Introduction
Encapsulating peritoneal sclerosis (EPS) is a clinical syndrome characterized by a thickened, fibrocollagenous peritoneal membrane that encases parts of the small intestine, leading to recurrent small bowel obstructions and malnutrition. Patient will present with nonspecific symptoms such as nausea, vomiting, abdominal pain, weight loss, diarrhea, or constipation. This fibrinous structure can complicate into ischemia, infection, and even cause death.
This rare disorder is most strongly associated with long-term peritoneal dialysis, as dialysis can cause chronic inflammation and subsequent sclerosis.[1] Multiple episodes of severe peritoneal infections or systemic inflammatory disorders can predispose a patient to EPS. This condition is also a potential late-onset complication of kidney transplantation in the absence of systemic inflammation.[2] Despite this, many cases of EPS remain idiopathic. Due to the rarity of this debilitating condition, diagnosis is often delayed.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of encapsulating peritoneal sclerosis is not well studied. However, EPS is most commonly seen in patients on long-term peritoneal dialysis diagnosed with end-stage renal disease. During peritoneal dialysis, the dialysate typically contains glucose or glucose degradation products, which can induce inflammation in the peritoneum. This inflammation can increase endothelial permeability and fibrinogenesis, causing further damage to the peritoneum and leading to fibrin deposition.
Multiple fibrin depositions can form a dense fibrocollagenous capsule around parts of the small bowel. Peritoneal inflammation will continue to accumulate, leading to adhesion formation and worsening fibrosis. This can cause not only acute bowel obstruction but also malnutrition (see Image. Encapsulating Peritoneal Sclerosis). Risk factors in patients on peritoneal dialysis (PD) include duration of PD, cessation of PD, renal transplantation, peritonitis, young age, low pH, high glucose within dialysate, ultrafiltration failure, and exposure to chlorhexidine.[3]
Also, there are causes of EPS that are not directly related to peritoneal dialysis. Associations include autoimmune diseases, sarcoidosis, peritoneal and intra-abdominal malignancies, chronic peritoneal ascites, intraperitoneal chemotherapy, specific dialysate fluids such as acetate or bioincompatible dialysate, abdominal surgery, endometriosis, intraperitoneal infections (particularly Staphylococcus aureus, Pseudomonas, and Mycobacterium tuberculosis, as well as fungal species), calcineurin inhibitors, and beta-blocker administration. Proinflammatory states can predispose patients to EPS. Renal transplantation shows an increased risk of developing encapsulating peritoneal sclerosis, most commonly seen shortly after transplantation. There is a theory that this could be due to the profibrotic effects and immunosuppressive medication, such as calcineurin inhibitors, which may also be a result of the acute cessation of peritoneal dialysis.[3]
Epidemiology
The epidemiology of encapsulating peritoneal sclerosis has been studied in Scotland, Australia, New Zealand, and Japan. In contrast, there is very little data reporting the incidence of EPS in the United States. Most research available in the US has been conducted at single-center institutions. In a single center in New Haven, Connecticut, a retrospective observational cohort analysis of patients on peritoneal dialysis for 5 years or longer revealed an incidence of EPS of 18.4%. In this study, only 76 patients met the inclusion criteria, with 11 patients meeting the International Society for Peritoneal Dialysis criteria for the diagnosis of EPS.[4]
At another US single-center institution, a retrospective study examined a 30-year-old peritoneal dialysis registry for the incidence of EPS. In this study, 676 patients met the inclusion criteria, and the incidence of EPS was 1.2%. The study also found that the incidence of EPS rose to 15% after 6 years and 38% after 9 years of peritoneal dialysis.[5]
Both US studies reveal not only how understudied EPS is, but the incidence of EPS increases for patients on peritoneal dialysis for at least 5 years or more. This finding is consistent with research in other countries, such as Scotland. Adult patients (n = 1238) who initiated peritoneal dialysis between 2000 and 2007 were identified by the Scottish Renal Registry. The incidence of EPS was 1.1% after 1 year, 3.4% after 3 years, 8.8% after 4 years, 9.4% after 5 years, and 22.2% after 7 years of staying on peritoneal dialysis.[6]
In a study involving 13 years of data from 7618 patients in Australia and New Zealand, the incidence rate was 1.8 per 1000 patients. Respective cumulative incidences of EPS were 0.3% at 3 years, 0.8% at 5 years, and 3.9% at 8 years of dialysis. Results from a Japanese study revealed the incidence (and mortality rates) for EPS were 0% (0%) at 3 years, 0.7% (0%) at 5 years, 2.1% (8.3%) at 8 years, 5.9% (28.6%) at 10 years, 5.8% (61.5%) at 15 years, and 17.2% (100%) with 15 years or greater of peritoneal dialysis.[7] Studies from other countries reveal that the prevalence of EPS varies between 0.4% and 8.9%, but can reach as high as 22.2% after 7 years or more of peritoneal dialysis, as highlighted by the Scottish study.[8]
