Introduction
Duane retraction syndrome, previously known as Stilling-Turk-Duane syndrome, is caused by the absence or partial development of the abducens nucleus and nerve. As a result, there is aberrant innervation of the lateral rectus by the oculomotor nerve. Similar developmental anomalies of 1 or more cranial nerves have come to be grouped under congenital cranial dysinnervation disorders. These anomalies may be termed primary due to the absence of normal innervation or secondary following aberrant innervations from other cranial nerves.[1] The evaluation and management of Duane retraction syndrome can be very challenging, and a judicious approach is essential.[2]
Duane retraction syndrome is a rare, congenital ocular motility disorder characterized by limitation or absence of horizontal eye movements, globe retraction, and narrowing of the palpebral fissure on attempted adduction. First described by Alexander Duane in 1905, this condition represents approximately 1% to 4% of all cases of strabismus. The pathophysiology is now understood to involve a congenital cranial dysinnervation disorder, in which aberrant innervation of the lateral rectus muscle by branches of the oculomotor nerve leads to paradoxical co-contraction of horizontal recti. Although classically unilateral, Duane retraction syndrome may be bilateral in 10% to 20% of cases and is more commonly observed in females, with a predilection for the left eye.[3]
The etiology is linked to developmental anomalies of the abducens nerve (cranial nerve VI) or its nucleus, resulting in absent or hypoplastic innervation and compensatory miswiring from the oculomotor nerve. This neurogenic origin is supported by magnetic resonance imaging (MRI) studies demonstrating absent abducens nerve and by electromyography (EMG) findings of simultaneous lateral and medial rectus contraction during attempted adduction. In some cases, Duane retraction syndrome is associated with systemic anomalies such as Goldenhar syndrome, Klippel-Feil anomaly, or other congenital malformations, reinforcing the notion of a broader embryologic insult affecting cranial nerve development.[4]
Clinically, Duane retraction syndrome is classified into 3 primary types according to Huber's classification (1974):
- Type I: Marked limitation or absence of abduction, with relatively normal adduction and globe retraction on adduction.
- Type II: Limitation or absence of adduction with relatively normal abduction.
- Type III: Limitation of both abduction and adduction, often with significant globe retraction.[5]
Patients may also exhibit upshoots or downshoots on adduction due to leash effects or mechanical factors within the extraocular muscle pulleys. Abnormal head posture is common as patients adopt compensatory face turns to maintain binocular single vision in primary gaze. The severity of motility restriction and retraction varies widely, influencing both functional and cosmetic concerns. Epidemiologically, Duane retraction syndrome accounts for a small fraction of strabismus cases worldwide but carries substantial clinical importance due to its distinct presentation, surgical challenges, and potential associations with systemic disorders. Population-based studies indicate prevalence rates ranging from 0.1 to 0.7 per 1000 live births, though true incidence may be underestimated due to underdiagnosis in mild cases. Awareness among pediatricians, ophthalmologists, and orthoptists is critical for early recognition and evaluation.[6]
From a diagnostic standpoint, Duane retraction syndrome is primarily a clinical diagnosis supported by a detailed ocular motility examination. Key signs include narrowing of the palpebral fissure on adduction, globe retraction, and variable upshoots or downshoots. Forced duction testing may reveal mechanical restrictions, but the hallmark finding is paradoxical co-contraction of horizontal recti, confirmed by EMG. Imaging with high-resolution orbital MRI or diffusion tensor imaging can delineate the absence of the abducens nerve, providing objective confirmation and aiding in surgical planning. Assessment should also include evaluation for associated systemic anomalies, as up to 30% of patients may have other congenital malformations.[7]
Management of Duane retraction syndrome is individualized and guided by the severity of motility limitation, presence of abnormal head posture, and patient symptoms. Mild cases with good primary gaze alignment may require only observation and periodic follow-up. Surgical intervention is indicated for significant misalignment in primary gaze, large abnormal head posture, or cosmetically disturbing globe retraction and upshoots or downshoots. Procedures may include recession of the medial rectus, lateral rectus, or a combination, as well as vertical rectus transpositions in selected cases. The surgical approach is often more complex than in other forms of strabismus due to the paradoxical innervation and risk of exacerbating globe retraction. Overcorrection, induced vertical deviations, and persistent limitation are recognized challenges.[8]
Duane retraction syndrome is nonprogressive, but long-term follow-up is essential, particularly in children, to monitor ocular alignment, binocular function, and amblyopia risk. Amblyopia occurs in up to 10% of cases, necessitating prompt detection and treatment. Orthoptic therapy plays a supportive role in maintaining binocular vision and managing mild head postures, although it does not correct the underlying innervational anomaly.[9]
Recent advances in understanding Duane retraction syndrome pathogenesis have emerged from genetic and neuroimaging studies. Mutations in genes such as CHN1 (encoding alpha2-chimaerin) have been identified in familial cases, implicating axon guidance defects in cranial nerve development. These findings place Duane retraction syndrome within the broader category of congenital cranial dysinnervation disorders, alongside Möbius syndrome and congenital fibrosis of the extraocular muscles. This reclassification has shifted the focus from purely mechanical explanations to neurodevelopmental mechanisms, fostering novel research avenues.[10]
The psychosocial impact of Duane retraction syndrome should not be underestimated. Visible eye movement anomalies and abnormal head posture can affect self-esteem, social interactions, and quality of life, particularly in adolescents. Counseling, patient education, and appropriate referral for psychological support may be beneficial in selected cases. In pediatric patients, parental reassurance and guidance are critical to alleviate anxiety and ensure adherence to follow-up schedules.[11]
Interprofessional collaboration is central to optimal Duane retraction syndrome management. Pediatric ophthalmologists, orthoptists, neurologists, radiologists, and genetic counselors all contribute to comprehensive evaluation and care. For example, neurologists may assess for associated cranial nerve or central nervous system anomalies, whereas genetic counselors provide insight into inheritance patterns and recurrence risks. Radiologists skilled in high-resolution orbital imaging play an important role in confirming diagnosis and guiding surgical strategy. Orthoptists assist with functional assessment, prism adaptation, and post-operative rehabilitation, enhancing overall outcomes.[12]
In conclusion, Duane retraction syndrome represents a distinct, nonprogressive congenital ocular motility disorder with complex neurogenic and mechanical features. Advances in neuroimaging and genetics have enriched our understanding of its pathophysiology, whereas surgical and non-surgical management strategies continue to evolve. Early recognition, thorough evaluation for systemic associations, individualized treatment planning, and long-term multidisciplinary follow-up are key pillars in optimizing functional and cosmetic outcomes for patients. This activity equips learners with an evidence-based, clinically relevant framework for diagnosing and managing Duane retraction syndrome, integrating current guidelines, expert consensus, and interprofessional care principles to improve patient-centered outcomes.[13]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Although the condition was first described in the literature as early as 1887, the etiology remains elusive. The advent of muscle electrophysiology and modern neuroimaging techniques, such as MRI, aided in the understanding that the underlying abnormality in Duane retraction syndrome is the absence or partial development of the abducent nucleus and nerve, resulting in aberrant innervation of the lateral rectus by the oculomotor nerve.[14][15][16]
Myofibers of extraocular muscles originate from mesodermal condensations around the eye. In embryos measuring about 7 mm in length, the extraocular muscles appear as a single muscle mass innervated by the oculomotor nerve. When the embryo is 8 to 12 mm long, this mass divides into separate muscles, at which point the trochlear and abducent nerves establish their connections. Due to the disturbing influences of unknown origin, the abducens nerve fails to develop, causing branches of the oculomotor nerve to remain in contact with the muscle mass that later becomes the lateral rectus.[16]
Considering the other ocular and systemic anomalies associated with Duane retraction syndrome, these disturbing influences are believed to affect the developing structures of the body between 4 and 8 weeks of gestation.[17] Pfaffenbach et al showed that sporadic forms of Duane retraction syndrome are at 10 to 20 times greater risk of having other congenital malformations, divided into mainly 4 categories—skeletal, auricular, ocular, and neural.[18]
Skeletal abnormalities include cleft palate, limb deformities, phocomelia, vertebral anomalies, and spina bifida. Auricular abnormalities include preauricular tags, pinna defects, and sensorineural deafness. Neural defects involve the third, fourth, and sixth cranial nerves. Ocular associations of Duane retraction syndrome are numerous and include epidermal dermoids, ptosis, dysplasia of the iris stroma, iris heterochromia, pupillary anomalies, cataracts, colobomas, optic nerve hypoplasias, morning glory disk, and nystagmus.[14]
Duane retraction syndrome is commonly a sporadic disorder, but in 10% of cases, it may be familial. Both autosomal dominant and recessive forms of Duane retraction syndrome have been documented. In cases of isolated Duane retraction syndrome, the DURS1 gene on chromosome 2q31 has been identified.[19] The autosomal dominant pattern of Duane retraction syndrome is associated with mutations in the CHN1 gene, which affects the guidance of the growing abducens nerve axons to the lateral rectus.[20][21] In Duane retraction syndrome with associated malformation syndromes, the spalt-like transcription factor 4 (SALL4) gene on chromosome 20 has been implicated.[22] These syndromes include Okihiro syndrome, Duane-radial ray syndrome, and acro-renal-ocular syndrome.
Duane retraction syndrome is also associated with mutations in the homeobox A1 (HOXA1) gene, which affects the creation or survival of cranial nerve neurons.[21] Associated syndromes include Bosley-Salih-Alorainy syndrome and Athabascan brainstem dysgenesis syndrome.
Table 1. Etiological Categories and Mechanisms of Duane Retraction Syndrome
|
Category |
Specific Causes/Mechanisms |
Notes |
|
Congenital (most common) |
Developmental anomaly of the abducens nerve (cranial nerve VI) with aberrant innervation of the lateral rectus by the oculomotor nerve (cranial nerve III) |
Due to defective brainstem nuclear development during embryogenesis (fourth to eighth week of gestation) |
|
Genetic |
Mutations in CHN1, SALL4, HOXA1, and MAFB genes |
Some cases are autosomal dominant; they may be associated with syndromes such as Okihiro, Wildervanck, or Moebius |
|
Syndromic associations |
Okihiro syndrome (Duane-radial ray), Wildervanck syndrome (triad: Duane retraction syndrome, Klippel-Feil anomaly, and hearing loss), and Moebius syndrome |
Often have systemic malformations |
|
Acquired (rare) |
Birth trauma with forceps injury to the abducens nerve nucleus, brainstem infarct, head trauma, viral neuritis, and iatrogenic injury during neurosurgery |
May present later in life |
|
Intrauterine insults |
Teratogens (eg, thalidomide and misoprostol), maternal infections, gestational diabetes, and hypoxia |
Can affect cranial nerve development |
|
Mechanical restriction |
Fibrotic or tight lateral rectus muscle and congenital muscle anomalies |
Contributes to limited abduction and globe retraction |
Epidemiology
Duane retraction syndrome is found in 1% to 4% of the strabismic population.[23] Most cases are sporadic and unilateral; however, 10% are bilateral. Females are predominantly affected, and the left eye is more frequently affected than the right.[24] Higher estrogen levels in females during embryogenesis, together with a greater risk of inflammation, lead to a higher risk of venous thromboembolic events. Furthermore, right-to-left shunts cause embolic phenomena affecting the left carotid artery more often, causing dysregulated apoptosis along with misinnervation affecting the left eye.[25]
Although Duane retraction syndrome is a congenital anomaly, the average age at presentation in types I, II, and III is 13.5, 23.0, and 21.9 years, respectively.[24]
Global and Regional Prevalence
- Worldwide: Estimated at 1% of the general population and 1% to 4% of all cases of strabismus.
- United States: Similar rates to global estimates; prevalence is slightly higher in specialized pediatric ophthalmology clinics.
- India: Multiple tertiary center series suggest a prevalence of approximately 2% to 3% among patients with strabismus, possibly underreported in rural areas due to limited access to pediatric eye care.
- Asia (outside India): Comparable prevalence, although early detection is higher in countries with established school screening programs (eg, Japan and South Korea).[26]
Sex Distribution
- Female predominance is well-documented, with a female-to-male ratio ranging from 6:1 to 2.5:1 in most epidemiological studies.
- This sex bias remains unexplained, though some genetic linkage studies suggest possible sex-influenced penetrance patterns.[27]
Laterality
- Left eye involvement is more common, seen in approximately 60% to 72% of unilateral cases.
- Bilateral involvement occurs in about 10% to 20% of cases, with variable symmetry of clinical features.[28]
Age at Presentation
- Most patients present in early childhood, often before the age of 5 years, when abnormal head posture or limitation of eye movement is first noticed by parents or teachers.
- Presentation in adulthood is rare and typically occurs in mild forms that often go undetected.[29]
Type Distribution (Huber's Classification)
- Type I (limited abduction, normal or near-normal adduction): Approximately 70% of cases.
- Type II (limited adduction, normal or near-normal abduction): Approximately 7% to 10%.
- Type III (limitation of both abduction and adduction): Approximately 20% to 25%.[30]
Associated Conditions
- Isolated Duane retraction syndrome: Approximately 70% to 80% of cases.
- Syndromic Duane retraction syndrome: Approximately 20% to 30% of cases, often associated with Goldenhar syndrome, Klippel-Feil anomaly, or other congenital craniofacial abnormalities.
- Systemic anomalies: More frequent in bilateral cases (up to 50%).[31]
Ethnic and Genetic Factors
- No strong ethnic predilection, though certain familial clusters have been reported with CHN1 gene mutations, particularly in autosomal dominant familial cases.
