribute to wound collapse. Small intermittent injections generally provide greater control than continuous filling techniques.[94]
Endothelial protection techniques
Protection of the corneal endothelium remains a critical aspect of advanced repair. Instrument contact with the endothelium and repeated collapse of the anterior chamber should be avoided whenever possible. Application of a dispersive viscoelastic coating may provide additional endothelial protection during complex procedures. Endothelial injury may result in chronic corneal edema and could ultimately necessitate keratoplasty.[95]
Micro-leak detection
Assessment for subtle wound leakage extends beyond conventional Seidel testing. Surgeons should monitor for signs, eg, slight shallowing of the anterior chamber and the presence of microbubbles at the wound site. Gentle drying of the corneal surface with a surgical sponge may reveal a thin fluid film indicative of leakage. Some wound leaks remain pressure-dependent and may become apparent only after normalization of intraocular pressure.[96]
Knot management optimization
Proper knot management contributes significantly to wound healing and patient comfort. Suture knots should remain small and be rotated into the corneal stroma whenever possible. Surface-exposed knots may cause epithelial defects and increase postoperative discomfort. Optimal placement positions knots away from both the visual axis and the wound edge.[97]
Multi-planar and complex wounds
Irregular, stellate, or multi-planar lacerations require a tailored approach. Linear closure techniques may not adequately address these complex wound patterns and should not be attempted. Instead, surgeons should divide the injury into multiple geometric segments and manage each segment independently while maintaining overall symmetry throughout the repair.[98]
Adjunctive therapies
Adjunctive therapies may enhance wound healing and closure when used appropriately. Sutures combined with tissue adhesive may improve sealing of micro-leaks, whereas sutures combined with amniotic membrane transplantation may provide additional epithelial support. In most cases, these adjuncts serve as supportive measures rather than primary closure techniques.
Intraoperative staged surgery
Completing all surgical objectives in a single procedure may not always be the optimal approach. Surgeons should consider staged management when severe inflammation, extensive tissue damage, or associated posterior segment injury complicates the repair.[99] A staged strategy may improve visualization, reduce surgical trauma, and facilitate more effective reconstruction during subsequent procedures.
Iatrogenic complication prevention
Careful surgical technique remains essential for preventing avoidable complications. Excessive pressure on the globe may cause extrusion of intraocular contents, excessively deep needle passes may produce endothelial trauma, and full-thickness suture passes may create a conduit for infection. Prevention of these complications requires gentle tissue handling, controlled needle entry, and meticulous attention throughout the procedure.[100]
Peripheral versus central strategy shift
The surgical approach to corneal laceration repair differs between the central and peripheral cornea because each region presents distinct anatomical and functional priorities (see Table 7).
Table 7. Central and Peripheral Corneal Approaches
|
Parameter |
Central Cornea |
Peripheral Cornea |
|
Goal |
Optical clarity |
Structural integrity |
|
Suture tension |
Minimal |
Slightly higher |
|
Suture length |
Short |
Longer |
|
Priority |
Reduce astigmatism |
Prevent leakage |
Final Integrity Assessment
Following wound closure, a comprehensive assessment of repair integrity remains essential. The surgeon should evaluate anterior chamber depth and carefully inspect wound alignment under magnification to confirm accurate tissue apposition and adequate globe restoration. Immediate inspection alone may fail to detect subtle defects; therefore, reassessment after several minutes provides an opportunity to detect delayed wound leaks that may not become apparent until intraocular dynamics stabilize. This final evaluation helps confirm a secure, watertight closure and reduces the risk of postoperative complications.
Recent advances have expanded the surgical options available for corneal laceration repair (see Table 8). MI-OCT provides real-time guidance regarding suture depth and wound apposition, allowing greater precision during reconstruction. Femtosecond-assisted repair, although still experimental, offers highly precise modulation of wound edges and may enhance surgical accuracy in selected cases. Biologic sealants have also emerged as adjunctive treatment options and may reduce inflammation when compared with cyanoacrylate-based materials.[9]
Several surgeon-level optimization principles can further improve outcomes. Initial suture tension should generally remain conservative, allowing subsequent adjustments as wound architecture and corneal contour evolve during the repair. Surgeons should approach corneal trauma with a "refractive-surgery mindset in trauma", recognizing that restoration of optical quality is as important as structural closure. Particular attention should focus on the placement of the first 3 sutures, as these initial sutures frequently establish wound alignment, corneal contour, and the overall trajectory of the final surgical result.
Table 8. Summary of Advanced Principles
|
Core Principle |
Clinical Impact |
|
Posterior alignment > anterior alignment |
Prevents leaks |
|
Symmetry in sutures |
Reduces astigmatism |
|
Minimal tissue handling |
Preserves clarity |
|
Controlled chamber dynamics |
Prevents prolapse |
|
Strategic planning |
Improves visual outcome |
Final Takeaway
Corneal laceration repair is no longer a purely reconstructive procedure, but rather a precision refractive and structural surgery performed under emergency conditions. Mastery lies in understanding not just how to close a wound, but how to restore corneal biomechanics, optical integrity, and long-term visual function simultaneously.
Complications
Complications are avoidable with preoperative and postoperative antibiotics and proper intraoperative surgical technique.[101]
Posttraumatic Endophthalmitis
Posttraumatic endophthalmitis is a devastating condition that occurs from 3.3% to 17% in penetrating trauma. The primary risk factors are a delay of primary surgical repair and violation of the lens capsule. The diagnosis can be difficult because the eye is already inflamed from the trauma and surgery.[102] Symptoms can be nonspecific, including ocular pain, redness, eyelid swelling, discharge, decreased vision, and floaters. Treatment recommendations vary from a vitreous tap and injection with broad-spectrum antibiotics to a vitrectomy if vision is light perception or worse.[103]
Retained Intraocular Foreign Body
Intraocular foreign bodies in ocular trauma occur in 18% to 41% of cases.[104] Ocular imaging prior to the surgical repair can identify foreign bodies. Sometimes foreign bodies cannot be removed during a surgical repair, especially if located in the vitreous, so further surgery may be necessary. Most foreign bodies are metallic and toxic to the eye; therefore, removal is recommended.[104]
Wound Leak
Evaluate the patient the day after the primary surgical repair with fluorescein to check for a wound leak. If a wound leak is present, a bandage, contact lens, or cyanoacrylate glue may seal it. If the leak is too brisk or too large, additional suturing is required to achieve a watertight closure. Wound leaks significantly increase the risk of infection.[105]
Suture Issues
Unburied knots and broken or loose sutures can cause patient discomfort and provide a pathway for microorganisms. All suture knots should be buried at the time of surgery; however, if a knot is recognized during the postoperative period, it can be rotated at the slit lamp. The timing of suture removal varies depending on the patient's age, the size of the laceration, and the refractive anomaly induced by the suture.[106] However, remove broken or loose sutures immediately.
Iris Damage
The iris can tear or be dislodged from its root during initial trauma or surgical repair. An abnormal iris can cause photophobia, visual disturbances, and an unpleasant aesthetic appearance.[107][108] Surgical techniques, corneal tattooing, contact lenses, and artificial iris implants are available for symptomatic patients.[109][110]
Cataract
Cataracts can form from the initial trauma or during the operative repair if the lens capsule is violated. The majority of traumatic cataracts can be safely removed and replaced with a posterior or scleral-fixed lens to improve vision.[111]
Infectious Keratitis
Infectious keratitis can occur following trauma and is caused by various organisms.[112] Bacteria can accumulate along the sutures or form abscesses.[113] Treatment typically starts with fluoroquinolones, although fortified broad-spectrum antibiotics may be necessary for severe infections or infections caused by resistant bacteria.
Retinal Detachment
Retinal detachments can occur during the trauma or subsequently in the postoperative period. Early intervention is key to preventing vision loss.
Posttraumatic Glaucoma
Secondary glaucoma occurring after penetrating trauma is not uncommon due to various mechanisms.[114] Monitor intraocular pressure during the postoperative period and counsel the patient about long-term risks.