Pathophysiology
The pathophysiology of encapsulating peritoneal sclerosis is multifactorial and not fully understood. Long-term peritoneal dialysis is a significant risk factor, and patients who require treatment will experience adverse cellular changes to the peritoneal membrane due to exposure to bioincompatible peritoneal dialysis fluids. Approximately 50% to 80% of all patients on peritoneal dialysis will experience progressive sclerosis of the peritoneal membrane within 1 to 2 years of initiating treatment. The chemical composition of the solutions used in peritoneal dialysis causes oxidative stress, which damages the peritoneal membrane. The acidic pH, elevated osmolarity, and increased glucose concentration contribute to fibrosis, vasculopathy, and a decline in peritoneal ultrafiltration.[9]
Peritoneal dialysis solutions undergo heat sterilization processes, which eventually form glucose degradation products. Glucose degradation products and the increased glucose concentration are then exposed to the peritoneal membrane when the fluid is used in dialysis. Glucose degradation products then undergo another chemical reaction, forming irreversible reactive molecules known as advanced glycation end products. The advanced glycation end products slowly accumulate in the peritoneal membrane after multiple rounds of dialysis, which can cause peritoneal cell injury via several mechanisms. Advanced glycation end products can induce morphological changes in intracellular proteins and alter the existing structure of extracellular matrix components and receptors within peritoneal cells.
Lastly, advanced glycation end products can modify proteins, tightly binding to specific multi-ligand transmembrane receptors on endothelial cells and macrophages. This adverse binding can activate free radicals, pro-inflammatory cytokines, and growth factors, such as vascular endothelial growth factors, which can lead to abnormal transcription of DNA and subsequent apoptosis. This binding can further enhance the production of advanced glycation end products, potentially leading to additional damage.[10]
The increased glucose-oxidation metabolism is also how glycation end products and advanced glycation end products trigger the creation of reactive oxidative species. When the fluid, high in glucose concentration, enters the peritoneal cells, it increases glucose catabolism, leading to an overproduction of electron donors to compensate for the increased glucose uptake. Overproduction can eventually overwhelm the cell's capacity to neutralize reactive oxidative species, leading to a higher formation of these species. These reactive oxidative species lead to an increase in fibrinogenesis and endothelial permeability. Even peritoneal fluids that have a significant reduction in glucose degradation products and glucose, with a neutral pH, can exhibit the slow, progressive development of reactive oxidative species, which subsequently form fibrosis that later becomes sclerotic.[11]
Peritonitis can also be a major risk factor for EPS, particularly Staphylococcus aureus, Pseudomonas, Mycobacterium tuberculosis, and fungal infections. Inflammation that occurs in the setting of peritonitis can accelerate the peritoneal transformation process, leading to the formation of fibrosis. One study found that peritoneal inflammation was common after dialysis catheter removal for refractory bacterial peritonitis, and these patients had a 31% likelihood of developing EPS with a mortality rate of 36%.[12]
Histopathology
Podoplanin is a type-1 transmembrane sialomucin-like glycoprotein present on the endothelium of lymphatic vessels in both submesothelial fibrotic and mesothelial cells. Podoplanin can modulate inflammatory reactions by binding to chemokines and plays a potential role in the inflammatory process. Results from a study revealed that patients with EPS exhibited a diffuse infiltration of podoplanin-positive cells, which may serve as a suitable histopathological marker for EPS.[13]
History and Physical
The diagnosis of encapsulating peritoneal sclerosis can be made based on a constellation of symptoms and their timing. EPS typically develops in a step-wise fashion with an inflammatory, encapsulating, and ileus stage. EPS can begin with an inflammatory stage, during which patients may present with symptoms such as fever, anemia, hypoalbuminemia, nausea, diarrhea, and an elevation in C-reactive protein. This is associated with the genesis of bowel encapsulation. The physical exam can often be unremarkable during the encapsulating phase, as the fibrotic capsule can also be too premature to inhibit intestinal peristalsis. Over time, the fibrotic capsule becomes sclerotic and causes bowel obstruction-like symptoms, which leads to the ileus stage. Early symptoms in the ileus stage are nausea, vomiting, diarrhea, intermittent abdominal pain, anorexia, and loss of appetite.