- Sporadic cases are far more common than inherited cases.[32]
Table 2. Etiology of Duane Retraction Syndrome
|
Category |
Specific Causes/Association |
Notes |
|
Developmental anomaly |
Agenesis or hypoplasia of the abducens (cranial nerve VI) nucleus and nerve |
Most consistent finding in neuroimaging and pathology studies |
|
Aberrant innervation |
Miswiring of the oculomotor nerve (cranial nerve III) to the lateral rectus muscle |
Results in paradoxical co-contraction of the medial and lateral recti on adduction |
|
Genetic factors |
CHN1 gene mutations (autosomal dominant); SALL4 mutations (Duane-radial ray syndrome); HOXA1 mutations |
Familial cases <10%; most are sporadic |
|
Syndromic associations |
Goldenhar syndrome, Klippel-Feil anomaly, Okihiro syndrome, and Wildervanck syndrome |
Often associated with bilateral Duane retraction syndrome and systemic anomalies |
|
Intrauterine insults |
Vascular disruption in the brainstem during 4 to 8 weeks of gestation |
May explain sporadic cases without genetic mutations |
|
Environmental/teratogenic factors |
Rare reports of maternal thalidomide exposure, gestational diabetes, or prenatal hypoxia |
Evidence largely from case reports; causality not firmly established |
|
Mechanical restriction (secondary) |
Fibrosis or tightness of the lateral rectus muscle |
May be secondary to a primary innervation defect |
|
Other neural tube defects |
Brainstem malformations and Möbius sequence |
May coexist with Duane retraction syndrome in complex congenital cranial dysinnervation disorders |
Pathophysiology
An understanding of the pathogenesis of characteristic features of Duane retraction syndrome, such as globe retraction and shoots, is essential in the evaluation and management of the condition. Paradoxical innervation of the lateral rectus by the oculomotor nerve leads to co-contraction of the lateral rectus and medial rectus on attempted adduction, resulting in globe retraction and narrowing of the palpebral aperture.[2]
Another characteristic feature is shoots, which can be explained by mechanical factors and innervational anomalies. The mechanical cause of these vertical movements is due to a bridle effect or leash effect of the tight lateral rectus.[33] As the globe adducts and moves above or below the horizontal plane, there is sudden slippage of the tight lateral rectus, causing an upshoot or downshoot. In severe cases, this has been described to manifest even with the slightest of movement in adduction, known as the knife-edge effect. In contrast, innervational upshoots and downshoots are due to abnormal synergistic innervation between the medial rectus muscle and the superior, inferior rectus, or oblique muscles.[34]
Duane retraction syndrome is a congenital cranial dysinnervation disorder characterized by limitation of horizontal eye movements, globe retraction, and palpebral fissure narrowing on attempted adduction. This condition results from abnormal innervation of the lateral rectus muscle due to agenesis or hypoplasia of the abducens (sixth cranial) nerve nucleus and miswiring from the oculomotor (third cranial) nerve.
Neural Basis
- Primary defect:
- Absence or severe hypoplasia of the abducens nucleus and nerve in the brainstem.
- Documented in MRI and histopathology studies.
- Aberrant innervation:
- Lateral rectus receives anomalous innervation from branches of the oculomotor nerve meant for the medial rectus.
- On adduction, both medial and lateral recti contract simultaneously, causing globe retraction and palpebral fissure narrowing.
- Reduced or absent abduction:
- Due to a lack of normal abducens function.
- Variable adduction limitation:
- Depending on the degree of miswiring.[3]
Muscle and Mechanical Factors
- Lateral rectus changes:
- Fibrosis and stiffness from chronic anomalous innervation.
- Reduced elasticity limits passive movement.
- Co-contraction effect:
- On attempted adduction, both the lateral rectus and the medial rectus pull the globe backward.
- Globe retraction mechanism:
- Symmetrical co-contraction shortens the anteroposterior axis of the orbit, pulling the globe posteriorly.[35]
Classification Correlation (Huber's classification)
- Type I:
- Marked abduction limitation, normal or slightly limited adduction.
- Co-contraction and globe retraction mainly occur in adduction.
- Type II:
- Marked adduction limitation, normal or slightly limited abduction.
- Type III:
- Limitations of both abduction and adduction.
EMG studies show abnormal lateral rectus firing patterns in all types, consistent with oculomotor misinnervation.[36]
Associated Brainstem Anomalies
- Some cases have other cranial nerve dysinnervation or systemic malformations:
- Hearing loss
- Skeletal anomalies (Klippel-Feil syndrome)
- Orofacial malformations [37]
Developmental Timeline
- Insult likely occurs between the fourth and eighth week of gestation, during the critical period of cranial nerve nuclear development and axonal targeting.
- Possible etiologies:
- Genetic mutations (eg, CHN1, SALL4, and HOXA1)
- Intrauterine vascular disruption
- Teratogenic exposures [4]
Functional Consequences
- Binocular vision:
- May develop compensatory head turn to maintain fusion.
- Strabismus:
- Often esotropia in primary gaze (type I) or exotropia (type II).
- Amblyopia risk:
- Especially if ocular misalignment is significant and not corrected early.[6]
Histopathology
Gross Findings
Histopathological studies are typically performed on post-mortem specimens or during rare surgical biopsies in Duane retraction syndrome. Grossly, the extraocular muscles, especially the lateral rectus, may appear abnormally small, fibrotic, or displaced. The muscle belly can be replaced partly by fibrous tissue, and its insertion on the globe is typically normal but may be thinned.[3]
Nerve Supply Abnormalities
- The hallmark histopathological finding is aberrant innervation.
- In most cases of type I Duane retraction syndrome, the abducens nerve (cranial nerve VI) is absent or hypoplastic on the affected side.
- Instead, branches from the oculomotor nerve (cranial nerve III) aberrantly innervate the lateral rectus muscle, leading to co-contraction of the medial and lateral recti on adduction.
- This anomalous innervation has been confirmed in autopsy series and supported by neuroimaging–histology correlations.[4]
Muscle Histology
- Lateral rectus muscle:
- Reduced number of muscle fibers, replaced by dense collagenous tissue.
- Remaining fibers are often atrophic with variable fiber size.
- Some muscle fibers may show central nuclei, indicative of chronic myopathic change.
- Medial rectus muscle:
- Typically structurally normal but may show mild hypertrophy due to chronic co-contraction.[38]
Neuromuscular Junction Changes
- Histochemical studies reveal irregular and sparse neuromuscular junctions in the lateral rectus.
- Acetylcholinesterase staining shows reduced endplate density compared to normal extraocular muscle.[39]
Fibrosis and Collagen Deposition
- Masson's trichrome and Gomori stains demonstrate increased perimysial and endomysial fibrosis in the lateral rectus.
- This fibrosis contributes to the restricted abduction and the retraction of the globe observed clinically.[40]
Vascular Findings
- No consistent vascular pathology is noted, but occasional thickening of small vessel walls has been reported, possibly secondary to chronic inflammation or ischemia.[41]
Pathophysiological Correlation
- The histopathology supports the theory that Duane retraction syndrome is primarily a neurogenic disorder with secondary myopathic changes.
- Absence or maldevelopment of the abducens nerve during embryogenesis leads to misdirected oculomotor innervation and subsequent abnormal muscle usage, fibrosis, and restricted motility.[42]
Toxicokinetics
Toxicokinetics refers to how a substance is absorbed, distributed, metabolized, and excreted in the body, but in the context of Duane retraction syndrome, it is typically discussed from a translational research perspective when evaluating drug safety, neuroteratogenicity, and ocular tissue exposure during pregnancy or in early development, since Duane retraction syndrome is a congenital cranial dysinnervation disorder.
Relevance to Duane Retraction Syndrome
- Congenital nature: Duane retraction syndrome results from developmental anomalies of the abducens nerve (cranial nerve VI) and aberrant innervation from the oculomotor nerve. This defect occurs during early embryogenesis (3-8 weeks of gestation).
- Drug exposure in pregnancy: Certain neurotoxic or teratogenic agents taken during early pregnancy may interfere with neural crest migration, axonal pathfinding, or cranial nerve nucleus development, potentially contributing to syndromes such as Duane retraction syndrome.
- Ocular tissue penetration: Understanding the toxicokinetics of drugs that cross the placenta and accumulate in fetal ocular tissues is crucial for assessing risk.[43]
Absorption and Distribution
- Maternal-fetal transfer: Lipophilic drugs and those with low molecular weight (eg, isotretinoin and thalidomide) can cross the placenta efficiently.
- Target tissue exposure: Some agents preferentially accumulate in developing neural tissues, including cranial nerve nuclei and extraocular muscles, which may alter their development.[43]
Metabolism
- Immature fetal metabolism: The fetal liver and kidneys have reduced capacity for Phase I and Phase II metabolism, prolonging the half-life of many xenobiotics in fetal circulation.
- Drug biotransformation: Certain prodrugs or metabolites can be more neurotoxic than the parent compound, potentially affecting cranial nerve formation.[44]
Elimination
- Placental clearance: Dependent on maternal circulation; impaired placental function can prolong fetal drug exposure.
- Amniotic fluid recycling: Drugs excreted into amniotic fluid may be re-ingested by the fetus, extending exposure time.[45]
Examples of Potentially Relevant Agents
- Teratogenic drugs: Thalidomide, isotretinoin, misoprostol—known to cause cranial nerve defects or ocular anomalies.
- Maternal toxins: Alcohol, methylmercury, and certain pesticides may disrupt neurodevelopment.
- Iatrogenic exposures: High-dose corticosteroids or chemotherapeutic agents during pregnancy, although not directly proven to cause Duane retraction syndrome, can contribute to related neural developmental defects.[2]
Implications for Research and Clinical Care
- Risk assessment: Understanding toxicokinetics helps in predicting which agents might pose higher risks for Duane retraction syndrome–like anomalies.
- Drug safety labeling: Agents with proven placental transfer and neurodevelopmental toxicity should be flagged in pregnancy categories.
- Preventive counseling: Women of reproductive age, especially those with a history of congenital cranial nerve anomalies in offspring, should be counseled about drug exposures during pregnancy.[46]
Table 3. Toxicokinetic Parameters and Their Relevance to Duane Retraction Syndrome
|
Toxicokinetic Parameter |
Relevance to Duane Retraction Syndrome |
Potential Teratogenic Agents |
Mechanism of Risk |
Implication for Clinical Care |
|
Absorption |
Early pregnancy drug exposure can affect cranial nerve development during weeks 3-8 of gestation |
Isotretinoin, thalidomide, and alcohol |
Readily absorbed lipophilic drugs cross the placenta rapidly |
Avoid high-risk drugs in women planning pregnancy |
|
Distribution |
Placental transfer delivers the drug directly to fetal tissues, including neural crest derivatives and ocular tissues |
Methylmercury, lead, and certain pesticides |
Lipid solubility and protein-binding determine fetal exposure |
Monitor environmental and occupational exposures |
|
Metabolism |
Fetal metabolism is immature, prolonging exposure to active drug or toxic metabolites |
Ethanol (acetaldehyde metabolite) and chemotherapeutics |
Accumulation of neurotoxic metabolites |
Prefer agents with proven safety in pregnancy |
|
Elimination |
Reduced clearance in the fetus due to immature renal and hepatic systems; amniotic recirculation prolongs exposure |
Nonsteroidal anti-inflammatory drugs (in late pregnancy) and high-dose steroids |
Persistent exposure may impact neural tissue development |
Consider the elimination half-life in prescribing decisions |
|
Target tissue toxicity |
Direct insult to abducens nerve nuclei or misguidance of oculomotor axons during development |
Thalidomide, misoprostol, and cocaine |
Neuroteratogenesis via apoptosis and altered axon guidance |
Educate pregnant patients about teratogen avoidance |
|
Timing sensitivity |
Greatest risk during organogenesis (first trimester) |
Various, depending on exposure |
Structural cranial nerve maldevelopment |
Risk counseling during preconception and the first trimester |
History and Physical
Parents may seek medical attention for a child with Duane retraction syndrome due to abnormal head posture, pseudoptosis when the affected eye adducts, limitation of eye movement, and abnormal eye movements. Clinical features of Duane retraction syndrome include the following:
- Abduction limitation: A hallmark feature of Duane retraction syndrome is abduction limitation resulting from subnormal innervation of the lateral rectus muscle. The amount of abduction limitation is disproportionately larger than the amount of primary position deviation. This disproportion is most likely due to an underlying adduction deficit present in varying amounts in Duane retraction syndrome. This characteristic pattern helps distinguish it from sixth nerve palsy, where the abduction limitation and primary position deviation are in proportion to each other.[47]
- Abnormal head posture: Commonly observed in unilateral cases, the abnormal head posture aims to center, enlarge, and maintain binocular single vision and compensate for the duction deficit. The head turn will be toward the side of the affected eye in esotropic Duane retraction syndrome and away from the affected eye in exotropic Duane retraction syndrome.
- Globe retraction: A characteristic feature of Duane retraction syndrome, which is typically accompanied by a narrowing of the palpebral fissure on adduction. According to Jampolsky, in some patients, globe retraction is replaced by retraction escapes or equivalents. Examples include knife-edge lateral rectus/globe slip with upshoot or downshoot, deficient inward rotation in opposite gaze, and exotropic Duane retraction syndrome with the splits.
- Upshoots and downshoots: As aforementioned, shoots may be mechanical or innervational. Although mechanical shoots are characterized by a sudden, abrupt movement following a small vertical movement in adduction, innervational shoots are characterized by gradual elevation or depression of the eye as it adducts. Mechanical shoots typically do not have a primary gaze vertical tropia, whereas innervational shoots may be associated with vertical tropia in the primary position.[14]
- Alphabet patterns: Alphabet patterns are due to the co-contraction of the vertical and lateral recti when the patient is looking toward the affected field of gaze. V pattern is the most common, whereas A and no pattern are found less frequently.[48]
- Strabismus: Patients with Duane retraction syndrome may present with esotropia, orthotropia, or exotropia, as discussed in subsequent sections.
Patients with Duane retraction syndrome typically present in childhood, often noticed by parents or teachers due to abnormal eye movements or an abnormal head posture. Key historical points include the following:
- Onset: Congenital, typically recognized in early childhood; symptoms are non-progressive.
- Presenting complaints
- Limited horizontal eye movement (more often abduction deficit, sometimes adduction limitation).
- Face turn or abnormal head posture to compensate for ocular misalignment.
