 Antibiotic Prophylaxis in Dental and Oral Surgery Practice
Antibiotic Prophylaxis in Dental and Oral Surgery Practice
Introduction
Disruption of the dental mucosa, whether during routine procedures or oral surgery, permits oral microorganisms to enter the bloodstream, resulting in transient bacteremia.[1] This phenomenon has long been recognized as a potential precursor to infective endocarditis and other biofilm-associated infections, including prosthetic joint infections.[2][3]
The association between dental procedures and infective endocarditis was first proposed in 1923. By 1935, Streptococcus viridans had been isolated from the blood cultures of 61% of patients with dental sepsis.[4] Recognition of these risks prompted the American Heart Association (AHA) to include recommendations for antimicrobial prophylaxis before dental procedures in its 1955 guidelines.[5] Although antibiotics were historically prescribed broadly in dental practice, contemporary recommendations advocate a more selective approach, limiting prophylaxis to patients at the highest risk of infection.
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
The oral cavity harbors a diverse and dynamic microbiota that varies by anatomical location and systemic health conditions. Near tooth roots and within cracks and fissures, the microbial community is dominated by non–mutans streptococcal species, particularly those in the S mitis group. In contrast, mutans-group streptococci are present only in minimal numbers in a healthy oral environment.[6]
In periodontal disease, the microbial profile shifts toward a predominance of anaerobic organisms, including Porphyromonas, Prevotella, and Capnocytophaga species. Aggregatibacter species, notably A actinomycetemcomitans, are frequently associated with aggressive forms of periodontitis.[7] Microorganisms involved in periodontal pathology often organize into structured consortia or complexes alongside specific companion species. For instance, Fusobacterium species belong to a microbial complex that may represent an early indicator of periodontal disease progression.[8]
Dental caries are associated with a distinct microbial ecology characterized by dominance of mutans-group streptococci, Lactobacillus, and Actinomyces species within cariogenic biofilms.[9] In addition, Enterococcus species are commonly isolated from the oral cavity and may play a more significant role in oral and systemic infections than previously recognized.[10]
Several organisms of oral origin have been implicated in infective endocarditis. Oral streptococci account for approximately 7% to 18% of cases, enterococci for 5% to 10%, and members of the HACEK (Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, and Kingella) group—particularly oral anaerobes such as Eikenella corrodens and Aggregatibacter species—for 1% to 2%.[11] Similarly, microorganisms potentially originating from the oral cavity have been identified in prosthetic joint infections, with streptococcal species responsible for approximately 8% of cases, enterococci for 3%, and anaerobes for 4%.[12]
Staphylococcus aureus and coagulase-negative Staphylococcus species account for the majority of prosthetic joint infections and are typically uncommon residents of the oral microbiome. Emerging evidence suggests that staphylococcal species present in the oral cavity may contribute to oral and systemic infections more frequently than previously recognized.[13]
Issues of Concern
Current guidelines regarding antibiotic prophylaxis before dental procedures have been shaped primarily by 2 considerations: the characteristics of transient bacteremia and the demonstrated efficacy of antimicrobial prophylaxis in preventing bacteremia and infective endocarditis. These factors are discussed in detail below.
Transient Bacteremia
Bacteremia refers to the presence of viable microorganisms in the bloodstream. This phenomenon can occur during invasive dental procedures, during routine daily activities such as toothbrushing or chewing, or as a result of local infections of the oral cavity. Host immune defenses rapidly eliminate these microorganisms in most instances, preventing systemic complications. However, transient bacteremia may progress to clinically significant infection or sepsis when immune function is impaired or predisposing factors, such as structural heart defects, prosthetic materials, or turbulent cardiac blood flow, are present.[14]
Transient bacteremia occurs frequently in the general population during normal daily activities. Therefore, the widespread use of antimicrobial prophylaxis is not justified for all patients. Despite the frequent occurrence of bacteremia, infective endocarditis remains relatively uncommon, with an estimated incidence of only 3 to 10 cases per 100,000 individuals annually. Patients with specific cardiac conditions, such as rheumatic heart disease, degenerative or prosthetic valve disease, and congenital heart defects, carry a substantially greater risk for developing endocarditis.
Advances in cardiac surgery and prosthetic valve technology have improved outcomes for these patients but have also been associated with higher rates of prosthetic valve–related endocarditis.[15] Consequently, these higher-risk populations are more likely to benefit from targeted antibiotic prophylaxis prior to dental procedures.
Efficacy of Antimicrobial Prophylaxis in the Prevention of Bacteremia and Infective Endocarditis
Antimicrobial prophylaxis before dental procedures can reduce the risk of bacteremia, but it does not guarantee complete protection. A systematic review of 12 studies found that preprocedural antibiotic administration decreased the incidence of postextraction bacteremia by approximately 50%. Specifically, amoxicillin reduced the risk by 59%, azithromycin by 49%, and clindamycin by 11%.[16] These findings indicate that antibiotics can lessen the bacterial load introduced into the bloodstream, but they do not eliminate bacteremia entirely.
Infective endocarditis is a microbial infection of the heart’s endocardial surface, typically involving cardiac valves, prosthetic materials, or implanted cardiac devices.[17] No randomized controlled trials have directly assessed the effectiveness of antimicrobial prophylaxis prior to dental procedures in preventing endocarditis. Evidence is largely derived from epidemiologic studies comparing infection rates before and after major changes in professional guidelines.