Sympathetic Ophthalmia
Sympathetic ophthalmia is an uncommon immune reaction that occurs in the nontraumatic eye after injuries or surgeries involving the uveal tissue.[115] Suspect this condition if inflammation occurs in the nontraumatic eye. The classic doctrine taught was to enucleate the traumatic eye within 2 weeks to prevent this condition; however, the current doctrine encourages leaving the traumatic eye in place if any vision remains.[49]
Vision Loss
Vision loss can occur from all of the complications discussed in this section. Traumatic damage to the optic nerve or other parts of the eye can also lead to vision loss. Corneal scarring, neovascularization, and irregular astigmatism are common reasons for decreased vision after a corneal laceration. Hard contact lenses can help determine whether the visual complaint is related to the cornea or other parts of the eye. A special-fit contact lens can often significantly improve vision.[116] If the vision loss is due to corneal pathology and does not improve with contact lenses, a corneal transplant may be beneficial once the eye has fully healed from the trauma.[117]
Corneal Scarring with Irregular Astigmatism
Even with optimal wound closure, stromal healing often leads to fibrosis and irregular astigmatism due to altered collagen alignment. This can significantly degrade visual quality, especially in central corneal injuries. Management ranges from rigid gas-permeable or scleral lenses to topography-guided procedures to delayed keratoplasty in severe cases.[118]
Corneal Neovascularization
Chronic inflammation, hypoxia, or prolonged contact lens use may induce corneal vascular ingrowth, compromising transparency and increasing the risk of graft rejection in future surgeries. Early control with topical steroids and, in selected cases, anti-VEGF therapy can help limit progression.[29]
Persistent Epithelial Defect
Failure of epithelial healing may result from poor ocular surface, neurotrophic status, or ongoing inflammation. This predisposes the cornea to secondary infection and stromal melt. Management includes aggressive lubrication, bandage contact lenses, and amniotic membrane transplantation when required.[119]
Corneal Melt and Keratolysis
Excessive inflammatory response or infection can lead to stromal degradation and progressive thinning, sometimes culminating in perforation. Prompt identification is crucial, and treatment involves addressing the underlying cause, using anticollagenase therapy, and surgical reinforcement if necessary.[30]
Epithelial or Fibrous Ingrowth
Ingress of epithelial or fibrous tissue at the wound interface may occur with imperfect closure, leading to chronic inflammation and interface opacity. Surgical debridement is often required to restore clarity and prevent progression.[120]
Anterior Chamber Instability/Hypotony
Persistent wound leaks or ciliary body dysfunction may result in hypotony, leading to complications, eg, choroidal detachment or maculopathy. Management focuses on restoring wound integrity and maintaining adequate intraocular pressure.[121]
Peripheral Anterior Synechiae
Inadequate anterior chamber depth or prolonged inflammation can lead to adhesions between the iris and angle structures, predisposing to secondary glaucoma. Early anatomical restoration and control of inflammation are key preventive strategies.[15]
Pupillary Abnormalities
Trauma or surgical manipulation may result in irregular pupil shape, size, or reactivity, leading to glare, halos, and cosmetic concerns. Management options include pharmacological modulation, tinted lenses, or surgical pupilloplasty in symptomatic cases.[33]
Lens Subluxation/Zonular Dialysis
Zonular weakness or disruption may be initially overlooked and can later manifest as lens instability or visual fluctuations. Careful follow-up is essential, with surgical intervention considered when visual function is significantly affected.[17]
Choroidal Detachment/Suprachoroidal Hemorrhage
Hypotony or intraoperative trauma can lead to the accumulation of fluid or blood in the suprachoroidal space, presenting with pain and a shallow anterior chamber. Management includes cycloplegia and, in severe cases, surgical drainage.[20]
Traumatic Uveitis
Inflammatory response following trauma may persist beyond the acute phase, leading to synechiae formation and secondary complications. Timely use of corticosteroids and cycloplegics helps control inflammation and prevent sequelae.[34]
Secondary Infection Beyond Cornea
Infections may extend beyond the cornea to involve the sclera or orbit, particularly in contaminated injuries. Such cases require aggressive systemic antibiotic therapy and close monitoring due to their potentially severe course.[101]
Vitreoretinal Complications (Delayed)
Posterior segment complications, eg, proliferative vitreoretinopathy, macular edema, or epiretinal membrane formation, may develop later and contribute to poor visual outcomes. Early retinal evaluation and intervention are critical.[122]
Ocular Surface Dysfunction
Trauma and surgical intervention can disrupt tear film stability and meibomian gland function, resulting in chronic dry eye symptoms. Long-term lubrication and ocular surface optimization are often necessary.[7]
Psychological and Functional Impact
Ocular trauma can have a significant psychological impact, including anxiety and reduced quality of life. Addressing patient concerns, counseling, and ensuring compliance are important components of holistic care.[9]
Missed Event Scenarios
Missed intraocular foreign bodies, subtle wound leaks, or unrecognized lens and retinal injuries can significantly worsen prognosis if not identified early. Regular postoperative reassessment, including imaging and careful slit-lamp evaluation, is essential for detecting these issues promptly and initiating appropriate management.[122]
Timeline-Based Understanding of Complications
Complications following corneal laceration repair evolve over time. Immediate issues include wound leaks and infection, early complications involve epithelial defects and inflammation, intermediate problems include cataract and glaucoma, while late sequelae often manifest as scarring, neovascularization, or retinal pathology. Understanding this timeline aids in structured follow-up and timely intervention.
Final Clinical Insight
The success of corneal laceration repair lies not only in surgical closure but in anticipating, preventing, and managing a wide spectrum of complications. A vigilant, longitudinal approach ensures optimal structural integrity and maximizes visual rehabilitation.[34]
Clinical Significance
Visual acuity loss is detrimental to the quality of life.[123] The United States Eye Registry highlights that at least a quarter of the patients with ocular trauma will have permanent vision loss.[124] Despite a perfect corneal laceration repair, vision loss may be present from corneal scarring, astigmatism, or damage to other parts of the eye.
Prevention through eye protection leads to better vision outcomes and fewer injuries.[125][126][127] The mandate for eye protection in the United States military led to fewer and less severe ocular injuries.[128] In a patient with vision loss, eye protection is strongly recommended to protect the better-seeing eye. After ocular trauma, educating patients on protective eyewear should be incorporated into practice patterns.[129]
Visual Outcomes and Rehabilitation
Visual impairment following corneal laceration extends beyond anatomical repair and reflects a complex interplay of optical distortion, neural adaptation, and associated ocular damage. Even when the cornea heals structurally, patients may experience reduced contrast sensitivity, glare, halos, and higher-order aberrations, which significantly affect real-world visual performance, eg, night driving and reading. Therefore, assessment of outcomes should not be limited to Snellen acuity alone but should include functional vision parameters and patient-reported quality-of-life measures.
Functional visual rehabilitation
Visual recovery often requires a staged rehabilitation approach. In addition to spectacles, rigid gas-permeable (RGP) lenses and scleral lenses play a crucial role in correcting irregular astigmatism by creating a new refractive surface. In selected stable cases, topography-guided refractive procedures or intrastromal corneal ring segments may be considered. When corneal opacity is the primary limiting factor, lamellar or penetrating keratoplasty remains the definitive option once the eye is quiet.[33]
Early visual rehabilitation remains especially critical in children to reduce the risk of amblyopia and in patients with unilateral injuries to preserve binocular vision. Clinicians should introduce temporary rehabilitative measures, including contact lenses or other optical aids, at an early stage rather than delaying intervention until complete healing occurs, as postponement of visual rehabilitation may contribute to permanent visual suppression.[38]
Neuroadaptation plays an important role in visual recovery following ocular trauma, as patients often require time to adjust to altered optical properties. Neural adaptation may partially compensate for irregular optics; however, persistent visual distortion continues in many cases despite successful anatomical repair. Clinicians should provide thorough counseling regarding realistic visual expectations because anatomical success may not correspond with complete functional visual recovery.[130]
Optimal rehabilitation commonly requires an interprofessional approach involving a cornea specialist, vitreoretinal surgeon, optometrist with expertise in contact lens fitting, and a low-vision rehabilitation specialist. Low-vision aids, including magnifiers, electronic visual devices, and contrast-enhancing tools, can substantially improve functional independence and quality of life in patients with irreversible visual impairment.[130]
Long-Term Management and Prevention Strategies
Visual outcomes following corneal trauma may continue to evolve over months or years, necessitating long-term monitoring for progressive astigmatism, secondary glaucoma, and delayed corneal decompensation. Selective suture removal, suture adjustment, and secondary refractive correction may significantly enhance visual outcomes even several months after the initial surgery.[131]
Prevention remains the most effective strategy for reducing the burden of ocular trauma. In addition to occupational and military safety measures, preventive efforts should emphasize household safety when handling sharp instruments or chemicals, sports-related eye protection with polycarbonate eyewear, and strict compliance with industrial safety regulations. Polycarbonate lenses remain strongly recommended because of their lightweight construction and high impact resistance.[132] Mandatory eye protection policies implemented in military and industrial settings have demonstrated substantial reductions in both the incidence and severity of ocular injuries. Expansion of similar policies to additional high-risk occupations and sports settings may further decrease preventable blindness worldwide.
Structured patient counseling forms a critical component of long-term management following ocular trauma. Clinicians should educate patients regarding the risk of future injury, the importance of protective eyewear, and the necessity of regular ophthalmic follow-up. Patients with monocular vision or markedly reduced vision in 1 eye require a strong recommendation for continuous use of protective eyewear because injury to the better-seeing eye can have devastating consequences.[132]
Visual loss following ocular trauma may contribute to reduced independence, occupational limitations, and significant psychological distress. Early referral for counseling and vision rehabilitation services may improve coping strategies, psychosocial adjustment, and overall quality of life. Emerging advances in visual rehabilitation include wavefront-guided correction for posttraumatic optical aberrations, customized scleral lenses for irregular corneal surfaces, and ongoing research involving corneal regeneration and bioengineered tissues. These innovations aim to narrow the gap between structural repair and restoration of functional vision.[42]
Clinical Prognosis
Visual outcomes after corneal laceration are determined not only by the success of surgical repair but also by timely rehabilitation, prevention of secondary complications, and patient education. A proactive, interprofessional, and prevention-focused approach is essential to maximize visual function and reduce the long-term impact of ocular trauma on quality of life. All team members educate the patient and family on postoperative care, including medication adherence, signs of complications, activity limitations, and expected symptoms throughout recovery. Setting realistic expectations is important because many cases result in poor outcomes.[133]
A corneal laceration will alter the patient's refractive error. The patient may need a special contact lens fitting by an optometrist or an updated prescription for their glasses to improve visual outcomes. Advances in contact lenses have improved patients' visual outcomes after ocular trauma. A study of 214 patients with open-globe injury demonstrated visual acuity improvement in 97% of patients who wore contact lenses.
Enhancing Healthcare Team Outcomes
Corneal laceration is a vision-threatening form of ocular trauma characterized by partial- or full-thickness disruption of corneal integrity, often resulting from high-velocity injury, blunt trauma, or penetrating foreign bodies. Clinical findings include ocular pain, decreased visual acuity, positive Seidel test, irregular pupil, prolapse of intraocular contents, and associated anterior or posterior segment injury. Prompt diagnosis and repair, typically within 24 hours, are essential to reduce the risks of infection, endophthalmitis, stromal necrosis, scarring, irregular astigmatism, glaucoma, retinal detachment, and permanent vision loss. Contemporary management integrates slit-lamp examination, anterior segment imaging, microsurgical repair, tissue adhesives, antimicrobial prophylaxis, and postoperative refractive rehabilitation to restore the integrity of the globe and optimize visual outcomes.
Interprofessional collaboration improves patient safety, reduces delays in care, and supports long-term visual rehabilitation. Emergency clinicians, paramedics, primary care clinicians, optometrists, and advanced practitioners play critical roles in early recognition, rigid eye shield placement, stabilization, and urgent ophthalmology referral. Ophthalmologists coordinate definitive surgical management, while radiologists identify open-globe injuries and retained foreign bodies on imaging studies.[134] Nurses monitor pain control, vital signs, medication adherence, and postoperative recovery while reinforcing patient and family education regarding warning signs, activity restrictions, and follow-up care. Pharmacists optimize antimicrobial, antiemetic, and analgesic therapy, including preparation of fortified antibiotics when indicated. Surgical technicians and anesthesia clinicians maintain operative safety and minimize intraoperative complications through coordinated perioperative care. Optometrists assist with postoperative refractive correction and specialty contact lens fitting to improve visual rehabilitation. Shared decision-making, use of prognostic tools such as the Ocular Trauma Score, timely communication among team members, and structured follow-up strategies support realistic expectations, complication prevention, and patient-centered outcomes.[135]
Nursing, Allied Health, and Interprofessional Team Interventions
The first person to recognize an eye injury should intervene by placing a rigid eye shield over the injured eye. Nurses are vital in keeping the patient calm before the repair. Control of pain and nausea before and after the repair is necessary. Antibiotics should be administered at the onset of the injury and continued throughout the recovery period. Any member of the care team should speak up if they notice anything unsafe or have any concerns.[7]
Effective management of corneal laceration is inherently team-based, extending well beyond the surgeon. Early recognition, coordinated stabilization, perioperative care, and long-term rehabilitation all depend on seamless collaboration between nursing staff, allied health professionals, and physicians. While the initial application of a rigid eye shield and patient calming are critical first steps, the broader interprofessional role is far more comprehensive and directly influences outcomes.
