Introduction
The basic concept of echocardiography was first demonstrated by Lazzaro Spallanzani in the 18 century when he described the reflected echoes of inaudible sound.[1] Hertz and Edler reported the first use of ultrasound in the cardiac evaluation and continuous monitoring of heart movements in 1954.[2] They used an industrial ultrasonic flaw detector and obtained time-varying echoes transcutaneously from the heart. The assessment of the mitral valve with the help of M-mode was the first clinical application of an echocardiogram.[3]
Since then, echocardiography has expanded tremendously and exponentially over the decades and has become an integral part of cardiac evaluation.[4] Although echocardiography started with B-mode, with the discovery of new technologies, including Doppler and 3-dimensional imaging, the echocardiographic examination has progressively become longer and more comprehensive.[5][6]
With the advent of echocardiographic contrast media and transesophageal probes, the sensitivity of echocardiographic examination has improved significantly, and it has become an important part of cardiac surgical procedures involving valvular reconstruction.[7][8]
In some aspects, new technologies have completely replaced old methods. In other circumstances, new technologies have been incorporated to enhance existing capabilities. Even in the contemporary era of newer imaging modalities, an echocardiogram is recommended as the first choice for structural and functional assessment of the heart. This chapter aims to review the basics of ultrasound physiology, important terms used in echocardiography, different echocardiographic techniques, and basic echocardiographic views.
Echocardiography is the use of ultrasound to evaluate the structural components of the heart in a minimally invasive strategy. Although, prior to the invention of today's routinely used 2-dimensional echocardiography, there was motion-based (M-mode) echocardiography. In 1953, Inge Edler, regarded as the father of echocardiography, first described M-mode technology, which began the era of diagnostic noninvasive echocardiography.[1] M-Mode echocardiography was the combination of amplitude-based (A-mode) ultrasonography with Brightness-based (B-mode) techniques, which allowed the addition of a "time" dimension when the B-mode was swept across the oscilloscope; however this was not a picture, per se, but how structures evolved through the cardiac cycle.[9] This was the primary technology until two-dimensional (2D) ultrasonography was developed over the next decades. In 1973, S.L. Johnson developed 2D ultrasonography and doppler technology, which ultimately allowed physicians to detect blood flow in vessels, and, in 1979, Holen and Hatle found that by using the Bernoulli equation they could detect pressure gradients.[1] The combination of all these technologies is the echocardiography that is commonly used every day in today's medical profession.
The most commonly used technique among these is transthoracic echocardiography (TTE). This allows the clinician to obtain real-time sizes, structure, and function of the heart during the cardiac cycle. Another useful and important use of these methods is stress echocardiography. Stress echocardiography is the combination of standard transthoracic echocardiography and either pharmacological or physical stress to the cardiac structures to assess wall motion abnormalities. Physical stresses may include running on a treadmill, and pharmacological stress, including medications.[10] When higher resolution imaging of cardiac structures, including valves, is required, transesophageal echocardiography (TEE) is considered. TEE is more invasive than standard TTE, as it requires the insertion of a probe into the patient's esophagus to obtain images not hindered by the patient's chest wall, including; muscle, tissue, and bone. When more accurate and even higher-resolution imaging is needed, during intracardiac procedures, intracardiac echocardiography (ICE) is an option that can be considered.
Echocardiography is a low cost, at times minimally invasive, and readily available test that can provide information that can change the treatment course, and in some cases, provide real-time life-saving information. Many of the clinical uses of echocardiography are multidisciplinary in practice, and the overlap between the different utilities of echocardiogram is large. The addition of contrast to echocardiography, or the addition of strain to TTE are all examples of combinations of these utilities. The utilization of echocardiography is vast and can be applied in a variety of ways and a wide range of situations, and these forms will be discussed in detail.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomic Position of the Heart
The heart is normally positioned within the middle mediastinum with one-third of its mass located to the right side of the midline, and its own long axis is directed from the right shoulder (base of the heart) towards the left hypochondrium (apex of the heart). There are variations in this cardiac position related to the patient's body habitus, and minor changes may occur with respiration.[11]
At other times, diseases of the lung or pleura or other mediastinal structures can displace the heart, making image acquisition and interpretation a challenging proposition. On echocardiographic parasternal long-axis views, the right ventricular free wall is the anterior-most structure while the left ventricular posterior (inferolateral) wall is the posterior-most structure. (Figure 1)
Ultrasound Physiology
Echocardiographic probes utilize ultrasound waves (sound waves) of frequencies ranging from 1.5 to 7.5 MHz. The velocity of these waves depends on the nature of the material in which the sound travels. The normal velocity of sound in air is 330 m/s, while in the heart tissue, the velocity is around 1540 m/s.[12]
Ultrasound waves are produced due to the transformation of electrical oscillations into mechanical (sound) waves by the crystals in an echocardiographic probe. In contrast, the reflected mechanical waves are converted back to electrical signals. This phenomenon of inter-conversion of electrical and mechanical oscillations is called the piezoelectric effect. Each echocardiographic machine probe has this piezoelectric crystal transducer. On applying varying voltages, it vibrates and transmits ultrasound. On receiving the reflected ultrasound waves, the transducer generates an electrical signal analyzed by the echo machine.[13]
The ultrasound probe transmits sound waves to the body part which is being imaged. The tissues and the boundaries between them reflect the waves back to the probe. Distance from the probe to the tissue is calculated using the speed of sound in the tissue and the time of each echo's return. The two-dimensional image is formed by displaying the intensities of the echos and the distances calculated.
Indications
Echocardiographic examination indications may include the following:[14][15][16]
- Evaluation and monitoring of left ventricular systolic and diastolic function.
- Evaluation of valvular function
- Evaluation of right ventricular function
- Evaluation and quantification of cardiac chamber size.
- Evaluation of cardiac hemodynamics
- Evaluation of prosthetic valves structure and function
- Evaluation of congenital heart diseases, especially intra-cardiac shunts.
- Evaluation of coronary artery disease by stress echocardiogram
- Evaluation of the functional significance of a valvular lesion
- Evaluation of cardiac source of embolism
- Evaluation of cardiac masses
- Evaluation of pericardial diseases
The indications for the use of transthoracic echocardiography is vast, and the basis of using this test is known or suspected cardiac disease. The Journal of the American Society of Echocardiography has published appropriate use criteria in 2019, which covers the criteria in its entirety.[17]
The use of echocardiography in asymptomatic patients includes screening patients who have first degree relatives with hypertrophic cardiomyopathy (HCM), aortic aneurysms or dissections, and those athletes that have electrocardiographic (ECG) changes. These patients may not have any immediate complaints, but their strong family history should give the clinician a high pretest probability to order an Echocardiogram. For example, patients with HCM may have a family history of sudden cardiac death in 1st-degree relatives at a young age.
Second, the initial evaluation of patients with clinical signs of or symptoms of heart disease. This includes palpitations, syncope, pre-syncope, newly diagnosed bundle branch blocks, arrhythmias, ACS, exertional shortness of breath, and evaluation of pulmonary hypertension.
Third, follow-up on previously diagnosed heart failure or valvular disease. In regards to the former, a re-evaluation of the patient's ejection fraction with echocardiography, especially in those with acute heart failure exacerbations, would provide important information to better treat the patient.
Finally, the evaluation of patent foramen ovale in those with cerebrovascular accidents (CVA).[17] One of the common causes of CVA is cardioembolic disease. Echocardiography with "bubble study" is a way to evaluate for a patent foramen ovale (PFO). Agitated saline is injected into the heart chambers, and flow across the atrium is evaluated for a defect. This defect may require surgical closure.
Bedside echocardiography has many indications in addition to the above listed. Since the early 1990s, bedside echocardiography use by intensivists and emergency medicine physicians has been increasing. Bedside echocardiography is routinely employed in critically ill patients who may or may not have previously diagnosed cardiac disease, but now require vascular support. Bedside echocardiography in the undifferentiated shortness breath can help elucidate cardiac failure vs. pericardial effusion vs. non-cardiac etiology. Some of the most common indications for bedside echocardiography include suspicion for pulmonary embolism, hypotension or respiratory failure of unknown etiology, complications after cardiothoracic surgery, identifications of pericardial effusion, and evaluation of right ventricular dysfunction.[18]
The indications for the use of stress echocardiography is the suspicion for coronary artery disease. This includes patients with stable angina with intermediate probability for coronary artery disease, with a pre-test probability of 15% to 85%.[19] This includes Suspected CAD with negative cardiac troponin and/or non-diagnostic ECG. If a patient has unstable angina and/or increasing troponin levels, the decision may be made to proceed with Percutaneous Coronary Intervention instead of stress testing.
Transesophageal Echocardiography (TEE) is used because it provides a superior imaging quality of the posterior heart chambers and structures when compared to TTE, can be used during coronary artery bypass graft surgery, aids in placement of transcatheter devices, and may be performed at the bedside in clinically ill patients.[20] This includes assessing valvular structures when the diagnosis of Infective endocarditis is suspected, or pre-operative evaluations of thrombus prior to cardioversion. TTE is a good initiate test of choice to evaluate cardiac structures for vegetation seen in infective endocarditis; however, if clinical suspicion is high, a TEE must be obtained to properly evaluate the valves and associated valvular structures.
