Introduction
Low back pain (LBP) represents a major global health concern, with a point prevalence of approximately 7% to 8% worldwide and affecting more than 570 million individuals. LBP has remained the leading cause of years lived with disability (YLDs) globally since at least 1990.[1][2] In the United States, total annual costs related to LBP, including direct healthcare expenditures and lost productivity, exceed $100 billion.[1] Chronic LBP ranks among the leading causes of adult disability in the United States, with prevalence increasing with age.[3][1]
Early physicians recognized a potential relationship between lumbar spine pathology and lower-extremity symptoms, but modern understanding of lumbar disc herniation developed in the early 20th century. The landmark publication by Mixter and Barr in 1934 established the foundation for the surgical treatment of lumbar disc herniation.[4] Lindblom first described discography in 1948 as a diagnostic method for evaluating intervertebral disc pathology.[5] Over time, discography evolved from subjective, manual injection techniques to pressure-controlled, automated manometry systems designed to improve diagnostic reproducibility.[6]
Modern imaging, particularly magnetic resonance imaging (MRI), frequently demonstrates multilevel degenerative changes that do not consistently correlate with clinical symptoms. Systematic reviews report a high prevalence of disc degeneration, bulging, and annular changes in asymptomatic individuals, with prevalence increasing with age.[7] Age-related intervertebral disc degeneration involves progressive loss of proteoglycans, decreased water content, altered biomechanics, and structural annular disruption.[8] These observations highlight a key clinical challenge: distinguishing symptomatic pathology from incidental age-related imaging findings.
Provocative discography serves as a diagnostic modality intended to correlate structural disc abnormalities with concordant pain reproduction. Ongoing debate surrounds its role, and clinical use remains generally limited to carefully selected patients undergoing evaluation for surgical or advanced intradiscal interventions. The 2 phenotypes of disc degeneration that have been described are endplate-driven degeneration, which includes endplate defects, inflammatory changes, Modic changes, and Schmorl’s nodes, and annulus-driven degeneration, which involves radial fissures or disc prolapse, as defined by the Modified Dallas Classification System.[9]
A high-intensity zone (HIZ) on MRI may suggest annular pathology; however, imaging findings alone do not establish the presence of symptomatic discogenic pain. Correlation studies demonstrate an association between HIZ and painful discs on provocative discography, but do not establish causation.[10] Pressure-controlled discography with defined pain and pressure thresholds has been proposed to distinguish symptomatic discs from morphologically abnormal but asymptomatic discs.[6] Manometry remains nonuniform in clinical use, and diagnostic criteria vary among practitioners.
Axial spine pain reflects a multifactorial process. Potential contributors include the intervertebral disc, facet joints, medial branch nerves, vertebral endplates, sacroiliac joints, paraspinal musculature, and spinal entheses.[6] In selected cases, provocative discography assists in differentiating discogenic pain from other pain generators. A sham injection component may help identify nonphysiologic responses. Discography functions as a diagnostic rather than therapeutic procedure and should be performed only when results are expected to meaningfully influence management decisions.
Postdiscogram computed tomography (CT) imaging further characterizes annular morphology and informs planning for surgical or intradiscal interventions. The procedure may cause discomfort and carries procedural risks, necessitating careful patient selection, including assessment of cardiovascular comorbidities and renal function due to contrast use. Renewed interest in discography has followed the emergence of regenerative therapies such as platelet-rich plasma and other biologic intradiscal treatments.[11] Certain minimally invasive intradiscal procedures also incorporate discography for procedural planning.
Classification Systems
The original Dallas Classification and the Modified Dallas Classification are 2 systems that are commonly used to describe discographic findings.[12] The original Dallas Classification, developed in the pre-CT era, relies on the following fluoroscopic contrast extravasation patterns to categorize provocative discography findings:
- Grade 0: No extravasation (“cotton ball” appearance of intact nucleus)
- Grade 1: Contrast into the inner annulus
- Grade 2: Contrast into the outer annulus
- Grade 3: Contrast beyond the outer annulus, often into the anterior epidural space
The Modified Dallas Classification incorporates coronal CT imaging and defines graded radial annular disruption from Grade 0, representing a normal disc, to Grade 5, representing a full-thickness radial tear with contrast extravasation beyond the annulus. Advanced annular disruption may contribute to chemical radiculopathy through exposure of neural structures to inflammatory mediators.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The intervertebral disc (IVD) is composed of 3 principal components: the nucleus pulposus centrally, the surrounding annulus fibrosus, and the superior and inferior cartilaginous endplates.[8] The cartilaginous endplate is a thin layer of hyaline cartilage that anchors the disc to the adjacent vertebral bodies and facilitates diffusion-based nutrient transport into the largely avascular disc.[13]
The nucleus pulposus is rich in proteoglycans and type II collagen, which confer water-binding capacity and allow the disc to resist compressive forces. With aging and degeneration, proteoglycan content declines, resulting in decreased hydration, reduced disc height, and altered mechanical properties.[14] Degenerative changes may include annular fissuring, loss of the nucleus–annulus distinction, endplate irregularities, and upregulation of inflammatory mediators.
Innervation of the intervertebral disc is limited in the healthy state. The outer annulus fibrosus is innervated by the sinuvertebral nerve (a recurrent branch of the ventral ramus) as well as contributions from sympathetic fibers via the gray rami communicantes.[15] In normal discs, sensory fibers are largely confined to the outer annular layers and perivascular regions. Neural elements include nociceptive fibers, mechanoreceptors, and sympathetic afferents.
In degenerative states, pathologic neural ingrowth may extend deeper into the inner annulus and, in some cases, into the nucleus pulposus.[15][16] This aberrant innervation is associated with the expression of inflammatory cytokines, including tumor necrosis factor-alpha and interleukin-1 beta, and may contribute to discogenic pain.[17] Increased vascularization and nerve growth factor expression have also been observed in degenerated discs.
The vertebral body itself has relatively sparse innervation, largely perivascular.[18] However, the vertebral endplates may demonstrate increased innervation and inflammatory cell infiltration in degenerative conditions, particularly in association with Modic type 1 changes.[17][19] Endplate-driven degeneration has been associated with the expression of inflammatory mediators and with bone marrow edema visible on MRI.
These anatomic and physiologic features are relevant to discography. Because the healthy nucleus pulposus lacks significant innervation, injection into an intact disc (Modified Dallas Grade 0) should not produce concordant pain. Conversely, advanced annular disruption with nerve ingrowth (grades 3–5) may reproduce concordant axial pain when pressurized. However, pain response is multifactorial and may also be influenced by central sensitization, psychological factors, and adjacent structural pathology.
With progressive degeneration, disc height may decrease, and endplates may become irregular. Loss of disc height, combined with facet hypertrophy, may narrow the foraminal and central canal dimensions, contributing to radicular or axial symptoms. In advanced degeneration with collapse or fusion, disc access for provocative discography may become technically limited or clinically inappropriate. Understanding disc structure, innervation patterns, and degenerative pathways is essential when interpreting discographic findings and correlating them with clinical symptoms.
Indications
Provocative discography is reserved for carefully selected patients with suspected discogenic low back pain when results are expected to meaningfully influence management decisions. Clinical use most often involves patients with chronic axial low back pain persisting for at least 3 months despite appropriate conservative management, including physical therapy, activity modification, pharmacologic therapy, and, when indicated, image-guided spinal injections.[2][6]
A high index of suspicion for primary discogenic pain remains essential before proceeding. Appropriate candidates typically present with severe axial pain with or without limited radicular features, imaging evidence of disc degeneration, and a clinical context in which surgical intervention, eg, spinal fusion, or advanced intradiscal procedures are under consideration. Discography may assist in identifying symptomatic discs among multiple morphologically abnormal levels on MRI, particularly when surgical planning requires level-specific confirmation.[20] Using pressure criteria aligned with Spine Intervention Society-style interpretation, disc desiccation (Pfirrmann ≥3) represents the strongest MRI predictor of a painful disc on provocative discography.[21]
Specific indications for fluoroscopy-guided provocative discography include:
- Evaluation of persistent axial low back pain when imaging findings are equivocal or multilevel degenerative changes are present, and operative intervention is being contemplated.