The physical exam can also be unremarkable; however, some patients on peritoneal dialysis have reported blood-tinged ascites or dialysis fluid during the procedure, especially after periods when the peritoneal dialysis cavity has been dry. Ineffective ultrafiltration and transition from low to a high transporter status may also be a sign of EPS.[14][15] Late symptoms in the ileus stage can progress to severe abdominal pain, intractable vomiting, malnutrition, constipation, and weight loss. At this stage of symptom progression, the physical examination may reveal an abdominal mass with tenderness upon light and deep palpation, hypoactive bowel sounds, and potentially abdominal rigidity. The timing of symptoms is also important, as most patients (70% to 90%) will be diagnosed with EPS after terminating peritoneal dialysis, which can develop as late as 5 years later.[16]
Evaluation
Currently, there are no laboratory tests for encapsulating peritoneal sclerosis; therefore, radiographic imaging is recommended to confirm the diagnosis. Computed tomography (CT) is the definitive imaging modality of choice for EPS, with one study affirming 100% sensitivity and 94% specificity for diagnosing EPS. CT imaging would reveal peritoneal enhancement, thickening, and calcifications; bowel tethering, thickening, and dilatation; and fluid septation/loculation (see Image. Abdomen/Pelvis Encapsulating Peritoneal Sclerosis, Computed Tomography).[17] However, the results of other studies suggest that early EPS may not exhibit changes beyond ascites, and a high clinical suspicion is necessary.[14][15]
EPS can be diagnosed with clinical signs of intestinal obstruction, with radiological imaging of bowel encapsulation. However, it is essential to note that other imaging modalities, such as abdominal radiography, can be used to diagnose EPS. This is because abdominal radiography lacks the same level of sensitivity and specificity. Still, air-fluid levels, signs of bowel dilation, and peritoneal calcifications can be used to suspect EPS in the setting of intestinal obstruction.
Notably, x-ray films can have a normal presentation despite having EPS. The most sensitive and specific method to confirm EPS can be achieved through a laparoscopy or laparotomy procedure, which allows for visualization of the peritoneal thickening that encloses the bowel. But due to the invasive nature and the elevated risks of surgery, this is rarely done to diagnose EPS.[18]
Treatment / Management
Initial treatment of EPS begins with considering the cessation of peritoneal dialysis to halt further derangements to the peritoneal membrane. Not every patient can benefit from stopping peritoneal dialysis; therefore, this decision must carefully weigh the benefits and risks, as hemodialysis is typically the next step for most patients. Hemodialysis carries a different set of complications and risks when compared to peritoneal dialysis, in addition to lifestyle changes. Notably, because many cases of EPS are diagnosed years after stopping peritoneal dialysis, there is the potential for symptoms to worsen even after discontinuing.[3]
Regardless, if the decision to cease peritoneal dialysis is made, the standard of care would be to switch from peritoneal dialysis to hemodialysis and remove the peritoneal dialysis catheter. To decrease the risk of abdominal adhesions, the peritoneum should be flushed twice a week with 100 to 200 mL of 1.36% dialysate with 3500 international units of heparin. Bowel rest should be maintained for 4 to 12 weeks, depending on the severity of the symptoms present.[19]
Medical management of EPS includes the use of corticosteroids or tamoxifen. Steroids act by decreasing inflammation and the development of fibrin deposition. In treating the early stages of EPS, steroids have been proven to be an effective medication. Still, the effect tends to decrease in the later stages when fibrosis is significant, and bowel obstruction occurs. For these earlier stages, prednisolone dosing is 0.5 to 1.0 mg/kg/day or a pulse dose of 500 to 1000 mg of methylprednisolone for 2 to 3 days.[20]
Treatment should be continued for at least 1 year with a steroid taper. If using prednisolone, the taper should be 0.5 to 1.0 mg/kg daily for the first month, 0.25 to 0.5 mg at 2 to 3 months, and then 10 mg at 6 months. C-reactive protein should be monitored, and a dramatic rise should raise the suspicion of inflammation due to bacterial peritonitis or intestinal obstruction. Tamoxifen can be an alternative treatment and may be considered the first choice, considering the well-documented adverse effects of steroids. Despite this, tamoxifen is typically given in combination with steroids. Tamoxifen is administered in doses of 10 to 40 mg/day for at least 2 to 6 months.[21]