Emergency and Triage-Level Interventions
Frontline clinicians, including emergency nurses, paramedics, and triage staff, play a decisive role in early outcomes. Rapid identification of a suspected open globe injury, avoidance of any pressure on the eye, and immediate escalation to ophthalmology services are essential. Ensuring proper documentation of injury mechanism and time of onset also helps guide subsequent management and prognosis.[42]
Nursing Role in Preoperative Optimization
Nurses are central to maintaining physiological stability and patient comfort prior to surgery, including:
- Continuous monitoring of vital signs
- Administration of prescribed analgesics, antiemetics, and antibiotics
- Reinforcing strict eye protection and patient positioning
Equally important is psychological reassurance, as anxiety and agitation can increase intraocular pressure and risk of further injury.[43]
Intraoperative Support and Safety Protocols
Operating room nurses and technicians ensure the following:
- Availability and sterility of microsurgical instruments
- Proper patient positioning without exerting pressure on the globe
- Adherence to surgical safety checklists
They also serve as an additional safety layer by identifying breaks in sterile technique or equipment issues and promptly communicating concerns.[40]
Postoperative Nursing Care and Monitoring
Postoperative care requires vigilant observation for early complications. Nursing responsibilities include:
- Monitoring for pain, discharge, or sudden vision changes
- Administering topical and systemic medications as prescribed
- Ensuring the eye shield remains in place
Education on medication adherence and activity restrictions is a key component of nursing care.[20]
Role of Allied Health Professionals
Interprofessional care remains fundamental to successful corneal laceration management. From initial recognition and emergency stabilization through surgical treatment, rehabilitation, and long-term follow-up, each team member provides a unique contribution to patient safety, visual recovery, and quality of life. A coordinated, communicative, and patient-centered approach supports not only successful surgical repair but also meaningful functional restoration and long-term visual outcomes.
Optometrists
Optometrists contribute significantly to visual recovery by providing early refractive assessment and fitting specialty contact lenses, including rigid gas-permeable and scleral lenses, to support visual rehabilitation and optimize functional outcomes.
Pharmacists
Pharmacists play a critical role in optimizing antibiotic regimens, ensuring appropriate dosing, identifying potential drug interactions, and promoting patient adherence to prescribed therapies throughout the treatment and recovery process.
Ophthalmic technicians
Ophthalmic technicians assist with visual acuity testing and diagnostic imaging and provide valuable support during follow-up assessments, facilitating ongoing evaluation of visual function and postoperative recovery.
Low vision specialists
Low vision specialists introduce visual aids and adaptive strategies for patients with permanent vision loss, helping maximize independence and improve daily functioning.[136]
Rehabilitation and Long-Term Care Coordination
Recovery extends beyond wound healing. The interprofessional team supports structured follow-up schedules, promotes early detection of complications such as glaucoma or retinal pathology, and facilitates timely referral for secondary interventions, including keratoplasty or cataract surgery. This coordinated approach enhances both anatomical and functional outcomes.[43]
Communication and Safety Culture
A strong culture of open communication remains essential throughout corneal laceration management. Every member of the healthcare team should feel empowered to report unsafe practices, raise clinical concerns, and seek clarification regarding treatment plans. Such collaboration reduces medical errors and strengthens patient safety, particularly in high-acuity trauma settings.
Patient and Family Education
Patient education represents a shared responsibility among all team members. Key educational topics include the proper use of protective eyewear, adherence to prescribed medications, and recognition of warning signs that require urgent medical evaluation. Family involvement remains especially important for pediatric and elderly patients, helping promote compliance, reinforce treatment recommendations, and provide ongoing support.[34]
Psychosocial Support and Counseling
Ocular trauma can produce substantial emotional and psychological consequences. Nurses and allied health professionals should recognize signs of anxiety, distress, or adjustment difficulties, facilitate access to counseling and support services when appropriate, and encourage realistic expectations regarding recovery and visual outcomes.
Public Health and Preventive Role
Healthcare teams also contribute to injury prevention by promoting workplace and sports-related eye safety, educating communities about protective measures, and advocating for the implementation of safety policies in high-risk environments.[42]
Nursing, Allied Health, and Interprofessional Team Monitoring
Monitoring a patient's pain, nausea, and other vitals should occur before and after the repair. After the repair, the patient is either discharged home with a follow-up visit at the clinic the next day or kept overnight in the hospital for observation. During the postoperative period, especially the first week, all team members should monitor for signs of infection, eg, increased pain or decreased vision.[15]
On the day of discharge, clear instructions from every team member to educate the patient about follow-up are paramount because many ocular trauma patients will not return.[137] Monitoring in corneal laceration care extends beyond routine vitals and early infection detection; it involves structured, time-sensitive surveillance of ocular status, systemic condition, and patient compliance to prevent vision-threatening complications.[15]
Immediate Postoperative Monitoring (First 24 Hours)
In the immediate postoperative period, close observation is essential to detect early complications. Along with pain, nausea, and vital signs, the team should monitor ocular parameters, including anterior chamber depth, the integrity of the eye shield, and any sudden increase in discomfort or deterioration in vision. Early signs of complications like wound leak, hyphema progression, or raised intraocular pressure may present subtly and require prompt escalation.[138]
Early Postoperative Period (First Week)
During the first week, which is the most critical phase, all team members should actively look for warning signs of infection, inflammation, or wound instability. These include increasing redness, discharge, photophobia, decreased vision, or eyelid swelling. Monitoring should also include assessment of medication adherence, as missed antibiotic doses significantly increase the risk of endophthalmitis or keratitis.[37]
Ocular-Specific Monitoring Parameters
In addition to general symptoms, targeted ophthalmic monitoring should include:
- Wound integrity (Seidel test if indicated)
- Corneal clarity and edema
- Position and condition of sutures
- Anterior chamber reaction (cells/flare)
- Intraocular pressure trends (once safe to measure)
This structured assessment ensures early detection of complications, eg, wound leak, glaucoma, or uveitis.[12]
Systemic Monitoring and Risk Management
Systemic parameters remain important, especially in trauma patients. Monitoring should include:
- Signs of systemic infection
- Drug-related adverse effects (eg, antibiotic reactions)
- Hydration and nutritional status
In polytrauma cases, coordination with other specialties is essential to ensure overall patient stability.[43]
Discharge Planning and Compliance Monitoring
Discharge is a critical transition point. Given that many ocular trauma patients may default on follow-up, the team must ensure:
- Clear, repeated verbal and written instructions
- Emphasis on the importance of next-day follow-up
- Explanation of red flag symptoms requiring urgent care
Where possible, contact verification, reminder systems, or telephonic follow-up should be implemented to improve compliance.[139]
Interprofessional Monitoring
Monitoring in corneal laceration management is a continuous, interprofessional process that spans from the immediate postoperative period to long-term follow-up. Vigilant observation, clear communication, and strong patient education are essential for detecting complications early, ensuring compliance, and ultimately preserving vision.[37] The following team members play a role in monitoring:
- Nurses: Continuous monitoring, medication administration, patient education, and early identification of complications
- Ophthalmic technicians: Visual acuity checks, slit-lamp assistance, documentation of changes
- Pharmacists: Ensuring correct medication usage and adherence
- Optometrists/rehabilitation specialists: Early detection of visual deficits and planning rehabilitation[40]
Even after the initial recovery phase, patients require ongoing follow-up to detect the following:
- Late-onset glaucoma
- Progressive corneal scarring or astigmatism
- Retinal complications
Regular monitoring allows timely intervention, eg, suture adjustment, optical correction, or secondary surgery.[122] Any deterioration in symptoms, eg, sudden pain, vision loss, or discharge, should trigger immediate escalation to the ophthalmology team. A well-defined communication pathway ensures that no warning sign is overlooked.
Patient-Centered Monitoring Approach
Patients should be encouraged to actively participate in monitoring by the following:
- Reporting symptoms promptly
- Adhering strictly to medication schedules
- Maintaining protective measures (eye shield, avoiding trauma)
Empowering patients improves early detection and outcomes.
Media
(Click Image to Enlarge)
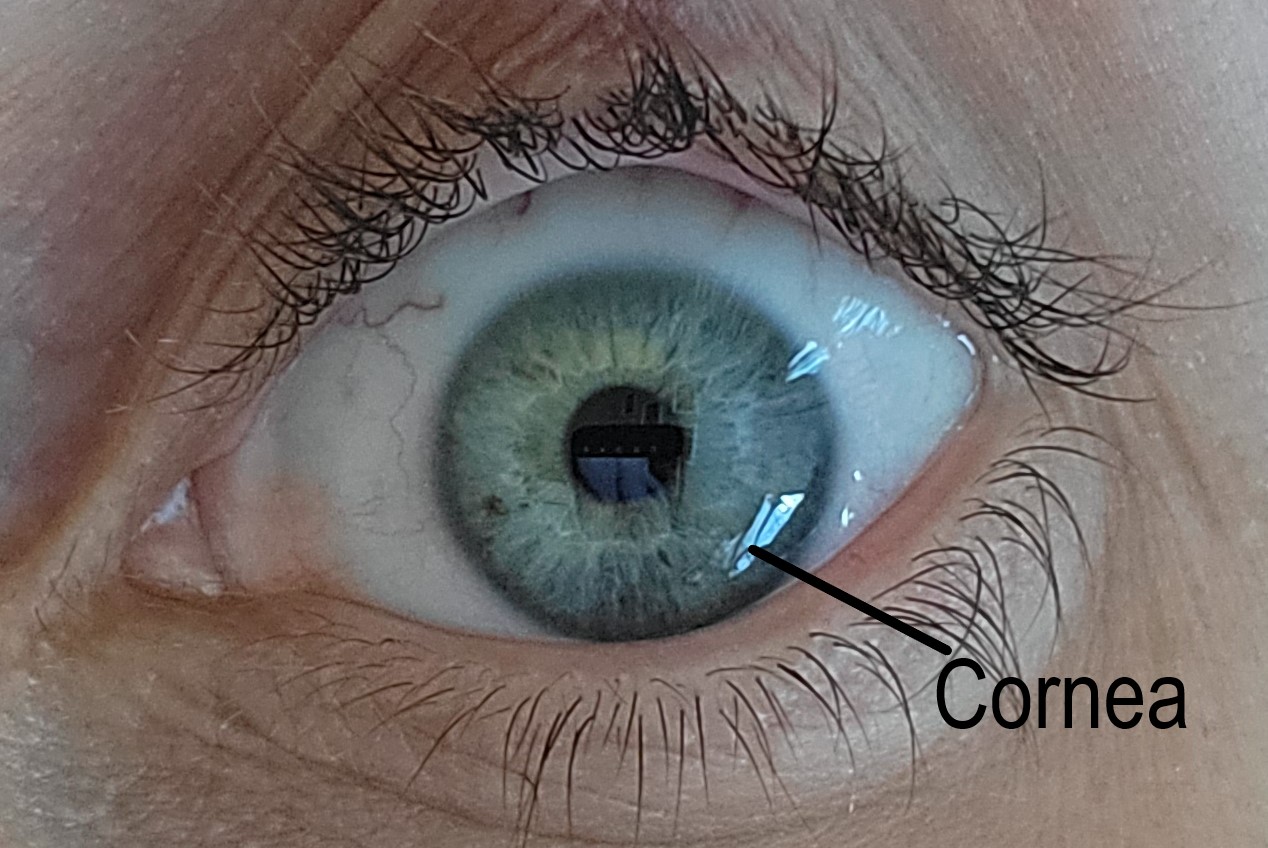
Normal Cornea. A normal cornea is transparent, avascular, and acts as a barrier to infection.