Intracardiac echocardiography (ICE) is used during transcatheter cardiac interventions. This includes closure of atrial septal defects, catheter-directed biopsy, thrombectomies, and during electrophysiological procedures, which include transeptal puncture.[21] As ICE obtains images from within the heart, higher resolution images are obtained to help guide catheter-directed procedures. Due to advances in TEE, there has been limited use for ICE; however, as there has been an increase in transvenous catheter procedures, ICE is being considered further.[21]
Intravascular ultrasound (IVUS) may be performed during cardiac catheterization to directly visualize atherosclerosis within the vessel walls; this is utilized when the extent and severity of stenosis are indeterminant during PCI.[22] Clinical trials have found improved luminal gains, decreased re-stenosis, stent thrombosis, myocardial infarction (MI), and the need for revascularization when compared to angiography alone. To overcome the limitations of both angiography and IVUS, the use of both during the same intervention can provide more accurate reconstructions of plaques size and volume.[23]
Strain rate (STR) Echocardiography, also known as deformation echocardiography, is indicated when there is high suspicion for wall motion abnormalities. However, TTE is initially used to evaluate wall abnormalities; it is based on visual estimates, which may be subjective because it is operator dependant.[24] If TTE imaging is not clear or evident enough, ST and STR echocardiography may be utilized as an adjunct for a more accurate and objective evaluation of wall motion abnormalities.
Three-dimensional (3D) echocardiography is used when a clearer image of cardiac structures, and how to relate to each other is required. This is used most often used with presurgical planning for interventional procedures, as it can prove improved views of valvular structures.[25] 3D echocardiography has also found to add prognostic value to wall motion abnormalities in those with ischemia and assessing viability in patients with myocardial infarction.[26]
Contrast echocardiography has been studied extensively in the assessment of myocardial perfusion and has been found to be of independent prognostic and diagnostic benefit.[27] The injection of agitated saline uses air microbubbles as contrast, which are used to detect right-to-left shunts in patients who are found to have a CVA or for evaluation of pulmonary arteriovenous malformations. Further clinical indications include the assessment of wall motion abnormalities at rest, apical left ventricular thrombus, rupture, and aneurysm, apical hypertrophy, cardiac masses, and during perfusion imaging.[27]
Contraindications
Although transthoracic echocardiography has no contraindications, it has a few limitations. First, due to the effects of body tissue on the transmission of ultrasound waves, echocardiogram yields only limited information in patients at the extremes of body weights.
Transesophageal echocardiogram has the following contraindications:[28]
Absolute Contraindications
- Esophageal obstruction
- Pharyngeal obstruction
- Suspected or known perforated viscera
- Gastrointestinal bleeding
- Instability of cervical vertebrae
Relative Contraindications
- Esophageal varices
- Esophageal diverticula
- Cervical arthritis
- Oropharyngeal distortion
- Bleeding diathesis or coagulopathy
- Uncooperative patient
Equipment
Following equipment is required for an echocardiographic examination.
- Echocardiographic machine
- Electrocardiographic leads
- Gel, for good surface contact
- Echocardiographic contrast
- Saline for bubble contrast
- Intravenous cannula
- Defibrillator for emergency arrhythmias
Echocardiography Terms
- Frequency: Sound waves are mechanical vibrations. The number of vibrations per unit time is called frequency, expressed in Hertz, 1 Hz = 1 vibration per second. Higher the frequency of the probe, the better the resolution but, the lesser the penetration.
- Grayscale: This indicates the different amplitude detected by the ultrasound system. High amplitudes are displayed bright, low amplitudes as dark grey, and no signal as black.
- Depth and Sector: Adjusting depth helps to adjust the size of the image on the screen. Sector indicates the width of the scan area. Both influence frame rate. Higher the frame rate, the higher is the resolution.
- Gain: Increasing gain increases the overall brightness of the image.
- TGC (time gain compensation): This compensates for attenuation of ultrasound energy with depth. These knobs help to increase or decrease the brightness at different depth levels.
- Frame Rate: The more the frame rate, the better the temporal resolution. Decreasing the depth, narrowing the sector width, or using live zoom can increase the frame rate.
Personnel
- Echocardiography technologist
- Registered cardiac nurse
- Cardiologist, an expert in echocardiography/imaging
Preparation
No special preparations are required for a standard transthoracic echocardiogram. Ideally, chest hairs should be removed in male patients for good probe contact and proper image acquisition.
For transesophageal echocardiogram, patients are required to be in a fasting state for at least six hours. Intravenous access is required for the administration of drugs or contrast media. Cardiac monitoring is done throughout the procedure. Light sedation is generally helpful.
Technique or Treatment
Patient Position and Electrocardiography Lead Placement
For the parasternal and apical tomographic views, the patient is required to lie in the left lateral decubitus position, with the left arm extended behind the head. This position brings the heart into close contact with the chest wall. The subcostal and suprasternal views require the patient to be in the supine position.[29] The modified electrocardiogram (ECG) leads are placed, which allow identification of arrhythmias and timing of cardiac events during the echocardiographic examination. An electrocardiogram is used as a timing marker for digital recording gating of echocardiographic images.
Echocardiographic Modes
M Mode
Initially, echocardiographic images were obtained by sending ultrasound waves along a single line followed by the display of amplitude of the reflected signal as well as the depth of that signal on an oscilloscope, which was called A-mode echocardiography. When these lines of ultrasound images were plotted concerning time, an M-mode (motion mode) was produced. Despite the increasing emphasis on 2D and 3D imaging, the M-mode remains a complementary part of the echocardiographic examination. M mode has a high sampling rate as compared to 2D echocardiography, which provides excellent temporal resolution. It is very useful in the timing of subtle cardiac events that can be missed in the 2D echocardiographic examination. Rapidly moving structures such as the aortic valve and mitral valve, and endocardium have characteristic movements in M-mode.[9]
M-mode also has a great spatial resolution, which is useful for measuring ventricular dimensions in systole and diastole.[30] The M-mode images are displayed like graphs, with time on the x-axis and distance from the transducer on the y-axis. The structures close to the transducer are displayed at the top of the image. (Figure.2)
2D Echocardiogram
2D echocardiographic imaging provides tomographic views of various planes of the cardiac structures and acts as a guide for the M-mode and Doppler echocardiogram. In 2D echocardiographic imaging, instead of having a fixed line of sight, the scan line is swept back and forth across an arc. After complex manipulation of the data received by the transducer from the multiple scan lines, a 2D tomographic image is generated by the echocardiographic machine for display.[31]
Doppler Imaging
The introduction of the Doppler technique to the 2D echocardiography not only added new imaging capabilities but also transformed echocardiography into a modality that could provide a non-invasive hemodynamic assessment. The Doppler principle states that “the sound frequency increases as the source moves toward the observer and decreases as the source moves away.” This change in frequency between the transmitter and the reflected sound waves is called the Doppler shift.[32] This Doppler frequency shift is used to measure the velocity of the red blood cell by using the Doppler equation.[33]
The cos θ in the Doppler equation calculates velocity dependent on the angle between the beam and the moving object (red blood cell). Echocardiography machines do not typically incorporate the angle for calculating the resultant velocity. Thus, it is necessary to have the angle between the ultrasound beam and the blood flow jet as close to zero as possible (cos 0 = 1). When this is not possible, the angle should be <20° so that the true flow velocity is underestimated by <6% (cos 20 = 0.94). Adhering to this requirement sometimes mandates off-axis or unusual 2D images to align the Doppler ultrasound signal with the desired target.
Spectral Analysis: The term used to describe how Doppler images (pulsed wave Doppler and continuous wave Doppler) are displayed.
- Pulsed Wave (PW) Doppler: The purpose of PW Doppler mode is to measure the Doppler shift to assess a velocity at a specific location of interest within a small sample volume (e.g., mitral inflow velocity at the mitral valve leaflet tips, the systolic velocity at the LVOT, and blood flow within the pulmonary veins). (Figure.3)) A single crystal sends short bursts of ultrasound waves at a specific pulse repetition frequency (PRF) to a specific location in this mode. The sound waves are reflected from moving blood cells at this location and received by the same crystal.[34]. The maximal velocity that can be measured is limited by the time required to transmit and receive the reflected ultrasound wave, which is called the Nyquist limit. If a velocity is greater than the Nyquist limit, the signal appears as a wrap around the baseline called aliasing. Color Doppler and tissue Doppler imaging (TDI) are based on the principle of pulsed-wave Doppler.
- Continuous Wave (CW) Doppler: CW Doppler utilizes two crystals; one of the crystals continuously sends ultrasound waves, and the other continuously receives the waves. Unlike PW Doppler, CW Doppler measures the maximal velocity along the entire ultrasound beam, and it does not help in localizing the precise position of that peak velocity.[35] Aliasing is not a feature of continuous-wave Doppler, so it is used to measure the higher velocities, e,g aortic stenosis. (Figure.4)
In general, CW Doppler is used to assessing a high-velocity flow, and PW Doppler is used to measuring the low-velocity flow in specific areas.