Surgical interventions become the treatment choice when patients are at risk of obstruction due to fibrotic adhesions.[22] A peritonectomy involves the lysis of adhesions and total ablation of sclerotic tissue in the abdomen. Surgery should only be considered in chronic individuals who fail medical and conservative management and in patients with acute symptoms of bowel obstruction. The risks of surgery include perforation of the intestines, sepsis, bleeding, fistula formation, and death. There is also a risk of recurrence of adhesions and symptoms. Despite this, suturing the intestine to itself to prevent recurrence has been proposed, and considering medical management with steroids or tamoxifen might decrease the risk.[23](A1)
Nutrition and hydration should be optimized in patients with EPS. Patients who elect to treat with surgery are at high risk of refeeding syndrome, so aggressive nutritional support should be a vital aspect of the management plan for these patients in the pre- and postoperative period. In research conducted in the United Kingdom, patients who underwent surgery reportedly experienced improved surgical outcomes when total parenteral nutrition was used in preoperative management. Importantly, total parenteral nutrition is not the mainstay treatment for all patients, as chronic EPS patients can benefit from close monitoring and increased oral intake.[24]
Differential Diagnosis
One important disease that can be mistaken for encapsulating peritoneal sclerosis is peritoneal encapsulation. This is also a rare disease in which a thin accessory peritoneal membrane can surround various parts of the small bowel. Peritoneal encapsulation forms an accessory peritoneal sac, which is typically asymptomatic and incidentally diagnosed; however, it can also cause symptoms of small bowel obstruction. This peritoneal sac differs from EPS, as peritoneal encapsulation is a congenital malformation, not one that develops from chronic inflammation.[25] Because many symptoms of EPS can be nonspecific gastrointestinal complaints, the differential diagnosis can be extensive, including small bowel obstruction, gastroparesis, irritable bowel syndrome, pancreatic adenocarcinoma, peptic ulcer disease, pancreatitis, Crohn disease, retroperitoneal fibrosis, tumors, malignancy, hernias, and peritonitis.[26]
Prognosis
Results from a Taiwanese study reviewed data from 3 Taiwanese medical centers and categorized patients into mild/moderate or severe encapsulating peritoneal sclerosis. Severe EPS included signs and symptoms of intractable obstruction, gut ischemia, sepsis, and those that needed surgical intervention. They found that the overall mortality rate of EPS was 35% and 74% in patients in the severe EPS group.[27] Results from a single-center Japanese retrospective observational study spanning nearly 15 years demonstrated Kaplan–Meier estimated survival rates at 1, 2, 3, 5, and 8 years after EPS diagnosis at 91%, 83%, 77%, 66%, and 53%, respectively.[28] Encapsulating peritoneal sclerosis carries high morbidity and a mortality rate that can approach as high as 50% within 12 months of diagnosis.[14][15]
Complications
The risk of developing complications from EPS is strongly and positively correlated with the duration of peritoneal dialysis treatment. Complications can arise from medical treatment and surgical intervention. Untreated EPS is associated with high morbidity and mortality, primarily secondary to recurrent bowel obstructions resulting in intestinal failure, malnutrition, and sepsis.[29] Worsening complications include bowel ischemia, perforation, and death. Tamoxifen has been associated with a higher risk of endometrial adenocarcinoma, uterine sarcoma, pulmonary embolism, and stroke in female patients.[30]
Prednisone has been reported to have adverse effects of tertiary adrenal insufficiency, hypertension, sodium retention, decreased serum potassium, fluid retention, psychiatric disturbances, cushingoid features, and hyperglycemia. From a surgical perspective, complications include excessive bleeding, inadvertent bowel injury, abscess formation, surgical site infection, perforation of intestinal contents, deep vein thrombosis, atelectasis, and sepsis.[31] Many of these complications occur in the postoperative period. Thus, prophylactic management should include deep vein thrombosis prophylaxis, preoperative antibiotics, insertion/removal of Foley catheters, incentive spirometry, and slowly escalating the diet as tolerated.[32]
Deterrence and Patient Education
Patient education is imperative in improving a patient's health literacy. By helping patients understand their condition, the risks/benefits of treatment, and potential complications, they can make more informed decisions regarding their care. In addition, clinicians and the healthcare team can implement the teach-back method by avoiding medical jargon, actively engaging with patient questions, and explaining the diagnosis to achieve this goal. Thus, it is prudent to inform any patient considering peritoneal dialysis of the benefits/risks, especially concerning an increased risk of encapsulating peritoneal dialysis.