Contributed by G Legault, MD
(Click Image to Enlarge)
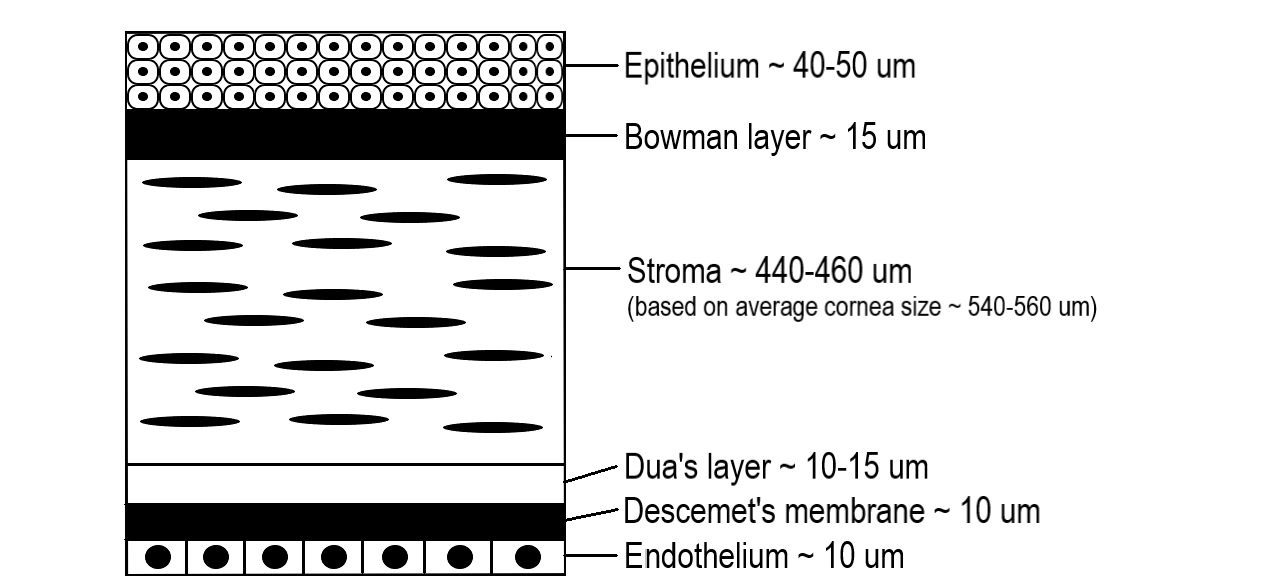
Layers of the Cornea.
Contributed by G Legault, MD
(Click Image to Enlarge)
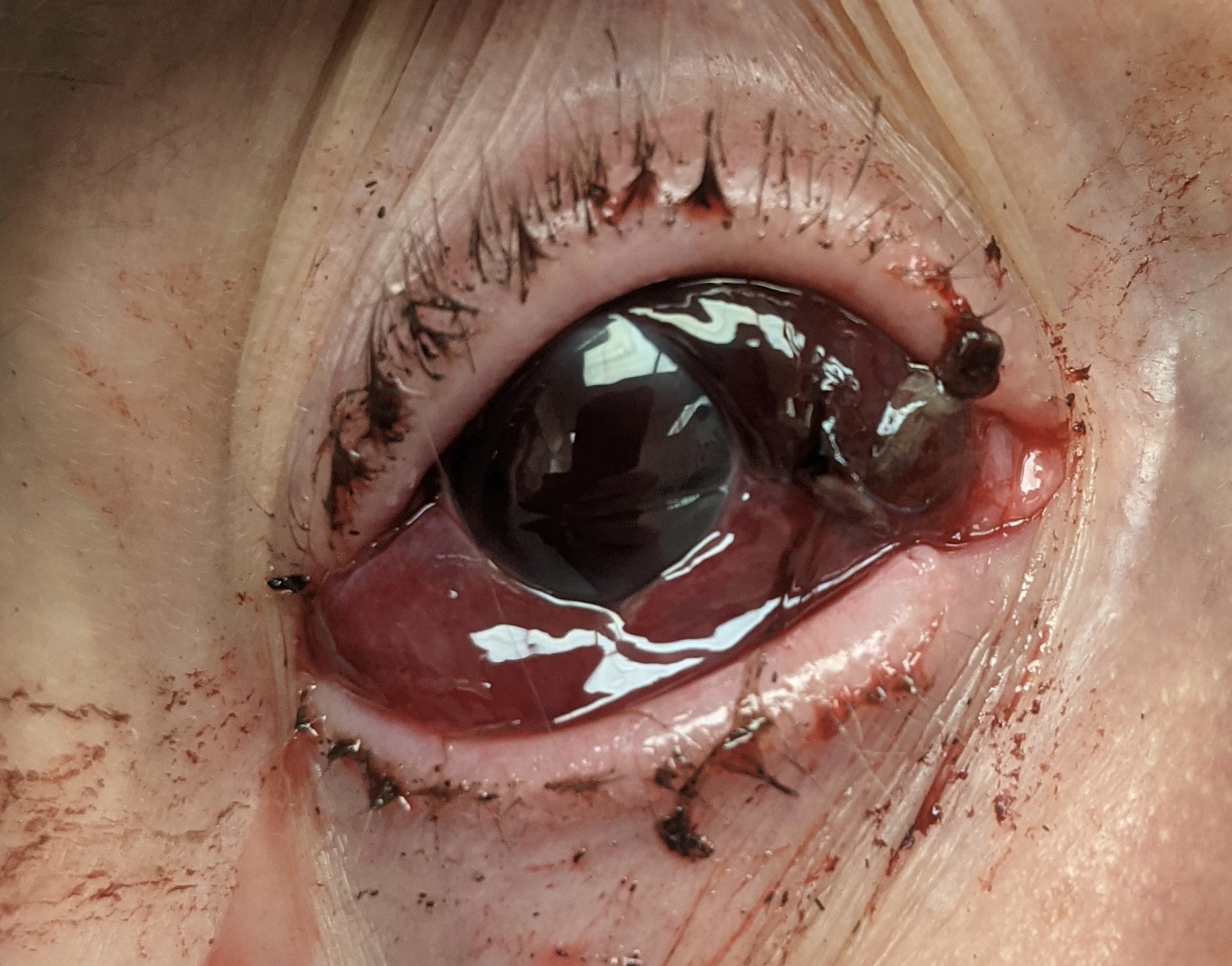
Corneoscleral Laceration. When performing a repair, after closing the limbus, clinicians should focus on the corneal aspect first and then the sclera to avoid tissue prolapse.
Contributed by H Blegen, DO
(Click Image to Enlarge)
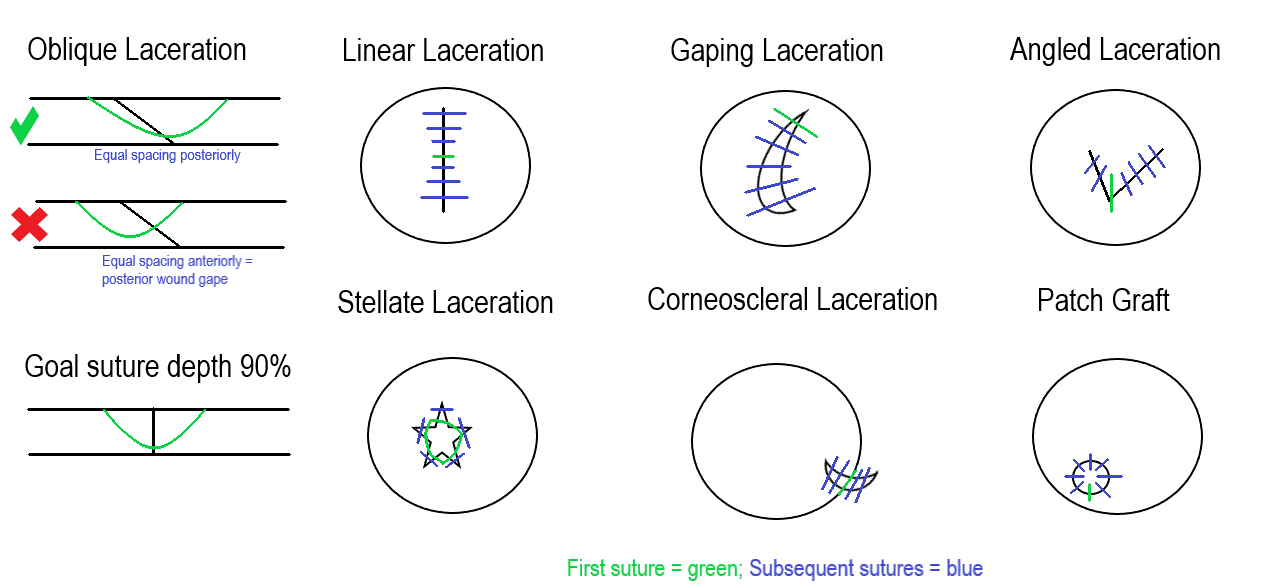
Corneal Laceration Suture Techniques. Image describing various corneal laceration techniques.
