 Cytoreduction (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC)
Cytoreduction (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC)
Introduction
Cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) has transformed the management of peritoneal surface malignancies, offering select patients with these historically devastating diseases the potential for long-term survival and durable disease control.[1] Peritoneal surface malignancies arise either primarily from the peritoneum or through direct spread from gastrointestinal and gynecologic malignancies, typically presenting with diffuse nodular or mucinous involvement across multiple sites within the peritoneal cavity.[2] Patients with untreated peritoneal disease often experience progressive complications, including bowel obstruction, fistula formation, intractable pain, and cachexia.[1]
The concept of combining aggressive surgical cytoreduction with regional chemotherapy delivery was first described by Spratt in 1980 through animal experiments using a thermal transfusion infiltration system.[3] This technique was subsequently refined and popularized by Sugarbaker in the 1990s.[4] The procedure involves the systematic removal of all visible tumor implants, followed by the intraoperative administration of heated cytotoxic agents directly into the peritoneal cavity, where elevated temperatures enhance drug penetration and cytotoxicity against residual microscopic disease.[5][6][7]
Optimal outcomes depend on careful patient selection, accurate assessment of peritoneal tumor burden using the peritoneal cancer index, and achieving complete macroscopic cytoreduction. Each tumor histology has specific peritoneal cancer index thresholds beyond which surgical intervention is unlikely to confer meaningful survival benefit.[8] HIPEC protocols vary by tumor type and institutional practice, with cisplatin commonly used for ovarian cancer and mitomycin C or oxaliplatin for colorectal primaries, administered at 40 °C to 43 °C for 60 to 90 minutes.[9] This article reviews the principles, techniques, and clinical applications of CRS-HIPEC in the multidisciplinary treatment of peritoneal surface malignancies.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Peritoneal Cavity
The peritoneum is a serous membrane lining the abdominal cavity, composed of an outer connective tissue layer and an inner layer of mesothelial cells. These mesothelial cells provide the primary surface for tumor cell adhesion during the development of peritoneal metastases. The peritoneum is divided into the parietal peritoneum, which covers the abdominopelvic wall and diaphragm, and the visceral peritoneum, which envelops the intra-abdominal organs. The peritoneal cavity typically contains a small volume of fluid (10–100 mL) enriched with nutrients, signaling molecules, and immune cells that interact with the bloodstream. Diaphragmatic motion propels this fluid upward, while stomata in the diaphragmatic peritoneum connect to lymphatic vessels, facilitating the clearance of debris, bacteria, and cells into systemic circulation (see Image. Pathways of Peritoneal Fluid Movement).[10]
Pathophysiology of Peritoneal Malignancies
Peritoneal malignancy develops through a sequential process that includes cancer cell detachment, dissemination within the peritoneal cavity, adhesion to mesothelial surfaces, and invasion of the submesothelial stroma. Increased tumor stiffness and elevated interstitial fluid pressure facilitate the release of cancer cells by disrupting cell–cell junctions and inducing epithelial-to-mesenchymal transition, thereby increasing cell motility and resistance to anoikis (detachment-induced cell death). Tumor rupture, surgical manipulation, or leakage of bile and blood may also introduce malignant cells into the peritoneal space. Certain tumor types, particularly right-sided or mucinous colorectal cancers, exhibit a greater tendency for peritoneal dissemination, likely due to stromal-rich molecular features.[11]
After entering the peritoneal cavity, tumor cells, frequently organized as multicellular clusters, are transported by peritoneal fluid flow, diaphragmatic movement, and gravity to preferred implantation sites, including the pelvis, paracolic gutters, and subdiaphragmatic regions. The omentum is a common site of implantation because its immune-rich structures, known as milky spots or fat-associated lymphoid clusters, provide a supportive environment through inflammatory and angiogenic signaling.[11][12] Free-floating cancer cells attach to mesothelial cells and extracellular matrix components through adhesion molecules. This process is amplified by inflammation, surgical trauma, or increased intraperitoneal pressure.
Neutrophil extracellular traps and fibrin deposition further promote tumor cell binding and survival on the peritoneal surface.[12][13] Following attachment, cancer cells penetrate the mesothelial layer by secreting proteolytic enzymes, including matrix metalloproteinases, and by inducing apoptosis in mesothelial cells. Within the submesothelial stroma, these cells remodel the local microenvironment into a tumor-promoting niche that facilitates cancer cell proliferation, angiogenesis, and immune evasion.[12][13]
Mechanism of Action of CRS-HIPEC
CRS-HIPEC constitutes a 2-step approach for treating peritoneal malignancies. The initial step, cytoreduction, involves surgical removal of all visible tumor deposits. Subsequently, HIPEC targets residual microscopic disease by circulating heated chemotherapy within the peritoneal cavity.[14][15]
During HIPEC, the peritoneal cavity is perfused with chemotherapy heated to 40 °C to 43 °C for 60 to 90 minutes, combining pharmacologic and thermal effects to enhance tumor cell destruction. The peritoneal–plasma barrier enables high local drug concentrations, resulting in prolonged exposure of residual tumor cells while minimizing systemic toxicity. Hyperthermia increases chemotherapy efficacy by enhancing tumor cell membrane permeability and drug penetration. Also, it potentiates the activity of agents such as platinum compounds and alkylating agents by promoting DNA adduct formation and transiently inhibiting DNA repair mechanisms, including BRCA2-mediated pathways. In addition to direct cytotoxic effects, hyperthermia induces the expression of heat shock proteins, which stimulate antitumor immune responses, particularly by activating natural killer cells.[16][15]
Indications
CRS-HIPEC constitutes an aggressive locoregional treatment for peritoneal surface malignancies. Appropriate patient selection involves thorough assessment of tumor histology, disease extent as measured by the peritoneal cancer index, and the probability of achieving complete cytoreduction.[17] The efficacy of CRS-HIPEC depends on the removal of all macroscopic disease, as intraperitoneal chemotherapy penetrates only 2 to 3 mm into tissue and is ineffective against larger tumor deposits. Completeness of cytoreduction (CC) scoring determines resection adequacy: CC-0 indicates no visible residual disease; CC-1 indicates residual nodules of 2.5 mm or less; CC-2 (2.5 mm to 2.5 cm) and CC-3 (>2.5 cm) are associated with poorer outcomes and generally preclude HIPEC.[18]
Ovarian Cancer
HIPEC has demonstrated survival benefit specifically in patients with stage III epithelial ovarian cancer undergoing interval cytoreductive surgery following neoadjuvant chemotherapy.[17][19] The landmark OVHIPEC-1 trial randomized 245 patients to interval CRS with or without HIPEC using cisplatin and demonstrated improved recurrence-free survival (14.2 vs 10.7 months) and overall survival (45.7 vs 33.9 months) in the HIPEC arm, with no significant differences in adverse event rates.[20] These findings apply exclusively to patients achieving complete or optimal cytoreduction during interval surgery. Current evidence does not support HIPEC administration during primary debulking surgery, as the ongoing OVHIPEC-2 trial is evaluating this setting. Similarly, HIPEC for platinum-sensitive recurrent ovarian cancer lacks definitive evidence outside clinical trial protocols.[21]
Colorectal Cancer with Peritoneal Metastases
The role of HIPEC in colorectal peritoneal metastases remains controversial following publication of the PRODIGE 7 trial, which randomized 265 patients with colorectal peritoneal metastases to CRS alone versus CRS-HIPEC using oxaliplatin. The trial showed no difference in overall survival (41.7 vs 41.2 months) between the arms, while the HIPEC group had higher 60-day morbidity.[22] These results challenged the previously accepted role of HIPEC established by earlier studies and prompted reevaluation of treatment paradigms.