- Preoperative assessment to identify symptomatic levels before spinal fusion or other surgical stabilization procedures.[20][12]
- Differentiation between painful pseudoarthrosis and adjacent segment disc pathology in patients with prior fusion.
- Evaluation before certain minimally invasive intradiscal interventions (eg, intradiscal electrothermal therapy, biologic intradiscal injections, endoscopic discectomy), when confirmation of symptomatic annular pathology is clinically relevant.[11]
- Selected cases of chronic spine-related pain syndromes with overlapping or atypical presentations, where correlation between imaging findings and concordant pain reproduction may alter management.
Discography is generally not indicated in patients with isolated radicular symptoms attributable to a clearly compressive lesion on MRI, nor when the procedure's outcome would not change clinical management. Current spine and pain management literature emphasizes that discography should be used selectively, primarily for surgical decision-making or planning advanced intradiscal therapy, rather than as a routine diagnostic test.[6][22]
Contraindications
Contraindications to provocative discography include both procedure-specific and general interventional considerations. As with other spinal injection procedures, careful patient selection is essential to minimize risk.
Absolute Contraindications
Procedure-specific factors in which fluoroscopy-guided provocative discography should not be performed include:
- Previously fused intervertebral body at the intended level (disc access is not possible)
- Active spinal cord, cauda equina, or conus medullaris compression at the intended level
- Known or suspected infectious discitis
- Active systemic infection
- Local infection or cellulitis at the skin entry site
- Posterolateral or transverse fusion mass preventing safe disc access
- Inability to obtain informed consent
Discography should not be performed at levels where hardware or fusion precludes safe needle entry. In patients with prior fusion, evaluation may be directed toward adjacent segments if clinically appropriate.
Relative Contraindications
Factors in which fluoroscopy-guided provocative discography may not be recommended include:
- Uncontrolled coagulopathy or ongoing anticoagulation/antiplatelet therapy that cannot be safely managed
- Pregnancy (due to fluoroscopic radiation exposure)
- Severe renal insufficiency (due to contrast use)
- Allergy to iodinated contrast (gadolinium-based contrast has been described as an alternative in select cases)
- Significant medical instability (eg, unstable angina, poorly controlled hypertension, severe arrhythmia risk)
- Untreated or unstable psychiatric conditions
- When the results of the diagnostic procedure would not alter management
Management of anticoagulation and antiplatelet therapy should follow established interventional spine guidelines, including ASRA recommendations, to reduce bleeding risk.[23][24] Clinically significant hemorrhage during discography remains rare; however, needle placement into deep paraspinal structures requires careful periprocedural planning. Updated antithrombotic guidance supports safe performance of spinal needle procedures, particularly for bleeding risk assessment and medication management.[24]
Severe renal dysfunction increases the risk of contrast-induced nephropathy. Baseline renal function assessment should be considered in patients with known kidney disease or significant comorbidities.[25] Ongoing debate surrounds the routine use of antibiotic prophylaxis for discography. Discitis remains an uncommon but potentially serious complication. Current literature does not demonstrate universal consensus regarding prophylactic antibiotic use, and institutional protocols vary.[26]
Patients with poorly controlled anxiety, somatization, or concerns related to secondary gain require careful evaluation. Discography depends on subjective pain reporting, and untreated psychological comorbidity may confound interpretation and increase the likelihood of false-positive results.[27] Discography should be avoided when imaging has already identified a clear surgical lesion that explains the patient’s symptoms or when results would not influence treatment decisions. The procedure requires a clearly defined role within clinical decision-making.
Equipment
Provocative Discogram Equipment
Equipment and supplies that are typically needed when performing fluoroscopy-guided provocative discography procedures include:
- Fluoroscopic C-arm: A mobile or fixed unit with an adequately trained radiology technologist; a biplane unit can improve efficiency, but is not required.
- Radiation protection: Lead aprons for all persons in the room (thyroid shields/lead eyewear as available)
- Needles
- Several 18-gauge, 1- or 1.5-inch needles (introducer/track)
- A 25- or 27-gauge, 1.5-inch (or longer) needle for local anesthesia infiltration (skin and deeper tissue)
- A 22-gauge, 5- or 7-inch needle for disc entry
- Medications and contrast
- Local anesthetic (lidocaine or bupivacaine)
- Injectable antibiotics (commonly cefazolin; alternative per allergy/institutional protocol)
- Myelogram-grade contrast agent (gadolinium may be used in patients with iodine contrast allergy per institutional protocol)
- Pregnancy testing, if applicable
- Sterile supplies
- Sterile gloves and drapes
- Betadine (povidone-iodine) or chlorhexidine gluconate (or equivalent sterile antiseptic solution)
- Sterile gauze
- Tubing: short IV-extension tubing
- If manometry is needed: manometer and attachments (often included in a sterile 1-piece kit, depending on manufacturer)
- If performing difficult L5/S1 entry
- An 18-gauge 5-inch spinal needle and a 22-gauge 7-inch spinal needle
- A 25-gauge 6-inch needle and a 20-gauge 3.5-inch introducer needle
- If performing light intravenous sedation
- Standard monitoring, eg, electrocardiogram (ECG), SpO2, NIBP
- Drugs for sedation eg, short-acting benzodiazepine (midazolam)
- Adequate resuscitative equipment (typically a code cart with reversal agents)
- If obtaining postdiscogram CT
- CT scanner
- Arrangements and transportation to the CT scanner
Personnel
The following team members are involved with discogram procedures:
- Physician performing the discogram
- Radiology technologist to operate the C-arm (and assist with CT if postdiscogram CT is obtained)
- At least 1 circulating medical assistant
- Transporter/escort if the patient requires transfer to CT for postdiscogram imaging
If intravenous sedation is used, additional team members may include:
- A designated, trained observer to monitor and record vital signs: Medication administration and monitoring requirements should follow state regulations and institutional policy (eg, requiring appropriately credentialed nursing and anesthesia personnel, depending on the site of service and the depth of sedation).
- Personnel capable of resuscitation: Additional personnel required to perform and assist with resuscitation efforts should be immediately available as needed (eg, in response to medication reaction, respiratory compromise, or cardiac arrest).
Preparation
The following steps should be followed in preparation for a fluoroscopy-guided provocative discography procedure:
-
Consent and preprocedure counseling: Confirm the indication, explain the diagnostic intent, review key risks (including discitis) and alternatives, and document informed consent.
-
Pregnancy screening: For patients of childbearing age, obtain a documented negative pregnancy test result (or a waiver per institutional policy) before fluoroscopy.
-
Medication and lab review: Review anticoagulant and antiplatelet medications, and obtain labs (eg, PT/INR) when applicable, per institutional policy, for spine interventions.
-
Intravenous (IV) access and baseline monitoring (as indicated): Establish IV access if IV antibiotics or sedation are planned; document baseline vitals and apply standard monitoring appropriate to the planned sedation depth.
-
Sedation plan (if used): If moderate procedural sedation is planned, ensure a dedicated trained observer (not the proceduralist) monitors the patient, with appropriate documentation and equipment, including ventilation monitoring and capnography when feasible and indicated.[28]
-
Preprep imaging and positioning (especially L5/S1): Obtain preliminary fluoroscopic views before sterile prep to anticipate challenges and adjust positioning as needed to optimize trajectory (see Images. L5/S1 Entry, and Iliac Crest Modifications).