3D Echocardiogram
3D echocardiographic images are obtained using a transducer that transmits and receives data simultaneously in a 3D volume, in the form of either real-time 3D images or simultaneous biplane (orthogonal) 2D images. The 3D data set is then manipulated using different software packages to assess function and anatomy. It is more accurate than 2D echocardiography for the localization of valvular abnormalities, left ventricular volume calculation, improved assessment of the right ventricle, guiding surgical interventions (e.g., mitral valve repair), and complex congenital heart disease. 3D color flow imaging allows for a comprehensive assessment of vena contracta and areas of flow convergence (PISA), which can improve the quantification of valvular regurgitation. It has been documented to allow for a more rapid evaluation of mitral valve area (MVA) in mitral stenosis as compared with conventional 2D planimetry.[36][37][38]
Echocardiographic Tomographic Views
Parasternal Views: The parasternal views are obtained in the left lateral decubitus position by placing the transducer at the left of the sternal border in the third or fourth intercostal space. A hybrid position between the steep left lateral and supine positions may be required to optimize the view. This position allows imaging of the long axis as well as the short axis of the heart.[39][29]
- Parasternal long axis (PLAX) view: The PLAX view is traditionally the first view of a standard transthoracic echocardiographic examination. The ultrasound beam is lined up between the patient’s right shoulder and the left flank. The right ventricular outflow tract (RVOT) is located at the top of the image, the aorta to the right, the inferolateral (or posterior) wall on the bottom, and the cardiac apex on the left. The anteroseptal is visualized between the right ventricular outflow tract (RVOT) and the left ventricular (LV) cavity. (Figure.1) Tilting the transducer towards the left shoulder with slight clockwise rotation brings the right ventricular (RV) inflow into view. This is good for obtaining the tricuspid regurgitation (TR) velocity and examining the tricuspid valve, RV apex, and the right atrium.
- Parasternal short axis (PSAX) view: While the transducer is in the parasternal long-axis position, rotating the transducer clockwise by approximately 90° displays the heart in the short axis. The ultrasound beam in this view is directed roughly from the left shoulder to the right flank. Using different degrees of transducer tilting, and moving up or down an intercostal space, results in different views of the heart. For example, on tilting from superior to inferior, the views obtained are aortic valve–RV outflow view, mitral valve level view, mid-ventricle at the papillary muscles, and the SAX view at the level of LV apex.
Apical Tomographic Views: The apical position is obtained with the patient in the left lateral position and the probe placed at the maximum apical impulse. This position allows imaging of the long axis of the heart.[40][29]
- Apical four-chamber (A4C) view: The A4C view is obtained with the ultrasound beam transecting the thorax in a superior-inferior fashion. In most echocardiographic laboratories, the transducer is oriented to place the left ventricle on the right side of the screen and the right ventricle on the left side. The apex is at the top of the image, and the atria are at the bottom, regardless of the orientation. The inferoseptal and anterolateral walls and the apex of the left ventricle are assessed in this view. Assessment of the right ventricular structure and function is also done in this view. (Figure.5)
- Apical five-chamber (A5C) view: A slight rotation of the transducer introduces the proximal aorta, a fifth “chamber,” as well as the aortic valve and LVOT. This view allows for qualitative assessment of aortic valve morphology along with the hemodynamic assessment of the LVOT and aortic valve.
- Apical two-chamber (A2C) view: From the apical 4C view, 90° counterclockwise rotation gives the A2C view. In this view, in addition to the left atrium, the LV anterior wall, inferior wall, apex, and mitral valve are also well visualized. (Figure.6)
- Apical long axis/three-chamber (A3C) view: A slightly more counterclockwise rotation (approximately 30°) from the A2C view brings the aorta back into the image, resulting in the A3C, or apical long-axis view. This view essentially has the same anatomical structures as those in the PLAX view with a different orientation. The apex is better visualized, and the RVOT usually drops out of the image. Additional information on mitral and aortic valve hemodynamics can also be obtained in this view. (Figure.7)
Subcostal Tomographic Views: The subcostal view is obtained with the patient in the supine position and the probe located caudal to the xiphoid process. The transducer is placed in the midline nearly parallel to the long axis of the patient’s body so that the ultrasound beam slices toward the spine. This shows the right ventricle at the top right, the left ventricle at the bottom right, and their respective atria on the left. (Figure.8) Clockwise rotation along with inferior tilting brings the inferior vena cava (IVC) and hepatic veins into view for right-sided hemodynamic assessments.[41][29]
Suprasternal Tomographic Views: Suprasternal view is obtained by placing the transducer in the suprasternal notch and pointing inferiorly. It is used to assess the ascending aorta, aortic arch, and descending aorta. Hemodynamics from this position can better characterize AR, patent ductus arteriosus, and the presence of coarctation of the aorta.[29][42]
Trans-esophageal Echocardiogram
Transesophageal echocardiography (TEE) is performed when transthoracic echocardiography (TTE) is insufficient to answer a particular question or there is a discrepancy between the clinical examination and TTE findings. It is also used to better define a pathology that has been identified by TTE or to obtain better images when transthoracic images are inadequate. The proximity of the esophagus to the heart improves visualization of the cardiac structures, particularly those located posteriorly. In addition, due to the shorter distance between the probe and the cardiac structures, higher frequency probes can be used in TEE, which further enhances the resolution. However, imaging planes are somewhat constrained by the relative position of the esophagus and the cardiac structure, making transthoracic imaging superior in assessing certain structures (i.e., pulmonic valve) and Doppler measurements.[43]
TEE is a useful imaging modality in the operating room as well as the cardiac catheterization laboratory. In cardiothoracic surgery, TEE is used to assess the mechanism of valvular abnormalities, and it subsequently helps evaluate the efficacy of valve repair or replacement. For example, TEE can be used to guide the location of the aortic cross-clamp so that the segments with severe atheromatous plaque can be avoided, thereby reducing the risk of embolization. In addition, TEE is an essential tool in providing a better assessment of left ventricular function and regional wall motion abnormalities. In congenital heart surgery, it is standard to assess the adequacy of repair with TEE in the operating room itself.
Transesophageal echocardiogram has been increasingly utilized in catheterization laboratories to help guide catheter position, transseptal punctures, implantation of percutaneous valves, and placement of left atrial appendage occluding devices, as well as the closure of periprosthetic leaks, atrial septal defects, ventricular septal defects, and patent foramen ovale. Prevention and early recognition of complications achieved by TEE imaging are often crucial for periprocedural success.[44] Details and tomographic views of transesophageal echocardiograms need a separate chapter.
Complications
Other than an allergic reaction to gel, a transthoracic echocardiogram has no significant complications. A transesophageal echocardiogram is rarely associated with trauma to the teeth, oral mucosa, and esophagus. Esophageal rupture, vasovagal reflex, and aspiration pneumonia are the other rare complications associated with a transesophageal echocardiogram.
Clinical Significance
Echocardiography is a reliable and non-invasive imaging modality for assessing cardiac structure, function, and hemodynamics. Compared to other cardiovascular imaging modalities, it is easily available and relatively inexpensive and does not expose the patient to radiation. Portable machines provide the ease of doing the study at the bedside for sick patients. Echocardiography displays live real-time images and are widely available. Although it is operator-dependent, its accuracy is comparable with other imaging modalities.[45]
Transthoracic Echocardiography (TTE): When a patient presents clinically with dyspnea or chest pain, and there is a high pre-test probability that the shortness of breath is of cardiac origin, TTE is recommended. It is useful in identifying the cause, location, and severity of myocardial ischemia, atrial sizes, ejections fraction (EF), left ventricular hypertrophy, and presence of valvular disease.[46] An EF is a common piece of information that is available from a TTE, especially in those with systolic congestive heart failure (CHF), because it dictates the course of treatment. An important assessment of cardiac structure by TTE is the size and thickness of the cardiac structures. Left and right atrial size will help aid in the diagnosis of diastolic dysfunction, and right and left ventricular hypertrophy will aid in the diagnosis of heart failure. This is especially important when the diagnosis of hypertrophic cardiomyopathy (HCM) is suspected. Asymmetric hypertrophy of left and right ventricles is the bases of the diagnosis for HCM. Patients who are found to have preserved ejection fraction (>50%) CHF are treated mainly with diuretics (furosemide, bumetanide) for symptom management.[47] On the contrary, those who are found to have reduced EF (<50%) CHF may be treated with diuretics, with the addition of beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and aldosterone antagonist which have shown to have a mortality benefit. This benefit is not seen in those with preserved EF heart failure. The evaluation of the mitral, tricuspid, aortic, and pulmonary valves is another important indication of TTE. Patients who have a new-onset heart murmur, clinical suspicion for infective endocarditis, dyspnea, and near-syncope may have structural valve pathology including tricuspid, mitral, aortic, and pulmonary stenosis and regurgitation. TEE is more sensitive for the diagnosis of valvular pathology, although TTE is generally performed first, as it is less invasive.[46] Another aspect of TTE is assessing heart chamber pressures, and the most useful of these is right pulmonary artery pressure, which aids in the diagnosis of pulmonary artery hypertension. In the acute setting, bedside TTE can assess pericardial effusions, and aid in the diagnosis of cardiac tamponade, this may require immediate interventions, including pericardiocentesis.