Current practice increasingly favors CRS combined with perioperative systemic chemotherapy rather than HIPEC for established colorectal peritoneal metastases. However, the HIPECT4 trial identified a potential prophylactic role, demonstrating that HIPEC added to CRS in patients with locally advanced T4 colon cancer at high risk for peritoneal recurrence reduced locoregional recurrence rates compared to surgery alone.[23] This prophylactic indication is an evolving area in which HIPEC may provide benefit by preventing, rather than treating, peritoneal metastases.[23] Patient selection for CRS, regardless of HIPEC administration, requires a limited peritoneal disease burden (generally a peritoneal cancer index <20), absence of extensive small-bowel involvement, and evidence of chemosensitivity, as demonstrated by stable or responding disease on systemic therapy.[24]
Gastric Cancer
Evidence supporting CRS-HIPEC for gastric cancer with peritoneal metastases remains limited, and indications are restricted to highly selected patients. Gastric peritoneal carcinomatosis historically carries a poor prognosis, with a median survival of 3 to 6 months with systemic therapy alone. CRS-HIPEC may be considered for patients with low-volume peritoneal disease (peritoneal cancer index ≤10), absence of distant metastases, and disease stability or response following at least 3 months of systemic chemotherapy.[17][25] Complete cytoreduction is paramount, as incomplete resection offers no survival advantage over systemic therapy alone.
The National Comprehensive Cancer Network recommends a multidisciplinary discussion before proceeding with CRS-HIPEC, emphasizing that treatment should be performed at high-volume centers with expertise in peritoneal surface malignancies. Prophylactic HIPEC following gastrectomy for serosa-positive gastric cancer has been evaluated in Asian populations with mixed results and is not standard practice in Western centers. Given the limited evidence base, enrollment in clinical trials is encouraged whenever possible.[25]
Appendiceal Neoplasms and Pseudomyxoma Peritonei
CRS-HIPEC represents the standard treatment for appendiceal mucinous neoplasms with peritoneal dissemination, including pseudomyxoma peritonei. Optimal candidates include patients with low-grade histology (low-grade appendiceal mucinous neoplasm or well-differentiated mucinous adenocarcinoma), absence of signet ring cell features, limited disease burden (peritoneal cancer index ≤21), and adequate performance status.[26] The Peritoneal Surface Oncology Group International consensus established histologic grade as the most important prognostic factor, with low-grade tumors achieving 10-year survival rates exceeding 70% following complete CRS-HIPEC. High-grade tumors, particularly those with signet ring cell differentiation, carry a significantly worse prognosis regardless of treatment approach.
Mitomycin C-based HIPEC regimens are most commonly employed for appendiceal neoplasms.[27] Repeat CRS-HIPEC may be considered for recurrent disease in carefully selected patients, particularly those with low-grade histology, prolonged disease-free interval following initial surgery, and limited peritoneal disease burden at recurrence. For high-grade recurrences, the interval since prior surgery and extent of recurrent disease should be carefully evaluated, with shorter intervals and extensive disease generally precluding repeat cytoreduction.[27][28]
Peritoneal Mesothelioma
CRS-HIPEC represents the preferred treatment for medically operable individuals with epithelioid peritoneal mesothelioma and unicavitary disease confined to the peritoneal cavity. Epithelioid histology is associated with significantly better outcomes compared to sarcomatoid or biphasic subtypes, with 5-year survival rates of 50% to 60% achievable at experienced centers. Optimal candidates have a peritoneal cancer index of less than 17, adequate performance status, and no pleural or extraperitoneal involvement. Cisplatin-based HIPEC regimens are most commonly employed, including cisplatin combined with doxorubicin, cisplatin alone, carboplatin, or cisplatin with mitomycin C.
The combination of CRS, HIPEC, and early postoperative intraperitoneal chemotherapy (EPIC) has been utilized at some centers, though comparative data are limited. CRS-HIPEC is not recommended as initial therapy for patients with sarcomatoid or biphasic histology, given poor outcomes; these patients should be treated with systemic therapy, with surgery considered only in highly selected cases demonstrating exceptional response. Bicavitary disease involving both pleural and peritoneal surfaces generally precludes curative-intent surgery, though sequential cytoreduction has been reported in isolated cases.[29]
Contraindications
Contraindications for CRS-HIPEC include inability to achieve complete cytoreduction, presence of extra-abdominal metastases, poor performance status, significant comorbidities, unresectable disease, elevated peritoneal cancer index, and high-risk histological features. Increased morbidity is associated with advanced age, frailty, poor nutritional status, hypoalbuminemia, and an American Society of Anesthesiologists score of 3 or higher.[30][31] Invasion of critical surgical sites such as the root of the mesentery, porta hepatis, and retroperitoneal structures also contraindicates CRS-HIPEC.
Impaired small bowel function with risk of short bowel syndrome is similarly a contraindication. These criteria are applicable across tumor types and are essential for appropriate patient selection.[32] Approximately one-quarter of patients undergoing exploratory surgery are ultimately found unsuitable for CRS-HIPEC, most commonly due to more extensive peritoneal disease than preoperative imaging suggested.[31]
Equipment
Prior to initiating this procedure in a hospital setting, it is essential to establish a chemotherapy approval system supported by surgical facilities and integrated with a medical-surgical resuscitation unit for patient monitoring. HIPEC may be performed using either an open or a closed l technique. In both approaches, the abdominal cavity is continuously perfused with a cytostatic solution heated to 40 °C to 43 °C via a drainage system with inlet and outlet catheters. Various pieces of equipment are required to perform this procedure.[15][33][34] This includes:
- A heat exchanger connected to a thermostat maintains a stable temperature of 40 °C to 43 °C in the inflow and outflow catheters to facilitate the infusion and distribution of the cytotoxic agent within the abdominal cavity.
- Temperature probes for monitoring temperatures within both the extracorporeal circuit and the peritoneal cavity.
- A roller pump to sustain the extracorporeal circulation of the cytotoxic agent.
- A reservoir for the cytotoxic agent.
- A computer system to regulate the heat exchanger and drainage pumps based on feedback from thermal probes.
- A timer to monitor the duration of infusion.
- Cytotoxic drugs for intra-abdominal chemotherapy, with mitomycin C, cisplatin, oxaliplatin, and paclitaxel being the most commonly used.
- The chemotherapeutic agent is administered with a carrier solution, typically 0.9% sodium chloride or 5% glucose. The volume of the carrier solution is determined according to the patient's body surface area, with typical infusion volumes ranging from 1.5 to 2 liters per square meter.
Personnel
CRS-HIPEC necessitates a multidisciplinary team comprising specialized surgical oncologists, anesthesiologists with expertise in complex oncologic procedures, perfusionists or trained surgical staff to operate the HIPEC delivery system, and intensive care specialists for postoperative management.[6] Surgeons with specialized training in cytoreductive techniques and peritonectomy procedures are essential. These operations frequently involve multivisceral resections and extensive peritoneal stripping, which require expertise beyond standard oncologic surgery. Due to the complexity and duration of these procedures, participation of multiple surgeons is often necessary.[35][36]
Anesthesiologists experienced in prolonged, complex oncologic procedures are required, as patients may undergo extended operations involving significant fluid shifts, challenges in temperature management during the hyperthermic phase, and the potential for substantial blood loss necessitating transfusion.[37] A perfusionist or specially trained surgical personnel is required to operate the HIPEC perfusion device, which functions similarly to a heart bypass system. This individual manages the circulation of heated chemotherapy solution through the abdominal cavity, maintaining temperatures between 40 °C and 43 °C during the 30- to 120-minute perfusion period.
The perfusion team is responsible for monitoring inflow and outflow catheters and ensuring adequate heating of the peritoneal surface.[36] Intensive care specialists and nursing staff with experience in managing postoperative complications from major oncologic surgery are essential, given the reported morbidity rates of 23% to 44% and the potential for serious complications such as fistulas, abscesses, bowel perforation, and renal failure. Specialized intensive care unit management is particularly important during the first 30 to 60 days postoperatively, when most major complications are likely to occur.[36]
Preparation
Patient Selection and Multidisciplinary Evaluation
A multidisciplinary tumor board should determine candidacy for CRS-HIPEC to ensure that decisions incorporate input from all relevant specialties.[34]
Prehabilitation and Optimization
Prehabilitation should commence once surgery is planned and continue throughout the recovery period. This approach enhances functional capacity and postoperative outcomes.[38][39] Key modifiable factors to optimize:
- Nutrition
- Poor nutritional status is associated with worse HIPEC outcomes; nutritional status should be optimized preoperatively.