Contributed by G Legault, MD
References
Swain T, McGwin G Jr. The Prevalence of Eye Injury in the United States, Estimates from a Meta-Analysis. Ophthalmic epidemiology. 2020 Jun:27(3):186-193. doi: 10.1080/09286586.2019.1704794. Epub 2019 Dec 17 [PubMed PMID: 31847651]
Level 1 (high-level) evidenceVlasov A, Ryan DS, Ludlow S, Coggin A, Weichel ED, Stutzman RD, Bower KS, Colyer MH. Corneal and Corneoscleral Injury in Combat Ocular Trauma from Operations Iraqi Freedom and Enduring Freedom. Military medicine. 2017 Mar:182(S1):114-119. doi: 10.7205/MILMED-D-16-00041. Epub [PubMed PMID: 28291461]
Level 2 (mid-level) evidenceMacsai MS. The management of corneal trauma: advances in the past twenty-five years. Cornea. 2000 Sep:19(5):617-24 [PubMed PMID: 11009314]
Level 3 (low-level) evidenceVote BJ, Elder MJ. Cyanoacrylate glue for corneal perforations: a description of a surgical technique and a review of the literature. Clinical & experimental ophthalmology. 2000 Dec:28(6):437-42 [PubMed PMID: 11202468]
Beatty RF, Beatty RL. The repair of corneal and scleral lacerations. Seminars in ophthalmology. 1994 Sep:9(3):165-76 [PubMed PMID: 10155636]
Koster HR, Kenyon KR. Complications of surgery associated with ocular trauma. International ophthalmology clinics. 1992 Fall:32(4):157-78 [PubMed PMID: 1399345]
Mohseni M, Gurnani B, Blair K. Blunt Eye Trauma. StatPearls. 2026 Jan:(): [PubMed PMID: 29261988]
Gurnani B, Kaur K. Artificial intelligence in retinoblastoma and uveal melanoma - a narrative review. Expert review of anticancer therapy. 2026 May 8:():1-17. doi: 10.1080/14737140.2026.2671252. Epub 2026 May 8 [PubMed PMID: 42089602]
Level 3 (low-level) evidenceZheng J, Lu H, Chen Y, Liu W, Liu W. AI-guided surgical decision support system for corneal laceration repair: a prospective, non-randomized controlled feasibility study. Scientific reports. 2026 Mar 6:16(1):. doi: 10.1038/s41598-026-42805-4. Epub 2026 Mar 6 [PubMed PMID: 41792236]
Level 1 (high-level) evidenceGurnani B, Kaur K. Differentiating Pythium Keratitis From Fungal and Acanthamoeba Keratitis: A Practical Guide. StatPearls. 2026 Jan:(): [PubMed PMID: 42044243]
Gurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert review of medical devices. 2025 Dec:22(12):1287-1292. doi: 10.1080/17434440.2025.2582616. Epub 2025 Nov 2 [PubMed PMID: 41147335]
Niu L, Xu H, Liu B, Song M, Hu C, Wang Y, Jiang R. A 20-year retrospective analysis of ocular and adnexal injuries resulting from animal attacks in Eastern China. Annals of medicine. 2025 Dec:57(1):2537915. doi: 10.1080/07853890.2025.2537915. Epub 2025 Jul 29 [PubMed PMID: 40731115]
Level 2 (mid-level) evidenceShah SS, Gurnani B. Lens-Induced Glaucoma. StatPearls. 2026 Jan:(): [PubMed PMID: 34662038]
Gurnani B, Kaur K. Ocular Surface Squamous Neoplasia. StatPearls. 2026 Jan:(): [PubMed PMID: 34424655]
Santhosh LM, Venugopal A, Shankar D, Sethi K. Bilateral Severe Ocular Trauma Resulting From Drone Accident: A Case Report. Cornea. 2025 Dec 1:44(12):1551-1553. doi: 10.1097/ICO.0000000000003923. Epub 2025 Jul 1 [PubMed PMID: 40591369]
Level 3 (low-level) evidenceSasaki SI, Sumioka T, Yasuda S, Miyajima M, Iwanishi H, Reinach PS, Okada Y, Saika S. Lacking TRPA1 Cation Channel Impairs Primary Closure of a Stromal Incision Injury in a Mouse Cornea. Laboratory investigation; a journal of technical methods and pathology. 2025 Sep:105(9):104193. doi: 10.1016/j.labinv.2025.104193. Epub 2025 May 8 [PubMed PMID: 40348381]
Brooks SE, Johnson A, Kreuger EA. Novel Technique to Close Stellate Corneal Lacerations. Cornea. 2025 Apr 1:44(4):522-524. doi: 10.1097/ICO.0000000000003730. Epub 2024 Oct 29 [PubMed PMID: 39499165]
Gurnani B, Kaur K. Artificial Intelligence and Deep Learning in the Diagnosis of Pythium Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 42044246]
Pelletier J, Reagan K, McLeod S, Kronk N, Dickson K, Ohman K, Santos M. Epidemiology of ocular trauma in limited-resource settings: a narrative review. Frontiers in medicine. 2025:12():1585527. doi: 10.3389/fmed.2025.1585527. Epub 2025 Aug 25 [PubMed PMID: 40927196]
Level 3 (low-level) evidenceThomas J, Armstrong G. Use of Yamane technique for secondary intraocular lens implantation following open globe injury. BMJ case reports. 2023 Nov 21:16(11):. doi: 10.1136/bcr-2023-255995. Epub 2023 Nov 21 [PubMed PMID: 37989326]
Level 3 (low-level) evidenceDelMonte DW, Kim T. Anatomy and physiology of the cornea. Journal of cataract and refractive surgery. 2011 Mar:37(3):588-98. doi: 10.1016/j.jcrs.2010.12.037. Epub [PubMed PMID: 21333881]
Ahmadi AJ, Jakobiec FA. Corneal wound healing: cytokines and extracellular matrix proteins. International ophthalmology clinics. 2002 Summer:42(3):13-22 [PubMed PMID: 12131579]
Yang AY, Chow J, Liu J. Corneal Innervation and Sensation: The Eye and Beyond. The Yale journal of biology and medicine. 2018 Mar:91(1):13-21 [PubMed PMID: 29599653]
Ozkan O, Utine CA. Clinical anatomy: cornea and ocular surface. Medical hypothesis, discovery & innovation ophthalmology journal. 2025 Fall:14(3):60-72. doi: 10.51329/mehdiophthal1524. Epub 2025 Sep 27 [PubMed PMID: 41111639]
Teo AWJ, Zhang J, Zhou L, Liu YC. Metabolomics in Corneal Diseases: A Narrative Review from Clinical Aspects. Metabolites. 2023 Mar 3:13(3):. doi: 10.3390/metabo13030380. Epub 2023 Mar 3 [PubMed PMID: 36984820]
Level 3 (low-level) evidenceGurnani B, Kaur K. Redefining Dry Eye Disease Management: Emerging Pharmacologic and Device-Based Therapies in the Era of Precision Care: A Narrative Review. Ophthalmology and therapy. 2026 May:15(5):1561-1584. doi: 10.1007/s40123-026-01354-9. Epub 2026 Mar 23 [PubMed PMID: 41866434]
Level 3 (low-level) evidenceGurnani B, Kaur K. Bilateral limbal stem cell deficiency with xeroderma pigmentosum in a young Asian child. Clinical case reports. 2023 Aug:11(8):e7746. doi: 10.1002/ccr3.7746. Epub 2023 Jul 30 [PubMed PMID: 37529126]
Level 3 (low-level) evidenceFu L, Gurnani B, Hollick EJ. Artificial Corneal Transplantation. StatPearls. 2026 Jan:(): [PubMed PMID: 33760451]
Gurnani B, Kaur K, Lalgudi VG, Tripathy K. Risk Factors for Descemet Membrane Endothelial Keratoplasty Rejection: Current Perspectives- Systematic Review. Clinical ophthalmology (Auckland, N.Z.). 2023:17():421-440. doi: 10.2147/OPTH.S398418. Epub 2023 Feb 1 [PubMed PMID: 36755886]
Level 1 (high-level) evidenceGurnani B, Kaur K. Renaissance of an Emerging Pathogen-Pythium insidiosum Keratitis: An Indian Perspective. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4811-4830. doi: 10.2147/OPTH.S568552. Epub 2025 Dec 18 [PubMed PMID: 41446894]
Level 3 (low-level) evidenceOgata FT, Verma S, Coulson-Thomas VJ, Gesteira TF. TGF-β-Based Therapies for Treating Ocular Surface Disorders. Cells. 2024 Jun 26:13(13):. doi: 10.3390/cells13131105. Epub 2024 Jun 26 [PubMed PMID: 38994958]
McKay TB, Seyed-Razavi Y, Ghezzi CE, Dieckmann G, Nieland TJF, Cairns DM, Pollard RE, Hamrah P, Kaplan DL. Corneal pain and experimental model development. Progress in retinal and eye research. 2019 Jul:71():88-113. doi: 10.1016/j.preteyeres.2018.11.005. Epub 2018 Nov 16 [PubMed PMID: 30453079]
Zhu W, Xing Y. A Case of Ocular Infection with Clostridium tertium Caused by a Salute Gun Explosion. Clinical laboratory. 2024 Sep 1:70(9):. doi: 10.7754/Clin.Lab.2024.240342. Epub [PubMed PMID: 39257107]
Level 3 (low-level) evidenceErkan Pota Ç, Çetinkaya Yaprak A, İlhan HD. Evaluation of Ocular Trauma Score and risk factors to predict evisceration or enucleation in open globe injuries. Journal francais d'ophtalmologie. 2024 Oct:47(8):104259. doi: 10.1016/j.jfo.2024.104259. Epub 2024 Aug 1 [PubMed PMID: 39094369]
Seery CW, Choudhry HS, Dastjerdi MH. Zone 1 trauma: wound dehiscence compared to primary trauma. International ophthalmology. 2024 Feb 13:44(1):74. doi: 10.1007/s10792-024-02923-2. Epub 2024 Feb 13 [PubMed PMID: 38349413]
Weider L, Hughes K, Ciarochi J, Dunn E. Early versus delayed repair of facial fractures in the multiply injured patient. The American surgeon. 1999 Aug:65(8):790-3 [PubMed PMID: 10432093]
Alawi KA, Jadeedi SA, Shaqsi SA, Sahib M, Balushi TA. Isolated orbital roof fracture with concurrent orbital compartment syndrome: a case report. Journal of trauma and injury. 2025 Dec 29:():. doi: 10.20408/jti.2025.0070. Epub 2025 Dec 29 [PubMed PMID: 41461141]