Bedside Echocardiography: The use of bedside echocardiography is widespread and allows a physician to obtain immediate information in the acute setting. A common use is an assessment of cardiovascular response while hydrating a hypovolemic patient, however, as mentioned above, this gives you information about pre-load, and further clinical assessment must be taken into account.[48] The use of bedside TTE for the assessment of pulmonary embolism has shown to have a specificity of 83% and sensitivity of 53%.[49] The most common "sign" used was the demonstration of right heart strain due to a pulmonary embolism. Due to its low sensitivity but high specificity, it may be an adequate rule-in test during critical situations at the bedside.
Transesophageal Echocardiography (TEE): When a patient has a high index of suspicion for infective endocarditis, it is important to have a much clearer image of the valvular structure to identify valvular prolapse, rupture, or infective vegetation on the valves[20] The ability to recognize vegetation will drive the time course of antibiotic treatment, TTE is not always sensitive enough to identity vegetation. Patients who undergo cardioversion for atrial fibrillation or flutter, who have not been anticoagulated previously, will need to undergo TEE to assess for thrombus first. TEE is able to assess the left atrial appendage (LAA) for the presence of thrombus, which is the most commonplace for the formation of clots. If a patient were to undergo cardioversion with a thrombus present, it could dislodge and cause a cerebrovascular accident. If a thrombus is not identified on echocardiography, the cardioversion may proceed.[20] Finally, when patients are undergoing intracardiac transcatheter valve procedures, septal closure device placement, or catheter ablation, TTE is generally used as it provides clearer imaging to assist in the procedures in real-time.
Stress Echocardiography: When appropriate, stress echocardiography is a great initial modality to assess for cardiac ischemia. First, the patient's heart function is assessed at rest to determine a baseline, next the heart is stressed using either running on a treadmill or pharmacological stressors, including dobutamine, adenosine, or dipyridamole.[46] Next, using ECG and echocardiogram, cardiac rhythm and images are obtained after the patient has achieved appropriate exercise capacity or 85% of age-predicted maximum heart rate.[46] If ECG changes and new or worsening wall motion abnormalities are seen on echocardiography, the patient will likely need to undergo cardiac catheterization and potentially percutaneous coronary intervention (PCI) with coronary stent placement if there is stenosis identified. If patients have significant chest pain or are unable to reach appropriate exercise capacity prior to completion, stress testing may be halted, and the patient would be referred for cardiac catheterization with possible PCI.
Intracardiac Echocardiography (ICE): The use of ICE is less frequent given its invasive technique, cost, steep learning curve, and due to the advancements in TTE and TEE.[21] The advantages of ICE include higher resolution imaging and avoids the need for sedation or endotracheal intubation.[50] As atrial septal defect closures are becoming more common to perform via transvenous route, and because TTE and TEE imaging may be limited, ICE provides better visualization of intra-cardiac structures for a safer and more accurate transeptal catheterization needed for repair.[51] Furthermore, the use of ICE during catheter ablations is helpful as it improves tissue contact while using the circular mapping catheter. ICE may lower procedural time and improve the optimal size of lesion formation during ablation, and thus, leading to improved success rates. However, the use of ICE during left-atrial appendage (LAA) closure was evaluated in the ICE-CHIP trial, and the study found the use of ICE form the right atrium, was inadequate at identifying a thrombus in the LAA.[50] Further advances in ICE are needed for LAA visualization, and at this time, TEE is more sensitive at identifying a thrombus in the LAA when compared to ICE.
Intravascular Ultrasound (IVUS): The mainstay of treatment for coronary artery disease is cardiac catheterization when appropriate, and most commonly, it is performed under the guidance of angiography. Contrast is introduced into the cardiac vasculature while radiography is performed, allowing the visualization of coronary anatomy. This is also the technique interventional cardiologists utilize to guide their wire and assess stenosis. When stenosis is <40%, no intervention is generally required, but with a greater than 70% stenosis, a percutaneous coronary intervention (PCI) is performed.[52] However, if lesions are in the indeterminate range, 40% to 70% stenosis, further imaging, such as IVUS, is required to better assess the lesion and guide intervention.[22] The blood flow and pressure is measured proximal and distal to the lesion, and the flow and pressure differential is calculated across the area of stenosis. If the lesion is causing significant flow defects, coronary stenting is likely to be performed. This utilization is called Fractional flow reserve (FFR), and Instantaneous wave-free Ratio (IFR), which is discussed in much greater detail in it's associated StatPearls.[52]
Strain rate (STR) Echocardiography: TTE is able to detect wall motion abnormalities in those with ischemic or non-ischemic cardiomyopathy; however, when these abnormalities are sub-clinical, STR echocardiography is a more sensitive utility. Early detection in asymptomatic patients is an important use of STR echocardiography, especially in those with diabetes, amyloidosis, and muscular dystrophies.[24] Furthermore, it has been shown that STR imaging is sensitive enough to detect early cardiac injury secondary to doxorubicin-based chemotherapy.[24] Dandel et al. described the utility of differentiating between an athlete's physiological hypertrophy and asymptomatic HCM. This utility is important as HCM is known to cause sudden cardiac death in young athletes. A study from Belgium also described that the use of STR echocardiography was the superior method in identifying cardiac tissue changes and fibrosis in patients with HCM.[53] Another important utility is the assessment of cardiac viability. The augmentation of STR imaging with dobutamine has been shown to improve the diagnostic and prognostic evaluation of ischemia and post-myocardial infarction scar tissue formation.[24] It is important to understand that STR imaging can be applied to other forms of echocardiography; this includes TEE, TTE, and 3D echocardiography. It is an adjunct to improve visualization of wall motion defects.
3-dimensional (3D) Echocardiography: The use of traditional 2D echocardiography is limited due to foreshortened views of the ventricles and atria, and this can underestimate volumes.[54] 3D imaging allows the user to select images that are not foreshortened, which eliminates the geometric assumptions performed when assessing ventricular and atrial volumes. 3D echocardiography can further improve the visualization of shapes and spatial relationships between cardiac structures, as well as improve the visualization and function of valves and valvular structure.[54] Qiangjun et al. describe a case of hepatic metastasis to the tricuspid and pulmonic valve, in which 2D echocardiography only visualized severe tricuspid and pulmonary regurgitation. However, 3D echocardiography was able to detect fixed, retracted, and thickened valves during the cardiac cycle; this utility provided significant data to the practitioners to allow for the diagnosis of metastatic disease.[55] The left atrial appendage is the most common place where thrombi form in patients with atrial fibrillation, and in those with a contraindication to anticoagulation, a left atrial appendage closure device such as a Watchman device may be placed. Interventional cardiologists are able to use 3D echocardiography to simulate the procedure morphology prior to placing the closure device.[54] 3D echocardiography is an invaluable tool that is being used more frequently with all forms of echocardiography to improve clinical assessments.
Contrast Echocardiography: When a patient has an embolic cerebrovascular accident, the most common origin is cardioembolic. Contrast-enhanced echocardiography is performed to assess for the presence of a patent foramen ovale, which may require surgical closure.[27] Agitated saline is used as a contrast media and injected into the right atrium, which is routinely called a "bubble study," TTE is performed to detect the passing of the bubbles from the right atrium to the left atrium. When a patient is to undergo cardioversion for arrhythmia and has not been anticoagulated for at least three weeks, a TEE is often performed to identify possible left atrial appendage thrombus and prevent dislodgement during cardioversion. Echocardiography contrast may obscure the visualization of a thrombus; on the other hand, hypoechogenic thrombi may be obscured during standard TEE.[56] Two studies involved using contrast-enhanced and non-contrast-enhanced TEE in the detection of cardiac thrombi found that contrast-enhanced imaging was able to better delineate thrombi and was able to further identify the presence of thrombi more frequently than non-contrast-enhanced imaging.[57][58] If non-contrast imaging is inconclusive, then the use of contrast-enhanced imaging may be warranted.
Enhancing Healthcare Team Outcomes
A comprehensive echocardiographic examination requires a team that includes an imaging cardiologist as well as an echocardiography technician. It is vital to take a proper history and perform a detailed physical examination pre-procedure to understand the appropriate indications of the procedure. Communication between the referring physician, echocardiography technicians, and the cardiologist is essential, especially when there is a discrepancy in the clinical examination and echocardiography findings.