- Physical fitness
- Preoperative exercise programs can improve patient performance status.
- Psychological health
- Counseling and mental health support services facilitate improved coping mechanisms.
- Smoking
- Active smoking should be identified and addressed before surgery.
Prehabilitation is particularly important given the significant nutritional, physical, and psychological burdens associated with advanced peritoneal disease.
Laboratory and Organ Function Assessment
Baseline laboratory assessment should be performed within 1 week before surgery and should include a complete blood count and evaluation of renal and hepatic function. Careful assessment of renal function is particularly important because HIPEC often involves high-dose cisplatin administration. Contraindications to proceeding include a creatinine clearance below 30 mL/min or a serum creatinine greater than 1 mg/dL.
Additional caution is warranted in patients with diabetes, preexisting neuropathy, hearing loss, or advanced age due to increased susceptibility to cisplatin toxicity. Perioperative exposure to nephrotoxic agents, including contrast media and nonsteroidal anti-inflammatory drugs, should be minimized. Prophylactic administration of sodium thiosulfate is recommended to mitigate the risk of cisplatin-induced nephrotoxicity.[40]
Institutional and Procedural Preparation
CRS-HIPEC should be performed at high-volume centers with experienced, multidisciplinary teams, as delivering intraperitoneal chemotherapy requires close coordination among surgical, anesthesia, nursing, and pharmacy personnel. While many high-volume institutions have developed formalized preoperative and perioperative pathways, there remains variability in practice patterns internationally. Key perioperative considerations include routine antiemetic prophylaxis and goal-directed fluid therapy to maintain hemodynamic stability and adequate tissue perfusion.
Advanced hemodynamic monitoring is recommended during the procedure, given the significant physiologic shifts associated with CRS-HIPEC. Multimodal analgesia strategies should be employed, often incorporating thoracic epidural analgesia when appropriate. Implementation of standardized, evidence-based perioperative care pathways, including enhanced recovery protocols, has been shown to improve outcomes, particularly in high-risk or complex cases.[40][41]
Technique or Treatment
CRS
CRS is an extensive operative procedure designed to remove all visible peritoneal tumor burden, with HIPEC administered subsequently to eradicate microscopic residual disease. The fundamental principle underlying treatment efficacy is achieving complete or near-complete macroscopic tumor removal, as intraperitoneal chemotherapy penetrates only 2 to 3 mm into tissue and cannot effectively treat larger deposits. Optimal cytoreduction leaves no gross residual disease or only nodules measuring 2.5 mm or less.[29][42]
Peritoneal Cancer Index Assessment
The peritoneal cancer index provides a standardized method for quantifying peritoneal tumor burden and guides both preoperative planning and intraoperative decision-making (see Image. Peritoneal Cancer Index). The abdominopelvic cavity is divided into 13 regions: 9 abdominopelvic regions (numbered 0–8) and 4 small bowel regions (numbered 9–12). Each region receives a lesion size score from 0 to 3, where 0 indicates no visible tumor, 1 denotes tumor deposits up to 0.5 cm, 2 indicates deposits between 0.5 and 5 cm, and 3 represents deposits exceeding 5 cm or confluent disease.
The sum of all regional scores yields a total peritoneal cancer index ranging from 0 to 39. A higher peritoneal cancer index is associated with a lower likelihood of achieving complete cytoreduction and a worse overall prognosis across tumor types. Peritoneal cancer index thresholds for surgical candidacy vary by histology, with appendiceal neoplasms tolerating higher scores (peritoneal cancer index [PCI] ≤20–21) than colorectal (PCI ≤15–20) or gastric malignancies (PCI ≤10).[25][29][42][43]
Peritonectomy Procedures
The surgical approach employs systematic peritonectomy tailored to tumor distribution, as initially described by Sugarbaker. Six distinct peritonectomy regions are addressed sequentially based on disease involvement. Anterior parietal peritonectomy involves resection of the peritoneum from the anterior abdominal wall, including the umbilicus and any prior surgical scars that may harbor tumor deposits. Electrosurgical dissection facilitates the separation of the peritoneum from the underlying musculature while maintaining hemostasis. The falciform ligament and round ligament are excised en bloc with the surrounding peritoneum.
Right upper quadrant peritonectomy addresses disease on the right hemidiaphragm, liver capsule, and hepatoduodenal ligament. Right subphrenic peritonectomy requires mobilization of the right hepatic lobe and careful dissection along the diaphragmatic surface, preserving the phrenic veins and avoiding diaphragmatic perforation. Glisson capsule resection may be necessary for tumor implants on the liver surface, performed using ball-tip electrocautery to strip the involved capsule while preserving the underlying parenchyma. Cholecystectomy is routinely performed to facilitate access and remove a common site of occult disease.
Left upper quadrant peritonectomy addresses the left hemidiaphragm, splenic hilum, and greater curvature of the stomach. Splenectomy is frequently required when the tumor involves the splenic hilum or capsule, and is performed en bloc with greater omentectomy. The greater omentum is resected from the transverse colon and the gastric greater curvature, ligating the gastroepiploic vessels. Careful attention to the short gastric vessels and splenic flexure of the colon is essential to avoid iatrogenic injury.
Pelvic peritonectomy addresses tumors within the pelvis, including disease on the bladder peritoneum, cul-de-sac, and pelvic sidewalls. In women, total hysterectomy with bilateral salpingo-oophorectomy is commonly performed, with en bloc resection of the rectosigmoid when involved. Careful dissection along the pelvic sidewalls identifies and preserves the ureters while removing the involved peritoneum.
The presacral space may require dissection in cases of posterior cul-de-sac disease. Lesser omentectomy removes the gastrohepatic ligament and provides access to the lesser sac, which frequently harbors tumor deposits. Complete lesser sac peritonectomy may require stripping of the peritoneum from the posterior stomach, pancreatic capsule, and transverse mesocolon.[44][45]
Visceral Resections
Visceral resections are performed based on tumor involvement and follow oncologic principles. Omentectomy (greater and lesser) is performed in nearly all cases, as the omentum serves as a preferential site for peritoneal metastases. Bowel resections are performed for tumors involving the intestinal serosa, mesentery, or bowel wall, with primary anastomosis or stoma creation depending on the extent of resection, nutritional status, and anastomotic reliability. Multiple bowel resections may be necessary, though preservation of intestinal length is prioritized to avoid short bowel syndrome. Small bowel involvement, pervasive serosal disease, or mesenteric retraction represents a relative contraindication to cytoreduction, given the difficulty of achieving complete resection while maintaining adequate intestinal function.
Additional visceral resections may include appendectomy (routine in most cases), partial hepatectomy for parenchymal invasion, distal pancreatectomy for tail involvement, partial gastrectomy for serosal or transmural disease, and segmental ureterectomy with reconstruction for ureteral involvement. The decision to proceed with extensive visceral resections requires careful consideration of the likelihood of achieving complete cytoreduction, balanced against operative morbidity and functional outcomes.[44][46]
Technical Considerations
Electrosurgical technique is fundamental to cytoreductive surgery, with ball-tip electrocautery used extensively for peritoneal stripping. High-voltage cutting current facilitates tissue separation while coagulation current achieves hemostasis. Argon beam coagulation provides superficial tissue destruction in areas of minimal residual disease and aids hemostasis on raw peritonectomy surfaces. Careful attention to tissue planes minimizes blood loss and facilitates identification of residual tumor deposits.