By effectively educating patients on this complication from dialysis, they will be more aware of the signs and symptoms to look out for, allowing them to catch EPS earlier. Patient education could decrease the risk of delayed diagnosis and ensure proper treatment. This method applies not only to the disease in question but also to management options. There are numerous risks/benefits to using steroids, tamoxifen, and surgical intervention. A better understanding of these interventions can lead to a more informed decision.[33]
Enhancing Healthcare Team Outcomes
Encapsulating peritoneal sclerosis requires a multifaceted approach regarding proper diagnosis, treatment, and follow-up care. Adequate communication and trust are pivotal because various healthcare professionals, including clinicians, surgeons, mid-level clinicians, nurses, pharmacists, and technicians, are involved in patient education and care. As highlighted above, the healthcare team can implement the teach-back method, avoid using medical jargon, actively engage with patients' questions, and clearly explain the diagnosis. This can help patients make more informed decisions regarding their care. Effective communication ensures that the healthcare team provides patients with the highest quality of care efficiently and effectively. Recognizing the complex interplays of various healthcare providers in the treatment of encapsulating peritoneal sclerosis is essential.
First, individuals with EPS are typically on peritoneal dialysis, typically under the care of a nephrologist managed by a dialysis-trained healthcare team. This team can consist of mid-level clinicians, nurses, medical assistants, and dialysis-trained technicians who actively manage patients' dialysis needs. In addition, should a patient become hospitalized for symptoms related to suspected EPS, consider the radiologist who reads the CT scan, the pharmacist who manages the tamoxifen or steroids, the primary care team that coordinates care with surgery, the surgeon who proceeds with lysis of adhesions, and the numerous other healthcare providers. This dynamic interplay necessitates the vital role of effective communication in ensuring optimal care, as one healthcare professional's actions can significantly impact another's interpretation and management plans.[34]
Regarding the decision to proceed with emergent surgical intervention, highlighting a patient's objective deterioration, understanding a patient's wishes, and involving the patient's family in the decision can help enhance care. In addition, trust is pivotal in this example and in all other healthcare interactions highlighted above. By trusting what another clinician writes regarding a patient's history and correlating it with the pertinent laboratory/imaging/physical exam findings made possible by the healthcare team, the team becomes more efficient. And by working efficiently and effectively on behalf of a patient, trust can develop. A meta-analysis of 4 databases on the relationship between trust in healthcare professionals and health outcomes revealed that patients reported more beneficial health behaviors, fewer symptoms, a higher quality of life, and greater satisfaction with treatment when they had higher trust in their healthcare professionals.[35]
Media
(Click Image to Enlarge)
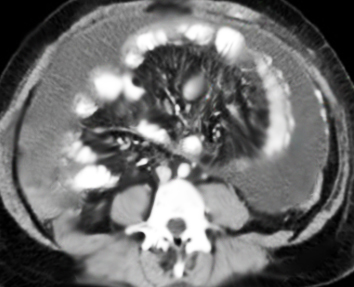
Abdomen/Pelvis Encapsulating Peritoneal Sclerosis, Computed Tomography. Imaging reveals peritoneal enhancement, thickening and calcifications, bowel tethering and thickening, dilatation, and fluid septation/loculation.
Contributed by R Kabir, MD
(Click Image to Enlarge)
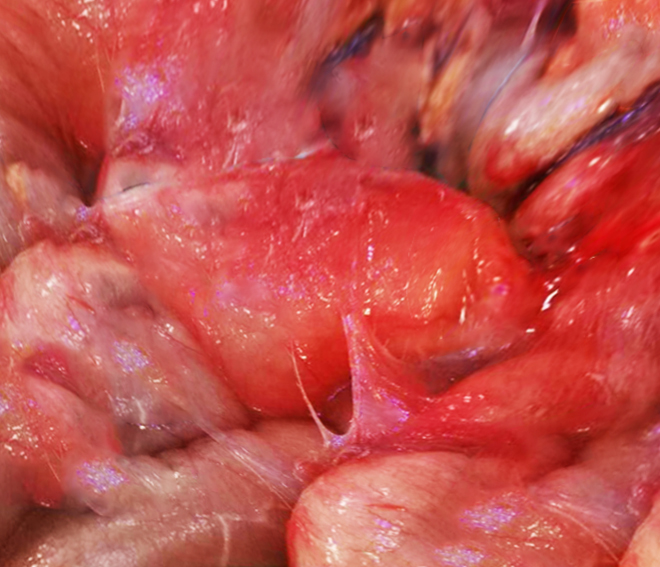
Encapsulating Peritoneal Sclerosis. Multiple fibrin depositions can form a dense fibrocollagenous capsule around parts of the small bowel; peritoneal inflammation will continue to accumulate, leading to adhesion formation and worsening fibrosis.