Level 3 (low-level) evidenceSun M, Acosta AC, Emerick V, Adams S, Avila MY, Margo CE, Espana EM. Dysfunctional latent transforming growth factor β activation after corneal injury in a classical Ehlers-Danlos model. Matrix biology : journal of the International Society for Matrix Biology. 2024 Apr:128():21-30. doi: 10.1016/j.matbio.2024.02.004. Epub 2024 Feb 9 [PubMed PMID: 38340967]
Ma L, Fei B. Comprehensive review of surgical microscopes: technology development and medical applications. Journal of biomedical optics. 2021 Jan:26(1):. doi: 10.1117/1.JBO.26.1.010901. Epub [PubMed PMID: 33398948]
Huang L, Larson J. Nonsurgical Management of a Traumatic, Full-Thickness Corneal Laceration: A Case Report. WMJ : official publication of the State Medical Society of Wisconsin. 2024 Sep:123(4):307-310 [PubMed PMID: 39284093]
Level 3 (low-level) evidenceRay A, Gurnani B. Pediatric Cataract. StatPearls. 2026 Jan:(): [PubMed PMID: 34283446]
Nie X, Hui J, Han Z, Wang H, Zhou Y, Shao J, Wang L, Xu Z, Wu B, Cui C, Han Q, Liu W. A natural corneal extracellular matrix-inspired dual-crosslinked hydrogel bioadhesive for emergency corneal trauma repair. Acta biomaterialia. 2026 Mar:212():216-234. doi: 10.1016/j.actbio.2026.01.034. Epub 2026 Jan 17 [PubMed PMID: 41554492]
Spangler MD, Kirupaharan N, Edalat C, Berkenstock MK. Epidemiology of globe injury repair mechanisms in the TriNetX US collaborative network database: retrospective cohort study. BMC ophthalmology. 2025 Aug 18:25(1):465. doi: 10.1186/s12886-025-04300-8. Epub 2025 Aug 18 [PubMed PMID: 40826042]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Post-market surveillance of ophthalmic implants: role of real-world evidence. Expert review of medical devices. 2025 Dec:22(12):1303-1308. doi: 10.1080/17434440.2025.2579578. Epub 2025 Oct 24 [PubMed PMID: 41123186]
Balamurugan S, Gurnani B, Kaur K, Gireesh P, Narayana S. Traumatic intralenticular abscess-What is so different? The Indian journal of radiology & imaging. 2020 Jan-Mar:30(1):92-94. doi: 10.4103/ijri.IJRI_369_19. Epub 2020 Mar 30 [PubMed PMID: 32476758]
Gurnani B, Kaur K, Gireesh P. A rare presentation of anterior dislocation of calcified capsular bag in a spontaneously absorbed cataractous eye. Oman journal of ophthalmology. 2021 May-Aug:14(2):120-121. doi: 10.4103/ojo.OJO_65_2019. Epub 2021 Jun 28 [PubMed PMID: 34345149]
Gurnani B, Kaur K, Venugopal A, Srinivasan B, Bagga B, Iyer G, Christy J, Prajna L, Vanathi M, Garg P, Narayana S, Agarwal S, Sahu S. Pythium insidiosum keratitis - A review. Indian journal of ophthalmology. 2022 Apr:70(4):1107-1120. doi: 10.4103/ijo.IJO_1534_21. Epub [PubMed PMID: 35325996]
Gurnani B, Christy J, Narayana S, Kaur K, Moutappa F. Corneal Perforation Secondary to Rosacea Keratitis Managed with Excellent Visual Outcome. Nepalese journal of ophthalmology : a biannual peer-reviewed academic journal of the Nepal Ophthalmic Society : NEPJOPH. 2022 Jan:14(27):162-167. doi: 10.3126/nepjoph.v14i1.36454. Epub [PubMed PMID: 35996914]
Paulbuddhe V, Addya S, Gurnani B, Singh D, Tripathy K, Chawla R. Sympathetic Ophthalmia: Where Do We Currently Stand on Treatment Strategies? Clinical ophthalmology (Auckland, N.Z.). 2021:15():4201-4218. doi: 10.2147/OPTH.S289688. Epub 2021 Oct 20 [PubMed PMID: 34707340]
Kaur K, Mishra S, Gurnani B. First case of sunflower pattern calcific deposits and posterior capsular opacification on a pseudophakos. Clinical case reports. 2022 Sep:10(9):e6345. doi: 10.1002/ccr3.6345. Epub 2022 Sep 12 [PubMed PMID: 36172332]
Level 3 (low-level) evidenceGurnani B, Gireesh P, Kaur K. Chopstick technique for nucleus prolapse in cases of hypermature cataract during manual small-incision cataract surgery. Indian journal of ophthalmology. 2023 Mar:71(3):1051-1052. doi: 10.4103/IJO.IJO_2923_22. Epub [PubMed PMID: 36872749]
Level 3 (low-level) evidenceGurnani B, Kaur K. Immune Camouflage in Pythium insidiosum Keratitis: A Hypothesis on Molecular Mimicry and Host Pattern Recognition Receptor Evasion. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4855-4873. doi: 10.2147/OPTH.S560311. Epub 2025 Dec 19 [PubMed PMID: 41446892]
Gurnani B, Kaur K. Pythium Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 34424645]
Gurnani B, Kaur K. Anti-infective therapies for Pythium insidiosum keratitis. Expert review of anti-infective therapy. 2024 Oct:22(10):805-817. doi: 10.1080/14787210.2024.2403146. Epub 2024 Sep 13 [PubMed PMID: 39268901]
Gurnani B, Kaur K. Intricacies and solutions for interpretation of microbiologic samples of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2024 Apr 1:72(4):602-603. doi: 10.4103/IJO.IJO_1573_23. Epub 2024 Mar 28 [PubMed PMID: 38546474]
Gurnani B, Natarajan R, Mohan M, Kaur K. Breaking-Down Barriers: Proposal of Using Cellulose Biosynthesis Inhibitors and Cellulase Enzyme as a Novel Treatment Modality for Vision Threatening Pythium Insidiosum Keratitis. Clinical ophthalmology (Auckland, N.Z.). 2024:18():765-776. doi: 10.2147/OPTH.S450665. Epub 2024 Mar 11 [PubMed PMID: 38495678]
Gurnani B, Kaur K. Understanding barriers, recommended solutions, and future prospects for the diagnosis and management of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 Dec 1:71(12):3584-3586. doi: 10.4103/IJO.IJO_1041_23. Epub 2023 Nov 20 [PubMed PMID: 37991287]
Level 3 (low-level) evidenceGurnani B, Kaur K. Leap forward in clinical and photographic diagnosis of Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 Sep:71(9):3263-3264. doi: 10.4103/IJO.IJO_355_23. Epub [PubMed PMID: 37602622]
Cao B, Gonugunta VT, Radhakrishnan N, Lalitha P, Gurnani B, Kaur K, Iyer G, Agarwal S, Srinivasan B, Keenan JD, Prajna NV. Outcomes of Pythium keratitis: a meta-analysis of individual patient data. Current ophthalmology reports. 2022 Dec:10(4):198-208. doi: 10.1007/s40135-022-00302-7. Epub 2022 Nov 10 [PubMed PMID: 37250102]
Level 1 (high-level) evidenceGurnani B, Kaur K, Kumar T. Commentary: Current concepts, recent updates, and future treatment options for Pythium insidiosum keratitis. Indian journal of ophthalmology. 2023 May:71(5):1874-1876. doi: 10.4103/IJO.IJO_80_23. Epub [PubMed PMID: 37203047]
Level 3 (low-level) evidenceMazzoli RA, Gross KR, Butler FK. The use of rigid eye shields (Fox shields) at the point of injury for ocular trauma in Afghanistan. The journal of trauma and acute care surgery. 2014 Sep:77(3 Suppl 2):S156-62. doi: 10.1097/TA.0000000000000391. Epub [PubMed PMID: 25159350]
Level 2 (mid-level) evidenceGurnani B, Narayana S, Christy J, Rajkumar P, Kaur K, Gubert J. Successful management of pediatric pythium insidiosum keratitis with cyanoacrylate glue, linezolid, and azithromycin: Rare case report. European journal of ophthalmology. 2022 Sep:32(5):NP87-NP91. doi: 10.1177/11206721211006564. Epub 2021 Mar 28 [PubMed PMID: 33779337]
Level 3 (low-level) evidenceGurnani B, Kaur K, Agarwal S, Lalgudi VG, Shekhawat NS, Venugopal A, Tripathy K, Srinivasan B, Iyer G, Gubert J. Pythium insidiosum Keratitis: Past, Present, and Future. Ophthalmology and therapy. 2022 Oct:11(5):1629-1653. doi: 10.1007/s40123-022-00542-7. Epub 2022 Jul 5 [PubMed PMID: 35788551]
Gurnani B, Christy J, Narayana S, Rajkumar P, Kaur K, Gubert J. Retrospective multifactorial analysis of Pythium keratitis and review of literature. Indian journal of ophthalmology. 2021 May:69(5):1095-1101. doi: 10.4103/ijo.IJO_1808_20. Epub [PubMed PMID: 33913840]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Modified drug regimen for ophthalmic anesthesia during COVID-19 pandemic: Revisiting pharmacological concepts. Indian journal of pharmacology. 2021 Mar-Apr:53(2):178-179. doi: 10.4103/ijp.ijp_89_21. Epub [PubMed PMID: 34100406]
Benson WH, Snyder IS, Granus V, Odom JV, Macsai MS. Tetanus prophylaxis following ocular injuries. The Journal of emergency medicine. 1993 Nov-Dec:11(6):677-83 [PubMed PMID: 8157904]
Level 3 (low-level) evidenceParunović AB, Popović BA. Antibiotic prophylaxis in penetrating injuries of the eye. Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. Albrecht von Graefe's archive for clinical and experimental ophthalmology. 1976 May 26:199(3):277-9 [PubMed PMID: 1084710]