Systematic exploration of all abdominopelvic regions ensures comprehensive tumor assessment. Adhesiolysis is performed to expose all peritoneal surfaces, and inspection includes the diaphragmatic surfaces, paracolic gutters, small bowel mesentery, pelvis, and omental bursa. Palpation of the small bowel from the ligament of Treitz to the ileocecal valve identifies serosal implants that may not be visually apparent.[44][45][47]
Completeness of Cytoreduction Scoring
The CC score quantifies residual disease following surgical resection and represents the strongest independent prognostic factor across all peritoneal surface malignancies. CC-0 indicates no visible residual disease, while CC-1 denotes residual nodules measuring 2.5 mm or less, both considered optimal outcomes amenable to HIPEC efficacy. CC-2 describes residual nodules between 2.5 mm and 2.5 cm, and CC-3 indicates nodules exceeding 2.5 cm; neither score is associated with a meaningful survival benefit from HIPEC administration. Achieving CC-0 or CC-1 cytoreduction should be the operative goal, and cases where complete cytoreduction appears unattainable may warrant abandonment of the procedure or conversion to palliative resection, depending on clinical circumstances.[29][42]
HIPEC Administration
HIPEC can be delivered using open (coliseum) or closed techniques, both of which demonstrate acceptable safety and efficacy when properly executed. Technique selection depends on institutional experience, surgeon preference, and patient factors. The open coliseum technique elevates the skin edges using a self-retaining retractor system to create an exposed abdominal cavity resembling a coliseum. Heated perfusate maintained at 40 °C to 43 °C circulates through the peritoneal cavity via a pump system that delivers 3 to 4 liters of chemotherapy solution through strategically placed inflow and outflow catheters.
Temperature probes monitor perfusate and tissue temperatures to ensure therapeutic hyperthermia. The primary advantage of the open technique is the ability to perform manual stirring throughout perfusion, promoting uniform distribution of chemotherapy across all peritoneal surfaces and preventing pooling in dependent areas. Disadvantages include greater heat loss, which requires higher inflow temperatures, and potential exposure of operating room personnel to aerosolized cytotoxic agents, necessitating appropriate protective equipment and ventilation.[15]
The closed technique involves placement of inflow and outflow catheters along with temperature probes, followed by temporary skin closure to create a sealed perfusion circuit. This approach minimizes heat loss, allowing more consistent maintenance of target temperatures, and substantially reduces operating room staff exposure to chemotherapy. Newer systems incorporating carbon dioxide recirculation have been developed to improve perfusate distribution within the closed abdomen. The primary disadvantage is the inability to perform manual manipulation during perfusion, which may limit the uniform distribution of chemotherapy throughout the peritoneal cavity, particularly in areas with adhesions or complex anatomy.[15][48]
Complications
CRS-HIPEC carries substantial perioperative risk, with contemporary series reporting major morbidity rates of 19% to 44% and mortality rates of 0% to 2.3%. The most frequent complications involve the gastrointestinal, infectious, renal, and hematologic systems. Serious (grade ≥3) complications occur in 9% to 40% of patients, with 32% to 42% experiencing severe events within 30 days.[22][49][50][51]
Gastrointestinal
- Digestive fistulas: 7% to 11%, among the most severe complications
- Anastomotic leaks: 5% to 10.5%
- Abscesses: 3%to 5%
- Bowel perforation and ileus
- Surgical site infections: ~7%
- Broader infectious complications include wound infections, sepsis, pneumonia, central line infections, and intra-abdominal abscesses
Renal
Particularly associated with cisplatin-based HIPEC:
- Elevated creatinine: ~15% (median onset 5 days postop)
- Renal insufficiency/failure requiring intervention
- Age 58 and older is an independent risk factor
Hematologic
These are more common with HIPEC, especially oxaliplatin-based regimens.
Other Major Complications
- Hemorrhage requiring transfusion
- Venous thromboembolism
- Myocardial infarction
- Pleural effusion, pneumothorax
- Pulmonary complications
- Wound dehiscence
Clinical Significance
Peritoneal surface malignancies historically carried a dismal prognosis, with median survival measured in months when treated with systemic chemotherapy alone. The development of cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy fundamentally transformed the treatment paradigm for selected patients with peritoneal carcinomatosis, converting a previously terminal diagnosis into a potentially curable condition. This aggressive locoregional approach exploits the pharmacokinetic advantage of intraperitoneal drug delivery, achieving peritoneal drug concentrations 20 to 1000 times higher than plasma levels while minimizing systemic toxicity. Hyperthermia enhances chemotherapy cytotoxicity by increasing cellular drug uptake, impairing DNA repair mechanisms, and directly injuring tumor cells. The combination of complete macroscopic tumor removal with high-dose regional chemotherapy addresses both visible disease and microscopic residual tumor deposits that would otherwise serve as sources of recurrence.[15]
The clinical impact of CRS-HIPEC varies substantially by tumor histology, with the most significant benefit observed in appendiceal neoplasms and pseudomyxoma peritonei. Patients with low-grade appendiceal mucinous neoplasms treated with complete cytoreduction and HIPEC achieve 10-year survival rates of 70% to 80%, representing a dramatic improvement over historical outcomes with debulking surgery alone.[52] Peritoneal mesothelioma, previously uniformly fatal, demonstrates 5-year survival rates of 50% to 60% following CRS-HIPEC in patients with epithelioid histology and limited disease burden.[53]
Women with ovarian cancer undergoing interval CRS-HIPEC following neoadjuvant chemotherapy experience improved recurrence-free and overall survival compared to surgery alone, as demonstrated in the OVHIPEC-1 trial.[20] The role of colorectal peritoneal metastases remains more controversial following the PRODIGE 7 trial. However, CRS with perioperative systemic therapy continues to offer survival benefits over systemic chemotherapy alone in selected patients.[22]
Patient selection represents the most critical determinant of outcomes, as the substantial morbidity associated with CRS-HIPEC is justified only when complete cytoreduction is achievable and durable disease control is anticipated. The completeness of cytoreduction consistently emerges as the strongest prognostic factor across all tumor types, with incomplete resection conferring no survival advantage over palliative approaches while exposing patients to significant surgical risk. Tumor histology, peritoneal cancer index, and response to preoperative systemic therapy further stratify outcomes and guide treatment decisions. Centralization of care at high-volume centers with multidisciplinary expertise has improved outcomes through refined patient selection, surgical technique, and perioperative management. The learning curve for CRS-HIPEC is substantial, with institutional experience correlating directly with morbidity, mortality, and oncologic outcomes.[41]
The morbidity profile of CRS-HIPEC reflects the extensive nature of the procedure, with major complication rates of 30% to 50% reported across large series. Common complications include anastomotic leak, intra-abdominal abscess, wound infection, venous thromboembolism, and prolonged ileus. Perioperative mortality ranges from 1% to 5% at experienced centers, with higher rates observed during institutional learning curves and in patients with extensive disease requiring multiple visceral resections.[50] The physiologic stress of prolonged surgery, large-volume fluid shifts, and chemotherapy exposure necessitates careful patient selection based on performance status, nutritional parameters, and comorbid conditions. Despite this morbidity, quality-of-life studies demonstrate a return to baseline function in most patients within 6 to 12 months, with long-term survivors reporting satisfactory quality of life comparable to that of the general population.[54]
The integration of CRS-HIPEC into the broader oncologic treatment algorithm requires coordination with systemic therapy, with sequencing dependent on tumor type and clinical circumstances. Neoadjuvant chemotherapy serves multiple purposes: assessing tumor biology through treatment response, controlling micrometastatic disease, and potentially reducing peritoneal tumor burden to facilitate complete cytoreduction. Adjuvant systemic therapy following CRS-HIPEC targets distant micrometastatic disease and may reduce the risk of peritoneal recurrence, although optimal regimens and durations remain areas of active investigation. The expanding role of targeted therapies and immunotherapy in peritoneal malignancies presents opportunities for integration with locoregional treatment, with ongoing clinical trials evaluating novel combinations.