Contributed by R Kabir, MD
References
Danford CJ, Lin SC, Smith MP, Wolf JL. Encapsulating peritoneal sclerosis. World journal of gastroenterology. 2018 Jul 28:24(28):3101-3111. doi: 10.3748/wjg.v24.i28.3101. Epub [PubMed PMID: 30065556]
Habib SM, Dor FJ, Korte MR, Hagen SM, Betjes MG. Post-transplantation encapsulating peritoneal sclerosis without inflammation or radiological abnormalities. BMC nephrology. 2013 Sep 26:14():203. doi: 10.1186/1471-2369-14-203. Epub 2013 Sep 26 [PubMed PMID: 24067112]
Level 3 (low-level) evidenceMoinuddin Z, Summers A, Van Dellen D, Augustine T, Herrick SE. Encapsulating peritoneal sclerosis-a rare but devastating peritoneal disease. Frontiers in physiology. 2014:5():470. doi: 10.3389/fphys.2014.00470. Epub 2015 Jan 5 [PubMed PMID: 25601836]
Gayomali C, Hussein U, Cameron SF, Protopapas Z, Finkelstein FO. Incidence of encapsulating peritoneal sclerosis: a single-center experience with long-term peritoneal dialysis in the United States. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2011 May-Jun:31(3):279-86. doi: 10.3747/pdi.2010.00196. Epub [PubMed PMID: 21555415]
Level 2 (mid-level) evidenceBansal S, Sheth H, Siddiqui N, Bender FH, Johnston JR, Piraino B. Incidence of encapsulating peritoneal sclerosis at a single U.S. university center. Advances in peritoneal dialysis. Conference on Peritoneal Dialysis. 2010:26():75-81 [PubMed PMID: 21348385]
Level 3 (low-level) evidencePetrie MC, Traynor JP, Mactier RA. Incidence and outcome of encapsulating peritoneal sclerosis. Clinical kidney journal. 2016 Aug:9(4):624-9. doi: 10.1093/ckj/sfw051. Epub 2016 Jun 20 [PubMed PMID: 27478609]
Johnson DW, Cho Y, Livingston BE, Hawley CM, McDonald SP, Brown FG, Rosman JB, Bannister KM, Wiggins KJ. Encapsulating peritoneal sclerosis: incidence, predictors, and outcomes. Kidney international. 2010 May:77(10):904-12. doi: 10.1038/ki.2010.16. Epub 2010 Mar 10 [PubMed PMID: 20375981]
Brown EA, Bargman J, van Biesen W, Chang MY, Finkelstein FO, Hurst H, Johnson DW, Kawanishi H, Lambie M, de Moraes TP, Morelle J, Woodrow G. Length of Time on Peritoneal Dialysis and Encapsulating Peritoneal Sclerosis - Position Paper for ISPD: 2017 Update. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2017 Jul-Aug:37(4):362-374. doi: 10.3747/pdi.2017.00018. Epub [PubMed PMID: 28676507]
Jagirdar RM, Bozikas A, Zarogiannis SG, Bartosova M, Schmitt CP, Liakopoulos V. Encapsulating Peritoneal Sclerosis: Pathophysiology and Current Treatment Options. International journal of molecular sciences. 2019 Nov 16:20(22):. doi: 10.3390/ijms20225765. Epub 2019 Nov 16 [PubMed PMID: 31744097]
Roumeliotis S, Dounousi E, Salmas M, Eleftheriadis T, Liakopoulos V. Unfavorable Effects of Peritoneal Dialysis Solutions on the Peritoneal Membrane: The Role of Oxidative Stress. Biomolecules. 2020 May 14:10(5):. doi: 10.3390/biom10050768. Epub 2020 May 14 [PubMed PMID: 32423139]
Giacco F, Brownlee M. Oxidative stress and diabetic complications. Circulation research. 2010 Oct 29:107(9):1058-70. doi: 10.1161/CIRCRESAHA.110.223545. Epub [PubMed PMID: 21030723]
Level 3 (low-level) evidenceWong YY, Wong PN, Mak SK, Chan SF, Cheuk YY, Ho LY, Lo KY, Lo MW, Lo KC, Tong GM, Wong AK. Persistent sterile peritoneal inflammation after catheter removal for refractory bacterial peritonitis predicts full-blown encapsulating peritoneal sclerosis. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2013 Sep-Oct:33(5):507-14. doi: 10.3747/pdi.2012.00281. Epub 2013 Aug 1 [PubMed PMID: 23907832]