Several studies have reported no significant change in the incidence of infective endocarditis following the narrowing of prophylactic recommendations. A 2007 study conducted in Olmstead County, Minnesota, observed no difference in the incidence of viridans group streptococcal endocarditis before and after the 2007 joint guideline revisions issued by the AHA and the American Dental Association (ADA), which restricted prophylaxis to high-risk patients.[18] Similarly, a nationwide French study found no increase in endocarditis incidence after the 2002 guideline changes that limited antibiotic use prior to dental procedures.[19]
Conversely, some investigations have documented an upward trend in endocarditis rates following these policy revisions. A US study reported an increase in cases of streptococcal infective endocarditis after the 2007 AHA/ADA recommendations, without a corresponding rise in valve replacement surgeries.[20] In England, a population-based analysis revealed a higher incidence of infective endocarditis after the 2008 National Institute for Health and Clinical Excellence (NICE) guidelines, which initially advised against antibiotic prophylaxis for all patient groups.[21] In response, the NICE guidelines were updated in 2016 to indicate that prophylaxis is not routinely recommended before dental procedures, while allowing individualized clinical judgment for high-risk cases.[22]
Clinical Significance
Antimicrobial prophylaxis is not routinely indicated for healthy patients undergoing dental or oral surgery procedures. However, specific high-risk patients may benefit from this intervention by reducing the likelihood of postoperative complications, including implant failure, local infection, or sinusitis. Prophylaxis is recommended for dental procedures involving manipulation of gingival tissue, periapical surgery, or perforation of the oral mucosa in high-risk patients.[23]
Indications for Antimicrobial Prophylaxis in Healthy Patients Receiving Dental Implants
The current consensus in the medical literature recommends a single preoperative dose of antibiotics for routine dental implant placement in healthy patients. The most widely supported regimen is 2 grams of amoxicillin administered orally 1 hour prior to surgery. This recommendation is based on moderate-quality evidence from randomized controlled trials and systematic reviews, demonstrating a reduction in early implant failures with this protocol. Postoperative antibiotic courses do not provide additional benefit and are not justified in straightforward cases.[24]
Alternatives such as clindamycin or azithromycin are commonly used in patients with a penicillin allergy, although the supporting evidence for these agents is less robust.[25] The AHA specifically recommends a single 2-gram oral dose of amoxicillin for endocarditis prophylaxis in at-risk patients, with clindamycin or azithromycin as alternatives for individuals allergic to penicillin. Professional consensus, including guidance from the Italian Academy of Osseointegration, advocates for a single preoperative dose for routine cases, reserving extended regimens for complex procedures, including interventions requiring prolonged surgical time or bone regeneration. Preoperative and postoperative chlorhexidine rinses are recommended to further reduce bacterial load. Despite these recommendations, survey data show that many clinicians prescribe antibiotic regimens that exceed the recommended duration or extend across the perioperative period. Such practices violate evidence-based guidelines and may contribute to antimicrobial resistance.[26][27] In summary, the recommended antibiotic regimen for dental implant placement in healthy patients is a single 2-gram oral dose of amoxicillin administered 1 hour preoperatively. Prolonged or postoperative antibiotic use is not supported for routine cases.
A single preoperative dose of amoxicillin (2 grams orally, 1 hour before surgery) is recommended for dental implant placement with concurrent sinus lift in healthy patients, as supported by systematic reviews and consensus guidelines.[28] Evidence does not support the superiority of extended (postoperative) antibiotic regimens or any specific protocol for sinus lift procedures. Postoperative antibiotics may be considered in complex cases, such as those involving membrane perforation, prolonged surgery, or patient immunosuppression, but are not routinely justified.
Amoxicillin, amoxicillin-clavulanate, and ciprofloxacin are highly effective against the bacteria encountered during sinus elevation. For patients allergic to penicillin, alternatives may include clindamycin or azithromycin.[29]
Despite these recommendations, many clinicians continue to prescribe antibiotics beyond evidence-based guidance, highlighting a persistent gap between guidelines and clinical practice. Data on infection rates and optimal prophylaxis specifically for sinus lift procedures remain limited, and further research is necessary to define best practices in this context.[30]
Indications for Antimicrobial Prophylaxis in Healthy Patients with Facial Fractures
Infection rates for mandibular fractures range from 3.3% to 43.9%, whereas infections of upper facial, midface, and third fractures occur in 0% to 12.5%.[31] Antimicrobials are generally administered to prevent hardware-associated infections in these cases.[32] Prophylactic antibiotics are indicated for open or contaminated facial fractures, including open mandibular fractures and fractures that communicate with the oral cavity, and should be limited to 24 hours or less. Consensus guidelines and systematic reviews support this approach, demonstrating that short-course prophylaxis is effective, whereas prolonged antibiotic regimens do not reduce infection risk and may increase the likelihood of adverse events.
Antimicrobial Prophylaxis in Special Populations
Severely immunocompromised patients, such as those receiving chemotherapy, should avoid invasive dental procedures whenever possible. When such procedures are necessary, dentists and oral surgeons should consult the patient’s managing physician.[33] Evidence remains insufficient for patients with severe neutropenia, high-dose immunosuppressant therapy, or primary immunodeficiencies.[34]
When prophylaxis is indicated in immunocompromised patients, a preoperative antibiotic regimen is recommended to reduce the risk of postoperative infection. This regimen typically involves administering 2 to 3 grams of amoxicillin approximately 1 hour before surgery. Amoxicillin–clavulanate may be used in cases that require broader antimicrobial coverage to target dental pathogenic bacteria, including β-lactamase–producing organisms. Extended antibiotic coverage may be considered due to an elevated risk of infection, although the optimal duration of therapy remains unclear.