Enhancing Healthcare Team Outcomes
Interprofessional collaboration in CRS-HIPEC relies on structured multidisciplinary tumor board decision-making, coordinated preoperative planning, standardized perioperative protocols, and continuous communication to optimize patient selection, surgical outcomes, and complication management. Surgical oncologists, medical oncologists, radiologists, pathologists, anesthesiologists, intensivists, pharmacists, and specialized nursing staff collectively assess disease biology, resectability, peritoneal cancer index, imaging, and patient fitness to determine candidacy and guide preparation. Radiologists refine staging and operative planning, anesthesia teams manage complex physiologic demands with goal-directed therapy and advanced monitoring, and all personnel require dedicated HIPEC training to ensure safe chemotherapy delivery.
Centers benefit from standardized pathways, including prehabilitation, nephrotoxicity prevention, antiemetic strategies, and multimodal pain control, to reduce variability and improve safety. Intraoperatively, real-time communication supports perfusion management and confirmation of complete cytoreduction before HIPEC administration. Postoperatively, experienced intensive care unit teams manage high-risk complications and implement early recovery measures. At the same time, long-term surveillance and decisions on systemic therapy or repeat CRS-HIPEC are coordinated through ongoing multidisciplinary review. High-volume centers with established multidisciplinary team models consistently demonstrate higher rates of complete cytoreduction, fewer complications, and shorter learning curves, underscoring the critical role of institutional experience and sustained team-based collaboration.
Nursing, Allied Health, and Interprofessional Team Interventions
To perform a HIPEC safely, a qualified nursing team for the operating room and postoperative recovery is needed. Nurses must be trained in intensive care units and the operating room to manage intraoperative and postoperative complications without difficulty.
Nursing, Allied Health, and Interprofessional Team Monitoring
HIPEC must be carried out in university centers equipped with invasive vital signs monitoring and management of complications related to both surgery and the toxicity of cytotoxic drugs. This involves invasive monitoring of arterial pressure, central venous pressure, cardiac output, and peripheral vascular resistance.
Media
(Click Image to Enlarge)
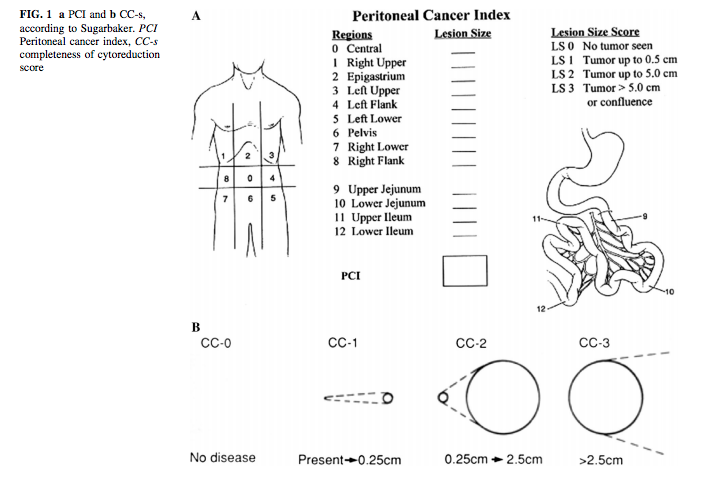
Peritoneal Cancer Index. The peritoneal cancer index (PCI) is a standardized quantitative tool for estimating the extent and distribution of peritoneal surface malignancies (PSMs).
Contributed by F Moustarah, MD, MPH, and J Desai, MBBS; adapted from Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res. 1996;82:359-374. doi: 10.1007/978-1-4613-1247-5_23.
(Click Image to Enlarge)
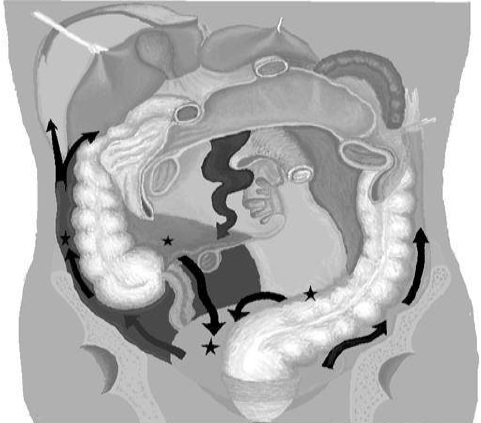
Pathways of Peritoneal Fluid Movement. The constant movement of peritoneal fluid, driven partly by diaphragmatic contractions and gravity, influences where malignant cells may implant within the abdomen.
Mikael Häggström, Public Domain, via Wikimedia Commons
{kind=link}
References
Lambert LA, Wiseman J. Palliative Management of Peritoneal Metastases. Annals of surgical oncology. 2018 Aug:25(8):2165-2171. doi: 10.1245/s10434-018-6335-7. Epub 2018 Jan 30 [PubMed PMID: 29383612]
Cortés-Guiral D, Hübner M, Alyami M, Bhatt A, Ceelen W, Glehen O, Lordick F, Ramsay R, Sgarbura O, Van Der Speeten K, Turaga KK, Chand M. Primary and metastatic peritoneal surface malignancies. Nature reviews. Disease primers. 2021 Dec 16:7(1):91. doi: 10.1038/s41572-021-00326-6. Epub 2021 Dec 16 [PubMed PMID: 34916522]
Spratt JS, Adcock RA, Sherrill W, Travathen S. Hyperthermic peritoneal perfusion system in canines. Cancer research. 1980 Feb:40(2):253-5 [PubMed PMID: 7356508]
Level 3 (low-level) evidenceJacquet P, Stephens AD, Averbach AM, Chang D, Ettinghausen SE, Dalton RR, Steves MA, Sugarbaker PH. Analysis of morbidity and mortality in 60 patients with peritoneal carcinomatosis treated by cytoreductive surgery and heated intraoperative intraperitoneal chemotherapy. Cancer. 1996 Jun 15:77(12):2622-9 [PubMed PMID: 8640714]
Stewart JH 4th, Shen P, Levine EA. Intraperitoneal hyperthermic chemotherapy: an evolving paradigm for the treatment of peritoneal surface malignancies. Expert review of anticancer therapy. 2008 Nov:8(11):1809-18. doi: 10.1586/14737140.8.11.1809. Epub [PubMed PMID: 18983241]
Jafari MD, Halabi WJ, Stamos MJ, Nguyen VQ, Carmichael JC, Mills SD, Pigazzi A. Surgical outcomes of hyperthermic intraperitoneal chemotherapy: analysis of the american college of surgeons national surgical quality improvement program. JAMA surgery. 2014 Feb:149(2):170-5. doi: 10.1001/jamasurg.2013.3640. Epub [PubMed PMID: 24352601]
Level 2 (mid-level) evidenceElias DM, Ouellet JF. Intraperitoneal chemohyperthermia: rationale, technique, indications, and results. Surgical oncology clinics of North America. 2001 Oct:10(4):915-33, xi [PubMed PMID: 11641098]
Stewart JH 4th, Blazer DG 3rd, Calderon MJG, Carter TM, Eckhoff A, Al Efishat MA, Fernando DG, Foster JM, Hayes-Jordan A, Johnston FM, Lautz TB, Levine EA, Maduekwe UN, Mangieri CW, Moaven O, Mogal H, Shen P, Votanopoulos KI. The Evolving Management of Peritoneal Surface Malignancies. Current problems in surgery. 2021 Apr:58(4):100860. doi: 10.1016/j.cpsurg.2020.100860. Epub 2020 Jul 14 [PubMed PMID: 33832580]
Srinivas Rao S, Uma Baskaran N, Cao J, Catalano OA, Brink JA, Cusack JC, Kambadakone AR. Imaging in Hyperthermic Intraperitoneal Chemotherapy. Radiographics : a review publication of the Radiological Society of North America, Inc. 2025 May:45(5):e240124. doi: 10.1148/rg.240124. Epub [PubMed PMID: 40310749]
Bermo MS, Koppula B, Kumar M, Leblond A, Matesan MC. The Peritoneum: What Nuclear Radiologists Need to Know. Seminars in nuclear medicine. 2020 Sep:50(5):405-418. doi: 10.1053/j.semnuclmed.2020.04.005. Epub 2020 Jun 10 [PubMed PMID: 32768005]