- Eye retraction or narrowing of the palpebral fissure when attempting adduction.
- Occasional upshoots or downshoots of the affected eye on adduction.
- Some may present with intermittent diplopia, although most adapt with suppression.
- Laterality: Unilateral in approximately 80% cases; the left eye is more commonly affected.
- Associated history: Possible history of birth anomalies, perinatal hypoxia, or systemic congenital syndromes (eg, Goldenhar syndrome and Klippel-Feil anomaly).
- Family history: Rare familial occurrence; autosomal dominant cases have been reported.[49]
Physical Examination
General examination:
- Evaluate for systemic dysmorphic features or other congenital anomalies that may be associated with syndromic Duane retraction syndrome.
Ocular examination:
- Visual acuity
- Usually normal; amblyopia may occur if there is significant deviation or anisometropia.
- Ocular alignment
- Esotropia in primary gaze (most common in type I).
- Orthotropia or exotropia may be observed in other subtypes.[50]
- Ocular motility
- Type I (abduction limitation, most common): Marked limitation of abduction, minimal limitation of adduction.
- Type II (adduction limitation): Marked limitation of adduction, minimal limitation of abduction.
- Type III: Limitation of both abduction and adduction.[51]
- Globe retraction
- Globe retraction and narrowing of the palpebral fissure on attempted adduction due to co-contraction of the medial and lateral rectus muscles.
- Upshoots/downshoots
- Sudden vertical deviation on adduction due to leash or slip phenomena.[35]
- Head posture
- Face toward the side of the affected eye to maintain binocular single vision.
- Binocular vision
- Many maintain binocular single vision in a compensatory head posture.[52]
- Refraction
- May reveal hyperopia, anisometropia, or astigmatism.
- Anterior segment and fundus
- Usually normal unless other associated ocular conditions are present.
Key Clinical Clues for Duane Retraction Syndrome Diagnosis
- Congenital onset with stable course.
- Limitation of horizontal movement (most often abduction).
- Globe retraction on adduction.
- Upshoot/downshoot on adduction in some cases.
- Compensatory head posture to avoid diplopia.[53]
Evaluation
Evaluation of a patient with Duane retraction syndrome is similar to any case of strabismus, including assessment of vision and cycloplegic refraction, inspection, motor evaluation, assessment of binocularity, and other supplemental tests.
A significant proportion (30%-70%) of patients with Duane retraction syndrome have hypermetropia or hypermetropic astigmatism of more than 1.5 D.[14] Some of these patients may also have an accommodative component; hence, cycloplegic refraction is essential for treatment planning.[54]
As patients adopt a compensatory head posture, strabismic amblyopia is not a common feature in patients with unilateral Duane retraction syndrome. In contrast, up to 25% of patients with bilateral Duane retraction syndrome have been found to have amblyopia.
Inspection and motor evaluation aid in determining the type of Duane retraction syndrome. Based on EMG, Huber classified the condition into 3 types:[55]
- Type 1: Marked limitation of abduction with minimally defective or normal adduction. This type is the most common, accounting for 70% to 80% of cases. EMG recordings showed paradoxical innervation of the lateral rectus on adduction and reduced impulses on attempted abduction, whereas the medial rectus had normal electrical activity.
- Type 2: Limitation of adduction with normal or slightly limited abduction. This type is the least common, accounting for 7% of the cases. EMG recordings showed innervation of the lateral rectus in both abduction and adduction, whereas the medial rectus was innervated normally.
- Type 3: Limitation or complete absence of adduction and abduction. EMG recordings showed simultaneous innervation of the lateral rectus and medial rectus in the primary position, adduction, and abduction.
Ahluwalia et al modified the Huber's classification by dividing each type based on the primary position deviation found. This classification is more useful for surgical planning and management.[56] Typically, patients with unilateral type I Duane retraction syndrome have esotropia more frequently than exotropia, whereas patients with type II Duane retraction syndrome have exotropia, and patients with type III Duane retraction syndrome have esotropia, exotropia, and orthotropia occurring in an equal proportion.[48] Overall, the most common primary position deviation is esotropia, followed by orthotropia.
Bilateral Duane retraction syndrome is less frequent than unilateral Duane retraction syndrome, with a reported incidence between 10% and 24%. Zanin et al classified bilateral Duane retraction syndrome into 3 types based on the works of Jampolski.
- Bilateral Duane retraction syndrome with fusion: Typically bilateral type I with a small angle of deviation or orthotropia with minimal eye movements, often without retraction or its equivalents.
- Bilateral Duane retraction syndrome without fusion: Characterized by prominent eso- or exodeviation.
- Bilateral Duane retraction syndrome with an alphabet pattern.[33]
As aforementioned, Duane retraction syndrome is associated with many ocular and systemic anomalies. Hence, a thorough multi-disciplinary evaluation is necessary.
Clinical Assessment
Obtaining a detailed history and performing a thorough examination are the cornerstones of diagnosis.
- History:
- Age at onset (typically congenital; often noted in early childhood).
- Family history of strabismus or congenital ocular motility disorders.
- Presence of abnormal head posture (face turn to maintain binocular single vision).
- Intermittent diplopia (rare).
- History of systemic anomalies (especially in syndromic Duane retraction syndrome: Goldenhar, Wildervanck, and Holt-Oram).
- Ocular examination:
- Primary position deviation measurement using the prism cover test.
- Ocular motility testing: Limitation of abduction, adduction, or both.
- Globe retraction on adduction and palpebral fissure narrowing (key sign).
- Upshoot/downshoot in adduction (due to leash effect or co-contraction).
- Evaluation of head posture for compensatory face turn.
- Presence of binocular single vision in various gaze positions.
- Binocular function testing: Worth four-dot test and Bagolini lenses.
- Cycloplegic refraction: To rule out accommodative elements.[3]
Ancillary Ophthalmic Tests
- Hess/Lees screen test: Maps ocular motility deficits and confirms the co-contraction pattern.
- Synoptophore: Quantifies ocular alignment and fusional capacity.
- Forced duction test: Performed to differentiate mechanical restriction from innervational limitation (typically shows mechanical restriction in adduction in Duane retraction syndrome).
- Forced generation test: Can show reduced abduction force in the affected eye.
- Saccadic velocity recordings: Show reduced abduction saccadic velocities.[4]
Radiological Imaging
- High-resolution MRI of the brainstem and orbits (especially CISS or FIESTA sequences):
- Absence or hypoplasia of the abducens nerve (cranial nerve VI) at the brainstem exit zone (confirmatory finding).
- Evaluation for anomalous extraocular muscle insertions or fibrosis.
- Assessment of coexisting cranial nerve abnormalities.
- CT scan of orbits: Less preferred, but may help rule out bony anomalies in trauma-related cases.[57]
Electrophysiological Tests
- EMG of extraocular muscles:
- Demonstrates simultaneous innervation of medial and lateral rectus on adduction: Hallmark of Duane retraction syndrome.
Systemic Evaluation
Given that up to 30% of Duane retraction syndrome cases are associated with systemic anomalies, a systemic work-up is often indicated:
- Audiology: For hearing defects (Wildervanck syndrome).
- Cardiac evaluation: Electrocardiogram/echocardiogram (Holt-Oram syndrome).
- Cervical spine x-ray: For vertebral anomalies.
- Renal ultrasound: For congenital renal anomalies.[58]
Diagnostic Criteria
Based on Huber's classification (types 1-3), diagnosis is confirmed when:
- Limitation of abduction (type 1), limitation of adduction (type 2), or both (type 3) is present.
- Globe retraction with fissure narrowing occurs on adduction.
- Evidence of co-contraction on EMG.
- MRI confirms abducens nerve abnormality.[59]
Guidelines Reference
- American Association for Pediatric Ophthalmology and Strabismus recommends:
- Imaging is needed only if atypical features, unclear diagnosis, or systemic syndromic associations are suspected.
- Conservative management is recommended unless there is a significant deviation in primary gaze or abnormal head posture.
- United Kingdom Royal College of Ophthalmologists:
- Early detection in children via orthoptic screening.
- Surgical planning should only be performed after careful ocular motility analysis and binocular assessment.[60]
Table 4. Table Clinical Tests and Assessments in Duane Retraction Syndrome
|
Test/Assessment |
Purpose |
Typical Findings in Duane Retraction Syndrome |
|
Detailed history |
Identify onset, family history, systemic associations |
Congenital onset, abnormal head posture, and possible syndromic clues |
|
Ocular motility examination |
Assess the limitations of abduction/adduction, globe retraction, and palpebral fissure changes |
Limited abduction (type 1), adduction (type 2), or both (type 3) |
|
Prism cover test |
Measure primary position deviation |
Esotropia or exotropia in primary gaze |
|
Binocular vision tests (Worth four-dot, Bagolini lenses) |
Assess fusion and suppression |
Fusion in some gazes and suppression in others |
|
Cycloplegic refraction |
Rule out accommodative strabismus |
Refractive errors |
|
Hess/Lees screen test |
Map ocular motility deficits and co-contraction |
Underaction in abduction and an abnormal co-contraction pattern |
|
Synoptophore assessment |
Quantify ocular alignment and fusion range |
Reduced fusion amplitudes in eccentric gazes |
|
Forced duction test |
Differentiate mechanical restriction from innervational limitation |
Restriction in adduction |
|
Forced generation test |
Assess abduction force |
Reduced abduction force |
|
Saccadic velocity recording |
Quantify abduction/adduction velocities |
Reduced abduction velocity |
|
High-resolution MRI (CISS/FIESTA sequences) |
Confirm absence/hypoplasia of the abducens nerve |
Abducens nerve absent or hypoplastic |
|
CT scan of orbits |
Assess the bony orbit if trauma is suspected |
Normal in congenital Duane retraction syndrome |
|
Electromyography of extraocular muscles |
Demonstrate co-contraction of the lateral rectus and medial rectus |
Simultaneous lateral rectus and medial rectus activity on adduction |
|
Audiology assessment |
Detect hearing loss (syndromic association) |
Sensorineural hearing loss in some cases |
|
Cardiac evaluation (ECG/Echo) |
Rule out associated cardiac anomalies |
Structural defects in Holt-Oram syndrome |
|
Cervical spine x-ray |
Identify vertebral anomalies |
Cervical vertebral fusion |
|
Renal ultrasound |
Detect congenital renal anomalies |
Renal agenesis or hypoplasia |
Abbreviations: MRI, magnetic resonance imaging; CISS/FIESTA, Constructive Interference in Steady State/Fast Imaging Employing Steady-State Acquisition; CT, computed tomography; ECG/Echo, electrocardiogram/echocardiogram.
Treatment / Management
Non-surgical management of Duane retraction syndrome consists of spectacles or contact lenses for refractive error, prism glasses to improve the compensatory head position, and treatment of amblyopia with standard therapy. The efficacy of botulinum toxin has also been investigated. In most patients, the results of the injection have been relatively short-term.[61](B2)
Indications for surgical management of Duane retraction syndrome include the following:
- Significant ocular deviation in the primary position.
- Marked anomalous head posture.
- Disfiguring retraction of the globe on attempted adduction.
- Upshoots and downshoots of the globe in adduction.
Patients should be informed that no treatment or surgical procedure can restore normal ocular movements in all gaze positions, as the underlying abnormality of paradoxical innervation cannot be corrected. Additionally, before operating on any case of Duane retraction syndrome, a forced duction test is necessary to rule out medial rectus or lateral rectus contracture in the affected eye.[62]
Surgical options for esotropic Duane retraction syndrome include the following:
- Medial rectus recession: In cases with a tight medial rectus and minimal co-contraction, medial rectus recession is generally indicated. Unilateral medial rectus recession of the Duane retraction syndrome eye can correct up to 20 prism diopters (PD) of esotropia. Medial rectus recession of the Duane retraction syndrome eye should be limited to less than 6 mm, as larger medial rectus recessions increase the likelihood of an iatrogenic adduction limitation, which compromises the field of binocular single vision by causing an exotropia in the contralateral gaze.[63] Excessive recession may also result in impaired convergence.
- Bilateral medial rectus recession: This approach is considered in certain situations.[63] First, in cases of esotropia with a primary position deviation of more than 20 PD, a single medial rectus recession of less than 6 mm is unlikely to be sufficient. Second, in cases with severe globe retraction, the lateral rectus may have to be recessed along with the medial rectus; conversely, this may increase the esotropia. Hence, recessing the contralateral medial rectus in such cases may also help correct the total esotropia. Finally, bilateral medial rectus recession may help prevent contracture of the medial rectus on the affected side by creating fixation duress in the contralateral eye. After surgery, the medial rectus of the fixing eye receives increased innervation to maintain fixation, which reduces innervation to its lateral rectus. This reciprocal adjustment decreases the innervational tone of the medial rectus in the affected eye, thereby lowering the risk of contracture.
- Medial rectus recession with lateral rectus recession: In cases of esotropic Duane retraction syndrome with moderate-to-severe co-contraction, medial rectus recession may be combined with lateral rectus recession to reduce the anomalous innervation of the lateral rectus during adduction.[64] (B3)
- Vertical rectus transposition: This procedure aims to create active abduction vector forces by creating a tone for the lateral rectus through the transposed muscle.[65] Vertical rectus transposition is indicated in cases of esotropic Duane retraction syndrome with minimal co-contraction. However, the transposition of both vertical muscles has several limitations. New vertical deviations have been described in 6% to 30% of patients after vertical rectus transposition, the most common being hypotropia.[66] Co-contraction may worsen after vertical rectus transposition. Nearly 50% of patients require a secondary procedure involving recession of the ipsilateral medial rectus to achieve acceptable eye alignment and head position. Additionally, when vertical rectus transposition needs to be combined with medial rectus recession, the risk of anterior ischemic syndrome increases.[67] (B2)
- Superior rectus transposition: This procedure eliminates the risk of iatrogenic vertical limitation and anterior segment ischemia. This procedure is recommended in esotropia of less than 15 PD with minimal co-contraction. In esotropias of 15 to 25 PD, superior rectus transposition combined with unilateral or bilateral medial rectus recession is recommended.[14]
- Recess-resect procedures: Lateral rectus resection of the concerned eye is typically not advised, as globe retraction may be worsened. However, combined medial rectus recession and lateral rectus resection may be considered in cases of esotropic Duane retraction syndrome of less than 25 PD, with normal adduction and severely limited abduction. Globe retraction and shoots should also be absent.