Media
(Click Image to Enlarge)
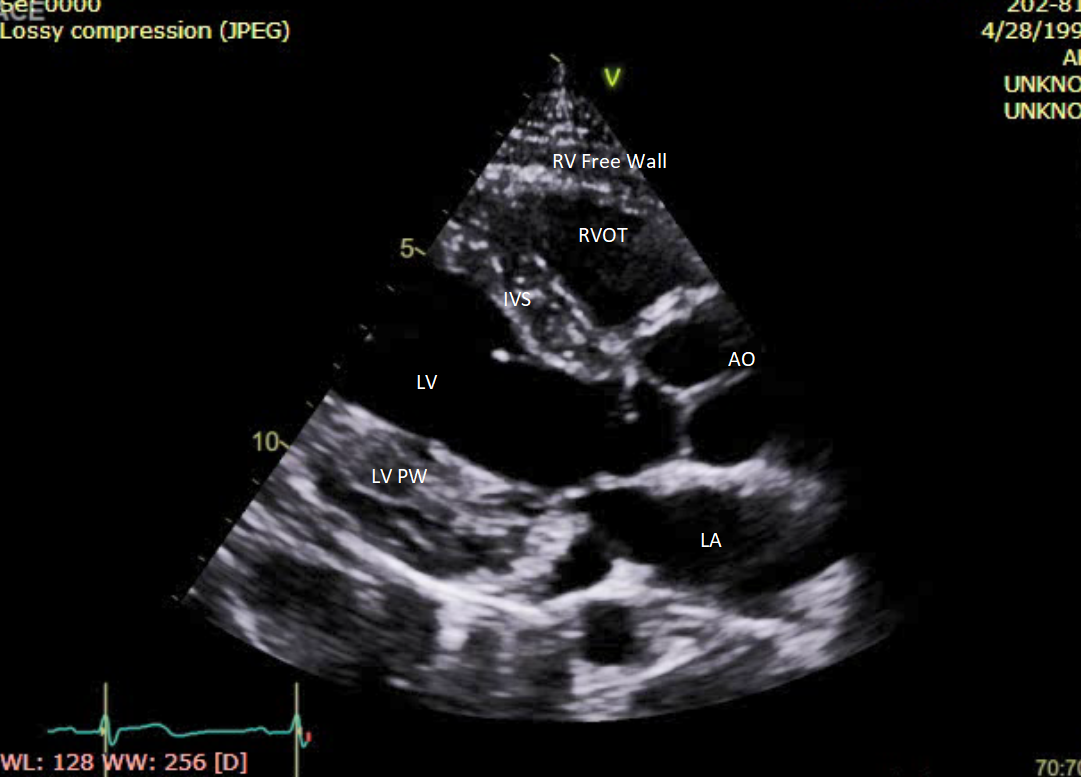
Figure.1 Parasternal long axis (PLAX) view. RV=Right ventricle, RVOT= Right ventricular outflow tract, LV= Left ventricle, LV PW= Left ventricular posterior wall, LA= Left atrium, AO= Aorta, IVS= Interventricular septum Contributed by Intisar Ahmed
(Click Image to Enlarge)
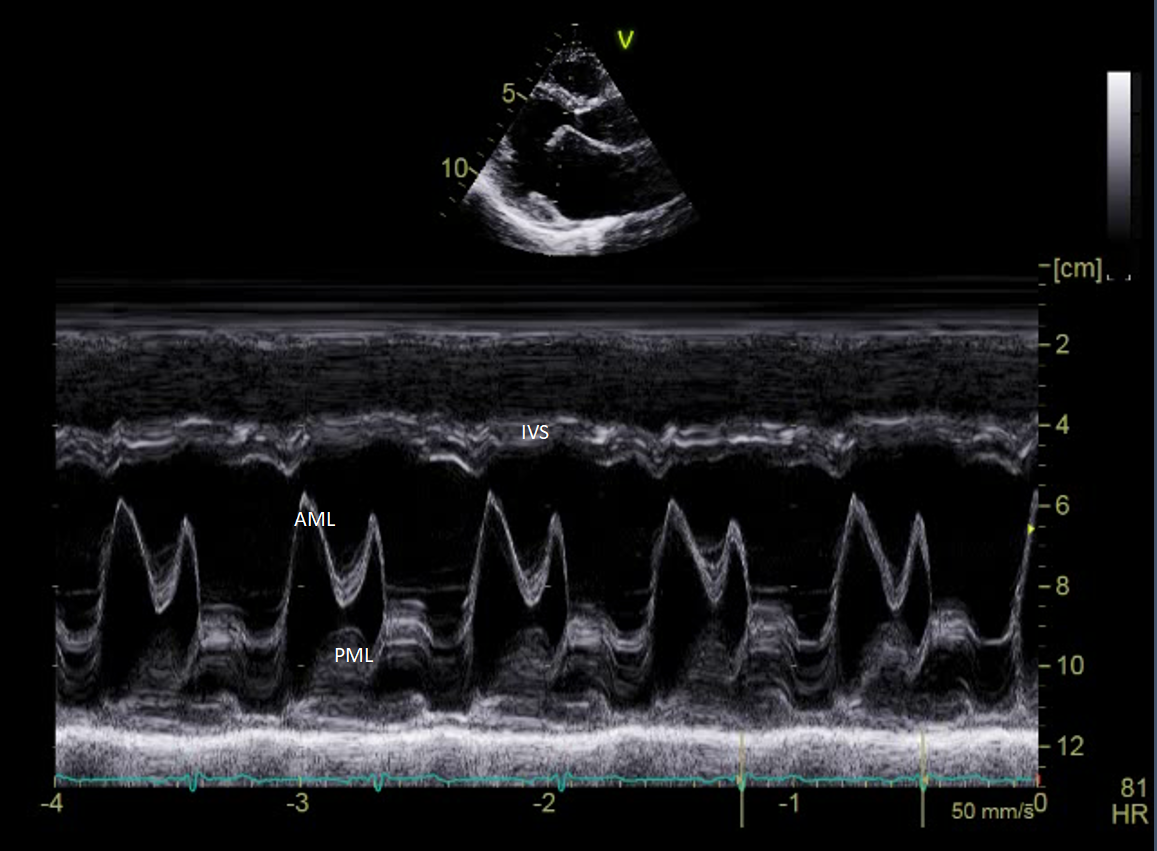
Figure.2 M-mode at mitral valve leaflets. AML=Anterior mitral leaflet, PML= Posterior mitral leaflet, IVS= Interventricular septum Contributed by Intisar Ahmed
(Click Image to Enlarge)
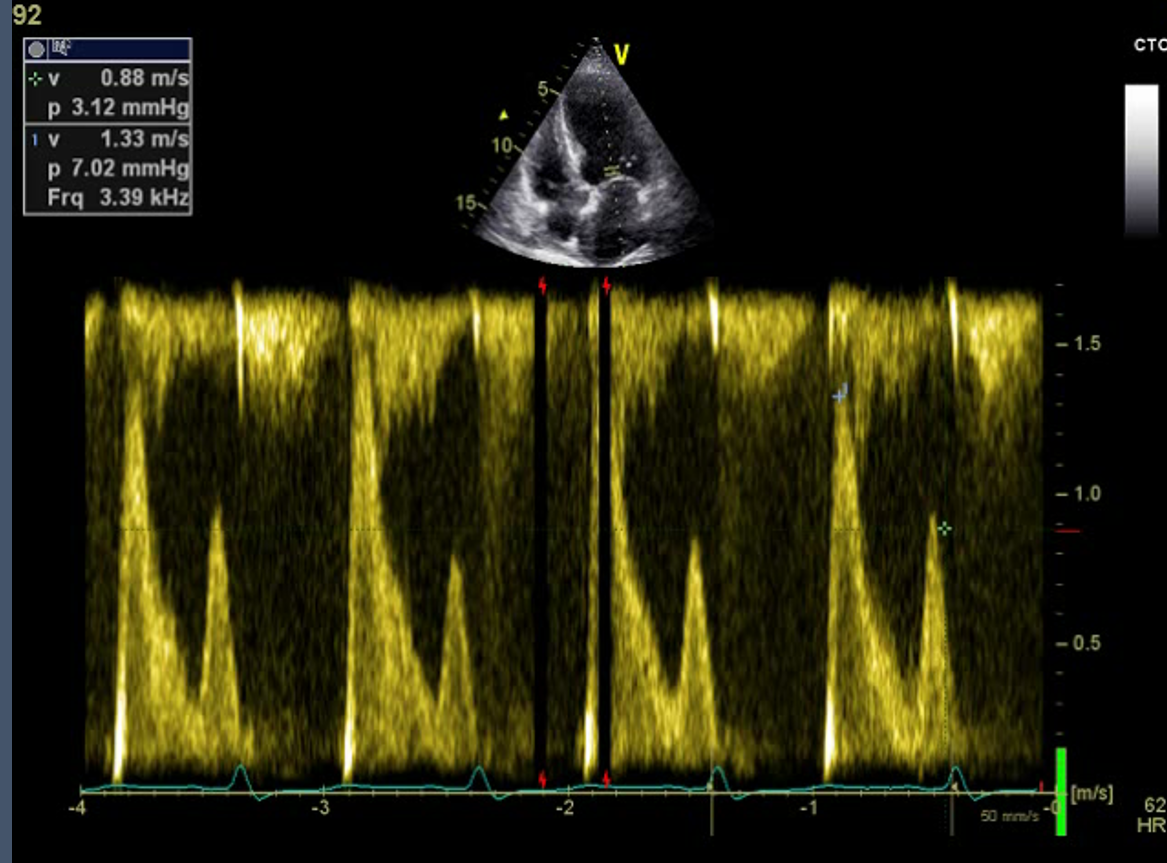
Figure.3 Pulsed wave (PW) Doppler at mitral inflow. Contributed by Intisar Ahmed
(Click Image to Enlarge)
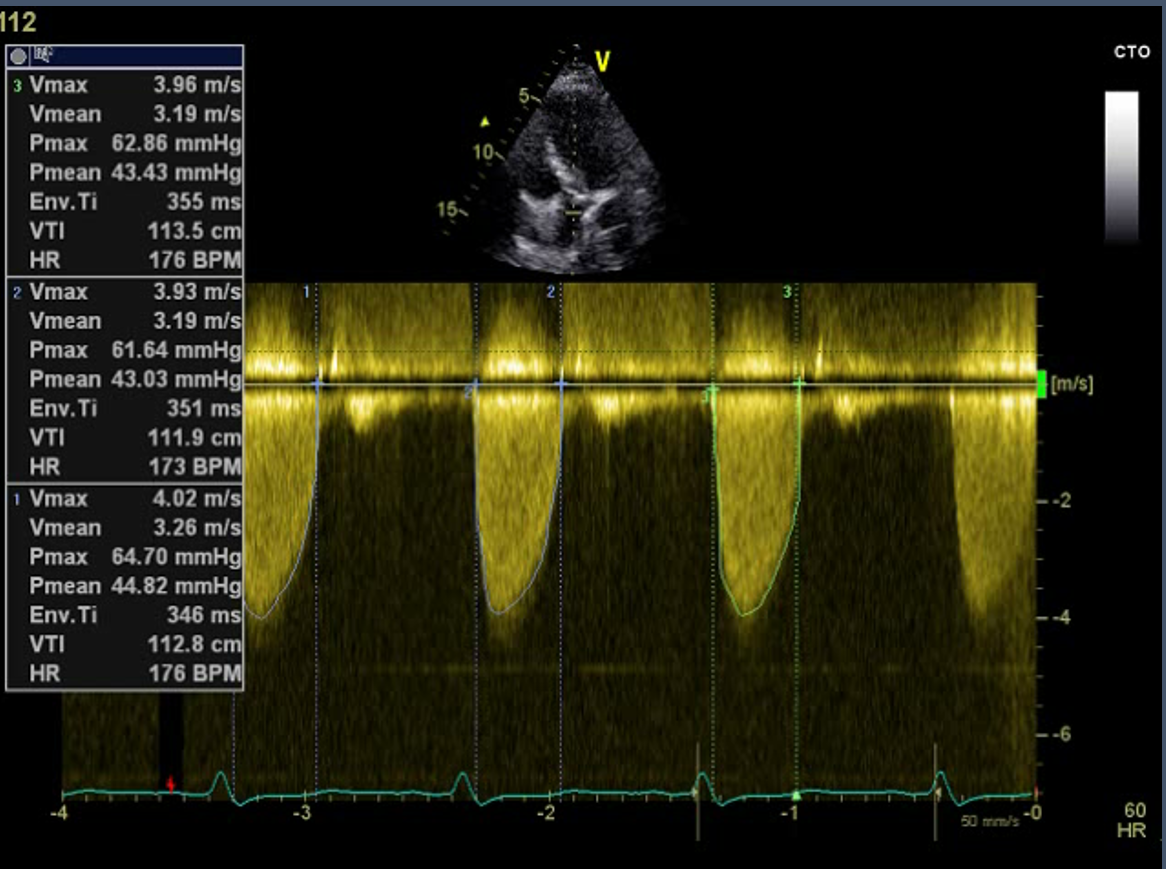
Figure.4 Continuous wave (CW) Doppler at aortic valve Contributed by Intisar Ahmed
(Click Image to Enlarge)
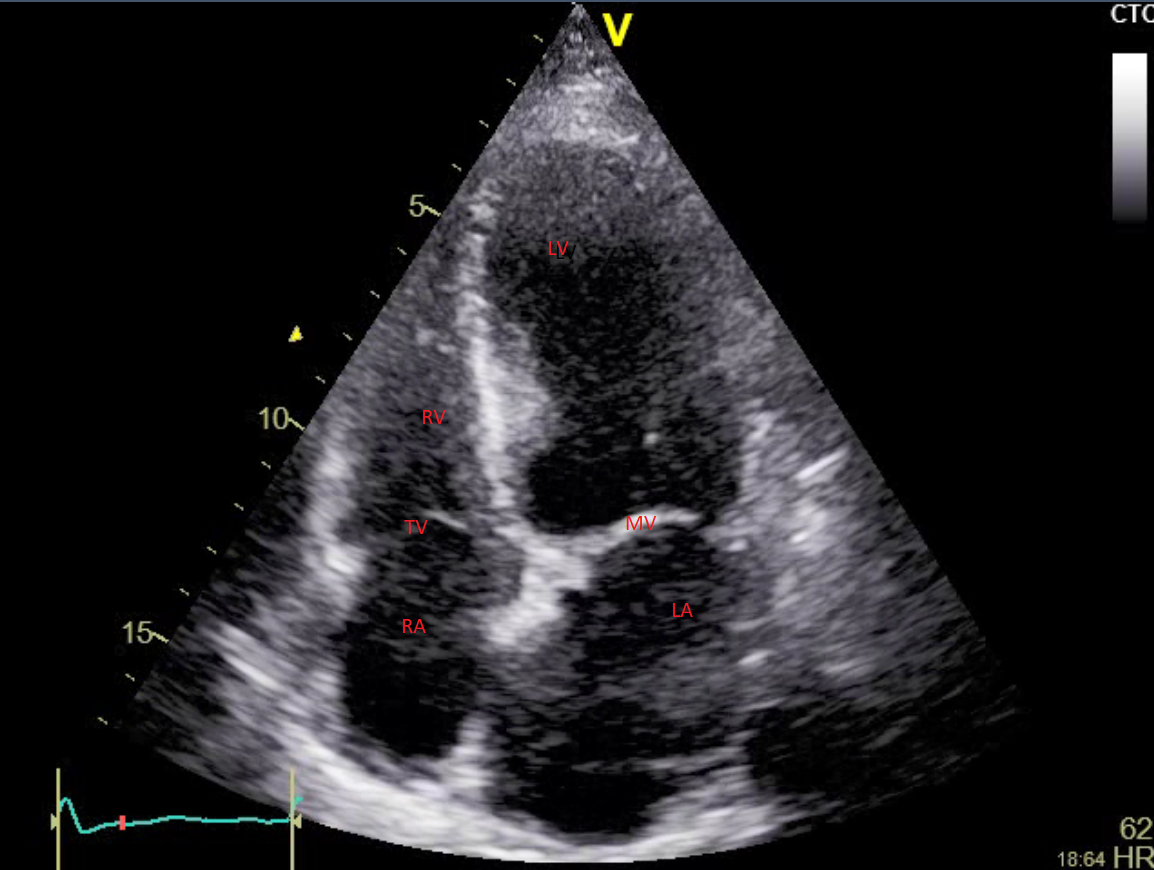
Figure.5 Apical four chamber (A4C) view. LV= Left ventricle, RV= Right ventricle, LA= Left atrium, RA= Right atrium, MV= Mitral valve, TV= Tricuspid valve Contributed by Intisar Ahmed
References
Singh S, Goyal A. The origin of echocardiography: a tribute to Inge Edler. Texas Heart Institute journal. 2007:34(4):431-8 [PubMed PMID: 18172524]
Edler I, Hertz CH. The use of ultrasonic reflectoscope for the continuous recording of the movements of heart walls. 1954. Clinical physiology and functional imaging. 2004 May:24(3):118-36 [PubMed PMID: 15165281]
Mintz GS, Kotler MN, Parry WR, Segal BL. Statistical comparison of M mode and two dimensional echocardiographic diagnosis of flail mitral leaflets. The American journal of cardiology. 1980 Feb:45(2):253-9 [PubMed PMID: 7355735]
Bom N, van der Steen AF, de Jong N, Roelandt JR. Early, recent and future applications of echocardiography. Clinical physiology and functional imaging. 2004 May:24(3):141-6 [PubMed PMID: 15165283]
Coman IM, Popescu BA. Shigeo Satomura: 60 years of Doppler ultrasound in medicine. Cardiovascular ultrasound. 2015 Dec 23:13():48. doi: 10.1186/s12947-015-0042-3. Epub 2015 Dec 23 [PubMed PMID: 26699126]
Li X, Ashraf M, Thiele K, Bhat AH, Sakaguchi R, Mitchell JC, Brie JA, Young M, Bader RS, Pemberton J, Sahn DJ. A novel method for the assessment of the accuracy of computing laminar flow stroke volumes using a real-time 3D ultrasound system: In vitro studies. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2005 Dec:6(6):396-404 [PubMed PMID: 15927537]
Level 3 (low-level) evidenceKaragodin I, Genovese D, Kruse E, Patel AR, Rashedi N, Lang RM, Mor-Avi V. Contrast-enhanced echocardiographic measurement of longitudinal strain: accuracy and its relationship with image quality. The international journal of cardiovascular imaging. 2020 Mar:36(3):431-439. doi: 10.1007/s10554-019-01732-4. Epub 2019 Nov 13 [PubMed PMID: 31720940]
Level 2 (mid-level) evidenceHan JC, Zhang HB, Gao S, Yu SM, Han J, Meng X, He YH. [Evaluation of the intraoperative transesophageal echocardiography for the aortic valve reconstruction]. Zhonghua yi xue za zhi. 2018 Oct 16:98(38):3064-3067. doi: 10.3760/cma.j.issn.0376-2491.2018.38.004. Epub [PubMed PMID: 30392264]
Feigenbaum H. Role of M-mode technique in today's echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2010 Mar:23(3):240-57; 335-7. doi: 10.1016/j.echo.2010.01.015. Epub [PubMed PMID: 20206828]
Kossaify A, Bassil E, Kossaify M. Stress Echocardiography: Concept and Criteria, Structure and Steps, Obstacles and Outcomes, Focused Update and Review. Cardiology research. 2020 Apr:11(2):89-96. doi: 10.14740/cr851. Epub 2020 Mar 10 [PubMed PMID: 32256915]
Anderson RH, Razavi R, Taylor AM. Cardiac anatomy revisited. Journal of anatomy. 2004 Sep:205(3):159-77 [PubMed PMID: 15379923]
Holmes JH. Diagnostic ultrasound during the early years of A.I.U.M. Journal of clinical ultrasound : JCU. 1980 Aug:8(4):299-308 [PubMed PMID: 6772678]
Krishnamoorthy VK, Sengupta PP, Gentile F, Khandheria BK. History of echocardiography and its future applications in medicine. Critical care medicine. 2007 Aug:35(8 Suppl):S309-13 [PubMed PMID: 17667454]
American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American College of Chest Physicians, Douglas PS, Garcia MJ, Haines DE, Lai WW, Manning WJ, Patel AR, Picard MH, Polk DM, Ragosta M, Parker Ward R, Weiner RB. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocardiography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medicine, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance American College of Chest Physicians. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2011 Mar:24(3):229-67. doi: 10.1016/j.echo.2010.12.008. Epub [PubMed PMID: 21338862]
Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P, Dehmer GJ, Doherty JU, Schoenhagen P, Amin Z, Bashore TM, Boyle A, Calnon DA, Carabello B, Cerqueira MD, Conte J, Desai M, Edmundowicz D, Ferrari VA, Ghoshhajra B, Mehrotra P, Nazarian S, Reece TB, Tamarappoo B, Tzou WS, Wong JB, Doherty JU, Dehmer GJ, Bailey SR, Bhave NM, Brown AS, Daugherty SL, Dean LS, Desai MY, Duvernoy CS, Gillam LD, Hendel RC, Kramer CM, Lindsay BD, Manning WJ, Mehrotra P, Patel MR, Sachdeva R, Wann LS, Winchester DE, Wolk MJ, Allen JM. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2017 Appropriate Use Criteria for Multimodality Imaging in Valvular Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2018 Apr:31(4):381-404. doi: 10.1016/j.echo.2017.08.012. Epub 2017 Oct 20 [PubMed PMID: 29066081]
Writing Group Members, Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P, Rating Panel Members, Dehmer GJ, Doherty JU, Schoenhagen P, Bashore TM, Bhave NM, Calnon DA, Carabello B, Conte J, Dickfeld T, Edmundowicz D, Ferrari VA, Hall ME, Ghoshhajra B, Mehrotra P, Naqvi TZ, Reece TB, Starling RC, Szerlip M, Tzou WS, Wong JB, Appropriate Use Criteria Task Force, Doherty JU, Dehmer GJ, Bailey SR, Bhave NM, Brown AS, Daugherty SL, Dean LS, Desai MY, Duvernoy CS, Gillam LD, Hendel RC, Kramer CM, Lindsay BD, Manning WJ, Patel MR, Sachdeva R, Wann LS, Winchester DE, Wolk MJ. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2019 Appropriate Use Criteria for Multimodality Imaging in the Assessment of Cardiac Structure and Function in Nonvalvular Heart Disease: A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and the Society of Thoracic Surgeons. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2019 May:32(5):553-579. doi: 10.1016/j.echo.2019.01.008. Epub 2019 Feb 7 [PubMed PMID: 30744922]
Doherty JU, Kort S, Mehran R, Schoenhagen P, Soman P, Rating Panel Members, Appropriate Use Criteria Task Force. ACC/AATS/AHA/ASE/ASNC/HRS/SCAI/SCCT/SCMR/STS 2019 Appropriate Use Criteria for Multimodality Imaging in the Assessment of Cardiac Structure and Function in Nonvalvular Heart Disease : A Report of the American College of Cardiology Appropriate Use Criteria Task Force, American Association for Thoracic Surgery, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and the Society of Thoracic Surgeons. Journal of nuclear cardiology : official publication of the American Society of Nuclear Cardiology. 2019 Aug:26(4):1392-1413. doi: 10.1007/s12350-019-01751-7. Epub [PubMed PMID: 31250324]
Casaroto E, Mohovic T, Pinto LM, Lara TR. Bedside echocardiography in critically ill patients. Einstein (Sao Paulo, Brazil). 2015 Oct-Dec:13(4):644-6. doi: 10.1590/S1679-45082015MD3271. Epub [PubMed PMID: 26761560]
Steeds RP, Wheeler R, Bhattacharyya S, Reiken J, Nihoyannopoulos P, Senior R, Monaghan MJ, Sharma V. Stress echocardiography in coronary artery disease: a practical guideline from the British Society of Echocardiography. Echo research and practice. 2019 Jun 1:6(2):G17-G33. doi: 10.1530/ERP-18-0068. Epub [PubMed PMID: 30921767]
Hahn RT, Abraham T, Adams MS, Bruce CJ, Glas KE, Lang RM, Reeves ST, Shanewise JS, Siu SC, Stewart W, Picard MH, American Society of Echocardiography, Society of Cardiovascular Anesthesiologists. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. Anesthesia and analgesia. 2014 Jan:118(1):21-68. doi: 10.1213/ANE.0000000000000016. Epub [PubMed PMID: 24356157]
Alkhouli M, Hijazi ZM, Holmes DR Jr, Rihal CS, Wiegers SE. Intracardiac Echocardiography in Structural Heart Disease Interventions. JACC. Cardiovascular interventions. 2018 Nov 12:11(21):2133-2147. doi: 10.1016/j.jcin.2018.06.056. Epub [PubMed PMID: 30409271]
Otake H, Kubo T, Shinke T, Hibi K, Tanaka S, Ishida M, Kataoka T, Takaya T, Iwasaki M, Sonoda S, Ioji T, Akasaka T. OPtical frequency domain imaging vs. INtravascular ultrasound in percutaneous coronary InterventiON in patients with Acute Coronary Syndrome: Study protocol for a randomized controlled trial. Journal of cardiology. 2020 Sep:76(3):317-321. doi: 10.1016/j.jjcc.2020.03.010. Epub 2020 Apr 24 [PubMed PMID: 32340781]
Level 1 (high-level) evidenceShi C, Luo X, Guo J, Najdovski Z, Fukuda T, Ren H. Three-Dimensional Intravascular Reconstruction Techniques Based on Intravascular Ultrasound: A Technical Review. IEEE journal of biomedical and health informatics. 2018 May:22(3):806-817. doi: 10.1109/JBHI.2017.2703903. Epub 2017 May 12 [PubMed PMID: 28504955]
Dandel M, Lehmkuhl H, Knosalla C, Suramelashvili N, Hetzer R. Strain and strain rate imaging by echocardiography - basic concepts and clinical applicability. Current cardiology reviews. 2009 May:5(2):133-48. doi: 10.2174/157340309788166642. Epub [PubMed PMID: 20436854]
Levine RA, Handschumacher MD, Sanfilippo AJ, Hagege AA, Harrigan P, Marshall JE, Weyman AE. Three-dimensional echocardiographic reconstruction of the mitral valve, with implications for the diagnosis of mitral valve prolapse. Circulation. 1989 Sep:80(3):589-98 [PubMed PMID: 2766511]