Demuytere J, Ernst S, Ceelen W. Pathophysiology of Peritoneal Metastasis. Journal of surgical oncology. 2024 Nov:130(6):1299-1305. doi: 10.1002/jso.27890. Epub 2024 Oct 13 [PubMed PMID: 39400354]
Bootsma S, Bijlsma MF, Vermeulen L. The molecular biology of peritoneal metastatic disease. EMBO molecular medicine. 2023 Mar 8:15(3):e15914. doi: 10.15252/emmm.202215914. Epub 2023 Jan 26 [PubMed PMID: 36700339]
Mikuła-Pietrasik J, Uruski P, Tykarski A, Książek K. The peritoneal "soil" for a cancerous "seed": a comprehensive review of the pathogenesis of intraperitoneal cancer metastases. Cellular and molecular life sciences : CMLS. 2018 Feb:75(3):509-525. doi: 10.1007/s00018-017-2663-1. Epub 2017 Sep 27 [PubMed PMID: 28956065]
Lim PQ, Han IH, Seow KM, Chen KH. Hyperthermic Intraperitoneal Chemotherapy (HIPEC): An Overview of the Molecular and Cellular Mechanisms of Actions and Effects on Epithelial Ovarian Cancers. International journal of molecular sciences. 2022 Sep 3:23(17):. doi: 10.3390/ijms231710078. Epub 2022 Sep 3 [PubMed PMID: 36077477]
Level 3 (low-level) evidencevan Stein RM, Aalbers AGJ, Sonke GS, van Driel WJ. Hyperthermic Intraperitoneal Chemotherapy for Ovarian and Colorectal Cancer: A Review. JAMA oncology. 2021 Aug 1:7(8):1231-1238. doi: 10.1001/jamaoncol.2021.0580. Epub [PubMed PMID: 33956063]
Pletcher E, Gleeson E, Labow D. Peritoneal Cancers and Hyperthermic Intraperitoneal Chemotherapy. The Surgical clinics of North America. 2020 Jun:100(3):589-613. doi: 10.1016/j.suc.2020.02.009. Epub 2020 Apr 16 [PubMed PMID: 32402303]
Gurusamy K, Leung J, Vale C, Roberts D, Linden A, Tan XW, Taribagil P, Patel S, Pizzo E, Davidson B, Saunders M, Aziz O, O'Dwyer ST. Cytoreductive surgery plus hyperthermic intraoperative peritoneal chemotherapy for people with peritoneal metastases from colorectal, ovarian or gastric origin: A systematic review of randomized controlled trials. World journal of surgery. 2024 Jun:48(6):1385-1403. doi: 10.1002/wjs.12186. Epub 2024 Apr 24 [PubMed PMID: 38658171]
Level 1 (high-level) evidenceGlehen O, Mohamed F, Gilly FN. Peritoneal carcinomatosis from digestive tract cancer: new management by cytoreductive surgery and intraperitoneal chemohyperthermia. The Lancet. Oncology. 2004 Apr:5(4):219-28 [PubMed PMID: 15050953]
Armstrong DK, Alvarez RD, Bakkum-Gamez JN, Barroilhet L, Behbakht K, Berchuck A, Chen LM, Cristea M, DeRosa M, Eisenhauer EL, Gershenson DM, Gray HJ, Grisham R, Hakam A, Jain A, Karam A, Konecny GE, Leath CA, Liu J, Mahdi H, Martin L, Matei D, McHale M, McLean K, Miller DS, O'Malley DM, Percac-Lima S, Ratner E, Remmenga SW, Vargas R, Werner TL, Zsiros E, Burns JL, Engh AM. Ovarian Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network : JNCCN. 2021 Feb 2:19(2):191-226. doi: 10.6004/jnccn.2021.0007. Epub 2021 Feb 2 [PubMed PMID: 33545690]
Level 1 (high-level) evidenceAronson SL, Lopez-Yurda M, Koole SN, Schagen van Leeuwen JH, Schreuder HWR, Hermans RHM, de Hingh IHJT, van Gent MDJM, Arts HJG, van Ham MAPC, van Dam PA, Vuylsteke P, Aalbers AGJ, Verwaal VJ, Van de Vijver KK, Aaronson NK, Sonke GS, van Driel WJ. Cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy in patients with advanced ovarian cancer (OVHIPEC-1): final survival analysis of a randomised, controlled, phase 3 trial. The Lancet. Oncology. 2023 Oct:24(10):1109-1118. doi: 10.1016/S1470-2045(23)00396-0. Epub 2023 Sep 11 [PubMed PMID: 37708912]
Level 1 (high-level) evidenceCaruso G, Weroha SJ, Cliby W. Ovarian Cancer: A Review. JAMA. 2025 Oct 14:334(14):1278-1291. doi: 10.1001/jama.2025.9495. Epub [PubMed PMID: 40690248]
Quénet F, Elias D, Roca L, Goéré D, Ghouti L, Pocard M, Facy O, Arvieux C, Lorimier G, Pezet D, Marchal F, Loi V, Meeus P, Juzyna B, de Forges H, Paineau J, Glehen O, UNICANCER-GI Group and BIG Renape Group. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): a multicentre, randomised, open-label, phase 3 trial. The Lancet. Oncology. 2021 Feb:22(2):256-266. doi: 10.1016/S1470-2045(20)30599-4. Epub 2021 Jan 18 [PubMed PMID: 33476595]
Level 1 (high-level) evidenceArjona-Sánchez A, Barrios P, Boldo-Roda E, Camps B, Carrasco-Campos J, Concepción Martín V, García-Fadrique A, Gutiérrez-Calvo A, Morales R, Ortega-Pérez G, Pérez-Viejo E, Prada-Villaverde A, Torres-Melero J, Vicente E, Villarejo-Campos P, Sánchez-Hidalgo JM, Casado-Adam A, García-Martin R, Medina M, Caro T, Villar C, Aranda E, Cano-Osuna MT, Díaz-López C, Torres-Tordera E, Briceño-Delgado FJ, Rufián-Peña S. HIPECT4: multicentre, randomized clinical trial to evaluate safety and efficacy of Hyperthermic intra-peritoneal chemotherapy (HIPEC) with Mitomycin C used during surgery for treatment of locally advanced colorectal carcinoma. BMC cancer. 2018 Feb 13:18(1):183. doi: 10.1186/s12885-018-4096-0. Epub 2018 Feb 13 [PubMed PMID: 29439668]
Level 1 (high-level) evidenceKazanowski M, Lesiak P, Wierzbicki J, Kapturkiewicz B, Maciejewski P, Pawłowski M, Jastrzębski T, Bębenek M. Peritoneal Cancer Index Dominates Prognosis After CRS-HIPEC for Colorectal Peritoneal Metastases: A Consecutive Single-Centre Cohort with 3-Year Follow-Up. Cancers. 2025 Nov 10:17(22):. doi: 10.3390/cancers17223614. Epub 2025 Nov 10 [PubMed PMID: 41300980]
Ajani JA, D'Amico TA, Bentrem DJ, Corvera CU, Das P, Enzinger PC, Enzler T, Gerdes H, Gibson MK, Grierson P, Gupta G, Hofstetter WL, Ilson DH, Jalal S, Kim S, Kleinberg LR, Klempner S, Lacy J, Lee B, Licciardi F, Lloyd S, Ly QP, Matsukuma K, McNamara M, Merkow RP, Miller AM, Mukherjee S, Mulcahy MF, Perry KA, Pimiento JM, Reddi DM, Reznik S, Roses RE, Strong VE, Su S, Uboha N, Wainberg ZA, Willett CG, Woo Y, Yoon HH, McMillian NR, Stein M. Gastric Cancer, Version 2.2025, NCCN Clinical Practice Guidelines In Oncology. Journal of the National Comprehensive Cancer Network : JNCCN. 2025 May:23(5):169-191. doi: 10.6004/jnccn.2025.0022. Epub [PubMed PMID: 40341199]