For patients with penicillin allergies, cephalosporins may be appropriate if no history of anaphylaxis is elicited. Azithromycin or doxycycline may be selected in accordance with AHA guidance. Chlorhexidine mouth rinses administered before and after surgery are recommended as an adjunctive measure to further reduce the microbial load.[35]
Previous guidelines recommended antimicrobial prophylaxis for patients with diabetes mellitus.[36] However, a recent systematic review found that guideline recommendations were inconsistent and identified no evidence supporting the effectiveness of prophylaxis in this population.[37]
Use of prophylaxis should balance potential benefits in infection prevention against risks of adverse effects, antimicrobial resistance, and microbiome disruption. Consultation with the patient’s clinicians is advisable to assess the current immune status and infection risk.[38]
The ADA does not routinely recommend antimicrobial prophylaxis for patients with implanted prosthetic joints prior to dental procedures.[39] Similarly, the American Academy of Orthopedic Surgeons does not recommend prophylaxis, citing a lack of evidence linking dental procedure–induced bacteremia to prosthetic joint infection. To date, no study has demonstrated that antimicrobial prophylaxis reduces the rate of prosthetic joint infection.
Indications for Antimicrobial Prophylaxis in Patients with Cardiac Risk Factors
Due to the elevated risk of infective endocarditis in patients with specific cardiac conditions, the AHA recommends antimicrobial prophylaxis before selected dental procedures for patients who meet any of the criteria listed below.:
- Presence of a prosthetic valve or implanted prosthetic cardiac material: This definition includes prosthetic valves, prosthetic material from prior cardiac valve repair, or other prosthetic material in situ, such as transvenous aortic valve replacements. This criterion also includes patients with a left ventricular assist device or artificial heart.
- History of infective endocarditis.
- Congenital heart disease with specific conditions: This includes unrepaired cyanotic congenital defects, repaired defects with prosthetic material within 6 months of repair, corrected defects with a retained prosthetic device and residual defects, and the presence of a pulmonary artery valve or conduit.
- Cardiac transplant with valvulopathy.
In patients who do not meet the criteria outlined above, the AHA does not recommend antimicrobial prophylaxis for infective endocarditis prior to dental procedures.[40] Examples of such conditions include:
- Use of pacemakers or automatic cardioverter-defibrillators
- Prior septal defect closure with successful repair
- Presence of peripheral vascular grafts (eg, for hemodialysis access) or vascular stents
- Presence of ventriculoatrial shunts
- Presence of vena cava filters
- Presence of pledgets
Dental procedures that carry sufficient risk to justify antimicrobial prophylaxis in the high-risk groups described above typically involve gingival or periapical manipulation or perforation of the oral mucosa. Examples of high- and low-risk procedures are outlined in the table below.[41][42] This list is not exhaustive, and each case should be evaluated individually by the treating clinician (see Image. Antibiotic Prophylaxis).
Table. Dental Procedures and Indications for Antibiotic Prophylaxis in Patients With Specific Cardiac Risk Factors
| Dental procedures warranting antibiotic prophylaxis | Dental procedures not warranting antibiotic prophylaxis |
| Periodontal procedures, including scaling and root planing, subgingival antibiotic strip placement, bone grafting, gingivectomy, gingivoplasty, gingival grafts, and periodontal flap surgery | Oral impressions, radiographs, and rubber dam placement |
| Endodontic instrumentation beyond the apical foramen and apicoectomy | Intracanal endodontic treatment confined to the pulp chamber |
| Dental implant placement | Restorative dentistry with or without retraction cord |
| Reimplantation of avulsed teeth | Physiologic shedding of primary teeth |
| Intraligamentary local anesthetic injections | Non-ligamentary local anesthetic injections |
| Dental cleaning procedures where bleeding is anticipated | Placement of removable prosthodontic or orthodontic appliances |
| – | Postoperative suture removal |
Antimicrobials should be administered as a single dose 30 to 60 minutes prior to the procedure. The preferred regimen for adults is 2 grams of amoxicillin administered orally, whereas pediatric dosing is 50 mg/kg. For patients unable to take oral medications, ampicillin 2 grams may be administered intravenously or intramuscularly.
Alternative regimens for adults with penicillin allergy include cephalexin 2 grams, azithromycin 500 mg, clarithromycin 500 mg, and doxycycline 100 mg. Pediatric alternatives for penicillin-allergic patients include cephalexin 50 mg/kg, azithromycin or clarithromycin 15 mg/kg, and doxycycline 2.2 mg/kg for patients with a body weight of less than 45 kg, or 100 mg for patients with a body weight of 45 kg or more.
Cephalexin is contraindicated in patients with type I hypersensitivity to penicillins and a history of anaphylaxis, angioedema, or urticaria. Alternative agents include azithromycin, clarithromycin, or doxycycline. For patients with a history of type I immunoglobulin E–mediated penicillin allergy who cannot take oral medications, recommended regimens include cefazolin or ceftriaxone 1 gram intravenously or intramuscularly in adults, and 50 mg/kg intravenously or intramuscularly in children.