Corsi C, Lang RM, Veronesi F, Weinert L, Caiani EG, MacEneaney P, Lamberti C, Mor-Avi V. Volumetric quantification of global and regional left ventricular function from real-time three-dimensional echocardiographic images. Circulation. 2005 Aug 23:112(8):1161-70 [PubMed PMID: 16103242]
Level 1 (high-level) evidenceEskandari M, Monaghan M. Contrast echocardiography in daily clinical practice. Herz. 2017 May:42(3):271-278. doi: 10.1007/s00059-017-4533-x. Epub [PubMed PMID: 28160033]
Hilberath JN, Oakes DA, Shernan SK, Bulwer BE, D'Ambra MN, Eltzschig HK. Safety of transesophageal echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2010 Nov:23(11):1115-27; quiz 1220-1. doi: 10.1016/j.echo.2010.08.013. Epub [PubMed PMID: 20864313]
Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster MC, Horton K, Ogunyankin KO, Palma RA, Velazquez EJ. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2019 Jan:32(1):1-64. doi: 10.1016/j.echo.2018.06.004. Epub 2018 Oct 1 [PubMed PMID: 30282592]
Kühl HP, Hanrath P, Franke A. M-mode echocardiography overestimates left ventricular mass in patients with normal left ventricular shape: a comparative study using three-dimensional echocardiography. European journal of echocardiography : the journal of the Working Group on Echocardiography of the European Society of Cardiology. 2003 Dec:4(4):312-9 [PubMed PMID: 14611828]
Level 2 (mid-level) evidenceBonagura JD, Blissitt KJ. Echocardiography. Equine veterinary journal. Supplement. 1995 Sep:(19):5-17 [PubMed PMID: 8933064]
Level 3 (low-level) evidenceNaredo E, Monteagudo I. Doppler techniques. Clinical and experimental rheumatology. 2014 Jan-Feb:32(1 Suppl 80):S12-9 [PubMed PMID: 24529255]
Level 3 (low-level) evidencePellett AA, Kerut EK. The Doppler equation. Echocardiography (Mount Kisco, N.Y.). 2004 Feb:21(2):197-8 [PubMed PMID: 14961804]
Mao YK, Zhao BW, Zhou L, Wang B, Chen R, Wang SS. Z-score reference ranges for pulsed-wave Doppler indices of the cardiac outflow tracts in normal fetuses. The international journal of cardiovascular imaging. 2019 May:35(5):811-825. doi: 10.1007/s10554-018-01517-1. Epub 2019 Jan 8 [PubMed PMID: 30623353]
Bolger AF, Eidenvall L, Ask P, Loyd D, Wranne B. Understanding continuous-wave Doppler signal intensity as a measure of regurgitant severity. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 1997 Jul-Aug:10(6):613-22 [PubMed PMID: 9282351]
Level 3 (low-level) evidenceMowers KL, Fullerton JB, Hicks D, Singh GK, Johnson MC, Anwar S. 3D Echocardiography Provides Highly Accurate 3D Printed Models in Congenital Heart Disease. Pediatric cardiology. 2021 Jan:42(1):131-141. doi: 10.1007/s00246-020-02462-4. Epub 2020 Oct 20 [PubMed PMID: 33083888]
Lakatos BK, Tokodi M, Kispál E, Merkely B, Kovács A. Morphological and Functional Assessment of the Right Ventricle Using 3D Echocardiography. Journal of visualized experiments : JoVE. 2020 Oct 28:(164):. doi: 10.3791/61214. Epub 2020 Oct 28 [PubMed PMID: 33191942]
Sugimoto T, Dulgheru R, Marchetta S, Ilardi F, Contu L, Go YY, Lancellotti P. What Does 3D Echocardiography Add to 2D Echocardiography in the Assessment of Mitral Regurgitation? Current cardiology reports. 2017 Aug 24:19(10):90. doi: 10.1007/s11886-017-0901-7. Epub 2017 Aug 24 [PubMed PMID: 28840567]
Remenyi B, Davis K, Draper A, Bayley N, Paratz E, Reeves B, Appelbe A, Wheaton G, da Silva Almeida IT, Dos Santos J, Carapetis J, Francis JR. Single Parasternal-Long-Axis-View-Sweep Screening Echocardiographic Protocol to Detect Rheumatic Heart Disease: A Prospective Study of Diagnostic Accuracy. Heart, lung & circulation. 2020 Jun:29(6):859-866. doi: 10.1016/j.hlc.2019.02.196. Epub 2019 Jun 11 [PubMed PMID: 31320258]
Denault AY, Langevin S, Lessard MR, Courval JF, Desjardins G. Transthoracic echocardiographic evaluation of the heart and great vessels. Canadian journal of anaesthesia = Journal canadien d'anesthesie. 2018 Apr:65(4):449-472. doi: 10.1007/s12630-018-1068-4. Epub 2018 Jan 19 [PubMed PMID: 29352414]
Flower L, Madhivathanan PR, Andorka M, Olusanya O, Roshdy A, Sanfilippo F. Getting the most from the subcostal view: The rescue window for intensivists. Journal of critical care. 2021 Jun:63():202-210. doi: 10.1016/j.jcrc.2020.09.003. Epub 2020 Sep 13 [PubMed PMID: 32958350]
Zhang XY, Cao TS, Yuan LJ, Liu J, Duan YY. Value of the echocardiographic suprasternal view for diagnosis of patent ductus arteriosus subtypes. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2012 Sep:31(9):1421-7 [PubMed PMID: 22922622]
Hahn RT, Abraham T, Adams MS, Bruce CJ, Glas KE, Lang RM, Reeves ST, Shanewise JS, Siu SC, Stewart W, Picard MH. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2013 Sep:26(9):921-64. doi: 10.1016/j.echo.2013.07.009. Epub [PubMed PMID: 23998692]