Level 1 (high-level) evidenceBai M, Li Y, Pu H, Xu Y, Chen J, Xu H, Wei H, Liang G, Ma R, Feng J. Optimal peritoneal cancer index cutoff point for predicting surgical resectability of pseudomyxoma peritonei in treatment-naive patients. World journal of surgical oncology. 2024 Jan 31:22(1):39. doi: 10.1186/s12957-024-03318-4. Epub 2024 Jan 31 [PubMed PMID: 38297355]
Godfrey EL, Mahoney F, Bansal VV, Su DG, Hanna DN, Lopez-Ramirez F, Baron E, Turaga KK, Benson AB 3rd, Setia N, Winer JH, Gunderson CG, Shah R, Magge DR, Solsky I, Eng C, Eng OS, Shergill A, Shen JP, Misdraji J, Foote MB, Luo W, Peritoneal Surface Malignancies (PSM) Consortium Group. Consensus Guideline for the Management of Patients with Appendiceal Tumors, Part 2: Appendiceal Tumors with Peritoneal Involvement. Annals of surgical oncology. 2025 Jun 25:():. doi: 10.1245/s10434-025-17364-z. Epub 2025 Jun 25 [PubMed PMID: 40560501]
Level 3 (low-level) evidenceLopez-Ramirez F, Gushchin V, Sittig M, King MC, Baron E, Nikiforchin A, Nieroda C, Sardi A. Iterative Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy for Recurrent Mucinous Adenocarcinoma of the Appendix. Annals of surgical oncology. 2022 Jun:29(6):3390-3401. doi: 10.1245/s10434-021-11233-1. Epub 2022 Feb 8 [PubMed PMID: 35133518]
Ettinger DS, Wood DE, Stevenson J, Aisner DL, Akerley W, Bauman JR, Bharat A, Bruno DS, Chang JY, Chirieac LR, DeCamp M, Dilling TJ, Dowell J, Durm GA, Gettinger S, Grotz TE, Gubens MA, Hegde A, Lackner RP, Lanuti M, Lin J, Loo BW, Lovly CM, Maldonado F, Massarelli E, Morgensztern D, Mullikin TC, Ng T, Otterson GA, Patel SP, Patil T, Polanco PM, Riely GJ, Riess J, Shapiro TA, Singh AP, Tam A, Tanvetyanon T, Yanagawa J, Yang SC, Yau E, Gregory KM, Hughes M. Mesothelioma: Peritoneal, Version 2.2023, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network : JNCCN. 2023 Sep:21(9):961-979. doi: 10.6004/jnccn.2023.0045. Epub [PubMed PMID: 37673108]
Level 1 (high-level) evidenceAuer RC, Sivajohanathan D, Biagi J, Conner J, Kennedy E, May T. Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: a systematic review. European journal of cancer (Oxford, England : 1990). 2020 Mar:127():76-95. doi: 10.1016/j.ejca.2019.10.034. Epub 2020 Jan 24 [PubMed PMID: 31986452]
Level 1 (high-level) evidencevan Oudheusden TR, Braam HJ, Luyer MD, Wiezer MJ, van Ramshorst B, Nienhuijs SW, de Hingh IH. Peritoneal cancer patients not suitable for cytoreductive surgery and HIPEC during explorative surgery: risk factors, treatment options, and prognosis. Annals of surgical oncology. 2015 Apr:22(4):1236-42. doi: 10.1245/s10434-014-4148-x. Epub 2014 Oct 16 [PubMed PMID: 25319584]
Ben-Yaacov A, Laks S, Goldenshluger M, Nevo Y, Mor E, Schtrechman G, Margalit O, Boursi B, Shacham-Shmueli E, Halpern N, Purim O, Hazzan D, Segev L, Zippel D, Adileh M, Nissan A. Impact of "critical lesions" on outcomes following cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2021 Nov:47(11):2933-2938. doi: 10.1016/j.ejso.2021.05.022. Epub 2021 May 19 [PubMed PMID: 34088586]
Chambers LM, Costales AB, Crean-Tate K, Kuznicki M, Morton M, Horowitz M, Jagielo T, Rose PG, Michener C, Vargas R, Debernardo R. A guide to establishing a hyperthermic intraperitoneal chemotherapy program in gynecologic oncology. Gynecologic oncology. 2020 Sep:158(3):794-802. doi: 10.1016/j.ygyno.2020.06.487. Epub 2020 Jul 2 [PubMed PMID: 32624234]
Hübner M, van Der Speeten K, Govaerts K, de Hingh I, Villeneuve L, Kusamura S, Glehen O. 2022 Peritoneal Surface Oncology Group International Consensus on HIPEC Regimens for Peritoneal Malignancies: Colorectal Cancer. Annals of surgical oncology. 2024 Jan:31(1):567-576. doi: 10.1245/s10434-023-14368-5. Epub 2023 Nov 8 [PubMed PMID: 37940803]
Level 3 (low-level) evidenceKusamura S, Barretta F, Yonemura Y, Sugarbaker PH, Moran BJ, Levine EA, Goere D, Baratti D, Nizri E, Morris DL, Glehen O, Sardi A, Barrios P, Quénet F, Villeneuve L, Gómez-Portilla A, de Hingh I, Ceelen W, Pelz JOW, Piso P, González-Moreno S, Van Der Speeten K, Deraco M, Peritoneal Surface Oncology Group International (PSOGI) and the French National Registry of Rare Peritoneal Surface Malignancies (RENAPE). The Role of Hyperthermic Intraperitoneal Chemotherapy in Pseudomyxoma Peritonei After Cytoreductive Surgery. JAMA surgery. 2021 Mar 1:156(3):e206363. doi: 10.1001/jamasurg.2020.6363. Epub 2021 Mar 10 [PubMed PMID: 33502455]
Foster JM, Sleightholm R, Patel A, Shostrom V, Hall B, Neilsen B, Bartlett D, Smith L. Morbidity and Mortality Rates Following Cytoreductive Surgery Combined With Hyperthermic Intraperitoneal Chemotherapy Compared With Other High-Risk Surgical Oncology Procedures. JAMA network open. 2019 Jan 4:2(1):e186847. doi: 10.1001/jamanetworkopen.2018.6847. Epub 2019 Jan 4 [PubMed PMID: 30646202]
González Sánchez S, García Fernández J, Cascales-Campos PA, Gonzalez Gil A, Manzanedo I, Pereira Perez F, Díaz Gómez D, González-de Pedro C, Asensio Diaz E, Pacheco Sanchez D, Prada-Villaverde A, Jaén Torrejimeno I, Lacueva J, Caravaca-Garcia I, Torres-Melero J, Sanchez-García S, Díaz Reques E, Ramírez Plaza C, Gutiérrez-Calvo A, González Bayón L, Morales-Soriano R, López-Mozos F, Bjelic L, Galindo Álvarez J, Marcello Fernandez ME, Turienzo Santos E, Titos García A, Álvarez Seoane R, Artiles Armas M, Garaulet ET, Villarejo Campos P, Boldó Roda E, Rihuete Caro C, García Fadrique A, Arjona-Sánchez Á, REGECOP collaborators. Interval Cytoreductive Surgery and Cisplatin- or Paclitaxel-Based HIPEC for Advanced Ovarian Cancer. JAMA network open. 2025 Jun 2:8(6):e2517676. doi: 10.1001/jamanetworkopen.2025.17676. Epub 2025 Jun 2 [PubMed PMID: 40569595]
Strijker D, Meijerink WJHJ, Bremers AJA, de Reuver P, van Laarhoven CJHM, van den Heuvel B. Prehabilitation to improve postoperative outcomes in patients with peritoneal carcinomatosis undergoing hyperthermic intraperitoneal chemotherapy (HIPEC): A scoping review. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2022 Mar:48(3):657-665. doi: 10.1016/j.ejso.2021.10.006. Epub 2021 Oct 20 [PubMed PMID: 34702591]