Level 2 (mid-level) evidenceBraun N, Alscher DM, Fritz P, Edenhofer I, Kimmel M, Gaspert A, Reimold F, Bode-Lesniewska B, Ziegler U, Biegger D, Wüthrich RP, Segerer S. Podoplanin-positive cells are a hallmark of encapsulating peritoneal sclerosis. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2011 Mar:26(3):1033-41. doi: 10.1093/ndt/gfq488. Epub 2010 Aug 13 [PubMed PMID: 20709739]
Level 2 (mid-level) evidenceReis M, Gomes AM, Santos C, Lopes D, Fernandes JC. Encapsulating peritoneal sclerosis: from early diagnosis to successful kidney transplantation. Jornal brasileiro de nefrologia. 2022 Oct-Dec:44(4):587-591. doi: 10.1590/2175-8239-JBN-2021-0001. Epub [PubMed PMID: 33891672]
Tseng CC, Chen JB, Wang IK, Liao SC, Cheng BC, Wu AB, Chang YT, Hung SY, Huang CC. Incidence and outcomes of encapsulating peritoneal sclerosis (EPS) and factors associated with severe EPS. PloS one. 2018:13(1):e0190079. doi: 10.1371/journal.pone.0190079. Epub 2018 Jan 2 [PubMed PMID: 29293548]
Kawanishi H, Kawaguchi Y, Fukui H, Hara S, Imada A, Kubo H, Kin M, Nakamoto M, Ohira S, Shoji T. Encapsulating peritoneal sclerosis in Japan: a prospective, controlled, multicenter study. American journal of kidney diseases : the official journal of the National Kidney Foundation. 2004 Oct:44(4):729-37 [PubMed PMID: 15384025]
Level 2 (mid-level) evidenceVlijm A, van Schuppen J, Lamers AB, Struijk DG, Krediet RT. Imaging in encapsulating peritoneal sclerosis. NDT plus. 2011 Oct:4(5):281-4. doi: 10.1093/ndtplus/sfr068. Epub 2011 Jun 17 [PubMed PMID: 25984169]
Kawaguchi Y, Saito A, Kawanishi H, Nakayama M, Miyazaki M, Nakamoto H, Tranaeus A. Recommendations on the management of encapsulating peritoneal sclerosis in Japan, 2005: diagnosis, predictive markers, treatment, and preventive measures. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2005 Apr:25 Suppl 4():S83-95 [PubMed PMID: 16300277]
Habib SM, Betjes MG, Fieren MW, Boeschoten EW, Abrahams AC, Boer WH, Struijk DG, Ruger W, Krikke C, Westerhuis R, de Sévaux RG, van der Sande FM, Gaasbeek A, Korte MR, Eps Registry. Management of encapsulating peritoneal sclerosis: a guideline on optimal and uniform treatment. The Netherlands journal of medicine. 2011 Nov-Dec:69(11):500-7 [PubMed PMID: 22173363]
Kawanishi H, Watanabe H, Moriishi M, Tsuchiya S. Successful surgical management of encapsulating peritoneal sclerosis. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2005 Apr:25 Suppl 4():S39-47 [PubMed PMID: 16300271]
de Freitas D, Jordaan A, Williams R, Alderdice J, Curwell J, Hurst H, Hutchison A, Brenchley PE, Augustine T, Summers AM. Nutritional management of patients undergoing surgery following diagnosis with encapsulating peritoneal sclerosis. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2008 May-Jun:28(3):271-6 [PubMed PMID: 18474920]
Huan W, Wenyuan G, Changxuan L, Wenli C. Effect of surgery for encapsulating peritoneal sclerosis on mortality in patients undergoing peritoneal dialysis: A meta-analysis. The Journal of international medical research. 2025 May:53(5):3000605251340162. doi: 10.1177/03000605251340162. Epub 2025 May 25 [PubMed PMID: 40415384]