Mahmood F, Shernan SK. Perioperative transoesophageal echocardiography: current status and future directions. Heart (British Cardiac Society). 2016 Aug 1:102(15):1159-67. doi: 10.1136/heartjnl-2015-307962. Epub 2016 Apr 5 [PubMed PMID: 27048769]
Level 3 (low-level) evidenceChiriac A, Kadkhodayan A, Pislaru SV, Dailey EJ, Scott CG, Buechler TE, Newman JS, Pellikka PA. Clinical Importance of Transthoracic Echocardiography with Direct Input from Treating Physicians. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2016 Mar:29(3):195-204. doi: 10.1016/j.echo.2015.11.009. Epub 2015 Dec 11 [PubMed PMID: 26687690]
Pellikka PA, Nagueh SF, Elhendy AA, Kuehl CA, Sawada SG, American Society of Echocardiography. American Society of Echocardiography recommendations for performance, interpretation, and application of stress echocardiography. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2007 Sep:20(9):1021-41 [PubMed PMID: 17765820]
Xie F, Zheng C, Yuh-Jer Shen A, Chen W. Extracting and analyzing ejection fraction values from electronic echocardiography reports in a large health maintenance organization. Health informatics journal. 2017 Dec:23(4):319-328. doi: 10.1177/1460458216651917. Epub 2016 Jun 7 [PubMed PMID: 27271114]
Boyd JH, Sirounis D, Maizel J, Slama M. Echocardiography as a guide for fluid management. Critical care (London, England). 2016 Sep 4:20(1):274. doi: 10.1186/s13054-016-1407-1. Epub 2016 Sep 4 [PubMed PMID: 27592289]
Fields JM, Davis J, Girson L, Au A, Potts J, Morgan CJ, Vetter I, Riesenberg LA. Transthoracic Echocardiography for Diagnosing Pulmonary Embolism: A Systematic Review and Meta-Analysis. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2017 Jul:30(7):714-723.e4. doi: 10.1016/j.echo.2017.03.004. Epub 2017 May 9 [PubMed PMID: 28495379]
Level 1 (high-level) evidenceSaksena S, Sra J, Jordaens L, Kusumoto F, Knight B, Natale A, Kocheril A, Nanda NC, Nagarakanti R, Simon AM, Viggiano MA, Lokhandwala T, Chandler ML, ICE-CHIP Investigator Study Group. A prospective comparison of cardiac imaging using intracardiac echocardiography with transesophageal echocardiography in patients with atrial fibrillation: the intracardiac echocardiography guided cardioversion helps interventional procedures study. Circulation. Arrhythmia and electrophysiology. 2010 Dec:3(6):571-7. doi: 10.1161/CIRCEP.110.936161. Epub 2010 Sep 18 [PubMed PMID: 20852299]
Level 1 (high-level) evidenceEnriquez A, Saenz LC, Rosso R, Silvestry FE, Callans D, Marchlinski FE, Garcia F. Use of Intracardiac Echocardiography in Interventional Cardiology: Working With the Anatomy Rather Than Fighting It. Circulation. 2018 May 22:137(21):2278-2294. doi: 10.1161/CIRCULATIONAHA.117.031343. Epub [PubMed PMID: 29784681]
Soos MP, McComb D. Instantaneous Wave-Free Ratio. StatPearls. 2026 Jan:(): [PubMed PMID: 31082183]
Pagourelias ED, Mirea O, Duchenne J, Unlu S, Van Cleemput J, Papadopoulos CE, Bogaert J, Vassilikos VP, Voigt JU. Speckle tracking deformation imaging to detect regional fibrosis in hypertrophic cardiomyopathy: a comparison between 2D and 3D echo modalities. European heart journal. Cardiovascular Imaging. 2020 Oct 20:21(11):1262-1272. doi: 10.1093/ehjci/jeaa057. Epub [PubMed PMID: 32294170]
Tanabe K. Three-Dimensional Echocardiography - Role in Clinical Practice and Future Directions. Circulation journal : official journal of the Japanese Circulation Society. 2020 Jun 25:84(7):1047-1054. doi: 10.1253/circj.CJ-20-0239. Epub 2020 May 12 [PubMed PMID: 32404540]
Level 3 (low-level) evidenceCai Q, Beckles DL, Ahmad M. Three-dimensional echocardiography assessment of carcinoid valvular heart disease: Images of each and all. Echocardiography (Mount Kisco, N.Y.). 2020 May:37(5):791-793. doi: 10.1111/echo.14679. Epub 2020 May 9 [PubMed PMID: 32386253]
Kato H, Nakanishi M, Maekawa N, Ohnishi T, Yamamoto M. Evaluation of left atrial appendage stasis in patients with atrial fibrillation using transesophageal echocardiography with an intravenous albumin-contrast agent. The American journal of cardiology. 1996 Aug 1:78(3):365-9 [PubMed PMID: 8759824]
von der Recke G, Schmidt H, Illien S, Lüderitz B, Omran H. Use of transesophageal contrast echocardiography for excluding left atrial appendage thrombi in patients with atrial fibrillation before cardioversion. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2002 Oct:15(10 Pt 2):1256-61 [PubMed PMID: 12411914]
Bernier M, Abdelmoneim SS, Stuart Moir W, Eifert Rain SS, Chandrasekaran K, Ammash NM, Mulvagh SL. CUTE-CV: a prospective study of enhanced left atrial appendage visualization with microbubble contrast agent use during transesophageal echocardiography guided cardioversion. Echocardiography (Mount Kisco, N.Y.). 2013 Oct:30(9):1091-7. doi: 10.1111/echo.12240. Epub 2013 May 11 [PubMed PMID: 23662846]