-
C-arm clearance check: Before sterile prep, confirm that positioning allows adequate anterior-posterior, lateral, and oblique views without collision or interference from radiopaque table components.
-
Aseptic technique standards for intradiscal procedures: Use meticulous aseptic technique (sterile gloves/drapes, appropriate skin antisepsis, and field discipline) consistent with infection-control guidance for pain procedures.[29]
-
Discitis-risk mitigation (planned before procedure initiated): Prefer styletted needles and a double-needle technique, which has been associated with lower discitis rates compared with nonstyletted single-needle approaches.[30]
-
Antibiotics (if used; evidence-aware): Practices vary; evidence reviews (in the setting of 2-needle technique) have not shown sufficient support for routine prophylactic antibiotics solely to prevent discitis. If antibiotics are used, follow institutional policy and label all syringes.[31]
Technique or Treatment
With preparation complete and the patient positioned prone, perform a standard time-out and confirm the marked lumbar levels. Bilateral disc access may not be feasible in every case; the operator’s standing position typically depends on handedness, room layout, and equipment configuration. When sedation is used, maintain a light level sufficient to preserve reliable pain reporting during provocation.[28]
Prepare the patient with ChloraPrep and apply sterile draping using a fenestrated drape. Place a radiopaque marker over the midlumbar region for reference. Obtain an initial anterior-posterior view, then adjust cephalad or caudad tilt to square the endplates at the target level. Oblique the C-arm toward the entry side until the anterior margin of the superior articular process aligns with the mid-portion of the disc, confirming and adjusting with anterior-posterior, lateral, and oblique views as needed based on disc collapse, rotation, and scoliosis (see Image. Needle Entry Into Disc Space).[20]
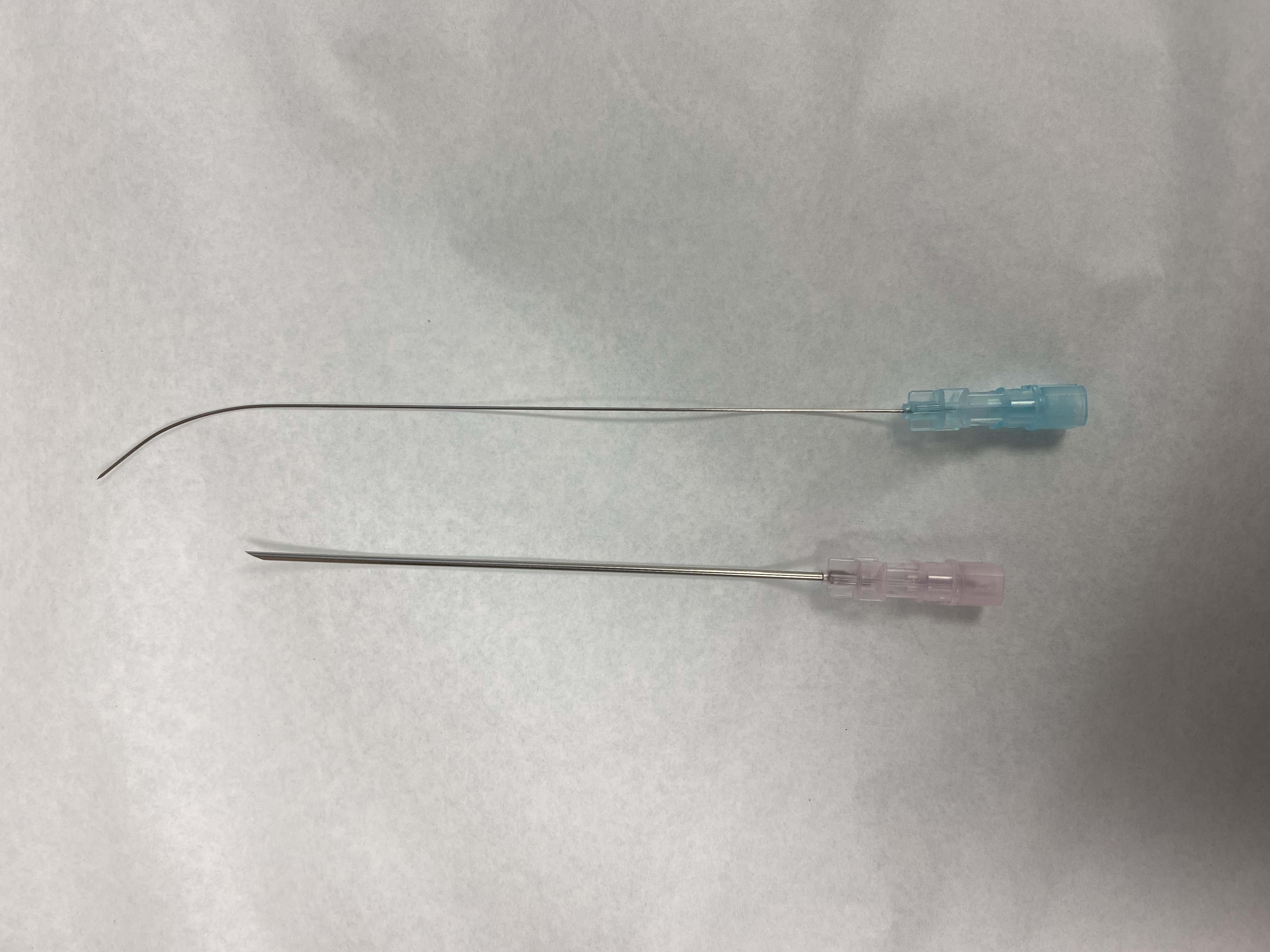
Avoid overly lateral entry points, particularly when vertebral rotation creates a misleading ipsilateral corridor; consider a contralateral approach in such cases. Following local anesthetic infiltration, commonly lidocaine without epinephrine, advance an 18-gauge introducer along the disc trajectory. Pass a 22-gauge disc needle, 5 to 7 inches in length, and either straight or bent-tip as needed, through the introducer using a needle-over-needle double-needle technique (see Images. Needle-Over-Needle Technique and Needle Entry Technique). Advance through the annulus, often perceived as a “rubbery” resistance, and position the needle tip centrally within the nucleus under AP and lateral fluoroscopic guidance.[26]
Rotate to a magnified lateral view to visualize the anterior and posterior disc margins and the spinal canal. After confirming the needle position, remove the stylet without displacing the needle, then connect the primed extension tubing and syringe. Before contrast injection, perform a brief sham maneuver, such as gentle syringe handling or tapping, and document any resulting pain response as a sham response. When using manometry, confirm zero pressure and zero volume at baseline. Inject contrast slowly under real-time fluoroscopy while documenting opening pressure, incremental pressure or volume changes, pain onset, pain location and intensity, and whether the response aligns with or differs from the patient’s typical pain pattern.[32]
During injection and at completion, including saved anterior-posterior and lateral images, document the contrast pattern according to the Dallas discogram description, distinguishing between contained contrast and extension into or through the annulus. Final characterization may be supplemented by postdiscogram CT when obtained.[12]
Complete and document each disc level individually to prevent data overlap. Some clinicians administer a small volume of local anesthetic, approximately 0.5 mL of bupivacaine, into the most symptomatic disc to provide postprocedure palliation. After completing the final series, obtain anterior-posterior and lateral images that encompass all injected levels, cleanse the preparation site, achieve hemostasis, apply a sterile dressing, and discontinue IV access once the patient stabilizes in recovery. When using biplane fluoroscopy or 2 C-arms, follow a similar workflow, integrating anterior-posterior and lateral imaging when oblique visualization remains limited.