Level 1 (high-level) evidenceKawanishi H. Surgical and medical treatments of encapsulation peritoneal sclerosis. Contributions to nephrology. 2012:177():38-47. doi: 10.1159/000336934. Epub 2012 May 8 [PubMed PMID: 22613913]
Selgas R, Bajo MA, Castro MJ, Sánchez-Tomero JA, Cirugeda A. Managing ultrafiltration failure by peritoneal resting. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2000 Nov-Dec:20(6):595-7 [PubMed PMID: 11216544]
Wirnsberger GH, Ganser K, Domej W, Sauseng G, Moore D, Moczygemba M, Krejs GJ. Sclerosing encapsulating peritonitis: differential diagnosis to peritoneal encapsulation and abdominal cocoon--a case report. Zeitschrift fur Gastroenterologie. 1992 Aug:30(8):534-7 [PubMed PMID: 1413936]
Level 3 (low-level) evidenceTeixeira D, Costa V, Costa P, Alpoim C, Correia P. Congenital peritoneal encapsulation. World journal of gastrointestinal surgery. 2015 Aug 27:7(8):174-7. doi: 10.4240/wjgs.v7.i8.174. Epub [PubMed PMID: 26328038]
Liakopoulos V, Georgianos PI, Vaios V, Roumeliotis S, Karligkiotis A, Zebekakis PE. 10-year-long survival in a PD patient with severe calcifying encapsulating peritoneal sclerosis treated with tamoxifen: a case-report. BMC nephrology. 2020 Mar 31:21(1):110. doi: 10.1186/s12882-020-01769-x. Epub 2020 Mar 31 [PubMed PMID: 32234031]
Level 3 (low-level) evidenceKawanishi H, Banshodani M, Yamashita M, Shintaku S, Dohi K. Surgical Treatment for Encapsulating Peritoneal Sclerosis: 24 Years' Experience. Peritoneal dialysis international : journal of the International Society for Peritoneal Dialysis. 2019 Mar-Apr:39(2):169-174. doi: 10.3747/pdi.2018.00042. Epub 2018 Jul 10 [PubMed PMID: 29991561]
Srisajjakul S, Prapaisilp P, Bangchokdee S. Imaging pearls and differential diagnosis of encapsulating peritoneal sclerosis: Emphasis on computed tomography. Clinical imaging. 2023 Feb:94():116-124. doi: 10.1016/j.clinimag.2022.12.001. Epub 2022 Dec 10 [PubMed PMID: 36527797]
Fisher B, Costantino JP, Wickerham DL, Redmond CK, Kavanah M, Cronin WM, Vogel V, Robidoux A, Dimitrov N, Atkins J, Daly M, Wieand S, Tan-Chiu E, Ford L, Wolmark N. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. Journal of the National Cancer Institute. 1998 Sep 16:90(18):1371-88 [PubMed PMID: 9747868]
Level 1 (high-level) evidencePuckett Y, Patel P, Bokhari AA. Prednisone. StatPearls. 2025 Jan:(): [PubMed PMID: 30521230]
Were F, Desai H. Adhesiolysis. StatPearls. 2025 Jan:(): [PubMed PMID: 33085366]
Paterick TE, Patel N, Tajik AJ, Chandrasekaran K. Improving health outcomes through patient education and partnerships with patients. Proceedings (Baylor University. Medical Center). 2017 Jan:30(1):112-113 [PubMed PMID: 28152110]
Anderson RJ, Bloch S, Armstrong M, Stone PC, Low JT. Communication between healthcare professionals and relatives of patients approaching the end-of-life: A systematic review of qualitative evidence. Palliative medicine. 2019 Sep:33(8):926-941. doi: 10.1177/0269216319852007. Epub 2019 Jun 11 [PubMed PMID: 31184529]
Level 2 (mid-level) evidenceBirkhäuer J, Gaab J, Kossowsky J, Hasler S, Krummenacher P, Werner C, Gerger H. Trust in the health care professional and health outcome: A meta-analysis. PloS one. 2017:12(2):e0170988. doi: 10.1371/journal.pone.0170988. Epub 2017 Feb 7 [PubMed PMID: 28170443]
Level 1 (high-level) evidence