Level 2 (mid-level) evidenceCortés-Guiral D, Mohamed F, Glehen O, Passot G. Prehabilitation of patients undergoing cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal malignancy. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2021 Jan:47(1):60-64. doi: 10.1016/j.ejso.2020.01.032. Epub 2020 Jan 30 [PubMed PMID: 32063398]
Raspé C, Flöther L, Schneider R, Bucher M, Piso P. Best practice for perioperative management of patients with cytoreductive surgery and HIPEC. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology. 2017 Jun:43(6):1013-1027. doi: 10.1016/j.ejso.2016.09.008. Epub 2016 Sep 28 [PubMed PMID: 27727026]
Maciver AH, Al-Sukhni E, Esquivel J, Skitzki JJ, Kane JM 3rd, Francescutti VA. Current Delivery of Hyperthermic Intraperitoneal Chemotherapy with Cytoreductive Surgery (CS/HIPEC) and Perioperative Practices: An International Survey of High-Volume Surgeons. Annals of surgical oncology. 2017 Apr:24(4):923-930. doi: 10.1245/s10434-016-5692-3. Epub 2016 Nov 29 [PubMed PMID: 27900630]
Level 3 (low-level) evidenceBenson AB, Venook AP, Adam M, Chang G, Chen YJ, Ciombor KK, Cohen SA, Cooper HS, Deming D, Garrido-Laguna I, Grem JL, Haste P, Hecht JR, Hoffe S, Hunt S, Hussan H, Johung KL, Joseph N, Kirilcuk N, Krishnamurthi S, Malla M, Maratt JK, Messersmith WA, Meyerhardt J, Miller ED, Mulcahy MF, Nurkin S, Overman MJ, Parikh A, Patel H, Pedersen K, Saltz L, Schneider C, Shibata D, Shogan B, Skibber JM, Sofocleous CT, Tavakkoli A, Willett CG, Wu C, Gurski LA, Snedeker J, Jones F. Colon Cancer, Version 3.2024, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network : JNCCN. 2024 Jun:22(2 D):. pii: e240029. doi: 10.6004/jnccn.2024.0029. Epub [PubMed PMID: 38862008]
Level 1 (high-level) evidenceGrotz TE, Overman MJ, Eng C, Raghav KP, Royal RE, Mansfield PF, Mann GN, Robinson KA, Beaty KA, Rafeeq S, Matamoros A, Taggart MW, Fournier KF. Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Moderately and Poorly Differentiated Appendiceal Adenocarcinoma: Survival Outcomes and Patient Selection. Annals of surgical oncology. 2017 Sep:24(9):2646-2654. doi: 10.1245/s10434-017-5938-8. Epub 2017 Jul 10 [PubMed PMID: 28695394]
Kusamura S, O'Dwyer ST, Baratti D, Younan R, Deraco M. Technical aspects of cytoreductive surgery. Journal of surgical oncology. 2008 Sep 15:98(4):232-6. doi: 10.1002/jso.21058. Epub [PubMed PMID: 18726883]
Sugarbaker PH. Peritonectomy procedures. Annals of surgery. 1995 Jan:221(1):29-42 [PubMed PMID: 7826158]
Armstrong DK, Alvarez RD, Backes FJ, Bakkum-Gamez JN, Barroilhet L, Behbakht K, Berchuck A, Chen LM, Chitiyo VC, Cristea M, DeRosa M, Eisenhauer EL, Gershenson DM, Gray HJ, Grisham R, Hakam A, Jain A, Karam A, Konecny GE, Leath CA III, Leiserowitz G, Liu J, Martin L, Matei D, McHale M, McLean K, Miller DS, Percac-Lima S, Remmenga SW, Schorge J, Stewart D, Thaker PH, Vargas R, Hendrickson AW, Werner TL, Zsiros E, Dwyer MA, Hang L. NCCN Guidelines® Insights: Ovarian Cancer, Version 3.2022. Journal of the National Comprehensive Cancer Network : JNCCN. 2022 Sep:20(9):972-980. doi: 10.6004/jnccn.2022.0047. Epub [PubMed PMID: 36075393]
Sugarbaker PH. Parietal peritonectomy. Annals of surgical oncology. 2012 Apr:19(4):1250. doi: 10.1245/s10434-012-2229-2. Epub 2012 Feb 10 [PubMed PMID: 22322950]
Diaz E, Fabra I, Vicente E, Quijano Y, Duran H, Malave L, Ruiz P, Costantini G, Nola V, Caruso R, Ferri V. Closed hyperthermic intraperitoneal chemotherapy with CO(2) recirculation system compared with the open Coliseum technique in peritoneal malignity treatment. Surgical oncology. 2023 Feb:46():101901. doi: 10.1016/j.suronc.2023.101901. Epub 2023 Jan 7 [PubMed PMID: 36638761]
Piso P, Nedelcut SD, Rau B, Königsrainer A, Glockzin G, Ströhlein MA, Hörbelt R, Pelz J. Morbidity and Mortality Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy: Data from the DGAV StuDoQ Registry with 2149 Consecutive Patients. Annals of surgical oncology. 2019 Jan:26(1):148-154. doi: 10.1245/s10434-018-6992-6. Epub 2018 Nov 19 [PubMed PMID: 30456672]
Carboni F, Valle M, Vaira M, Sammartino P, Federici O, Robella M, Deraco M, Framarini M, Macrì A, Sassaroli C, Lippolis PV, Di Giorgio A, Biacchi D, Martin-Roman L, Sperduti I, Baratti D. Complications and Mortality Rate of Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy: Italian Peritoneal Surface Malignancies Oncoteam Results Analysis. Cancers. 2022 Nov 25:14(23):. doi: 10.3390/cancers14235824. Epub 2022 Nov 25 [PubMed PMID: 36497306]
Alberto Vilchez ME, Halskov S, Winter A, Pratschke J, Rau B, Gül S. Morbidity and Mortality after Cytoreductive Surgery and HIPEC in a National Reference Center: A Six-Year Experience under Independent Evaluation. Journal of clinical medicine. 2024 Aug 31:13(17):. doi: 10.3390/jcm13175182. Epub 2024 Aug 31 [PubMed PMID: 39274395]
Han Z, Liu X, Tian Y, Shen S, Wang H, Hu S, Wu X, Yan Z, Lu C, Wang P, Bai Y, Kong Y, Wang L, Cao S, Li Z, Zhong H, Meng C, Zhou Y. Long term survival outcomes of surgery combined with hyperthermic intraperitoneal chemotherapy for perforated low-grade appendiceal mucinous neoplasms: A multicenter retrospective study. World journal of surgery. 2024 Jan:48(1):86-96. doi: 10.1002/wjs.12018. Epub 2023 Dec 14 [PubMed PMID: 38686746]
Level 2 (mid-level) evidenceYan TD, Deraco M, Baratti D, Kusamura S, Elias D, Glehen O, Gilly FN, Levine EA, Shen P, Mohamed F, Moran BJ, Morris DL, Chua TC, Piso P, Sugarbaker PH. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: multi-institutional experience. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2009 Dec 20:27(36):6237-42. doi: 10.1200/JCO.2009.23.9640. Epub 2009 Nov 16 [PubMed PMID: 19917862]
Kwakman R, Schrama AM, van Olmen JP, Otten RH, de Lange-de Klerk ES, de Cuba EM, Kazemier G, Te Velde EA. Clinicopathological Parameters in Patient Selection for Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Colorectal Cancer Metastases: A Meta-analysis. Annals of surgery. 2016 Jun:263(6):1102-11. doi: 10.1097/SLA.0000000000001593. Epub [PubMed PMID: 26756756]
Level 1 (high-level) evidence