Clindamycin is not recommended for antibiotic prophylaxis prior to dental procedures or oral surgery due to a high incidence of adverse events, including Clostridioides difficile colitis. C difficile infection may range from asymptomatic carriage to life-threatening colitis, which can result in toxic megacolon—a condition that may require surgical intervention or cause death. High recurrence rates further complicate the treatment and management of this infection.[43]
Other Issues
Antimicrobial Stewardship in Dentistry and Oral Surgery
Dentists account for 10% of all outpatient antibiotic prescriptions and prescribe more antibiotics than any other specialty in the United States.[44] Therefore, increased attention to antimicrobial stewardship in dentistry and oral surgery could have a substantial impact.
A study evaluating antibiotic prophylaxis at 168,420 dental visits in the United States between 2011 and 2015 found that only 19.1% of these prescriptions were concordant with guidelines.[45] The study reported that 1.4% of prescriptions were associated with an adverse event within 14 days. Emergency room visits accounted for 83% of these events, whereas antibiotic allergy accounted for 16%. C difficile colitis occurred at a rate of 0.007 per 1000 patient days, and anaphylaxis at a rate of 0.003 per 1000 person days.[46] Although these events affected only a small proportion of patients who received unnecessary antibiotic prophylaxis, they were entirely preventable by compliance with current guidelines.
Unnecessary use of antimicrobials contributes to the development of antibiotic resistance, which poses a growing threat to public health. In the United States alone, antibiotic-resistant bacteria cause approximately 23,000 deaths annually.[47]
Dentists working in academic hospitals or university settings demonstrated higher adherence to guideline-directed antibiotic prophylaxis than those practicing in other settings. Dentists with 15 or more years of practice were more likely to deviate from recommended prophylaxis guidelines.[48] Increased education regarding the risks of antibiotic-related adverse events, including C difficile colitis and antimicrobial resistance, may improve prescribing practices. A small prospective cohort study showed that outreach by infectious diseases antimicrobial stewardship personnel to private practice dentists reported an increase in appropriate antibiotic prescribing from 19% before education to 87.9% after education.[49]
Enhancing Healthcare Team Outcomes
Appropriate antimicrobial prophylaxis involves coordination across the entire healthcare team, including dentists, oral and orthopedic surgeons, infectious disease specialists, cardiologists, primary care physicians, and pharmacists. Dentists play a central role in the prescribing of antimicrobial prophylaxis.
In 2014, a panel of experts developed the ADA guidelines on antibiotic prophylaxis before dental procedures to prevent prosthetic joint infection. Impediments to guideline-adherent prescribing include incomplete information regarding patients’ cardiac histories at the time of dental procedures, pressure from other physicians or patients to prescribe antibiotics, and insufficient education on current recommendations. The current AHA guidelines for infective endocarditis prophylaxis were developed following an exhaustive review of all available data.
Cardiologists play a crucial role in advising patients and dentists regarding the need for antimicrobial prophylaxis before dental procedures and oral surgery. Orthopedic surgeons contribute by guiding patients with implanted prosthetic joints. Primary care providers are also involved because patients frequently inquire about prophylaxis prior to dental visits.
Infectious disease physicians provide guidance to both patients and other healthcare providers and contribute significantly to education and outreach. Pharmacists assist in antimicrobial selection for complex cases, such as patients with antibiotic allergies, while antimicrobial stewardship pharmacists support appropriate prescribing through outreach and education. Many physicians, surgeons, and pharmacists further advance knowledge on this subject through research.