For exotropic Duane retraction syndrome, lateral rectus recession is advocated when there is normal lateral rectus activity in abduction. Unilateral rectus recession corrects up to 20 PD of exotropia. For exotropia of more than 20 PD, bilateral rectus recession may be considered. Recessing the lateral rectus may worsen abduction limitation if present; therefore, if bilateral LR recession is required, the larger recession should be performed in the contralateral eye.[63]
Conversely, if the anomalous activity of the lateral rectus is present, periosteal fixation of the lateral rectus may be considered. In this procedure, the insertion of the lateral rectus is moved from the globe to the lateral orbital wall, eliminating the effect of paradoxical innervation and co-contraction in adduction. The resultant absence of abduction is correctable with transposition procedures, which may increase the risk of anterior segment ischemia. As a relatively new procedure, there are limited literature data on its efficacy.[62]
Surgical options to correct the shoots and globe retraction include the following:
- Y-split of the lateral rectus: This procedure has been advocated to treat mechanical shoots. In this procedure, the lateral rectus is divided into 2 horizontal limbs as far posteriorly as possible and inserted 20 mm apart. Thus, when the eye elevates in adduction, the lower half of the lateral rectus contracts to prevent the globe from slipping upwards.[68]
- Periosteal fixation of the lateral rectus.[62]
- Vertical rectus muscle recession or inferior oblique myectomy: This procedure has been advocated to treat innervational shoots.[69][70][69] (B3)
General Principles
Duane retraction syndrome is a congenital, non-progressive ocular motility disorder, and its management depends on the severity of symptoms, presence of compensatory head posture, degree of ocular misalignment, globe retraction, and psychosocial impact. Many patients require no intervention apart from observation, whereas others may benefit from surgical correction to improve head posture, alignment, and cosmesis.
Goals of Management
- Achieve or maintain binocular single vision in primary gaze
- Correct or reduce abnormal head posture
- Minimize ocular misalignment in the primary position
- Improve cosmesis and patient comfort
- Prevent amblyopia in pediatric patients [71]
Non-Surgical Management
- Observation
- Indicated for patients with minimal deviation, acceptable head posture (<15°), and no significant cosmetic concerns.
- Regular follow-up to monitor for progression or development of amblyopia.
- Amblyopia therapy
- Patching or penalization in children with reduced vision in one eye.
- Early detection and treatment are essential to optimize visual potential.
- Optical correction
- Spectacles for refractive errors (hyperopia, myopia, and astigmatism).
- Prisms are used in selected cases to reduce abnormal head posture in mild deviations.[4]
Surgical Management
Surgery is considered in patients with:
- Significant abnormal head posture (>15°)
- Large ocular deviation in the primary position
- Severe globe retraction or narrowing of the palpebral fissure on adduction
- Severe upshoots or downshoots
- Psychosocial or cosmetic concerns [38]
Common Surgical Procedures
- Horizontal muscle recession
- Unilateral medial rectus recession (for type I with limited abduction and esotropia).
- Bilateral medial rectus recessions for large deviations.
- Lateral rectus recession in type III with large exodeviation.
- Vertical rectus transposition
- Full-tendon or partial-tendon vertical rectus transposition for severe abduction limitation, often combined with medial rectus recession.
- Y-splitting of the lateral rectus
- Reduces upshoots or downshoots caused by the leash effect.
- Combined procedures
- Address multiple components—horizontal deviation, globe retraction, and vertical overshoots—in a single sitting if feasible.[36]
Special Considerations
- Avoid over-recession of the horizontal rectus muscles to prevent inducing secondary limitations.
- Globe retraction is not eliminated by surgery but can be reduced.
- Pediatric patients require amblyopia therapy in parallel with surgical intervention.[72]
Postoperative Care
- Monitor ocular motility, alignment, and head posture.
- Assess for residual or consecutive deviations and treat accordingly.
- Continue amblyopia management in children as needed.[10]
Guideline References
- American Academy of Ophthalmology Preferred Practice Pattern: Surgery should be individualized, aiming to optimize head posture and binocular vision while minimizing surgical risk.
- Indian Strabismus Society Guidelines: Observation for mild cases, surgery for significant deviations, and amblyopia management as a priority in children.[73]
Differential Diagnosis
Differential diagnoses of Duane retraction syndrome include disorders that cause or may appear to cause abduction deficits, such as sixth nerve palsy, infantile esotropia, Mobius syndrome, and congenital ocular motor apraxia. Most of these conditions can be differentiated from Duane retraction syndrome based on associated clinical features. For example, in infantile esotropia, abduction saccades and cross fixation are typically present; patients with Mobius syndrome may have associated feeding and speech difficulties; in congenital ocular motor apraxia, there is an inability to generate horizontal saccades. However, there is full retention of eye movements, and gradual improvement with time occurs.
Esotropic Duane retraction syndrome and congenital sixth nerve palsy may be differentiated based on the following clues:
- Globe retraction in adduction is present in cases of Duane retraction syndrome, whereas it is absent in sixth nerve palsy.
- The esotropic angle is typically smaller in patients with Duane retraction syndrome compared to patients with sixth nerve palsy who have the same limitation of abduction.
- The amount of abduction deficit varies in upgaze and downgaze in patients with Duane retraction syndrome, whereas it is similar in patients with sixth nerve palsy.[47]
Duane et al described certain mechanical and neurogenic conditions that lead to globe retraction in adduction and limitation of abduction but are etiologically distinct from classical Duane retraction syndrome. These conditions are collectively termed acquired retraction syndrome.[74] Mechanical conditions include fracture of the medial orbital wall, orbital inflammation, thyroid myopathy, and bony orbital metastasis. Neurogenic conditions include head injury, intracranial metastases, and brainstem tumors such as glioma. These conditions can be differentiated from true Duane retraction syndrome based on the history of systemic illness, diplopia, trauma, or surgery.[14]
Table 5. Differential Diagnosis of Duane Retraction Syndrome
|
Conditions |
Distinguishing Features from Duane Retraction Syndrome |
|
Sixth nerve palsy |
Abrupt onset, often acquired; limited abduction without globe retraction or palpebral fissure narrowing on adduction, often with diplopia. |
|
Third nerve palsy |
Ptosis, limitation of most ocular movements, possible pupillary involvement, and absent globe retraction. |
|
Brown syndrome |
Limitation of elevation in adduction; normal abduction; mechanical restriction due to a superior oblique tendon sheath abnormality. |
|
Congenital fibrosis of extraocular muscles |
Severe congenital ophthalmoplegia with ptosis; marked limitation in multiple gaze directions; often bilateral with systemic associations. |
|
Mobius syndrome |
Congenital bilateral facial and abducens nerve palsy; facial weakness; limb anomalies; absence of globe retraction. |
|
Thyroid eye disease |
Restrictive myopathy with diplopia, proptosis, lid retraction, absence of globe retraction, often adult onset. |
|
Myasthenia gravis |
Variable and fatigable ophthalmoplegia; ptosis; no globe retraction; positive edrophonium or antibody test. |
|
Orbital fracture with entrapment |
Trauma history; diplopia in certain gaze positions; imaging shows muscle entrapment; no congenital features. |
|
Internuclear ophthalmoplegia |
Failure of adduction with abducting nystagmus of the contralateral eye; lesion in the medial longitudinal fasciculus; typically acquired. |
|
Chronic progressive external ophthalmoplegia |
Slowly progressive bilateral ophthalmoplegia; ptosis; mitochondrial disorders; no globe retraction. |
|
Endophthalmitis with restrictive strabismus |
Pain, redness, reduced vision, inflammatory signs; not congenital. |
|
Superior oblique palsy |
Head tilt compensation; hypertropia; overaction of the inferior oblique; normal globe movement on adduction. |
|
Oculomotor nerve misinnervation syndromes (other than Duane retraction syndrome) |
Variable patterns of abnormal co-contraction without classical Duane retraction syndrome features. |
|
Multiple cranial nerve palsies (eg, cavernous sinus lesions) |
Associated sensory loss; ptosis; pupillary involvement; systemic or neurological signs. |
|
Orbital tumors (restrictive) |
Gradual onset; proptosis; imaging evidence of mass lesion; no congenital misinnervation pattern. |
|
Congenital ptosis with pseudostrabismus |
Lid droop mimicking eye movement limitation; full motility on testing. |
|
Marcus Gunn jaw-winking syndrome |
Lid elevation with jaw movement; normal ocular motility. |
|
Congenital esotropia |
Large-angle esotropia present early in life; full abduction present; no globe retraction. |
|
Convergence spasm |
Episodic convergence with miosis and accommodation; psychogenic or organic cause; normal motility between episodes. |
|
Restrictive strabismus from orbital inflammation (eg, myositis) |
Pain, acute onset; imaging shows enlarged extraocular muscles; no congenital features. |
Pertinent Studies and Ongoing Trials
Key Study Themes and Findings
- Neuroanatomy and Imaging
- High-resolution MRI (CISS/FIESTA) series demonstrated absence or hypoplasia of the abducens nerve and variable brainstem anomalies in Duane retraction syndrome, validating Duane retraction syndrome as a congenital cranial dysinnervation disorder.
- Diffusion tensor imaging further revealed aberrant white-matter tracts, supporting miswiring of the lateral rectus by cranial nerve III.[75]
- Electrophysiology
- EMG studies (classical Huber work and successors) confirmed co-contraction of medial and lateral rectus on adduction, underpinning globe retraction and the Huber Types I through III clinical schema.
- Genetics and syndromic associations
- Familial or series studies reported mutations in CHN1, SALL4 (Duane radial ray), HOXA1, and MAFB, linking Duane retraction syndrome to congenital cranial dysinnervation disorders and explaining bilateral or syndromic cases.[76]
- Epidemiology or natural history
- Clinic-based cohorts: Female predominance, left-eye bias, 10%-20% bilateral; most maintain binocular single vision with compensatory head posture.[77]
- Surgical outcomes
- Medial rectus recession (unilateral or bilateral) improves esotropia and head turn in type I.
- Vertical rectus transposition (full or partial) ± Foster augmentation improves abduction and primary-position alignment in severe cases.
- Y-splitting of the lateral rectus reduces upshoots or downshoots; lateral rectus recession helps in exotropic or type III patterns.
- Combined procedures show best results when tailored to primary deviation + pattern (retraction or overshoots) + head posture; over-recession risks consecutive limitations.[56]
- Amblyopia or quality of life
- Pediatric series underline low-to-moderate amblyopia risk (higher in significant primary deviation), with improved quality of life after alignment or head-turn surgery.[78]
Findings from Ongoing or Recent Trial Activity
Due to the rarity of Duane retraction syndrome, formal randomized controlled trials remain limited. However, current registry entries and prospective studies commonly explore the following areas.
- Comparative effectiveness: Partial versus full vertical rectus transposition (with or without augmentation) versus large medial rectus recession for severe abduction deficit.
- Adjuncts: Botulinum toxin to the medial rectus as an adjunct to reduce co-contraction in selected patterns.
- Imaging biomarkers: Prospective MRI-based classification correlating anatomy with surgical choice or outcomes.
- Genetic or phenotype registries: Multi-center congenital cranial dysinnervation disorder databases collecting genotype-phenotype patterns with surgical results.
- Patient-reported outcomes: Standardized questionnaires assessing head posture and diplopia, administered before and after surgery.[79]
Take-Home Message
- Anatomical evidence from MRI and EMG studies supports the understanding of Duane retraction syndrome as a misinnervation disorder with secondary muscle fibrosis. Surgical planning should focus on rebalancing extraocular forces rather than attempting to strengthen abduction.
- The best available evidence supports individualized combinations, such as medial rectus recession, vertical rectus transposition with or without augmentation, and Y-split, aimed at primary-gaze alignment and head-turn reduction, not normal motility.
Treatment Planning
Treatment planning for Duane retraction syndrome is highly individualized, focusing on alleviating abnormal head posture, reducing binocular diplopia, and improving ocular alignment rather than restoring normal ocular motility, which is generally not possible due to congenital innervation defects. The approach requires careful assessment of subtype (type I, II, and III), degree of globe retraction, presence of upshoot or downshoot, binocular vision potential, and associated anomalies.[80]
Comprehensive Clinical Assessment
- History: Onset, progression, compensatory head posture, diplopia, systemic associations.
- Examination: Detailed motility assessment, prism cover testing, head posture measurement, globe retraction grading, and forced duction testing.
- Imaging: MRI or CT in atypical cases to rule out structural orbital abnormalities or associated cranial dysinnervation syndromes.[81]
Non-Surgical Management
- Observation: For mild cases without significant head posture or diplopia.
- Optical corrections: Refractive error correction, prisms for small deviations.
- Orthoptic exercises: Limited role, mainly for binocular stability.
- Amblyopia therapy: Especially in pediatric cases with unilateral involvement.[82]
Indications for Surgery
Surgical intervention is symptom-driven and aims to improve function and cosmesis:
- Abnormal head posture >15°.
- Significant primary position deviation.
- Disfiguring globe retraction.
- Large upshoots or downshoots causing cosmetic or functional problems.
- Associated vertical deviations.[2]
Surgical Options
- Horizontal rectus recession:
- Lateral rectus recession: For esotropia in primary gaze (type I).
- Medial rectus recession: For exotropia (type II) or combined recession with lateral rectus in severe cases.
- Y-Splitting of lateral rectus: Reduces upshoot or downshoot caused by leash effect.
- Vertical rectus transposition: For severe abduction limitation; may be augmented with Foster sutures to improve the field of single binocular vision.