Complications
Complications associated with fluoroscopy-guided provocative discography remain relatively uncommon but clinically significant. Reported overall complication rates for lumbar discography range from 0% to 2.7% across published series, with many reviews citing rates below 1% when modern techniques are used.[20][33]
Discitis is the most feared complication, with incidence varying by technique and patient population. Reported rates include 0.25% per patient and 0.094% per disc when a 2-needle technique is used, based on systematic review data. An older series reported rates of 2.7% with a nonstyletted single-needle approach compared with 0.7% using a styletted 2-needle technique. Cervical discography discitis rates have been estimated at 0.15% per injection and 0.44% per patient in meta-analysis data.[31][30][34][29] Evidence-based strategies for infection prevention, adherence to sterile technique, and postprocedure surveillance play a critical role in mitigating complications.[29] Hematoma and postprocedure headache have been reported in a large cervical series, each occurring at a rate of 0.62% (1/161 procedures), with an overall complication rate of 2.48% per procedure (4/161) in that cohort.[35]
Additional reported complications, although less well quantified and often described in isolated cases or small series, include:
-
Meningitis, epidural abscess, and osteomyelitis
-
Nerve root irritation or injury (often transient paresthesia if it occurs)
-
Vascular injury and bleeding
-
Contrast reaction and other medication reactions
-
Cardiovascular and vasovagal-type stress responses related to pain and anxiety
-
Increased pain (commonly transient; persistent flare can occur)
-
Disc herniation and disc rupture (rare)
Long-term concerns include potential disc injury, accelerated degeneration, and associated clinical events. In a 10-year matched cohort study, patients exposed to discography underwent more lumbar surgeries (16 vs 4) and experienced higher rates of imaging utilization, medical visits, work loss, and prolonged pain episodes compared with controls.[36]
Clinical Significance
When performed by a skilled physician, provocative discography is a safe, though often uncomfortable, adjunctive diagnostic procedure that supports the evaluation and workup of axial spine pain, with or without radicular symptoms, in carefully selected patients, particularly when findings may influence surgical decision-making.[37]
Postdiscogram CT provides additional anatomic detail on annular fissures and internal disc disruption after contrast injection and may be valuable when MRI remains contraindicated or nondiagnostic.[38] Discography functions strictly as a diagnostic tool rather than a therapeutic intervention. Optimal interpretation depends on adherence to strict technique and standardized criteria, including the use of control levels, while maintaining awareness of the potential for false-positive pain provocation.[39] In isthmic spondylolisthesis, provocative discography and discoblock demonstrate limited sensitivity compared with mechanical provocation methods, underscoring challenges in accurate pain localization.[40]
Systematic review data demonstrate heterogeneity in definitions of a “positive discogram.” Common criteria include a visual analog scale score of 6 or more and inclusion of an adjacent negative-control disc, yet consistent standardization remains lacking.[41] Quantitative chemical exchange saturation transfer (qCEST) imaging and the qCEST/T2-weighted ratio correlate with painful versus nonpainful discs identified on discography, providing clinically useful discrimination metrics.[42]
Prospective validation of magnetic resonance spectroscopy-derived pain biomarkers against provocative discography supports the development of structured, noninvasive adjunctive or alternative pathways for identifying symptomatic discs.[43] Modeling studies suggest that magnetic resonance spectroscopy–based strategies may reduce costs under favorable outcome assumptions while avoiding adverse-event risks associated with provocative discography.[44] The role of provocative discography remains less clearly defined in predominantly endplate-driven degenerative pain syndromes. Patient counseling should address the potential for long-term disc injury associated with disc puncture and pressurization.[19][36]
Enhancing Healthcare Team Outcomes
Provocative discography serves as a high-stakes diagnostic tool for carefully selected patients with chronic axial spine pain, particularly when results may influence surgical planning or targeted intradiscal therapies. The procedure involves controlled intradiscal pressurization under fluoroscopic guidance, aiming to identify concordant pain sources among multiple morphologically abnormal discs. Accurate interpretation requires standardized technique, precise pain-provocation assessment, and careful differentiation of symptomatic versus incidental degenerative changes. Potential complications, including discitis, hematoma, transient neurologic symptoms, and rare long-term disc injury, necessitate rigorous patient selection, infection-risk mitigation, and peri-procedural monitoring. Postdiscogram CT or advanced imaging may supplement evaluation, especially when MRI is inconclusive. Shared decision-making ensures patients understand procedural limitations, expected discomfort, and potential long-term effects, aligning diagnostic goals with therapeutic planning.[45]
Interprofessional collaboration enhances patient-centered outcomes, safety, and care quality throughout the discography workflow. Primary care clinicians and advanced practitioners optimize comorbidities, ensure prior conservative management, and identify urgent referral needs.[46] Proceduralists maintain technical accuracy and infection prevention, while nursing staff monitors vitals, sedation, and neurologic status. When sedation is used, the team should follow moderate-sedation monitoring standards, including a dedicated trained observer (separate from the proceduralist) and appropriate ventilation monitoring per policy.[28][29] The radiology technologist optimizes image quality while minimizing exposure (ALARA principles), ensures appropriate shielding (lead apron and thyroid protection for staff), and coordinates efficient fluoroscopy workflows, thereby reducing occupational and patient radiation risk and supporting consistent needle localization/interpretation.[47] Pharmacists reconcile anticoagulants and assess medication interactions, and radiology technologists optimize imaging quality while minimizing radiation exposure. Structured communication of findings to referring clinicians and rehabilitation teams ensures timely, coordinated management, reduces fragmented care, and supports evidence-based, systems-oriented decision-making.
Nursing, Allied Health, and Interprofessional Team Interventions
The following interprofessional management strategies are recommended when performing fluoroscopy discography assessment:
-
Standard outpatient support plus sterile technique: Nursing, allied health, and other team members should provide standard-of-care outpatient procedural support, including sterile field maintenance and basic assistance with setup/preparation consistent with other interventional pain procedures.[29]
-
IV access, medication administration, and labeling: Antibiotics and light sedation are commonly administered intravenously per local policy; if an antibiotic is mixed with contrast at the institution, use a standardized preparation process and label all syringes/solutions clearly to prevent medication errors.[48]
-
Emergency preparedness (during and after the procedure): Team interventions should include the capability, training, and written protocols to manage medical emergencies (eg, contrast/drug reactions, vasovagal episodes, oversedation or respiratory compromise), with appropriate monitoring, resuscitation equipment, and reversal agents immediately available per facility policy.[28]
-
Postprocedure monitoring and escalation: Postprocedural nursing care (postprocedure area, PACU, or medical floor) is similar to that for other spine interventions and should include monitoring vital signs, assessing for new focal neurologic deficits, ensuring adequate pain control, and observing for delayed medication reactions and evolving infectious symptoms. Maintain a low threshold for notifying the physician of fever, worsening back pain, severe headache, or new neurologic complaints.[20]
-
Patients with significant cardiac disease or implanted cardiac devices: Some patients undergoing spine pain evaluation have cardiac comorbidities with or without cardiac implantable electronic devices; ensure cardiopulmonary symptoms (chest pain, shortness of breath, or anginal-equivalent symptoms) trigger prompt evaluation and appropriate escalation, and coordinate imaging modality selection when MRI is limited by device status or institutional capability.[49]
Nursing, Allied Health, and Interprofessional Team Monitoring
Nursing or medical assistant post-procedure monitoring should include basic patient observation and serial vital signs, with prompt notification to the physician of any deterioration in the patient's status.[28] Because the patient may have received light sedation (often a benzodiazepine and/or opioid), the team should have established reversal protocols (eg, naloxone and flumazenil per institutional policy) and readily available resuscitation equipment in case of an emergency.[28]
Media
(Click Image to Enlarge)
Needle-Over-Needle Technique. Initial setup for needle-over-needle technique for difficult L5/S1 entry.