As multiple healthcare professionals are often involved alongside the dentist or oral surgeon, all members of the patient’s care team must deliver consistent guidance and education. Clear and consistent guidance helps prevent antibiotic overprescribing, reduces the risk of antimicrobial resistance, and avoids unnecessary adverse events when prophylaxis provides no benefit.
Media
(Click Image to Enlarge)
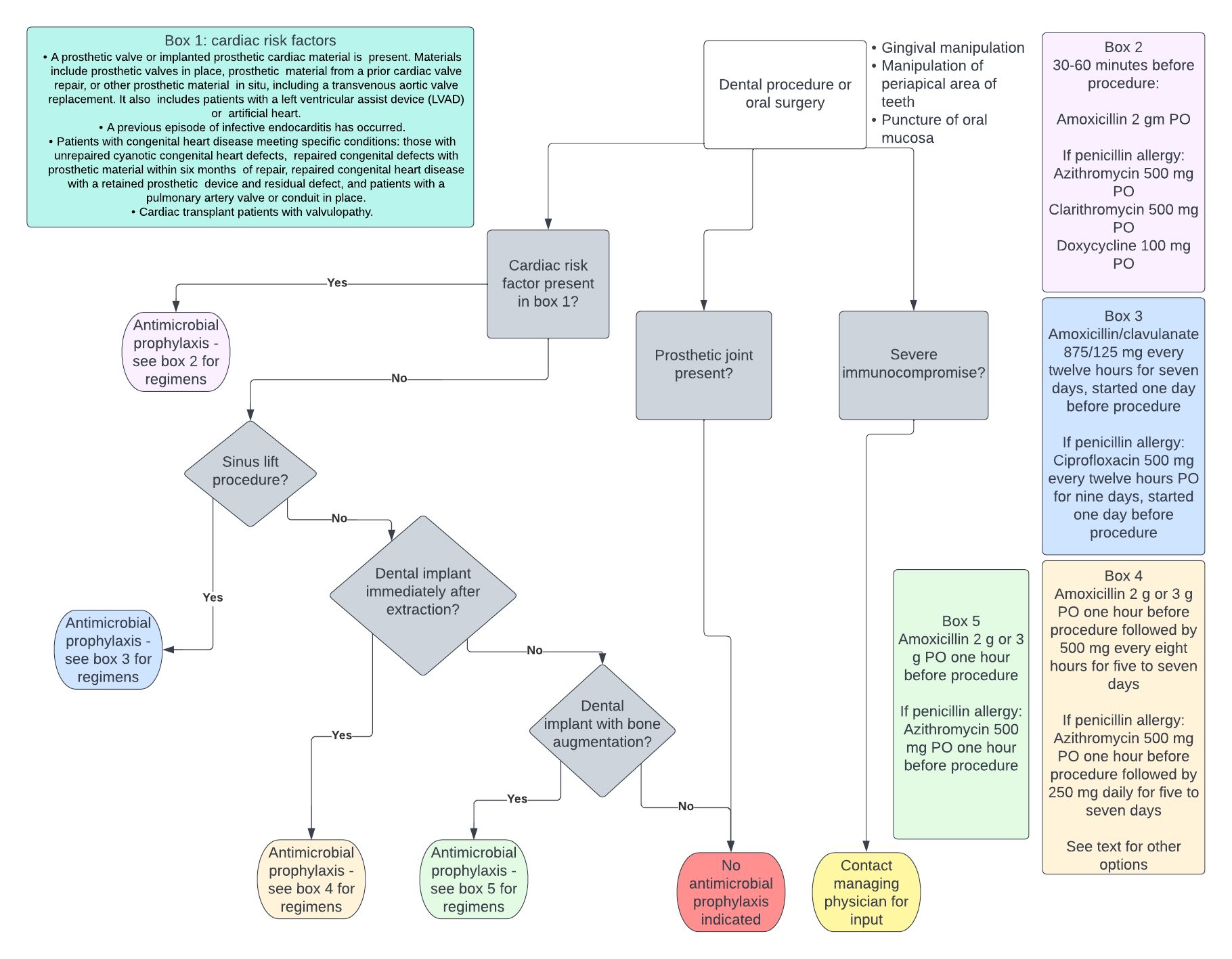
Antibiotic Prophylaxis. The figure shows a flowchart outlining the decision-making process for antibiotic prophylaxis before dental and oral surgery procedures.
Contributed by CM Hollingshead, MD
References
Carroll GC, Sebor RJ. Dental flossing and its relationship to transient bacteremia. Journal of periodontology. 1980 Dec:51(12):691-2 [PubMed PMID: 6937641]
Andersen MH, Holle SLK, Klein CF, Bruun NE, Arpi M, Bundgaard H, Tønder N, Iversen KK. Risk for infective endocarditis in bacteremia with Gram positive cocci. Infection. 2020 Dec:48(6):905-912. doi: 10.1007/s15010-020-01504-6. Epub 2020 Aug 25 [PubMed PMID: 32844380]
Honkanen M, Jämsen E, Karppelin M, Huttunen R, Eskelinen A, Syrjänen J. Periprosthetic Joint Infections as a Consequence of Bacteremia. Open forum infectious diseases. 2019 Jun:6(6):ofz218. doi: 10.1093/ofid/ofz218. Epub 2019 May 7 [PubMed PMID: 31214625]
Dayer M, Thornhill M. Is antibiotic prophylaxis to prevent infective endocarditis worthwhile? Journal of infection and chemotherapy : official journal of the Japan Society of Chemotherapy. 2018 Jan:24(1):18-24. doi: 10.1016/j.jiac.2017.10.006. Epub 2017 Oct 26 [PubMed PMID: 29107651]
. PREVENTION of rheumatic fever and bacterial endocarditis through control of streptococcal infections. Modern concepts of cardiovascular disease. 1956 Dec:25(12 Suppl):365-9 [PubMed PMID: 13387501]
Patil S, Rao RS, Sanketh DS, Amrutha N. Microbial flora in oral diseases. The journal of contemporary dental practice. 2013 Nov 1:14(6):1202-8 [PubMed PMID: 24858777]
Fine DH, Markowitz K, Furgang D, Fairlie K, Ferrandiz J, Nasri C, McKiernan M, Gunsolley J. Aggregatibacter actinomycetemcomitans and its relationship to initiation of localized aggressive periodontitis: longitudinal cohort study of initially healthy adolescents. Journal of clinical microbiology. 2007 Dec:45(12):3859-69 [PubMed PMID: 17942658]
Level 2 (mid-level) evidenceSocransky SS, Haffajee AD, Cugini MA, Smith C, Kent RL Jr. Microbial complexes in subgingival plaque. Journal of clinical periodontology. 1998 Feb:25(2):134-44 [PubMed PMID: 9495612]
Struzycka I. The oral microbiome in dental caries. Polish journal of microbiology. 2014:63(2):127-35 [PubMed PMID: 25115106]
Level 3 (low-level) evidenceKomiyama EY, Lepesqueur LS, Yassuda CG, Samaranayake LP, Parahitiyawa NB, Balducci I, Koga-Ito CY. Enterococcus Species in the Oral Cavity: Prevalence, Virulence Factors and Antimicrobial Susceptibility. PloS one. 2016:11(9):e0163001. doi: 10.1371/journal.pone.0163001. Epub 2016 Sep 15 [PubMed PMID: 27631785]
Selton-Suty C, Célard M, Le Moing V, Doco-Lecompte T, Chirouze C, Iung B, Strady C, Revest M, Vandenesch F, Bouvet A, Delahaye F, Alla F, Duval X, Hoen B, AEPEI Study Group. Preeminence of Staphylococcus aureus in infective endocarditis: a 1-year population-based survey. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2012 May:54(9):1230-9. doi: 10.1093/cid/cis199. Epub [PubMed PMID: 22492317]
Level 3 (low-level) evidenceTande AJ, Patel R. Prosthetic joint infection. Clinical microbiology reviews. 2014 Apr:27(2):302-45. doi: 10.1128/CMR.00111-13. Epub [PubMed PMID: 24696437]
Smith AJ, Jackson MS, Bagg J. The ecology of Staphylococcus species in the oral cavity. Journal of medical microbiology. 2001 Nov:50(11):940-946. doi: 10.1099/0022-1317-50-11-940. Epub [PubMed PMID: 11699589]
Christaki E, Giamarellos-Bourboulis EJ. The complex pathogenesis of bacteremia: from antimicrobial clearance mechanisms to the genetic background of the host. Virulence. 2014 Jan 1:5(1):57-65. doi: 10.4161/viru.26514. Epub 2013 Sep 25 [PubMed PMID: 24067507]