- Globe retraction management: Large recession of the involved muscle with or without adjustable sutures.
- Combined Procedures: Often required in complex or asymmetric cases.[83]
Postoperative Considerations
- Residual limitations in abduction or adduction should be anticipated and explained preoperatively.
- Risk of induced vertical deviations or new motility limitations.
- Some patients may require secondary surgery for optimal alignment.[84]
Interprofessional Coordination
- Ophthalmologists and strabismologists: Primary planning and execution of surgery.
- Orthoptists: Pre- and postoperative alignment assessment and therapy.
- Neurologists: When associated cranial dysinnervation syndromes are suspected.
- Genetic counselors: In familial or syndromic cases.
- Pediatricians: For systemic association screening.
Table 5. Management Steps in Duane Retraction Syndrome
|
Step |
Details |
Key Considerations |
|
Clinical assessment |
Detailed motility testing, prism cover test, abnormal head posture measurement, and forced duction testing. |
Classify into Duane retraction syndrome Type I, II, III; assess globe retraction and up/downshoots; check binocular vision potential. |
|
Non-surgical management |
Observation for mild cases; refractive correction; prisms; amblyopia therapy. |
Reserved for patients without significant head posture, diplopia, or large deviations. |
|
Surgical indications |
Abnormal head posture >15°, large primary gaze deviation, cosmetically significant globe retraction, severe up/downshoots. |
Surgery is functional and cosmetic, not curative for a motility defect. |
|
Surgical options |
|
Consider adjustable sutures; avoid overcorrection; anticipate residual motility limits. |
|
Postoperative care |
Monitor for vertical deviations, diplopia, and residual misalignment. |
May require secondary surgery; postoperative orthoptic assessment. |
|
Interprofessional collaboration |
Ophthalmologists, orthoptists, neurologists, genetic counselors, pediatricians. |
Ensures systemic evaluation, genetic counseling, and optimal functional rehabilitation. |
Toxicity and Adverse Effect Management
Although Duane retraction syndrome is primarily a congenital ocular motility disorder and not a pharmacologic or radiation-induced condition, toxicity in this context refers to the potential adverse outcomes from medical, surgical, or rehabilitative interventions aimed at managing Duane retraction syndrome. These effects can arise from the surgical correction of ocular misalignment, the use of botulinum toxin, or prolonged optical interventions. Effective management requires early recognition, prompt intervention, and preventive strategies.
Surgical Intervention–Related Adverse Effects
- Overcorrection or undercorrection of deviation may result in diplopia or cosmetic dissatisfaction.
- Induced vertical deviations following horizontal muscle surgery due to altered force vectors.
- Anterior segment ischemia (rare) after multiple rectus muscle surgeries, especially in older patients.
- Scarring and adhesions may lead to restricted motility and reduced surgical effect.
- Iatrogenic ptosis or lid malposition occurs if the levator or periocular tissues are inadvertently affected.[8]
Management:
- Careful preoperative planning with forced duction testing.
- Staging surgeries in high-risk cases to minimize ischemia risk.
- Postoperative steroid drops or ointments to control inflammation.
- Early physiotherapy and ocular motility exercises to maintain the range of movement.[2]
Botulinum Toxin–Related Adverse Effects
- Ptosis from toxin diffusion into the levator palpebrae.
- Vertical deviation or unwanted weakening of non-target muscles.
- Transient diplopia during the period of muscle weakening.
Management:
- Use EMG-guided injection for accuracy.
- Employ minimal effective dose to reduce diffusion.
- Reassure patients that most side effects resolve within weeks.[85]
Optical and Orthoptic Management–Related Adverse Effects
- Asthenopia from prolonged prism use in nonresponsive patients.
- Induced visual confusion in poorly adapted binocular systems.
Management:
- Gradual prism adaptation trials before prescribing permanent correction.
- Regular follow-up to reassess ocular alignment and symptoms.[86]
General Postoperative or Intervention Risks
- Infections (eg, conjunctivitis and rare cases of orbital cellulitis) require strict asepsis during surgery.
- Allergic reactions to suture materials or medications.
Management:
- Prophylactic topical antibiotics post-surgery.
- Switch to hypoallergenic materials if a previous reaction is noted.[87]
Key Takeaway
Adverse effect management in Duane retraction syndrome hinges on anticipation, prevention, and early correction. Individualized surgical planning, minimal intervention when possible, and interdisciplinary follow-up (ophthalmologist, orthoptist, and pediatrician) significantly reduce complication rates and improve functional as well as cosmetic outcomes.
Staging
Huber's Classification (1974)
Huber's classification is the most widely accepted system, based on electromyographic (EMG) findings of the lateral rectus muscle.[88]
Table 6. Types of Duane Retraction Syndrome
|
Type |
Findings |
EMG Pattern |
Clinical Features |
|
Type I |
Marked limitation or absence of abduction; variable adduction |
Lateral rectus shows no or minimal activity in abduction and paradoxical activity in adduction |
Narrow palpebral fissure on adduction, globe retraction, and upshoot or downshoot possible |
|
Type II |
Marked limitation or absence of adduction; abduction is normal or slightly limited |
Lateral rectus shows paradoxical activity in abduction and minimal or absent activity in adduction |
Palpebral fissure widening on abduction |
|
Type III |
Limitations of both abduction and adduction |
Lateral rectus shows co-contraction during attempted abduction and adduction |
Severe globe retraction and fissure narrowing in both directions |
Khurana's Description
In Khurana's Ophthalmology textbook, the classification is described in clinical rather than EMG terms, emphasizing ocular motility patterns and lid fissure changes:
- Type I: Abduction limitation; adduction normal or mildly restricted; globe retraction on adduction.
- Type II: Adduction limitation; abduction relatively preserved; globe retraction on attempted adduction.
- Type III: Limitation in both adduction and abduction; pronounced globe retraction on either gaze.
Anatomical/Etiological Subclassification
Anatomical or etiological subclassification based on imaging and surgical exploration includes the following:
- Innervational anomaly type (miswiring of cranial nerves III and VI)
- Fibrotic muscle type (lateral rectus fibrosis)
- Mixed type [57]
Associated Staging Considerations
Although Duane retraction syndrome is not staged in the classical sense as tumors are, disease severity can be graded clinically for management decisions:
- Mild: Minimal movement limitation; small head turn; little cosmetic concern.
- Moderate: Clear limitation; compensatory head posture; functional diplopia in extremes.
- Severe: Marked bilateral restriction; large head turn; significant upshoot or downshoot; severe retraction.
Laterality and Subtypes
- Unilateral Duane retraction syndrome: Most common (Type I in left eye predominates).
- Bilateral Duane retraction syndrome: Often symmetric, more common in syndromic cases (eg, Okihiro syndrome).
Table 7. Comparative Overview of Duane Retraction Syndrome Classifications
|
System |
Type |
Key Ocular Motility Findings |
Electromyography Findings |
Other Notable Features |
|
Huber's Classification (1974) |
Type I |
Marked limitation of abduction; adduction is normal or mildly limited |
Minimal/absent lateral rectus activity in abduction; paradoxical lateral rectus activity in adduction |
Narrow palpebral fissure and globe retraction on adduction; upshoot/downshoot possible |
|
Type II |
Marked limitation of adduction; abduction is normal or slightly limited |
Paradoxical lateral rectus activity in abduction; minimal/absent activity in adduction |
Widening of the palpebral fissure on abduction |
|
|
Type III |
Limitations of both abduction and adduction |
Lateral rectus co-contraction on attempted abduction and adduction |
Severe globe retraction and fissure narrowing in both gazes |
|
|
Khurana's Clinical Description |
Type I |
Abduction limitation; adduction near normal |
Not EMG-based |
Globe retraction and fissure narrowing on adduction |
|
Type II |
Adduction limitation; abduction near normal |
Not EMG-based |
Fissure widening on abduction |
|
|
Type III |
Limitation in both abduction and adduction |
Not EMG-based |
Marked globe retraction in both directions |
|
|
Simplified Clinical/Functional Grading |
Mild |
Minimal movement limitation; small compensatory head posture |
— |
Minimal cosmetic concern |
|
Moderate |
Clear limitation with functional head turn; occasional diplopia |
— |
Visible globe retraction |
|
|
Severe |
Marked restriction in both directions; large head turn; frequent upshoot/downshoot |
— |
Major functional and cosmetic impact |
Prognosis
Isolated Duane retraction syndrome leads to an excellent long-term prognosis for vision if managed appropriately. With a motley of non-surgical and surgical options available, features of Duane retraction syndrome, such as abnormal head posture, globe retraction, shoots, and misalignment of the visual axes, can be improved. Advances in surgery, such as transposition of vertical muscles, also aid in improving ductions in patients with Duane retraction syndrome.
The prognosis of Duane retraction syndrome is generally favorable in terms of visual potential, as most patients have good visual acuity in at least 1 eye and adapt well with compensatory head posture. However, outcomes depend on type, severity, presence of amblyopia, ocular alignment, and associated systemic or ocular anomalies.[62]
Visual Prognosis
- Good prognosis if amblyopia is detected early and appropriately managed with occlusion or refractive correction.
- Most patients maintain stable binocular vision and functional fusion.
- Poor prognosis may occur if there is untreated amblyopia, significant globe retraction, or severe misalignment.[2]
Motor Outcomes
- Surgical intervention can improve abnormal head posture, ocular alignment, and globe retraction but cannot restore normal ocular motility.
- Some residual limitation of movement is almost always present postoperatively.[3]
Long-Term Stability
- Duane retraction syndrome is a non-progressive congenital condition; motility deficits remain static throughout life.
- Surgical results are typically stable, though small degrees of drift may occur.[4]
Functional Prognosis
- With proper management, patients generally have normal daily functioning and minimal cosmetic concerns.
- Early intervention in children prevents secondary complications such as facial asymmetry due to chronic abnormal head turn.[6]
Prognosis in Associated Syndromic Cases
- If associated with systemic malformations (eg, Goldenhar, Wildervanck, and Okihiro syndromes), prognosis depends on the severity of the systemic disease.
- Visual prognosis may be guarded if associated ocular anomalies (optic nerve hypoplasia and coloboma) are present.[89]
Table 8. Key Prognostic Factors
|
Prognostic Factor |
Good Outcome Indicators |
Poor Outcome Indicators |
|
Type of Duane retraction syndrome |
Type I with minimal misalignment |
Severe misalignment or type III |
|
Amblyopia |
Early detection and treatment |
Untreated amblyopia |
|
Head posture |
Mild, non-progressive |
Severe with facial asymmetry |
|
Associated anomalies |
None or mild |
Severe ocular or systemic anomalies |
|
Surgical response |
Stable alignment |
Recurrence or residual large deviations |
Complications
- Undercorrection and residual esotropia: Residual esotropia may result if an inadequate amount of horizontal muscle recession is performed, contracture of the medial rectus occurs with time, or an inadequate vector force is generated by muscle transposition.[66]
- Consecutive exotropia: Consecutive exotropia may result if excess tension is created by vertical muscle transposition, if the ipsilateral medial rectus is weak, or if co-contraction is worsened by transposition.[63]
- Induced vertical deviation: Induced vertical deviation may result in a restrictive imbalance between the transposed muscles or if recession or slippage of the transposed muscle occurs. If excess muscle belly is used for transposition, the vertical action of the muscle may also be weakened, leading to induced vertical deviation.[63]
Table 9. Complications of Duane Retraction Syndrome
| Complication | Etiology/Mechanism | Clinical Consequences |
| Amblyopia | Strabismus, anisometropia, or suppression | Reduced visual acuity, especially in children |
| Loss of binocular vision | Large ocular deviation or suppression of 1 eye | Impaired depth perception and stereopsis |
| Abnormal head posture | Compensatory face turn to maintain binocular single vision | Long-term musculoskeletal strain, facial asymmetry |
| Globe retraction | Co-contraction of the medial and lateral rectus muscles | Cosmetic deformity, functional limitation in adduction |
| Upshoots or downshoots | Mechanical leash effect or slipped lateral rectus | Disfiguring vertical deviation in adduction |
| Persistent ocular deviation | Residual misalignment despite surgical intervention | Strabismus symptoms, possible diplopia |
| Surgical complications | Over/under-recession of the recti, induced vertical deviation | New motility restrictions, residual or recurrent deviation |
| Diplopia | Disruption of fusion post-surgery | Visual discomfort may affect daily activities |
| Neck or spinal issues | Chronic abnormal head posture | Musculoskeletal pain, torticollis |
| Syndromic associations | Part of systemic anomalies (eg, Goldenhar, Klippel-Feil, and Okihiro syndromes) | Vertebral anomalies, hearing loss, renal malformations |
| Psychosocial issues | Visible globe retraction, abnormal eye movements, and facial asymmetry | Reduced self-esteem, social anxiety, and impact on quality of life |
Postoperative and Rehabilitation Care
Postoperative and rehabilitation care for patients with Duane retraction syndrome is crucial to ensure optimal surgical outcomes, prevent complications, and support functional adaptation. Although surgery in Duane retraction syndrome primarily aims to improve ocular alignment in primary gaze, reduce abnormal head posture, and minimize globe retraction, it does not restore normal ocular motility. Therefore, postoperative care focuses on maximizing the benefits achieved through surgery while addressing any residual or recurrent symptoms.
Immediate Postoperative Care
- Pain and inflammation control: Topical antibiotics combined with corticosteroid drops are commonly prescribed for 1 to 2 weeks to reduce inflammation and prevent infection.
- Monitoring wound healing: Regular slit-lamp examination to assess conjunctival healing, suture status, and absence of infection.
- Ocular motility assessment: Early postoperative motility checks to identify overcorrection, undercorrection, or unexpected limitations in movement.[56]
Functional Rehabilitation
- Management of residual head posture: Patients with persistent abnormal head posture may benefit from prism glasses or orthoptic therapy to improve binocular function and reduce compensatory movements.
- Amblyopia therapy: In pediatric patients, especially those with unilateral involvement, occlusion therapy may be continued or initiated to prevent amblyopia.