Level 3 (low-level) evidenceGurnani B, Kaur K. Successful management of delayed hyaluronidase hypersensitivity after subtenon's anesthesia during the COVID-19 pandemic: A rare case report. Indian journal of pharmacology. 2023 Jan-Feb:55(1):59-61. doi: 10.4103/ijp.ijp_995_21. Epub [PubMed PMID: 36960522]
Level 3 (low-level) evidenceParkash RO, Gurnani B, Kaur K, Parkash TO, Vajpayee RB, Baldev V. Novel nucleus management technique in hypermature morgagnian cataracts with liquified cortex during phacoemulsification. European journal of ophthalmology. 2023 Jul:33(4):1750-1754. doi: 10.1177/11206721231158143. Epub 2023 Feb 22 [PubMed PMID: 36811620]
Gurnani B, Kaur K, Tandon A. Letter Regarding: Randomized Double-Masked Placebo-Controlled Trial for the Management of Pythium Keratitis: Combination of Antibiotics Versus Monotherapy. Cornea. 2023 Dec 1:42(12):e22-e23. doi: 10.1097/ICO.0000000000003350. Epub 2023 Jul 18 [PubMed PMID: 37487172]
Level 1 (high-level) evidenceScott R. The injured eye. Philosophical transactions of the Royal Society of London. Series B, Biological sciences. 2011 Jan 27:366(1562):251-60. doi: 10.1098/rstb.2010.0234. Epub [PubMed PMID: 21149360]
Gurnani B, Kaur K. Predicting Prognosis Based on Regional Prevalence, Ulcer Morphology and Treatment Strategy in Vision-Threatening Pythium insidiosum Keratitis. Clinical ophthalmology (Auckland, N.Z.). 2023:17():1307-1314. doi: 10.2147/OPTH.S412274. Epub 2023 May 5 [PubMed PMID: 37181081]
Campbell TD, Gnugnoli DM. Seidel Test. StatPearls. 2026 Jan:(): [PubMed PMID: 31082063]
Isenberg SJ. The ocular application of povidone-iodine. Community eye health. 2003:16(46):30-1 [PubMed PMID: 17491857]
Gurnani B, Kaur K. Tips to prevent inadvertent stromal staining and Descemet membrane detachment while performing paracentesis during cataract surgery. Indian journal of ophthalmology. 2023 May:71(5):2300-2301. doi: 10.4103/IJO.IJO_3310_22. Epub [PubMed PMID: 37202984]
Gurnani B, Kaur K, Gurav J. Natasol as a future management option to combat fungal keratitis. Indian journal of ophthalmology. 2023 May:71(5):2302-2303. doi: 10.4103/IJO.IJO_190_23. Epub [PubMed PMID: 37202986]
Omotoye OJ, Ajayi IA, Ajite KO, Bodunde OF. Factors Responsible for Poor Visual Outcome Following Emergency Eye Surgery in a Tertiary Eye Centre. Ethiopian journal of health sciences. 2019 Sep:29(5):631-638. doi: 10.4314/ejhs.v29i5.14. Epub [PubMed PMID: 31666785]
Gurnani B, Kaur K. Traumatic Iris Reconstruction. StatPearls. 2026 Jan:(): [PubMed PMID: 35201728]
Lodhi O, Tripathy K. Anesthesia for Ophthalmic Surgery. StatPearls. 2026 Jan:(): [PubMed PMID: 34283497]
Kohli R, Ramsingh H, Makkad B. The anesthetic management of ocular trauma. International anesthesiology clinics. 2007 Summer:45(3):83-98 [PubMed PMID: 17622831]
Tan J, Foster LJR, Watson SL. Corneal Sealants in Clinical Use: A Systematic Review. Current eye research. 2020 Sep:45(9):1025-1030. doi: 10.1080/02713683.2020.1764052. Epub 2020 May 27 [PubMed PMID: 32460646]
Level 1 (high-level) evidenceZhang T, Jia Y, Li S, Shi W. Individualized Corneal Patching for Treatment of Corneal Trauma Combined with Tissue Defects. Journal of ophthalmology. 2020:2020():8437479. doi: 10.1155/2020/8437479. Epub 2020 Nov 23 [PubMed PMID: 33299602]
Sharma A, Kaur R, Kumar S, Gupta P, Pandav S, Patnaik B, Gupta A. Fibrin glue versus N-butyl-2-cyanoacrylate in corneal perforations. Ophthalmology. 2003 Feb:110(2):291-8 [PubMed PMID: 12578769]
Level 1 (high-level) evidenceMatalia HP, Nandini C, Matalia J. Surgical technique for the management of corneal perforation in brittle cornea. Indian journal of ophthalmology. 2021 Sep:69(9):2521-2523. doi: 10.4103/ijo.IJO_2542_20. Epub [PubMed PMID: 34427257]
Vinchon M, Cotten A, Clarisse J, Chiki R, Christiaens JL. Cervical myelopathy secondary to Hunter syndrome in an adult. AJNR. American journal of neuroradiology. 1995 Aug:16(7):1402-3 [PubMed PMID: 7484623]
Krysik K, Dobrowolski D, Wylegala E, Lyssek-Boron A. Amniotic Membrane as a Main Component in Treatments Supporting Healing and Patch Grafts in Corneal Melting and Perforations. Journal of ophthalmology. 2020:2020():4238919. doi: 10.1155/2020/4238919. Epub 2020 Feb 14 [PubMed PMID: 32148944]
Ashena Z, Holmes C, Nanavaty MA. Pericardium Patch Graft for Severe Corneal Wound Burn. Journal of current ophthalmology. 2021 Jul-Sep:33(3):342-344. doi: 10.4103/joco.joco_195_20. Epub 2021 Oct 22 [PubMed PMID: 34765825]
Daoud YJ, Smith R, Smith T, Akpek EK, Ward DE, Stark WJ. The intraoperative impression and postoperative outcomes of gamma-irradiated corneas in corneal and glaucoma patch surgery. Cornea. 2011 Dec:30(12):1387-91. doi: 10.1097/ICO.0b013e31821c9c09. Epub [PubMed PMID: 21993467]
Gurnani B, Kaur K, Rustagi IM. Is refractive enhancement a safer option for post laser in situ keratomileusis and small incision lenticule extraction regression - How far we have come? Indian journal of ophthalmology. 2023 Jun:71(6):2597-2598. doi: 10.4103/IJO.IJO_450_23. Epub [PubMed PMID: 37322689]
Parkash RO, Gurnani B, Kaur K, Parkash TO, Sharma T. Assessing the validity of flap motility sign in predicting the extent of anterior capsular tears in phacoemulsification. Indian journal of ophthalmology. 2023 Aug:71(8):3095-3099. doi: 10.4103/IJO.IJO_2552_22. Epub [PubMed PMID: 37530287]
Okoye GS, Gurnani B. Traumatic Cataract. StatPearls. 2026 Jan:(): [PubMed PMID: 37603642]
Gurnani B, Balamurugan S, Kanakath A, Kaur K, Gupta A, Chaudhary S. First clinical case series of frosted branch angiitis: A diagnostic algorithm is suggested. Clinical case reports. 2023 Sep:11(9):e7778. doi: 10.1002/ccr3.7778. Epub 2023 Aug 25 [PubMed PMID: 37636879]
Level 2 (mid-level) evidenceYin XL, Ji ZY, Li XX, Liang XM, Ji SX. Surgical approaches to correct corneal astigmatism at time of cataract surgery: a mini-review. International journal of ophthalmology. 2024:17(7):1370-1374. doi: 10.18240/ijo.2024.07.23. Epub 2024 Jul 18 [PubMed PMID: 39026920]
Parkash RO, Gurnani B, Kaur K, Parkash TO, Vajpayee RB. Novel trocar assisted intraocular lens and capsular bag complex fixation. European journal of ophthalmology. 2024 Mar:34(2):583-588. doi: 10.1177/11206721231208662. Epub 2023 Oct 26 [PubMed PMID: 37882171]
Gurnani B, Kaur K. Leveraging ChatGPT for ophthalmic education: A critical appraisal. European journal of ophthalmology. 2024 Mar:34(2):323-327. doi: 10.1177/11206721231215862. Epub 2023 Nov 16 [PubMed PMID: 37974429]
Meena A, Agrawal A, Parmar G, Gurnani B. Subconjunctival dexamethasone-assisted conjunctival autograft harvesting versus normal saline during pterygium surgery - A randomized clinical trial. Indian journal of ophthalmology. 2024 Feb 1:72(2):217-222. doi: 10.4103/IJO.IJO_969_23. Epub 2023 Dec 15 [PubMed PMID: 38099381]
Level 1 (high-level) evidenceHall WA, Gurnani B. Compressive Optic Neuropathy. StatPearls. 2026 Jan:(): [PubMed PMID: 32809418]
Murugan SB, Sunil Kumar, Gurnani B, Kaur K. Assessment of Subjective Visual Experiences During Intraocular Surgery and Intravitreal Injection Among Uveitis Patients at a Tertiary Eye Hospital: A Cross-Sectional Observational Study. Ophthalmology and therapy. 2026 Jan:15(1):173-191. doi: 10.1007/s40123-025-01264-2. Epub 2025 Nov 6 [PubMed PMID: 41196490]
Level 2 (mid-level) evidenceAzmat CE, Council M. Wound Closure Techniques. StatPearls. 2026 Jan:(): [PubMed PMID: 29262163]
Gurnani B, Kaur K. Refractive Surprises After Cataract Surgery: Identification and Management in Optometric Practice- A Comprehensive Review. Clinical optometry. 2026:18():572733. doi: 10.2147/OPTO.S572733. Epub 2026 Apr 29 [PubMed PMID: 42083643]
Shetty PA, Natarajan R, Bhalerao SA, Vuyyuru S, Thigale UY, Tara D. Prognostic factors for visual outcome after surgical repair of limbal corneal laceration at a tertiary eye care center in South India. Indian journal of ophthalmology. 2023 Sep:71(9):3198-3202. doi: 10.4103/IJO.IJO_156_23. Epub [PubMed PMID: 37602608]
El Chehab H, Renard JP, Dot C. [Post-traumatic endophthalmitis]. Journal francais d'ophtalmologie. 2016 Jan:39(1):98-106. doi: 10.1016/j.jfo.2015.08.005. Epub 2015 Nov 10 [PubMed PMID: 26563842]
Sheu SJ. Endophthalmitis. Korean journal of ophthalmology : KJO. 2017 Aug:31(4):283-289. doi: 10.3341/kjo.2017.0036. Epub 2017 Jun 28 [PubMed PMID: 28752698]