Cahill TJ, Prendergast BD. Infective endocarditis. Lancet (London, England). 2016 Feb 27:387(10021):882-93. doi: 10.1016/S0140-6736(15)00067-7. Epub 2015 Sep 1 [PubMed PMID: 26341945]
Lafaurie GI, Noriega LA, Torres CC, Castillo Y, Moscoso SB, Mosquera S, Díaz-Báez D, Chambrone L. Impact of antibiotic prophylaxis on the incidence, nature, magnitude, and duration of bacteremia associated with dental procedures: A systematic review. Journal of the American Dental Association (1939). 2019 Nov:150(11):948-959.e4. doi: 10.1016/j.adaj.2019.06.017. Epub 2019 Sep 25 [PubMed PMID: 31561837]
Level 1 (high-level) evidenceHubers SA, DeSimone DC, Gersh BJ, Anavekar NS. Infective Endocarditis: A Contemporary Review. Mayo Clinic proceedings. 2020 May:95(5):982-997. doi: 10.1016/j.mayocp.2019.12.008. Epub 2020 Apr 13 [PubMed PMID: 32299668]
Desimone DC, Tleyjeh IM, Correa de Sa DD, Anavekar NS, Lahr BD, Sohail MR, Steckelberg JM, Wilson WR, Baddour LM, Mayo Cardiovascular Infections Study Group. Incidence of infective endocarditis caused by viridans group streptococci before and after publication of the 2007 American Heart Association's endocarditis prevention guidelines. Circulation. 2012 Jul 3:126(1):60-4. doi: 10.1161/CIRCULATIONAHA.112.095281. Epub 2012 Jun 11 [PubMed PMID: 22689929]
Duval X, Delahaye F, Alla F, Tattevin P, Obadia JF, Le Moing V, Doco-Lecompte T, Celard M, Poyart C, Strady C, Chirouze C, Bes M, Cambau E, Iung B, Selton-Suty C, Hoen B, AEPEI Study Group. Temporal trends in infective endocarditis in the context of prophylaxis guideline modifications: three successive population-based surveys. Journal of the American College of Cardiology. 2012 May 29:59(22):1968-76. doi: 10.1016/j.jacc.2012.02.029. Epub [PubMed PMID: 22624837]
Level 2 (mid-level) evidencePant S, Patel NJ, Deshmukh A, Golwala H, Patel N, Badheka A, Hirsch GA, Mehta JL. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. Journal of the American College of Cardiology. 2015 May 19:65(19):2070-6. doi: 10.1016/j.jacc.2015.03.518. Epub [PubMed PMID: 25975469]
Dayer MJ, Jones S, Prendergast B, Baddour LM, Lockhart PB, Thornhill MH. Incidence of infective endocarditis in England, 2000-13: a secular trend, interrupted time-series analysis. Lancet (London, England). 2015 Mar 28:385(9974):1219-28. doi: 10.1016/S0140-6736(14)62007-9. Epub 2014 Nov 18 [PubMed PMID: 25467569]
Level 2 (mid-level) evidenceThornhill MH, Dayer M, Lockhart PB, McGurk M, Shanson D, Prendergast B, Chambers JB. A change in the NICE guidelines on antibiotic prophylaxis. British dental journal. 2016 Aug 12:221(3):112-4. doi: 10.1038/sj.bdj.2016.554. Epub [PubMed PMID: 27514339]
Khouly I, Braun RS, Chambrone L. Antibiotic prophylaxis may not be indicated for prevention of dental implant infections in healthy patients. A systematic review and meta-analysis. Clinical oral investigations. 2019 Apr:23(4):1525-1553. doi: 10.1007/s00784-018-2762-x. Epub 2019 Mar 1 [PubMed PMID: 30824982]
Level 1 (high-level) evidenceLund B, Hultin M, Tranaeus S, Naimi-Akbar A, Klinge B. Complex systematic review - Perioperative antibiotics in conjunction with dental implant placement. Clinical oral implants research. 2015 Sep:26 Suppl 11():1-14. doi: 10.1111/clr.12637. Epub 2015 Jun 16 [PubMed PMID: 26080862]
Level 1 (high-level) evidenceTabrizi R, Mobin F, Dehghanpour M, Torabi ZS. Comparison of three antibiotic protocols for prevention of infection in dental implant surgery: A randomized clinical trial. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2022 Apr:50(4):293-297. doi: 10.1016/j.jcms.2022.03.003. Epub 2022 Mar 31 [PubMed PMID: 35387739]
Level 1 (high-level) evidenceCaiazzo A, Canullo L, Consensus Meeting Group, Pesce P. Consensus Report by the Italian Academy of Osseointegration on the Use of Antibiotics and Antiseptic Agents in Implant Surgery. The International journal of oral & maxillofacial implants. 2021 Jan-Feb:36(1):103-105. doi: 10.11607/jomi.8264. Epub [PubMed PMID: 33600529]