Contributed by MF Stretanski, DO
(Click Image to Enlarge)
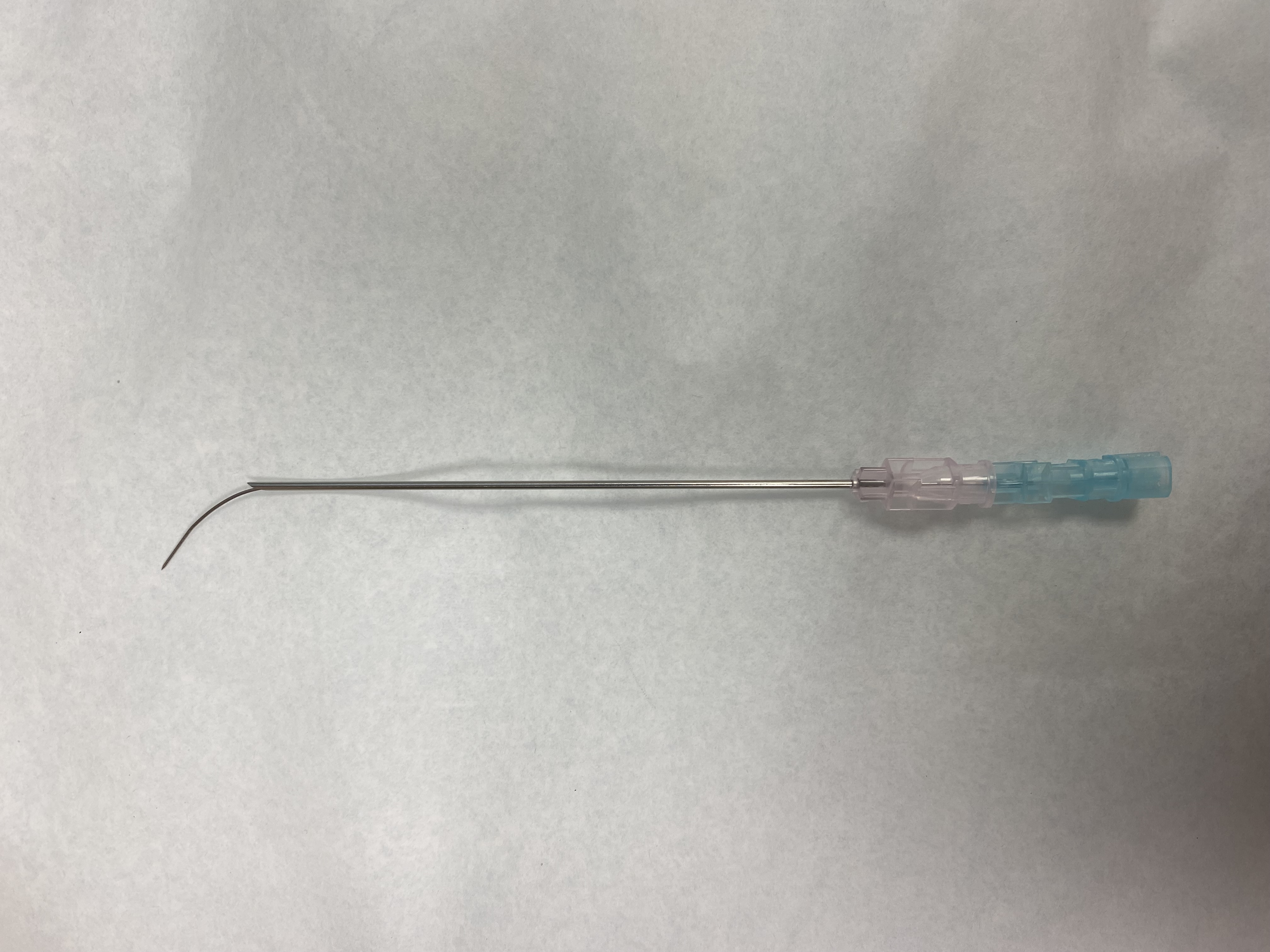
Needle Entry Technique. Image of a 25-gauge needle inserted through an 18-gauge needle, bevel of 18-gauge facing inward, bevel of 25-gauge facing outward, to navigate medially to the center of the disc and avoid getting too far anterior.
Contributed by MF Stretanski, DO
(Click Image to Enlarge)

Needle Entry Into Disc Space. Needle entry into disc spaces above L5/S1, here shown L4/5, is usually more straightforward due to the more self-allowed placement from the iliac crest.
Contributed by MF Stretanski, DO
(Click Image to Enlarge)
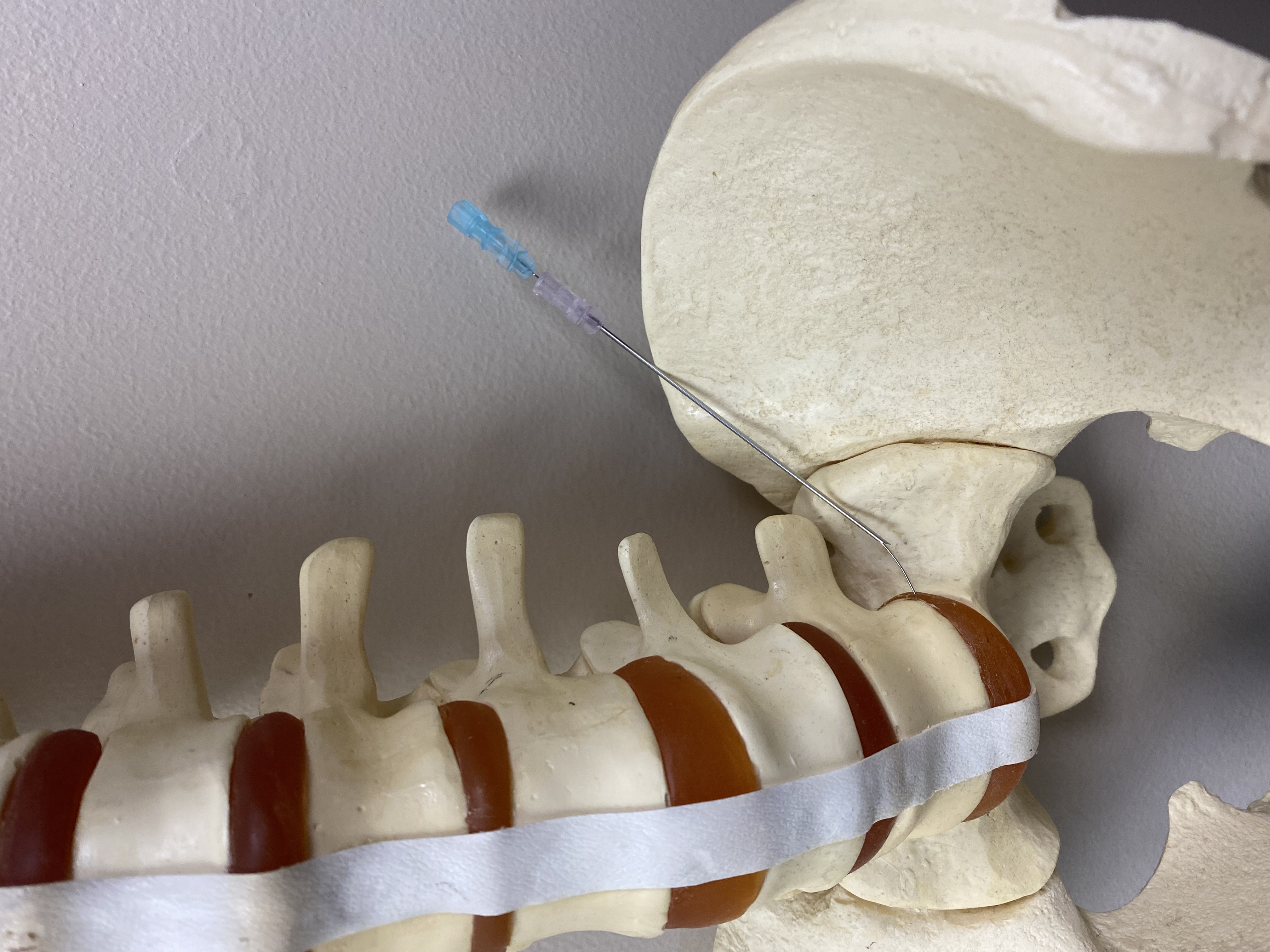
L5/S1 Entry. Anterior view of L5/S1 entry demonstrating how this technique may be required due to the placement of the iliac crest. This is not required as often in females compared to males due to the lower iliac crest and generally wider sacrum.