- Binocular vision training: Orthoptic exercises can enhance fusional amplitudes and improve visual comfort, especially in cases with residual deviation in lateral gazes.[90]
Patient Education and Follow-up
- Realistic expectations: Patients and parents should be counseled that surgery aims to improve alignment and head posture but does not restore normal eye movements.
- Long-term follow-up: Regular follow-up is needed to monitor for recurrence of deviation, especially during growth in children, and to detect any late complications such as muscle slippage or scarring.
- Activity guidance: No swimming or contact sports for at least 2 to 3 weeks post-surgery; avoid eye rubbing to prevent wound dehiscence.[91]
Interprofessional Care
A coordinated approach involving ophthalmologists, orthoptists, optometrists, and pediatricians ensures comprehensive rehabilitation. Orthoptists play a key role in vision therapy, whereas pediatricians monitor developmental milestones and overall well-being. In cases with syndromic associations, neurologists or geneticists may be involved in ongoing care.[92]
Long-term Considerations
Some patients may require secondary procedures for residual misalignment or for improving cosmetic appearance. Lifelong surveillance is recommended for children, as craniofacial growth may alter ocular alignment over time.[93]
Consultations
Effective management of Duane retraction syndrome often requires a multidisciplinary approach, as the condition may present with associated ocular, neurological, or systemic anomalies. The primary consultation is with an ophthalmologist—preferably a pediatric ophthalmologist or strabismus specialist—who establishes the diagnosis, classifies the subtype, and outlines treatment options. An orthoptist plays a critical role in assessing ocular motility, binocular function, and abnormal head posture, aiding in both diagnosis and follow-up evaluation.[5]
Given that Duane retraction syndrome can occasionally be associated with systemic syndromes such as Goldenhar syndrome, Wildervanck syndrome, or Klippel-Feil anomaly, referral to a pediatrician or geneticist is advisable for comprehensive evaluation. A neurologist may be consulted in atypical cases or when neurological involvement is suspected. For patients undergoing surgical intervention, an anesthesiologist consultation is important, especially in pediatric patients and those with cervical spine anomalies.[94]
Additionally, involvement of a low vision specialist may be warranted in cases with amblyopia or significant visual impairment. Occupational therapists can support children with associated motor or developmental delays. For older patients or those concerned about appearance, psychological support or counseling may be beneficial to address self-esteem and social challenges. Coordinated care between these professionals ensures optimal functional and cosmetic outcomes, early detection of associated conditions, and comprehensive patient support.[95]
Deterrence and Patient Education
Patients and their families should be informed of the necessity of a thorough systemic evaluation and genetic analysis, as Duane retraction syndrome may be associated with other systemic anomalies. If surgery is not indicated, the importance of complying with spectacle or prism correction and amblyopia therapy should be explained. If surgery is indicated, it should be emphasized to the patient that no procedure can guarantee full ocular motility, as the underlying abnormality of paradoxical innervation cannot be corrected.[96]
Effective deterrence and patient education in Duane retraction syndrome centers on early recognition, informed counseling, and fostering realistic expectations regarding visual outcomes and surgical limitations. Although Duane retraction syndrome is a congenital, non-progressive condition with no known preventive measures, proactive strategies can help reduce secondary complications and improve quality of life.
Patient and Caregiver Counseling
Patients and families should be informed that Duane retraction syndrome results from aberrant innervation of the extraocular muscles, not from progressive muscle disease. Emphasis should be placed on the generally stable nature of the condition, the importance of regular ophthalmic follow-up, and the fact that surgery—when indicated—aims primarily to improve head posture, ocular alignment, and binocular function, rather than to restore normal ocular motility.[2]
Lifestyle and Daily Adaptations
Encouraging adaptive head posture techniques can help minimize diplopia and improve the field of vision in affected gaze positions. Parents should be advised to monitor children for abnormal head turns, tilts, or squints, which may require early intervention to prevent musculoskeletal strain or social discomfort.[97]
Avoidance of Risk Factors for Amblyopia
Routine vision screening is crucial to detect and treat amblyopia early. Timely correction of refractive errors, use of occlusion therapy when indicated, and addressing anisometropia are essential in preventing long-term vision loss.[98]
Educational Support
Teachers should be made aware of the child's visual limitations so that seating arrangements and classroom activities can be adapted to optimize binocular vision and comfort.[36]
Surgical Decision-Making Education
Patients and caregivers should understand that surgical correction does not eliminate the underlying neural miswiring. Recurrence of abnormal movements or residual limitations in ocular motility may persist postoperatively, and multiple procedures may be needed in complex cases.[10]
Long-Term Prognosis Communication
Reassuring patients about the non-progressive nature of Duane retraction syndrome can reduce anxiety. Emphasizing that most patients adapt well and can lead normal, functional lives helps set realistic and positive expectations.[72]
Pearls and Other Issues
Key Pearls
- Early recognition: Duane retraction syndrome is often diagnosed in childhood due to abnormal head posture or limited ocular movements; early identification allows timely management of amblyopia and prevention of secondary complications.
- Avoid unnecessary surgery: Not all patients require surgical correction; many maintain satisfactory binocular function through compensatory head posture.
- Tailored surgical approach: When surgery is indicated (eg, for significant misalignment or abnormal head turn), procedures should be individualized according to Duane retraction syndrome type (Huber's classification) and presence of globe retraction or upshoot/downshoot.
- Amblyopia risk: Although less common than in other strabismus types, amblyopia can occur, especially in patients with anisometropia or large deviations; proactive screening is essential.[99]
Common Pitfalls
- Misdiagnosing Duane retraction syndrome as sixth nerve palsy or congenital esotropia, leading to inappropriate investigations or interventions.
- Overcorrecting horizontal deviation surgically can worsen globe retraction or induce vertical deviations.
- Ignoring compensatory head posture in functional assessment potentially underestimates the impact of the condition on daily activities.[100]
Disposition and Prevention
- Most patients require long-term follow-up into adulthood to monitor ocular alignment, binocular vision, and refractive status.
- Early refractive correction, amblyopia treatment, and patient/family counseling help optimize outcomes.
- Education on maintaining head posture within safe ergonomic limits can prevent musculoskeletal strain.[77]
Additional Considerations
- Duane retraction syndrome can be associated with other congenital anomalies (eg, Goldenhar syndrome and Klippel-Feil anomaly); thorough systemic evaluation may be warranted.
- Genetic counseling may be beneficial for families, especially in bilateral or familial cases.
- Interprofessional collaboration with orthoptists, pediatric ophthalmologists, neurologists, and physiotherapists enhances holistic care and patient satisfaction.[31]
Enhancing Healthcare Team Outcomes
Although cases of isolated Duane retraction syndrome can be managed by ophthalmologists alone, a thorough systemic evaluation by other healthcare professionals, such as the pediatrician, family clinician, and ENT specialist, operating as an interprofessional healthcare team, is necessary to rule out systemic anomalies, which are not uncommon in Duane retraction syndrome. Additionally, pedigree analysis, MRI, and genetic studies play a role in enhancing understanding of the clinical condition, thus improving the quality of life for these patients and their families. Ophthalmology nurses also play a significant role by assisting in surgery and providing post-procedural care and counseling for the patient. These interprofessional activities drive better patient outcomes.[2]
Effective management of Duane retraction syndrome requires a coordinated, multidisciplinary approach involving ophthalmologists, pediatric ophthalmologists, orthoptists, neurologists, optometrists, and, when necessary, genetic counselors. Clear interprofessional communication ensures accurate diagnosis, particularly in differentiating Duane retraction syndrome from other forms of strabismus, cranial nerve palsies, or restrictive myopathies. Clinicians and advanced practitioners play a central role in establishing the treatment plan, whether involving observation, prisms, botulinum toxin injections, or surgical correction, and in coordinating care across specialties. Orthoptists provide detailed motility assessments, essential for surgical planning and postoperative evaluation. Genetic counselors contribute by assessing hereditary patterns and counseling affected families. Nurses and allied health professionals support perioperative care, patient education, and follow-up scheduling. Pharmacists assist with the safe use of adjunctive therapies such as lubricants or botulinum toxin preparations. By integrating shared decision-making, evidence-based protocols, and clear referral pathways, the interprofessional team can enhance patient-centered care, improve functional and cosmetic outcomes, ensure patient safety, and optimize long-term quality of life for individuals with Duane retraction syndrome.[3]
Media
(Click Image to Enlarge)
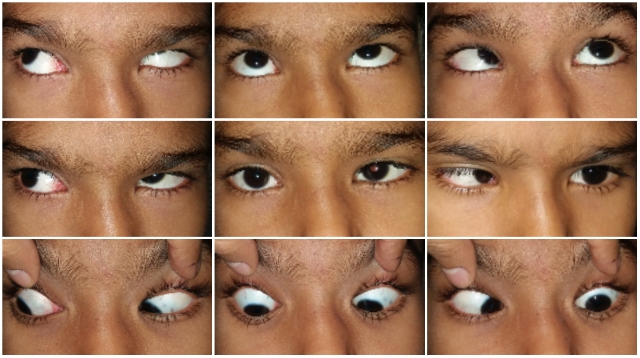
11 year old boy with esotropic DRS of left eye, showing limitation of abduction and globe retraction and upshoot in adduction Contributed by Dr. Ipsita Muni, MS
References
Assaf AA. Congenital innervation dysgenesis syndrome (CID)/congenital cranial dysinnervation disorders (CCDDs). Eye (London, England). 2011 Oct:25(10):1251-61. doi: 10.1038/eye.2011.38. Epub 2011 Jul 1 [PubMed PMID: 21720410]
Komori M, Sato M, Arakawa A, Kaneko H, Hikoya A. Surgical Management of a Prominent Adduction-Induced Upshoot in Duane Retraction Syndrome Type III: A Case Report. Cureus. 2025 Jul:17(7):e87397. doi: 10.7759/cureus.87397. Epub 2025 Jul 6 [PubMed PMID: 40772180]
Level 3 (low-level) evidencePrinz J, Hartmann K, Walter P, Lohmann T, Fuest M, Kuerten D. Tendon Elongation with Fascia Lata Grafts in Strabismus Surgery - Multiple Indications Apart from Graves' Orbitopathy. Klinische Monatsblatter fur Augenheilkunde. 2026 Mar:243(3):205-211. doi: 10.1055/a-2611-2250. Epub 2025 Jun 16 [PubMed PMID: 40523404]
Huang L, Chen B, Cai C, Wu Y, Sun Z, Xie Y, Li N. Etiology and clinical features of Han Chinese patients with Duane retraction syndrome. Frontiers in genetics. 2025:16():1500090. doi: 10.3389/fgene.2025.1500090. Epub 2025 Mar 27 [PubMed PMID: 40212284]
Erduran B, Niyaz Şahin L. Screening of Clinical Data of Patients with Abnormal Head Posture and Investigation of Abnormal Head Posture Change After Treatment. Turkish journal of ophthalmology. 2025 Feb 27:55(1):11-15. doi: 10.4274/tjo.galenos.2024.71163. Epub [PubMed PMID: 40013480]
Gokahru S, Gupta E, Das S. Inverse Duane's retraction syndrome: rare presentation of orbital myocysticercosis. Strabismus. 2025 Dec:33(4):283-287. doi: 10.1080/09273972.2025.2468245. Epub 2025 Feb 24 [PubMed PMID: 39991906]
Jauregui R, Grossman SN. Teaching Video NeuroImage: Globe Retraction in Duane Syndrome. Neurology. 2025 Mar 11:104(5):e213409. doi: 10.1212/WNL.0000000000213409. Epub 2025 Jan 31 [PubMed PMID: 39889267]