Level 3 (low-level) evidenceBernabeu-Mira JC, Peñarrocha-Diago M, Peñarrocha-Oltra D. Prescription of Antibiotic Prophylaxis for Dental Implant Surgery in Healthy Patients: A Systematic Review of Survey-Based Studies. Frontiers in pharmacology. 2020:11():588333. doi: 10.3389/fphar.2020.588333. Epub 2021 Feb 10 [PubMed PMID: 33643035]
Level 1 (high-level) evidenceMomand P, Becktor JP, Naimi-Akbar A, Tobin G, Götrick B. Effect of antibiotic prophylaxis in dental implant surgery: A multicenter placebo-controlled double-blinded randomized clinical trial. Clinical implant dentistry and related research. 2022 Feb:24(1):116-124. doi: 10.1111/cid.13068. Epub 2022 Jan 24 [PubMed PMID: 35075765]
Level 1 (high-level) evidenceCarreño Carreño J, Gómez-Moreno G, Aguilar-Salvatierra A, Martínez Corriá R, Menéndez López-Mateos ML, Menéndez-Núñez M. The antibiotic of choice determined by antibiogram in maxillary sinus elevation surgery: a clinical study. Clinical oral implants research. 2018 Nov:29(11):1070-1076. doi: 10.1111/clr.12835. Epub 2016 Mar 19 [PubMed PMID: 26992460]
Salgado-Peralvo ÁO, Garcia-Sanchez A, Kewalramani N, Romandini M, Velasco-Ortega E. Preventive Antibiotic Therapy in Sinus Elevation Procedures: A Systematic Review. The International journal of oral & maxillofacial implants. 2023 Jan-Feb:38(1):19-28. doi: 10.11607/jomi.9930. Epub [PubMed PMID: 37099582]
Level 1 (high-level) evidenceGoormans F, Coropciuc R, Vercruysse M, Spriet I, Willaert R, Politis C. Systemic Antibiotic Prophylaxis in Maxillofacial Trauma: A Scoping Review and Critical Appraisal. Antibiotics (Basel, Switzerland). 2022 Apr 5:11(4):. doi: 10.3390/antibiotics11040483. Epub 2022 Apr 5 [PubMed PMID: 35453234]
Level 2 (mid-level) evidenceChoi SH, Lee JH. Absorbable Plate-Related Infection after Facial Bone Fracture Reduction. Archives of craniofacial surgery. 2016 Mar:17(1):1-4. doi: 10.7181/acfs.2016.17.1.1. Epub 2016 Mar 21 [PubMed PMID: 28913243]
Elad S, Raber-Durlacher JE, Brennan MT, Saunders DP, Mank AP, Zadik Y, Quinn B, Epstein JB, Blijlevens NM, Waltimo T, Passweg JR, Correa ME, Dahllöf G, Garming-Legert KU, Logan RM, Potting CM, Shapira MY, Soga Y, Stringer J, Stokman MA, Vokurka S, Wallhult E, Yarom N, Jensen SB. Basic oral care for hematology-oncology patients and hematopoietic stem cell transplantation recipients: a position paper from the joint task force of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) and the European Society for Blood and Marrow Transplantation (EBMT). Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer. 2015 Jan:23(1):223-36. doi: 10.1007/s00520-014-2378-x. Epub 2014 Sep 5 [PubMed PMID: 25189149]
de Leeuw K, Bootsma H, Middel A, Vissink A. [Antibiotic prophylaxis and immune-compromised patients]. Nederlands tijdschrift voor tandheelkunde. 2019 Oct:126(10):521-525. doi: 10.5177/ntvt.2019.10.19065. Epub [PubMed PMID: 31613281]
Taplitz RA, Kennedy EB, Bow EJ, Crews J, Gleason C, Hawley DK, Langston AA, Nastoupil LJ, Rajotte M, Rolston KV, Strasfeld L, Flowers CR. Antimicrobial Prophylaxis for Adult Patients With Cancer-Related Immunosuppression: ASCO and IDSA Clinical Practice Guideline Update. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2018 Oct 20:36(30):3043-3054. doi: 10.1200/JCO.18.00374. Epub 2018 Sep 4 [PubMed PMID: 30179565]
Level 1 (high-level) evidenceGutiérrez JL, Bagán JV, Bascones A, Llamas R, Llena J, Morales A, Noguerol B, Planells P, Prieto J, Salmerón JI. Consensus document on the use of antibiotic prophylaxis in dental surgery and procedures. Medicina oral, patologia oral y cirugia bucal. 2006 Mar 1:11(2):E188-205 [PubMed PMID: 16505802]
Level 3 (low-level) evidenceSykara M, Maniatakos P, Tentolouris A, Karoussis IK, Tentolouris N. The necessity of administrating antibiotic prophylaxis to patients with diabetes mellitus prior to oral surgical procedures-a systematic review. Diabetes & metabolic syndrome. 2022 Oct:16(10):102621. doi: 10.1016/j.dsx.2022.102621. Epub 2022 Sep 24 [PubMed PMID: 36183455]