Contributed by MF Stretanski, DO
(Click Image to Enlarge)
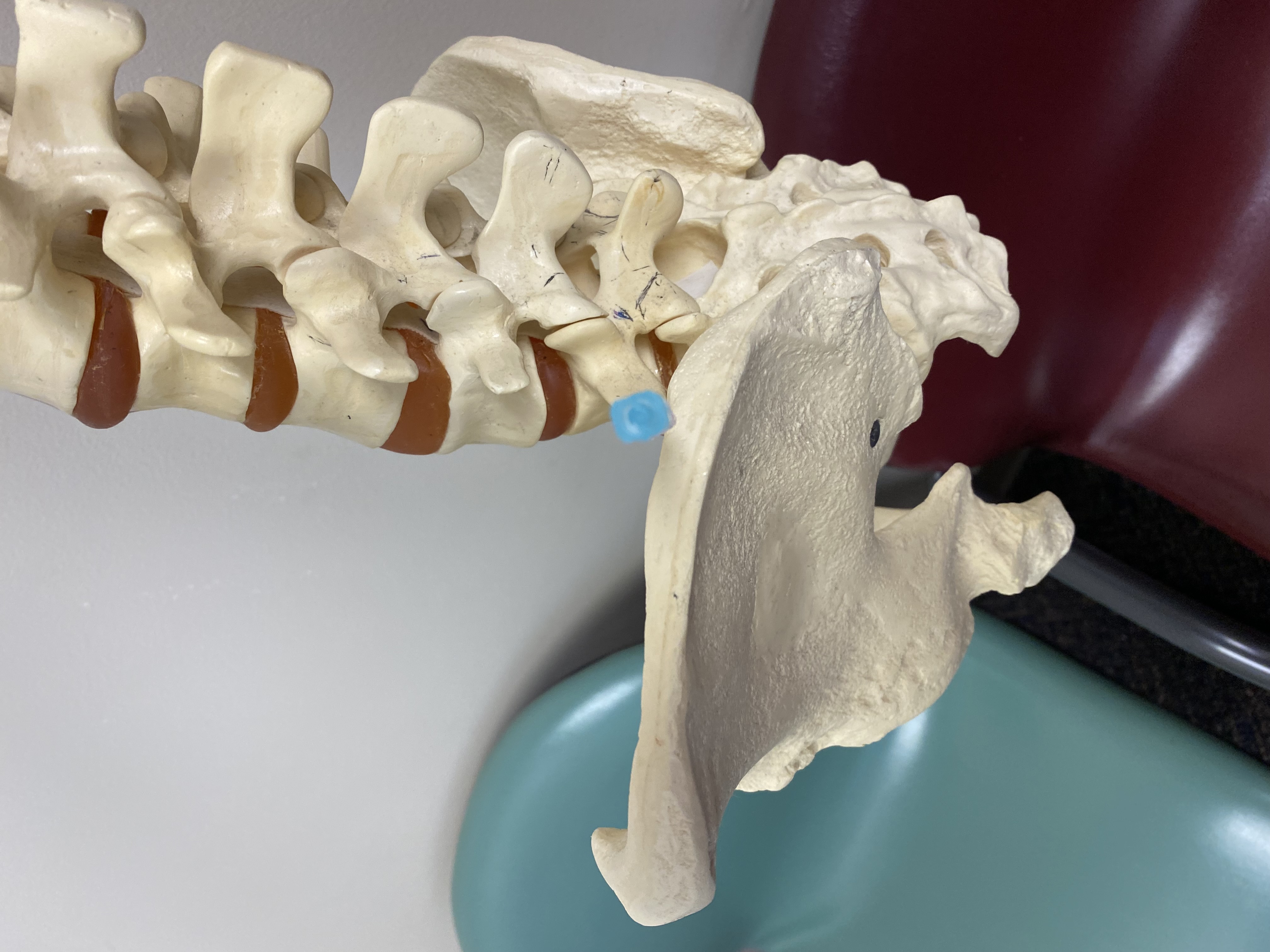
Iliac Crest Modifications. The iliac crest may require the initial entry to be high, above the inferior endplate of the L5 vertebra, and/or too far anterior to enter the center of the disc at L5/S1, and, potentially, in cases of a very high sacrum with loss of the height of the disc spaces and vertebral bodies, even the L4/5 disc space.
Contributed by MF Stretanski, DO
References
Katz JN. Lumbar disc disorders and low-back pain: socioeconomic factors and consequences. The Journal of bone and joint surgery. American volume. 2006 Apr:88 Suppl 2():21-4 [PubMed PMID: 16595438]
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M, Lancet Low Back Pain Series Working Group. What low back pain is and why we need to pay attention. Lancet (London, England). 2018 Jun 9:391(10137):2356-2367. doi: 10.1016/S0140-6736(18)30480-X. Epub 2018 Mar 21 [PubMed PMID: 29573870]
Wu A, March L, Zheng X, Huang J, Wang X, Zhao J, Blyth FM, Smith E, Buchbinder R, Hoy D. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Annals of translational medicine. 2020 Mar:8(6):299. doi: 10.21037/atm.2020.02.175. Epub [PubMed PMID: 32355743]
Truumees E. A history of lumbar disc herniation from Hippocrates to the 1990s. Clinical orthopaedics and related research. 2015 Jun:473(6):1885-95. doi: 10.1007/s11999-014-3633-7. Epub [PubMed PMID: 24752913]
LINDBLOM K. Diagnostic puncture of intervertebral disks in sciatica. Acta orthopaedica Scandinavica. 1948:17(3-4):231-9 [PubMed PMID: 18879767]
Derby R, Kim BJ, Lee SH, Chen Y, Seo KS, Aprill C. Comparison of discographic findings in asymptomatic subject discs and the negative discs of chronic LBP patients: can discography distinguish asymptomatic discs among morphologically abnormal discs? The spine journal : official journal of the North American Spine Society. 2005 Jul-Aug:5(4):389-94 [PubMed PMID: 15996608]
Brinjikji W, Luetmer PH, Comstock B, Bresnahan BW, Chen LE, Deyo RA, Halabi S, Turner JA, Avins AL, James K, Wald JT, Kallmes DF, Jarvik JG. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR. American journal of neuroradiology. 2015 Apr:36(4):811-6. doi: 10.3174/ajnr.A4173. Epub 2014 Nov 27 [PubMed PMID: 25430861]
Level 1 (high-level) evidenceRaj PP. Intervertebral disc: anatomy-physiology-pathophysiology-treatment. Pain practice : the official journal of World Institute of Pain. 2008 Jan-Feb:8(1):18-44. doi: 10.1111/j.1533-2500.2007.00171.x. Epub [PubMed PMID: 18211591]
Stretanski MF, Vu L. Fluoroscopy Discography Assessment, Protocols, and Interpretation. StatPearls. 2026 Jan:(): [PubMed PMID: 34283485]
Wang H, Li Z, Zhang C, Zhang W, Li L, Guo J, Wu W, Hou S. Correlation between high-intensity zone on MRI and discography in patients with low back pain. Medicine. 2017 Jul:96(30):e7222. doi: 10.1097/MD.0000000000007222. Epub [PubMed PMID: 28746177]
Schneider BJ, Hunt C, Conger A, Qu W, Maus TP, Vorobeychik Y, Cheng J, Duszynski B, McCormick ZL. The effectiveness of intradiscal biologic treatments for discogenic low back pain: a systematic review. The spine journal : official journal of the North American Spine Society. 2022 Feb:22(2):226-237. doi: 10.1016/j.spinee.2021.07.015. Epub 2021 Aug 2 [PubMed PMID: 34352363]
Level 1 (high-level) evidenceSachs BL, Vanharanta H, Spivey MA, Guyer RD, Videman T, Rashbaum RF, Johnson RG, Hochschuler SH, Mooney V. Dallas discogram description. A new classification of CT/discography in low-back disorders. Spine. 1987 Apr:12(3):287-94 [PubMed PMID: 2954226]
Moore RJ. The vertebral endplate: disc degeneration, disc regeneration. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2006 Aug:15 Suppl 3(Suppl 3):S333-7 [PubMed PMID: 16816945]
Palepu V, Kodigudla M, Goel VK. Biomechanics of disc degeneration. Advances in orthopedics. 2012:2012():726210. doi: 10.1155/2012/726210. Epub 2012 Jun 17 [PubMed PMID: 22745914]
Level 3 (low-level) evidenceGarcía-Cosamalón J, del Valle ME, Calavia MG, García-Suárez O, López-Muñiz A, Otero J, Vega JA. Intervertebral disc, sensory nerves and neurotrophins: who is who in discogenic pain? Journal of anatomy. 2010 Jul:217(1):1-15. doi: 10.1111/j.1469-7580.2010.01227.x. Epub 2010 Apr 26 [PubMed PMID: 20456524]
Freemont AJ, Peacock TE, Goupille P, Hoyland JA, O'Brien J, Jayson MI. Nerve ingrowth into diseased intervertebral disc in chronic back pain. Lancet (London, England). 1997 Jul 19:350(9072):178-81 [PubMed PMID: 9250186]
Ohtori S, Inoue G, Ito T, Koshi T, Ozawa T, Doya H, Saito T, Moriya H, Takahashi K. Tumor necrosis factor-immunoreactive cells and PGP 9.5-immunoreactive nerve fibers in vertebral endplates of patients with discogenic low back Pain and Modic Type 1 or Type 2 changes on MRI. Spine. 2006 Apr 20:31(9):1026-31 [PubMed PMID: 16641780]
Buonocore M, Aloisi AM, Barbieri M, Gatti AM, Bonezzi C. Vertebral body innervation: Implications for pain. Journal of cellular physiology. 2010 Mar:222(3):488-91. doi: 10.1002/jcp.21996. Epub [PubMed PMID: 20020509]