Al-Dabet S, Turaev S, Zaki N. Ocular-induced abnormal head postures: A systematic review and analysis. Survey of ophthalmology. 2025 Jul-Aug:70(4):771-816. doi: 10.1016/j.survophthal.2025.01.016. Epub 2025 Feb 9 [PubMed PMID: 39933628]
Level 1 (high-level) evidencePark J, Yang HK, Hwang JM. Long-term surgical outcomes of esotropic duane retraction syndrome type 1. Scientific reports. 2025 Jan 27:15(1):3358. doi: 10.1038/s41598-024-78738-z. Epub 2025 Jan 27 [PubMed PMID: 39870649]
Zhou HY, Langue M, Tien DR. Successful outcome in synergistic divergence after unilateral lateral rectus recession and medial rectus resection. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2025 Feb:29(1):104092. doi: 10.1016/j.jaapos.2024.104092. Epub 2024 Dec 30 [PubMed PMID: 39742952]
Kefeli I, Yaman A, Saatci AO. Angiographically silent macular retinoschisis and vitreomacular traction in a patient with same - side Duane retraction syndrome. Strabismus. 2025 Mar:33(1):58-60. doi: 10.1080/09273972.2024.2399351. Epub 2024 Sep 3 [PubMed PMID: 39227363]
Tran L, Oatts JT, Indaram M. Duane retraction syndrome associated with EP300 variant of Rubinstein-Taybi syndrome. American journal of ophthalmology case reports. 2024 Dec:36():102226. doi: 10.1016/j.ajoc.2024.102226. Epub 2024 Nov 28 [PubMed PMID: 39697674]
Level 3 (low-level) evidenceAbu Melha A, Abbas AI, Alghamdi WS, Alghamdi SM, Alkhathami A. Duane Retraction Syndrome: A Report of Two Cases and Review of Literature. Cureus. 2024 Nov:16(11):e74460. doi: 10.7759/cureus.74460. Epub 2024 Nov 25 [PubMed PMID: 39734938]
Level 3 (low-level) evidenceKekunnaya R, Negalur M. Duane retraction syndrome: causes, effects and management strategies. Clinical ophthalmology (Auckland, N.Z.). 2017:11():1917-1930. doi: 10.2147/OPTH.S127481. Epub 2017 Oct 30 [PubMed PMID: 29133973]
Strachan IM, Brown BH. Electromyography of extraocular muscles in Duane's syndrome. The British journal of ophthalmology. 1972 Aug:56(8):594-9 [PubMed PMID: 5079406]
Hoyt WF, Nachtigäller H. Anomalies of ocular motor nerves. Neuroanatomic correlates of paradoxical innervation in Duane's syndrome and related congenital ocular motor disorders. American journal of ophthalmology. 1965 Sep:60(3):443-8 [PubMed PMID: 5828681]
Yüksel D, Orban de Xivry JJ, Lefèvre P. Review of the major findings about Duane retraction syndrome (DRS) leading to an updated form of classification. Vision research. 2010 Nov 23:50(23):2334-47. doi: 10.1016/j.visres.2010.08.019. Epub 2010 Aug 27 [PubMed PMID: 20801148]
Pfaffenbach DD, Cross HE, Kearns TP. Congenital anomalies in Duane's retraction syndrome. Archives of ophthalmology (Chicago, Ill. : 1960). 1972 Dec:88(6):635-9 [PubMed PMID: 4628563]
Appukuttan B, Gillanders E, Juo SH, Freas-Lutz D, Ott S, Sood R, Van Auken A, Bailey-Wilson J, Wang X, Patel RJ, Robbins CM, Chung M, Annett G, Weinberg K, Borchert MS, Trent JM, Brownstein MJ, Stout JT. Localization of a gene for Duane retraction syndrome to chromosome 2q31. American journal of human genetics. 1999 Dec:65(6):1639-46 [PubMed PMID: 10577917]
Miyake N, Chilton J, Psatha M, Cheng L, Andrews C, Chan WM, Law K, Crosier M, Lindsay S, Cheung M, Allen J, Gutowski NJ, Ellard S, Young E, Iannaccone A, Appukuttan B, Stout JT, Christiansen S, Ciccarelli ML, Baldi A, Campioni M, Zenteno JC, Davenport D, Mariani LE, Sahin M, Guthrie S, Engle EC. Human CHN1 mutations hyperactivate alpha2-chimaerin and cause Duane's retraction syndrome. Science (New York, N.Y.). 2008 Aug 8:321(5890):839-43. doi: 10.1126/science.1156121. Epub 2008 Jul 24 [PubMed PMID: 18653847]
Level 3 (low-level) evidenceBosley TM, Abu-Amero KK, Oystreck DT. Congenital cranial dysinnervation disorders: a concept in evolution. Current opinion in ophthalmology. 2013 Sep:24(5):398-406. doi: 10.1097/ICU.0b013e3283645ad6. Epub [PubMed PMID: 23872818]
Level 3 (low-level) evidenceKohlhase J, Schubert L, Liebers M, Rauch A, Becker K, Mohammed SN, Newbury-Ecob R, Reardon W. Mutations at the SALL4 locus on chromosome 20 result in a range of clinically overlapping phenotypes, including Okihiro syndrome, Holt-Oram syndrome, acro-renal-ocular syndrome, and patients previously reported to represent thalidomide embryopathy. Journal of medical genetics. 2003 Jul:40(7):473-8 [PubMed PMID: 12843316]
DeRespinis PA, Caputo AR, Wagner RS, Guo S. Duane's retraction syndrome. Survey of ophthalmology. 1993 Nov-Dec:38(3):257-88 [PubMed PMID: 8310396]
Level 3 (low-level) evidenceKekunnaya R, Gupta A, Sachdeva V, Krishnaiah S, Venkateshwar Rao B, Vashist U, Ray D. Duane retraction syndrome: series of 441 cases. Journal of pediatric ophthalmology and strabismus. 2012 May-Jun:49(3):164-9. doi: 10.3928/01913913-20111101-01. Epub 2011 Nov 8 [PubMed PMID: 22074356]
Level 2 (mid-level) evidenceMohan K, Sharma A, Pandav SS. Differences in epidemiological and clinical characteristics between various types of Duane retraction syndrome in 331 patients. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2008 Dec:12(6):576-80. doi: 10.1016/j.jaapos.2008.04.015. Epub 2008 Aug 23 [PubMed PMID: 18723379]
Level 2 (mid-level) evidenceHerron MS, Wang L, von Bartheld CS. Prevalence and types of strabismus in cerebral palsy: A global and historical perspective based on a systematic review and meta-analysis. medRxiv : the preprint server for health sciences. 2024 Jan 24:():. pii: 2024.01.23.24301684. doi: 10.1101/2024.01.23.24301684. Epub 2024 Jan 24 [PubMed PMID: 38343841]
Level 1 (high-level) evidencePlevkova J, Brozmanova M, Harsanyiova J, Sterusky M, Honetschlager J, Buday T. Various aspects of sex and gender bias in biomedical research. Physiological research. 2020 Dec 31:69(Suppl 3):S367-S378 [PubMed PMID: 33464920]
Topilow NJ, Tran AQ, Koo EB, Alabiad CR. Etiologies of Proptosis: A review. Internal medicine review (Washington, D.C. : Online). 2020 Mar:6(3):. doi: 10.18103/imr.v6i3.852. Epub [PubMed PMID: 32382689]
Self JE, Dunn MJ, Erichsen JT, Gottlob I, Griffiths HJ, Harris C, Lee H, Owen J, Sanders J, Shawkat F, Theodorou M, Whittle JP, Nystagmus UK Eye research group (NUKE). Management of nystagmus in children: a review of the literature and current practice in UK specialist services. Eye (London, England). 2020 Sep:34(9):1515-1534. doi: 10.1038/s41433-019-0741-3. Epub 2020 Jan 9 [PubMed PMID: 31919431]
Alreheli AQ, Aloufi MM, Aalam W, Kordi ES, Al-Habboubi HF. The clinical characteristics of Duane retraction syndrome in Al-Medina region. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2019 Oct-Dec:33(4):338-341. doi: 10.1016/j.sjopt.2019.07.007. Epub 2019 Aug 8 [PubMed PMID: 31920443]
Tsirikos AI, McMaster MJ. Goldenhar-associated conditions (hemifacial microsomia) and congenital deformities of the spine. Spine. 2006 Jun 1:31(13):E400-7 [PubMed PMID: 16741440]
Level 2 (mid-level) evidenceMiyake N, Andrews C, Fan W, He W, Chan WM, Engle EC. CHN1 mutations are not a common cause of sporadic Duane's retraction syndrome. American journal of medical genetics. Part A. 2010 Jan:152A(1):215-7. doi: 10.1002/ajmg.a.33168. Epub [PubMed PMID: 20034095]
Zanin E, Gambarelli N, Denis D. Distinctive clinical features of bilateral Duane retraction syndrome. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2010 Aug:14(4):293-7. doi: 10.1016/j.jaapos.2010.02.010. Epub [PubMed PMID: 20736120]
Level 2 (mid-level) evidenceScott AB, Wong GY. Duane's syndrome. An electromyographic study. Archives of ophthalmology (Chicago, Ill. : 1960). 1972 Feb:87(2):140-7 [PubMed PMID: 5057862]
Cheah JASS, Tharmathurai S, Bahari NA, Rahmat J, Muhammed J. Duane Retraction Syndrome With Mechanical and Innervational Upshoot and Secondary Superior Rectus Contracture: A Surgical Challenge. Cureus. 2022 Oct:14(10):e30470. doi: 10.7759/cureus.30470. Epub 2022 Oct 19 [PubMed PMID: 36415378]
Khorrami-Nejad M, Akbari MR, Masoomian B, Mahmood HA, Daneshvar K, Majdi A. Astigmatism in Duane Retraction Syndrome. BMC ophthalmology. 2025 Jan 10:25(1):15. doi: 10.1186/s12886-025-03855-w. Epub 2025 Jan 10 [PubMed PMID: 39794722]
Vujasinovic Stupar N, Pavlov-Dolijanovic S, Hatib N, Banko B, Djukic M, Nikolic Jakoba N. Multiple Major and Minor Anomalies Associated With Klippel-Feil Syndrome: A Case Report. Archives of rheumatology. 2016 Mar:31(1):82-86. doi: 10.5606/ArchRheumatol.2016.5714. Epub 2015 Nov 3 [PubMed PMID: 29901000]
Level 3 (low-level) evidenceFarvardin H, Farvardin M, Zare K. Type III Duane Retraction Syndrome and Monocular Elevation Deficiency, Simultaneous Presentation in a 16-year-old girl. Romanian journal of ophthalmology. 2024 Oct-Dec:68(4):439-442. doi: 10.22336/rjo.2024.79. Epub [PubMed PMID: 39936058]
Vemula S, Muvavarirwa T, Doornbos F, Whitman MC. Neuromuscular Junction Development Differs Between Extraocular and Skeletal Muscles and Between Different Extraocular Muscles. Investigative ophthalmology & visual science. 2024 May 1:65(5):28. doi: 10.1167/iovs.65.5.28. Epub [PubMed PMID: 38767908]
Van De Vlekkert D, Machado E, d'Azzo A. Analysis of Generalized Fibrosis in Mouse Tissue Sections with Masson's Trichrome Staining. Bio-protocol. 2020 May 20:10(10):e3629. doi: 10.21769/BioProtoc.3629. Epub 2020 May 20 [PubMed PMID: 33659302]
Gao Y, Li D, Lin J, Thomas AM, Miao J, Chen D, Li S, Chu C. Cerebral small vessel disease: Pathological mechanisms and potential therapeutic targets. Frontiers in aging neuroscience. 2022:14():961661. doi: 10.3389/fnagi.2022.961661. Epub 2022 Aug 12 [PubMed PMID: 36034144]
Ravenscroft G, Laing NG, Bönnemann CG. Pathophysiological concepts in the congenital myopathies: blurring the boundaries, sharpening the focus. Brain : a journal of neurology. 2015 Feb:138(Pt 2):246-68. doi: 10.1093/brain/awu368. Epub 2014 Dec 31 [PubMed PMID: 25552303]
Dixit R, Riviere J, Krishnan K, Andersen ME. Toxicokinetics and physiologically based toxicokinetics in toxicology and risk assessment. Journal of toxicology and environmental health. Part B, Critical reviews. 2003 Jan-Feb:6(1):1-40 [PubMed PMID: 12587252]
Krauer B, Dayer P. Fetal drug metabolism and its possible clinical implications. Clinical pharmacokinetics. 1991 Jul:21(1):70-80 [PubMed PMID: 1914342]
Hudson RE, Metz TD, Ward RM, McKnite AM, Enioutina EY, Sherwin CM, Watt KM, Job KM. Drug exposure during pregnancy: Current understanding and approaches to measure maternal-fetal drug exposure. Frontiers in pharmacology. 2023:14():1111601. doi: 10.3389/fphar.2023.1111601. Epub 2023 Mar 23 [PubMed PMID: 37033628]
Level 3 (low-level) evidenceKotta-Loizou I, Pritsa A, Antasouras G, Vasilopoulos SN, Voulgaridou G, Papadopoulou SK, Coutts RHA, Lechouritis E, Giaginis C. Fetus Exposure to Drugs and Chemicals: A Holistic Overview on the Assessment of Their Transport and Metabolism across the Human Placental Barrier. Diseases (Basel, Switzerland). 2024 Jun 1:12(6):. doi: 10.3390/diseases12060114. Epub 2024 Jun 1 [PubMed PMID: 38920546]
Level 3 (low-level) evidenceKasturi N. Congenital sixth nerve palsy with associated anomalies. Indian journal of ophthalmology. 2017 Oct:65(10):1056-1057. doi: 10.4103/ijo.IJO_335_17. Epub [PubMed PMID: 29044089]
Isenberg S, Urist MJ. Clinical observations in 101 consecutive patients with Duane's retraction syndrome. American journal of ophthalmology. 1977 Sep:84(3):419-25 [PubMed PMID: 900234]
Level 2 (mid-level) evidencePenix K, Swanson MW, DeCarlo DK. Nystagmus in pediatric patients: interventions and patient-focused perspectives. Clinical ophthalmology (Auckland, N.Z.). 2015:9():1527-36. doi: 10.2147/OPTH.S62786. Epub 2015 Aug 21 [PubMed PMID: 26345377]
Level 3 (low-level) evidenceHutchinson AK, Morse CL, Hercinovic A, Cruz OA, Sprunger DT, Repka MX, Lambert SR, Wallace DK, American Academy of Ophthalmology Preferred Practice Pattern Pediatric Ophthalmology/Strabismus Panel. Pediatric Eye Evaluations Preferred Practice Pattern. Ophthalmology. 2023 Mar:130(3):P222-P270. doi: 10.1016/j.ophtha.2022.10.030. Epub 2022 Dec 19 [PubMed PMID: 36543602]
Awadein A, Arfeen SA, Chougule P, Kekunnaya R. Duane-minus (Duane sine retraction and Duane sine limitation): possible incomplete forms of Duane retraction syndrome. Eye (London, England). 2021 Jun:35(6):1673-1679. doi: 10.1038/s41433-020-1118-3. Epub 2020 Aug 24 [PubMed PMID: 32839562]