Loporchio D, Mukkamala L, Gorukanti K, Zarbin M, Langer P, Bhagat N. Intraocular foreign bodies: A review. Survey of ophthalmology. 2016 Sep-Oct:61(5):582-96. doi: 10.1016/j.survophthal.2016.03.005. Epub 2016 Mar 17 [PubMed PMID: 26994871]
Level 3 (low-level) evidenceTong AY, Gupta PK, Kim T. Wound closure and tissue adhesives in clear corneal incision cataract surgery. Current opinion in ophthalmology. 2018 Jan:29(1):14-18. doi: 10.1097/ICU.0000000000000431. Epub [PubMed PMID: 28902719]
Level 3 (low-level) evidenceHamill MB. Corneal and scleral trauma. Ophthalmology clinics of North America. 2002 Jun:15(2):185-94 [PubMed PMID: 12229235]
Kaufman SC, Insler MS. Surgical repair of a traumatic iridodialysis. Ophthalmic surgery and lasers. 1996 Nov:27(11):963-6 [PubMed PMID: 8938808]
Level 3 (low-level) evidenceMikhail M, Koushan K, Sharda RK, Isaza G, Mann KD. Traumatic aniridia in a pseudophakic patient 6 years following surgery. Clinical ophthalmology (Auckland, N.Z.). 2012:6():237-41. doi: 10.2147/OPTH.S25396. Epub 2012 Feb 10 [PubMed PMID: 22347795]
Level 3 (low-level) evidenceReed JW. Corneal tattooing to reduce glare in cases of traumatic iris loss. Cornea. 1994 Sep:13(5):401-5 [PubMed PMID: 7995061]
Level 3 (low-level) evidenceMayer CS, Reznicek L, Hoffmann AE. Pupillary Reconstruction and Outcome after Artificial Iris Implantation. Ophthalmology. 2016 May:123(5):1011-8. doi: 10.1016/j.ophtha.2016.01.026. Epub 2016 Feb 28 [PubMed PMID: 26935356]
Blum M, Tetz MR, Greiner C, Voelcker HE. Treatment of traumatic cataracts. Journal of cataract and refractive surgery. 1996 Apr:22(3):342-6 [PubMed PMID: 8778368]
Level 2 (mid-level) evidenceStefan C, Nenciu A. Post-traumatic bacterial keratitis--a microbiological prospective clinical study. Oftalmologia (Bucharest, Romania : 1990). 2006:50(3):118-22 [PubMed PMID: 17144518]
Adler E, Miller D, Rock O, Spierer O, Forster R. Microbiology and biofilm of corneal sutures. The British journal of ophthalmology. 2018 Nov:102(11):1602-1606. doi: 10.1136/bjophthalmol-2018-312133. Epub 2018 Aug 12 [PubMed PMID: 30100555]
Jones WL. Posttraumatic glaucoma. Journal of the American Optometric Association. 1987 Sep:58(9):708-15 [PubMed PMID: 3502262]
Subudhi P, Kanungo S, Subudhi BN. AN ATYPICAL CASE OF SYMPATHETIC OPHTHALMIA AFTER LIMBAL CORNEAL LACERATION. Retinal cases & brief reports. 2017 Spring:11(2):141-144. doi: 10.1097/ICB.0000000000000313. Epub [PubMed PMID: 27124790]
Level 3 (low-level) evidenceScanzera AC, Dunbar G, Shah V, Cortina MS, Leiderman YI, Shorter E. Visual Rehabilitation With Contact Lenses Following Open Globe Trauma. Eye & contact lens. 2021 May 1:47(5):288-291. doi: 10.1097/ICL.0000000000000756. Epub [PubMed PMID: 33181528]
Nobe JR, Moura BT, Robin JB, Smith RE. Results of penetrating keratoplasty for the treatment of corneal perforations. Archives of ophthalmology (Chicago, Ill. : 1960). 1990 Jul:108(7):939-41 [PubMed PMID: 2369351]
Gurnani B, Kaur K. Corneal cross-linking for keratoconus: a global economic and clinical perspective. Journal of medical economics. 2025 Dec:28(1):2119-2124. doi: 10.1080/13696998.2025.2587416. Epub 2025 Nov 30 [PubMed PMID: 41320236]
Level 3 (low-level) evidenceGurnani B, Feroze KB, Patel BC. Neurotrophic Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 28613758]
Pastar I, Stojadinovic O, Yin NC, Ramirez H, Nusbaum AG, Sawaya A, Patel SB, Khalid L, Isseroff RR, Tomic-Canic M. Epithelialization in Wound Healing: A Comprehensive Review. Advances in wound care. 2014 Jul 1:3(7):445-464 [PubMed PMID: 25032064]
Level 3 (low-level) evidenceMurugan SRB, Sanjay S, Somanath A, Mahendradas P, Patil A, Kaur K, Gurnani B. Artificial Intelligence in Uveitis: Innovations in Diagnosis and Therapeutic Strategies. Clinical ophthalmology (Auckland, N.Z.). 2024:18():3753-3766. doi: 10.2147/OPTH.S495307. Epub 2024 Dec 14 [PubMed PMID: 39703602]
Ostadian F, Farrahi F, Zolfaghari M, Latifi SM. Analysis of Operated Patients with Ocular Trauma: A 10-Year Retrospective Study. Advanced biomedical research. 2023:12():64. doi: 10.4103/abr.abr_108_21. Epub 2023 Mar 21 [PubMed PMID: 37200739]
Level 2 (mid-level) evidenceBrown GC. Vision and quality-of-life. Transactions of the American Ophthalmological Society. 1999:97():473-511 [PubMed PMID: 10703139]
Level 2 (mid-level) evidenceKuhn F, Morris R, Witherspoon CD, Mann L. Epidemiology of blinding trauma in the United States Eye Injury Registry. Ophthalmic epidemiology. 2006 Jun:13(3):209-16 [PubMed PMID: 16854775]
Level 2 (mid-level) evidenceHenderson D. Ocular trauma: one in the eye for safety glasses. Archives of emergency medicine. 1991 Sep:8(3):201-4 [PubMed PMID: 1930506]
Ong HS, Barsam A, Morris OC, Siriwardena D, Verma S. A survey of ocular sports trauma and the role of eye protection. Contact lens & anterior eye : the journal of the British Contact Lens Association. 2012 Dec:35(6):285-7. doi: 10.1016/j.clae.2012.07.007. Epub 2012 Aug 13 [PubMed PMID: 22898257]
Level 3 (low-level) evidenceHoskin AK, Mackey DA, Keay L, Agrawal R, Watson S. Eye Injuries across history and the evolution of eye protection. Acta ophthalmologica. 2019 Sep:97(6):637-643. doi: 10.1111/aos.14086. Epub 2019 Mar 25 [PubMed PMID: 30907494]
Thomas R, McManus JG, Johnson A, Mayer P, Wade C, Holcomb JB. Ocular injury reduction from ocular protection use in current combat operations. The Journal of trauma. 2009 Apr:66(4 Suppl):S99-103. doi: 10.1097/TA.0b013e31819d8695. Epub [PubMed PMID: 19359977]
Level 2 (mid-level) evidenceBoss JD, Shah CT, Elner VM, Hassan AS. Assessment of Office-Based Practice Patterns on Protective Eyewear Counseling for Patients With Monocular Vision. Ophthalmic plastic and reconstructive surgery. 2015 Sep-Oct:31(5):361-3. doi: 10.1097/IOP.0000000000000348. Epub [PubMed PMID: 25393903]
Level 2 (mid-level) evidenceVillabona-Martinez V, Dutra BAL, Wilson SE. Insights from animal studies exploring the efficacy and safety of topical losartan, in prophylaxis and treatment of corneal scarring fibrosis. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie. 2025 Feb:183():117857. doi: 10.1016/j.biopha.2025.117857. Epub 2025 Jan 17 [PubMed PMID: 39826357]
Level 3 (low-level) evidenceGurnani B, Kaur K. Manual Small Incision Cataract Surgery. StatPearls. 2026 Jan:(): [PubMed PMID: 35881728]
Kaur K, Gurnani B. Ectopia Lentis. StatPearls. 2026 Jan:(): [PubMed PMID: 35201721]
Engelhard SB, Salek SS, Justin GA, Sim AJ, Woreta FA, Reddy AK. Malpractice Litigation in Ophthalmic Trauma. Clinical ophthalmology (Auckland, N.Z.). 2020:14():1979-1986. doi: 10.2147/OPTH.S260226. Epub 2020 Jul 12 [PubMed PMID: 32764863]
Sung EK, Nadgir RN, Fujita A, Siegel C, Ghafouri RH, Traband A, Sakai O. Injuries of the globe: what can the radiologist offer? Radiographics : a review publication of the Radiological Society of North America, Inc. 2014 May-Jun:34(3):764-76. doi: 10.1148/rg.343135120. Epub [PubMed PMID: 24819794]
Kuhn F, Maisiak R, Mann L, Mester V, Morris R, Witherspoon CD. The Ocular Trauma Score (OTS). Ophthalmology clinics of North America. 2002 Jun:15(2):163-5, vi [PubMed PMID: 12229231]
Maqsood SE, Hamada S, Lake D, Matsou A, Elalfy M. Management of Ocular Surface Inflammation with Persistent Epithelial Defects Using a Sutureless Human Amniotic Membrane Dehydrated Matrix: A Prospective Study Utilizing a Digital Ocular Surface Assessment Tool. Clinical ophthalmology (Auckland, N.Z.). 2024:18():1467-1478. doi: 10.2147/OPTH.S456864. Epub 2024 May 25 [PubMed PMID: 38813539]
Aaland MO, Marose K, Zhu TH. The lost to trauma patient follow-up: a system or patient problem. The journal of trauma and acute care surgery. 2012 Dec:73(6):1507-11. doi: 10.1097/TA.0b013e31826fc928. Epub [PubMed PMID: 23147179]
Level 2 (mid-level) evidenceGurnani B, Kaur K. Response to letter regarding "Evaluating the novel role of ChatGPT-4 in addressing corneal ulcer queries: An AI-powered insight". European journal of ophthalmology. 2026 May:36(3):NP5-NP7. doi: 10.1177/11206721251357376. Epub 2025 Jul 9 [PubMed PMID: 40629931]
Level 3 (low-level) evidenceSadegh G, Sima S, Mehdi B. Penetrating globe injury during rhinoplasty surgery; A case report. JPRAS open. 2023 Dec:38():269-273. doi: 10.1016/j.jpra.2023.10.011. Epub 2023 Oct 28 [PubMed PMID: 38021321]
Level 3 (low-level) evidence