Viswanathan VK, Shetty AP, Rajasekaran S. Modic changes - An evidence-based, narrative review on its patho-physiology, clinical significance and role in chronic low back pain. Journal of clinical orthopaedics and trauma. 2020 Sep-Oct:11(5):761-769. doi: 10.1016/j.jcot.2020.06.025. Epub 2020 Jun 18 [PubMed PMID: 32879563]
Level 3 (low-level) evidenceWalker J 3rd, El Abd O, Isaac Z, Muzin S. Discography in practice: a clinical and historical review. Current reviews in musculoskeletal medicine. 2008 Jun:1(2):69-83. doi: 10.1007/s12178-007-9009-9. Epub [PubMed PMID: 19468876]
Jain A, Jain S, Barasker SK, Agrawal A. Predictors of discogenic pain in magnetic resonance imaging: a retrospective study of provocative discography performed by posterolateral approach. The Korean journal of pain. 2021 Oct 1:34(4):447-453. doi: 10.3344/kjp.2021.34.4.447. Epub [PubMed PMID: 34593662]
Level 2 (mid-level) evidenceQaseem A, Wilt TJ, McLean RM, Forciea MA, Clinical Guidelines Committee of the American College of Physicians, Denberg TD, Barry MJ, Boyd C, Chow RD, Fitterman N, Harris RP, Humphrey LL, Vijan S. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Annals of internal medicine. 2017 Apr 4:166(7):514-530. doi: 10.7326/M16-2367. Epub 2017 Feb 14 [PubMed PMID: 28192789]
Level 1 (high-level) evidenceNarouze S, Benzon HT, Provenzano D, Buvanendran A, De Andres J, Deer T, Rauck R, Huntoon MA. Interventional Spine and Pain Procedures in Patients on Antiplatelet and Anticoagulant Medications (Second Edition): Guidelines From the American Society of Regional Anesthesia and Pain Medicine, the European Society of Regional Anaesthesia and Pain Therapy, the American Academy of Pain Medicine, the International Neuromodulation Society, the North American Neuromodulation Society, and the World Institute of Pain. Regional anesthesia and pain medicine. 2018 Apr:43(3):225-262. doi: 10.1097/AAP.0000000000000700. Epub [PubMed PMID: 29278603]
Kopp SL, Vandermeulen E, McBane RD, Perlas A, Leffert L, Horlocker T. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (fifth edition). Regional anesthesia and pain medicine. 2025 Oct 17:():. pii: rapm-2024-105766. doi: 10.1136/rapm-2024-105766. Epub 2025 Oct 17 [PubMed PMID: 39880411]
Level 1 (high-level) evidenceDavenport MS, Perazella MA, Yee J, Dillman JR, Fine D, McDonald RJ, Rodby RA, Wang CL, Weinreb JC. Use of Intravenous Iodinated Contrast Media in Patients with Kidney Disease: Consensus Statements from the American College of Radiology and the National Kidney Foundation. Radiology. 2020 Mar:294(3):660-668. doi: 10.1148/radiol.2019192094. Epub 2020 Jan 21 [PubMed PMID: 31961246]
Level 3 (low-level) evidenceSharma SK, Jones JO, Zeballos PP, Irwin SA, Martin TW. The prevention of discitis during discography. The spine journal : official journal of the North American Spine Society. 2009 Nov:9(11):936-43. doi: 10.1016/j.spinee.2009.06.001. Epub 2009 Jul 29 [PubMed PMID: 19643677]
Carragee EJ, Tanner CM, Khurana S, Hayward C, Welsh J, Date E, Truong T, Rossi M, Hagle C. The rates of false-positive lumbar discography in select patients without low back symptoms. Spine. 2000 Jun 1:25(11):1373-80; discussion 1381 [PubMed PMID: 10828919]
. Practice Guidelines for Moderate Procedural Sedation and Analgesia 2018: A Report by the American Society of Anesthesiologists Task Force on Moderate Procedural Sedation and Analgesia, the American Association of Oral and Maxillofacial Surgeons, American College of Radiology, American Dental Association, American Society of Dentist Anesthesiologists, and Society of Interventional Radiology. Anesthesiology. 2018 Mar:128(3):437-479. doi: 10.1097/ALN.0000000000002043. Epub [PubMed PMID: 29334501]
Level 1 (high-level) evidenceProvenzano DA, Hanes M, Hunt C, Benzon HT, Grider JS, Cawcutt K, Doshi TL, Hayek S, Hoelzer B, Johnson RL, Kalagara H, Kopp S, Loftus RW, Macfarlane AJR, Nagpal AS, Neuman SA, Pawa A, Pearson ACS, Pilitsis J, Sivanesan E, Sondekoppam RV, Van Zundert J, Narouze S. ASRA Pain Medicine consensus practice infection control guidelines for regional anesthesia and pain medicine. Regional anesthesia and pain medicine. 2025 Jul 17:():. pii: rapm-2024-105651. doi: 10.1136/rapm-2024-105651. Epub 2025 Jul 17 [PubMed PMID: 39837579]
Level 3 (low-level) evidenceFraser RD, Osti OL, Vernon-Roberts B. Discitis after discography. The Journal of bone and joint surgery. British volume. 1987 Jan:69(1):26-35 [PubMed PMID: 3818728]
Willems PC, Jacobs W, Duinkerke ES, De Kleuver M. Lumbar discography: should we use prophylactic antibiotics? A study of 435 consecutive discograms and a systematic review of the literature. Journal of spinal disorders & techniques. 2004 Jun:17(3):243-7 [PubMed PMID: 15167342]
Level 1 (high-level) evidenceDerby R, Lee SH, Lee JE, Lee SH. Comparison of pressure-controlled provocation discography using automated versus manual syringe pump manometry in patients with chronic low back pain. Pain medicine (Malden, Mass.). 2011 Jan:12(1):18-26. doi: 10.1111/j.1526-4637.2010.00990.x. Epub 2010 Oct 28 [PubMed PMID: 21040439]
Level 2 (mid-level) evidencePeh W. Provocative discography: Current status. Biomedical imaging and intervention journal. 2005 Jul:1(1):e2. doi: 10.2349/biij.1.1.e2. Epub 2005 Jul 1 [PubMed PMID: 21625274]