Level 1 (high-level) evidenceTaplitz RA, Kennedy EB, Flowers CR. Antimicrobial Prophylaxis for Adult Patients With Cancer-Related Immunosuppression: ASCO and IDSA Clinical Practice Guideline Update Summary. Journal of oncology practice. 2018 Nov:14(11):692-695. doi: 10.1200/JOP.18.00366. Epub 2018 Sep 4 [PubMed PMID: 30179525]
Level 1 (high-level) evidenceSollecito TP, Abt E, Lockhart PB, Truelove E, Paumier TM, Tracy SL, Tampi M, Beltrán-Aguilar ED, Frantsve-Hawley J. The use of prophylactic antibiotics prior to dental procedures in patients with prosthetic joints: Evidence-based clinical practice guideline for dental practitioners--a report of the American Dental Association Council on Scientific Affairs. Journal of the American Dental Association (1939). 2015 Jan:146(1):11-16.e8. doi: 10.1016/j.adaj.2014.11.012. Epub 2014 Dec 18 [PubMed PMID: 25569493]
Level 1 (high-level) evidenceWilson WR, Gewitz M, Lockhart PB, Bolger AF, DeSimone DC, Kazi DS, Couper DJ, Beaton A, Kilmartin C, Miro JM, Sable C, Jackson MA, Baddour LM, American Heart Association Young Hearts Rheumatic Fever, Endocarditis and Kawasaki Disease Committee of the Council on Lifelong Congenital Heart Disease and Heart Health in the Young; Council on Cardiovascular and Stroke Nursing; and the Council on Quality of Care and Outcomes Research. Prevention of Viridans Group Streptococcal Infective Endocarditis: A Scientific Statement From the American Heart Association. Circulation. 2021 May 18:143(20):e963-e978. doi: 10.1161/CIR.0000000000000969. Epub 2021 Apr 15 [PubMed PMID: 33853363]
Level 2 (mid-level) evidenceSung S, Kim EH, Kwon JW, Lee JS, Lee SB, Moon SH, Lee HM, Jung I, Lee BH. Invasive dental procedures as risk factors for postoperative spinal infection and the effect of antibiotic prophylaxis. Journal of clinical periodontology. 2021 Sep:48(9):1270-1280. doi: 10.1111/jcpe.13514. Epub 2021 Jul 8 [PubMed PMID: 34189757]
Ito HO. Infective endocarditis and dental procedures: evidence, pathogenesis, and prevention. The journal of medical investigation : JMI. 2006 Aug:53(3-4):189-98 [PubMed PMID: 16953053]
Czepiel J, Dróżdż M, Pituch H, Kuijper EJ, Perucki W, Mielimonka A, Goldman S, Wultańska D, Garlicki A, Biesiada G. Clostridium difficile infection: review. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology. 2019 Jul:38(7):1211-1221. doi: 10.1007/s10096-019-03539-6. Epub 2019 Apr 3 [PubMed PMID: 30945014]
Hicks LA, Bartoces MG, Roberts RM, Suda KJ, Hunkler RJ, Taylor TH Jr, Schrag SJ. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2015 May 1:60(9):1308-16. doi: 10.1093/cid/civ076. Epub 2015 Mar 5 [PubMed PMID: 25747410]
Suda KJ, Calip GS, Zhou J, Rowan S, Gross AE, Hershow RC, Perez RI, McGregor JC, Evans CT. Assessment of the Appropriateness of Antibiotic Prescriptions for Infection Prophylaxis Before Dental Procedures, 2011 to 2015. JAMA network open. 2019 May 3:2(5):e193909. doi: 10.1001/jamanetworkopen.2019.3909. Epub 2019 May 3 [PubMed PMID: 31150071]
Gross AE, Suda KJ, Zhou J, Calip GS, Rowan SA, Hershow RC, Perez R, Evans CT, McGregor JC. Serious antibiotic-related adverse effects following unnecessary dental prophylaxis in the United States. Infection control and hospital epidemiology. 2021 Jan:42(1):110-112. doi: 10.1017/ice.2020.1261. Epub 2020 Nov 11 [PubMed PMID: 33172505]
Brinkac L, Voorhies A, Gomez A, Nelson KE. The Threat of Antimicrobial Resistance on the Human Microbiome. Microbial ecology. 2017 Nov:74(4):1001-1008. doi: 10.1007/s00248-017-0985-z. Epub 2017 May 11 [PubMed PMID: 28492988]
Šutej I, Par M, Lepur D, Peroš K, Pintarić H, Alajbeg I, Vuger L. Dentists' practice and compliance with current guidelines of infective endocarditis prophylaxis- National survey study. Journal of clinical and experimental dentistry. 2021 Jul:13(7):e648-e652. doi: 10.4317/jced.58054. Epub 2021 Jul 1 [PubMed PMID: 34306527]
Level 3 (low-level) evidenceGoff DA, Mangino JE, Trolli E, Scheetz R, Goff D. Private Practice Dentists Improve Antibiotic Use After Dental Antibiotic Stewardship Education From Infectious Diseases Experts. Open forum infectious diseases. 2022 Aug:9(8):ofac361. doi: 10.1093/ofid/ofac361. Epub 2022 Jul 25 [PubMed PMID: 35959211]