Candy TR, Cormack LK. Recent understanding of binocular vision in the natural environment with clinical implications. Progress in retinal and eye research. 2022 May:88():101014. doi: 10.1016/j.preteyeres.2021.101014. Epub 2021 Oct 6 [PubMed PMID: 34624515]
Level 3 (low-level) evidenceSemeraro F,Forbice E,Nascimbeni G,Cillino S,Bonfiglio VME,Filippelli ME,Bartollino S,Costagliola C, Ocular Refraction at Birth and Its Development During the First Year of Life in a Large Cohort of Babies in a Single Center in Northern Italy. Frontiers in pediatrics. 2019; [PubMed PMID: 32083036]
Kekunnaya R, Velez FG, Pineles SL. Outcomes in patients with esotropic duane retraction syndrome and a partially accommodative component. Indian journal of ophthalmology. 2013 Dec:61(12):701-4. doi: 10.4103/0301-4738.124744. Epub [PubMed PMID: 24413823]
Level 2 (mid-level) evidenceHuber A. Electrophysiology of the retraction syndromes. The British journal of ophthalmology. 1974 Mar:58(3):293-300 [PubMed PMID: 4834602]
Akbari MR, Manouchehri V, Mirmohammadsadeghi A. Surgical treatment of Duane retraction syndrome. Journal of current ophthalmology. 2017 Dec:29(4):248-257. doi: 10.1016/j.joco.2017.08.008. Epub 2017 Sep 11 [PubMed PMID: 29270470]
Kim JH, Hwang JM. Imaging of Cranial Nerves III, IV, VI in Congenital Cranial Dysinnervation Disorders. Korean journal of ophthalmology : KJO. 2017 Jun:31(3):183-193. doi: 10.3341/kjo.2017.0024. Epub 2017 May 12 [PubMed PMID: 28534340]
Galldiks N, Haupt WF. Diagnostic value of the electromyography of the extraocular muscles. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2008 Dec:119(12):2785-8. doi: 10.1016/j.clinph.2008.08.026. Epub 2008 Nov 4 [PubMed PMID: 18986833]
Lee YJ, Lee HJ, Kim SJ. Clinical Features of Duane Retraction Syndrome: A New Classification. Korean journal of ophthalmology : KJO. 2020 Apr:34(2):158-165. doi: 10.3341/kjo.2019.0100. Epub [PubMed PMID: 32233150]
Silbert DI, Matta NS, Burkholder D, Gehman A, Fenwick J. Clinical accuracy of the AAPOS pediatric vision screening referral criteria. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2012 Aug:16(4):361-4. doi: 10.1016/j.jaapos.2012.02.016. Epub 2012 Jul 21 [PubMed PMID: 22824492]
Dawson EL, Maino A, Lee JP. Diagnostic use of botulinum toxin in patients with Duane syndrome. Strabismus. 2010 Mar:18(1):21-3. doi: 10.3109/09273970903580199. Epub [PubMed PMID: 20230203]
Level 2 (mid-level) evidenceGaur N, Sharma P. Management of Duane retraction syndrome: A simplified approach. Indian journal of ophthalmology. 2019 Jan:67(1):16-22. doi: 10.4103/ijo.IJO_967_18. Epub [PubMed PMID: 30574884]
Kekunnaya R, Kraft S, Rao VB, Velez FG, Sachdeva V, Hunter DG. Surgical management of strabismus in Duane retraction syndrome. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2015 Feb:19(1):63-9. doi: 10.1016/j.jaapos.2014.10.019. Epub [PubMed PMID: 25727590]
Sprunger DT. Recession of both horizontal rectus muscles in Duane syndrome with globe retraction in primary position. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 1997 Mar:1(1):31-3 [PubMed PMID: 10530982]
Level 3 (low-level) evidenceRosenbaum AL. Costenbader Lecture. The efficacy of rectus muscle transposition surgery in esotropic Duane syndrome and VI nerve palsy. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2004 Oct:8(5):409-19 [PubMed PMID: 15492732]
Level 2 (mid-level) evidenceRuth AL, Velez FG, Rosenbaum AL. Management of vertical deviations after vertical rectus transposition surgery. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2009 Feb:13(1):16-9. doi: 10.1016/j.jaapos.2008.08.015. Epub 2008 Dec 31 [PubMed PMID: 19117778]
Level 2 (mid-level) evidenceSaunders RA, Bluestein EC, Wilson ME, Berland JE. Anterior segment ischemia after strabismus surgery. Survey of ophthalmology. 1994 Mar-Apr:38(5):456-66 [PubMed PMID: 8009429]
Level 3 (low-level) evidenceRogers GL, Bremer DL. Surgical treatment of the upshoot and downshoot in Duanes' retraction syndrome. Ophthalmology. 1984 Nov:91(11):1380-3 [PubMed PMID: 6514307]
Level 3 (low-level) evidenceMohan K, Saroha V. Vertical rectus recession for the innervational upshoot and downshoot in Duane's retraction syndrome. Journal of pediatric ophthalmology and strabismus. 2002 Mar-Apr:39(2):94-9 [PubMed PMID: 11911551]
Awadein A. Inferior oblique myectomy for upshoots mimicking inferior oblique overaction in Duane retraction syndrome. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2013 Jun:17(3):253-8. doi: 10.1016/j.jaapos.2013.01.005. Epub 2013 May 11 [PubMed PMID: 23672883]
Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, Barry BJ, Whitman MC, Hunter DG, Engle EC. Duane Syndrome. GeneReviews(®). 1993:(): [PubMed PMID: 20301369]
Farvardin H, Safari F, Safari F, Farvardin H, Farvardin M. Y-split Recession of Lateral Rectus With and Without Medial Rectus Recession in the Management of Exotropic Duane Retraction Syndrome With Significant Overshoot and Retraction. Journal of pediatric ophthalmology and strabismus. 2025 Jan-Feb:62(1):67-74. doi: 10.3928/01913913-20241105-05. Epub 2024 Dec 2 [PubMed PMID: 39620612]
Lim HW, Hwang B, Archambault C, Lambert SR. Rates of Reoperation in Duane Retraction Syndrome. Ophthalmology science. 2024 Sep-Oct:4(5):100479. doi: 10.1016/j.xops.2024.100479. Epub 2024 Jan 28 [PubMed PMID: 38827492]
Duane TD, Schatz NJ, Caputo AR. Pseudo-Duane's retraction syndrome. Transactions of the American Ophthalmological Society. 1976:74():122-32 [PubMed PMID: 867622]
Kanazawa T, Iwasaki T, Takahashi M, Kakinuma K, Ezuka I, Yamada H. [Detailed magnetic resonance imaging of abducens nerve by 3D-CISS]. Nihon Hoshasen Gijutsu Gakkai zasshi. 2003 Aug:59(8):958-64 [PubMed PMID: 12960949]
Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, Kohlhase J. SALL4-Related Disorders. GeneReviews(®). 1993:(): [PubMed PMID: 20301547]
Sprunger DT, Lambert SR, Hercinovic A, Morse CL, Repka MX, Hutchinson AK, Cruz OA, Wallace DK, American Academy of Ophthalmology Preferred Practice Pattern Pediatric Ophthalmology/Strabismus Panel. Esotropia and Exotropia Preferred Practice Pattern®. Ophthalmology. 2023 Mar:130(3):P179-P221. doi: 10.1016/j.ophtha.2022.11.002. Epub 2022 Dec 14 [PubMed PMID: 36526451]
Webber A, Randhawa S, Felizzi F, Soos M, Arbuckle R, O'Brien P, Harrad R, Khuddus N, Bouchet C, Panter C. The Amblyopia Quality of Life (AmbQoL): Development and Content Validation of a Novel Health-Related Quality of Life Instrument for Use in Adult and Pediatric Amblyopia Populations. Ophthalmology and therapy. 2023 Apr:12(2):1281-1313. doi: 10.1007/s40123-023-00668-2. Epub 2023 Feb 24 [PubMed PMID: 36828953]
Level 1 (high-level) evidenceYao J, Jiang C, Wang X, Xia W, Ling L, Zhu W, Wu L, Zhao C. Effect of Modified Vertical Rectus Belly Transposition vs Augmented Superior Rectus Transposition Plus Medial Rectus Recession for Chronic Sixth Nerve Palsy: A Randomized Clinical Trial. JAMA ophthalmology. 2022 Sep 1:140(9):872-879. doi: 10.1001/jamaophthalmol.2022.2856. Epub [PubMed PMID: 35925582]
Level 1 (high-level) evidenceSnir M, Dotan A, Friling R, Ron-Kella Y, Goldenberg-Cohen N, Stiebel-Kalish H. Contralateral lateral rectus muscle recession in patients with Duane retraction syndrome type 3. Eye (London, England). 2014 Mar:28(3):279-84. doi: 10.1038/eye.2013.260. Epub 2013 Dec 6 [PubMed PMID: 24310235]
Gaballah KA, Shawky D. Treatment modalities in Duane's Retraction Syndrome. International journal of ophthalmology. 2020:13(2):278-283. doi: 10.18240/ijo.2020.02.12. Epub 2020 Feb 18 [PubMed PMID: 32090038]
Kaur K, Gurnani B. Intermittent Exotropia. StatPearls. 2026 Jan:(): [PubMed PMID: 34662028]
Zandi A, Amirkhani A, Pourazizi M. Unilateral medial rectus muscle recession combined lateral rectus muscle marginal myotomy for the treatment of Duane's retraction syndrome: A promising surgical procedure. Journal of research in medical sciences : the official journal of Isfahan University of Medical Sciences. 2020:25():54. doi: 10.4103/jrms.JRMS_836_19. Epub 2020 May 22 [PubMed PMID: 32765624]
Negalur M, Sachdeva V, Kekunnaya R. Superior Rectus Transposition in the Management of Duane Retraction Syndrome: Current Insights. Clinical ophthalmology (Auckland, N.Z.). 2022:16():201-212. doi: 10.2147/OPTH.S284608. Epub 2022 Jan 26 [PubMed PMID: 35115760]
Nestor MS, Han H, Gade A, Fischer D, Saban Y, Polselli R. Botulinum toxin-induced blepharoptosis: Anatomy, etiology, prevention, and therapeutic options. Journal of cosmetic dermatology. 2021 Oct:20(10):3133-3146. doi: 10.1111/jocd.14361. Epub 2021 Aug 11 [PubMed PMID: 34378298]
North RV, Henson DB. Effect of orthoptics upon the ability of patients to adapt to prism-induced heterophoria. American journal of optometry and physiological optics. 1982 Dec:59(12):983-6 [PubMed PMID: 7158656]
Zabaglo M, Leslie SW, Sharman T. Postoperative Wound Infections. StatPearls. 2025 Jan:(): [PubMed PMID: 32809368]
Mizukawa K, Kimura H, Fukai S, Tabuchi A. Classification of Duane's retraction syndrome: two additional electromyogram types. Japanese journal of ophthalmology. 2004 Mar-Apr:48(2):148-53 [PubMed PMID: 15060794]
Ashokan CS, Sreenivasan A, Saraswathy GK. Goldenhar syndrome - review with case series. Journal of clinical and diagnostic research : JCDR. 2014 Apr:8(4):ZD17-9. doi: 10.7860/JCDR/2014/7926.4260. Epub 2014 Apr 15 [PubMed PMID: 24959523]
Level 2 (mid-level) evidenceKassem IS, Miller MT, Archer SM. One Year of Pediatric Ophthalmology and Strabismus Research in Review. Asia-Pacific journal of ophthalmology (Philadelphia, Pa.). 2013 Nov-Dec:2(6):388-400. doi: 10.1097/APO.0000000000000019. Epub [PubMed PMID: 26107151]
Blöndal K, Sveinsdóttir H, Ingadottir B. Patients' expectations and experiences of provided surgery-related patient education: A descriptive longitudinal study. Nursing open. 2022 Sep:9(5):2495-2505. doi: 10.1002/nop2.1270. Epub 2022 Jun 5 [PubMed PMID: 35666048]
Ray A, Gurnani B. Pediatric Cataract. StatPearls. 2026 Jan:(): [PubMed PMID: 34283446]
Gurnani B, Feroze KB, Patel BC. Neurotrophic Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 28613758]
Kumar A, Sahu V, Misra S, Rathore V, Gurnani B, Kaur K. Changes in various ocular parameters of patients undergoing hemodialysis. European journal of ophthalmology. 2025 Nov:35(6):2235-2243. doi: 10.1177/11206721251349681. Epub 2025 Jun 18 [PubMed PMID: 40530962]
Gurnani B, Kaur K, Chaudhary S, Gandhi AS, Balakrishnan H, Mishra C, Gosalia H, Dhiman S, Joshi S, Nagtode AH, Jain S, Aguiar M, Rustagi IM. Nystagmus in Clinical Practice: From Diagnosis to Treatment-A Comprehensive Review. Clinical ophthalmology (Auckland, N.Z.). 2025:19():1617-1657. doi: 10.2147/OPTH.S523224. Epub 2025 May 17 [PubMed PMID: 40401036]
Aygit ED, Kocamaz M, Inal A, Fazil K, Ocak OB, Akar S, Gokyigit B. Management of Duane retraction syndrome with prismatic glasses. Clinical ophthalmology (Auckland, N.Z.). 2017:11():697-700. doi: 10.2147/OPTH.S124183. Epub 2017 Apr 12 [PubMed PMID: 28442887]
Atay G, Tellioğlu B, Tellioğlu HT, Avcı NB, Çınar BÇ, Şekeroğlu HT. Evaluation of auditory pathways and comorbid inner ear malformations in pediatric patients with Duane retraction syndrome. International journal of pediatric otorhinolaryngology. 2025 Jan:188():112207. doi: 10.1016/j.ijporl.2024.112207. Epub 2024 Dec 22 [PubMed PMID: 39732049]
Gurnani B, Kaur K, Chaudhary S, Kaur RP, Nayak S, Mishra D, Balakrishnan H, Parkash RO, Morya AK, Porwal A. Pediatric corneal transplantation: techniques, challenges, and outcomes. Therapeutic advances in ophthalmology. 2024 Jan-Dec:16():25158414241237906. doi: 10.1177/25158414241237906. Epub 2024 Mar 25 [PubMed PMID: 38533487]
Level 3 (low-level) evidenceKaur K, Muralikrishnan J, Hussaindeen JR, Deori N, Gurnani B. Impact of Covid-19 on Pediatric Ophthalmology Care: Lessons Learned. Pediatric health, medicine and therapeutics. 2023:14():309-321. doi: 10.2147/PHMT.S395349. Epub 2023 Oct 12 [PubMed PMID: 37849985]
Hakimeh C, Shahraki K, Courtois L, Suh DW. Surgical management of chronic sixth cranial nerve palsy: case report and literature review. Medical hypothesis, discovery & innovation ophthalmology journal. 2024:13(1):55-62. doi: 10.51329/mehdiophthal1494. Epub 2024 Jul 1 [PubMed PMID: 38978824]
Level 3 (low-level) evidence