Kapoor SG, Huff J, Cohen SP. Systematic review of the incidence of discitis after cervical discography. The spine journal : official journal of the North American Spine Society. 2010 Aug:10(8):739-45. doi: 10.1016/j.spinee.2009.12.022. Epub 2010 Feb 19 [PubMed PMID: 20171935]
Level 1 (high-level) evidenceGuyer RD, Ohnmeiss DD, Mason SL, Shelokov AP. Complications of cervical discography: findings in a large series. Journal of spinal disorders. 1997 Apr:10(2):95-101 [PubMed PMID: 9113607]
Cuellar JM, Stauff MP, Herzog RJ, Carrino JA, Baker GA, Carragee EJ. Does provocative discography cause clinically important injury to the lumbar intervertebral disc? A 10-year matched cohort study. The spine journal : official journal of the North American Spine Society. 2016 Mar:16(3):273-80. doi: 10.1016/j.spinee.2015.06.051. Epub 2015 Jun 29 [PubMed PMID: 26133255]
Eck JC, Sharan A, Resnick DK, Watters WC 3rd, Ghogawala Z, Dailey AT, Mummaneni PV, Groff MW, Wang JC, Choudhri TF, Dhall SS, Kaiser MG. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 6: discography for patient selection. Journal of neurosurgery. Spine. 2014 Jul:21(1):37-41. doi: 10.3171/2014.4.SPINE14269. Epub [PubMed PMID: 24980583]
Loneragan R, Khangure MS, McCormick C, Hardcastle P. Comparison of magnetic resonance imaging and computed tomographic discography in the assessment of lumbar disc degeneration. Australasian radiology. 1994 Feb:38(1):6-9 [PubMed PMID: 8147805]
Wolfer LR, Derby R, Lee JE, Lee SH. Systematic review of lumbar provocation discography in asymptomatic subjects with a meta-analysis of false-positive rates. Pain physician. 2008 Jul-Aug:11(4):513-38 [PubMed PMID: 18690280]
Level 1 (high-level) evidenceNyström B, Schillberg B, Jin S, Taube A. Usefulness of discography, discoblock and a new mechanical method for identifying a painful segment/disc. Neuro-Chirurgie. 2023 Jan:69(1):101397. doi: 10.1016/j.neuchi.2022.101397. Epub 2022 Dec 9 [PubMed PMID: 36502874]
Méndez-Gutiérrez A, Marín Navas F, Acevedo-González JC. [Translated article] Frequency of use of discography findings for the diagnosis of low back pain of discogenic origin. Systematic review of the literature. Revista espanola de cirugia ortopedica y traumatologia. 2024 May-Jun:68(3):T209-T222. doi: 10.1016/j.recot.2024.03.008. Epub 2024 Mar 18 [PubMed PMID: 38508378]
Level 1 (high-level) evidencePelled G, Salas MM, Han P, Gill HE 3rd, Lautenschlager KA, Lai TT, Shawver CM, Hoch MB, Goff BJ, Betts AM, Zhou Z, Lynch C, Schroeder G, Bez M, Maya MM, Bresee C, Gazit Z, McCallin JP 3rd, Gazit D, Li D. Intradiscal quantitative chemical exchange saturation transfer MRI signal correlates with discogenic pain in human patients. Scientific reports. 2021 Sep 28:11(1):19195. doi: 10.1038/s41598-021-97672-y. Epub 2021 Sep 28 [PubMed PMID: 34584114]
Gornet MG, Peacock J, Ryken T, Schranck FW, Eastlack RK, Lotz JC. Establishing a Gold Standard for Noninvasive Identification of Painful Lumbar Discs: Prospective Comparison of Magnetic Resonance Spectroscopy vs Low-Pressure Provocation Discography. International journal of spine surgery. 2024 Feb 27:18(1):91-100. doi: 10.14444/8574. Epub 2024 Feb 27 [PubMed PMID: 38413238]
Wilson L, Beall DP, Eastlack RK, Berven S, Lotz JC. The Comparison of Cost-Effectiveness Between Magnetic Resonance Spectroscopy and Provocative Discography in the Identification of Chronic Low Back Pain Surgery Candidates. ClinicoEconomics and outcomes research : CEOR. 2025:17():19-31. doi: 10.2147/CEOR.S501058. Epub 2025 Jan 23 [PubMed PMID: 39872472]
Margetic P, Pavic R, Stancic MF. Provocative discography screening improves surgical outcome. Wiener klinische Wochenschrift. 2013 Oct:125(19-20):600-10. doi: 10.1007/s00508-013-0404-5. Epub 2013 Aug 30 [PubMed PMID: 23989460]
Hooten WM, Cohen SP. Evaluation and Treatment of Low Back Pain: A Clinically Focused Review for Primary Care Specialists. Mayo Clinic proceedings. 2015 Dec:90(12):1699-718. doi: 10.1016/j.mayocp.2015.10.009. Epub [PubMed PMID: 26653300]
Cheon BK, Kim CL, Kim KR, Kang MH, Lim JA, Woo NS, Rhee KY, Kim HK, Kim JH. Radiation safety: a focus on lead aprons and thyroid shields in interventional pain management. The Korean journal of pain. 2018 Oct:31(4):244-252. doi: 10.3344/kjp.2018.31.4.244. Epub 2018 Oct 1 [PubMed PMID: 30310549]
Klessig HT, Showsh SA, Sekorski A. The use of intradiscal antibiotics for discography: an in vitro study of gentamicin, cefazolin, and clindamycin. Spine. 2003 Aug 1:28(15):1735-8 [PubMed PMID: 12897501]
Kim D, Collins JD, White JA, Hanneman K, Lee DC, Patel AR, Hu P, Litt H, Weinsaft JW, Davids R, Mukai K, Ng MY, Luetkens JA, Roguin A, Rochitte CE, Woodard PK, Manisty C, Zareba KM, Mont L, Bogun F, Ennis DB, Nazarian S, Webster G, Stojanovska J. SCMR expert consensus statement for cardiovascular magnetic resonance of patients with a cardiac implantable electronic device. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2024 Summer:26(1):100995. doi: 10.1016/j.jocmr.2024.100995. Epub 2024 Jan 12 [PubMed PMID: 38219955]
Level 3 (low-level) evidence