Introduction
Uveitis is a common condition evaluated by ophthalmologists. Uveitis involves inflammation of the middle layers of the eye, the uvea, which comprises the iris, ciliary body, and choroid. This condition accounts for approximately 2.8% to 10% of legal blindness in the US.[1] The etiologies of uveitis can be infectious, inflammatory, medication-related, or idiopathic.[2][3] Uveitis often requires interdisciplinary collaboration among ophthalmologic and rheumatologic teams for diagnosis and treatment. This article discusses granulomatous uveitis, a specific type of inflammatory uveitis. Granulomatous uveitis is traditionally defined by specific clinical findings, including:
- Large mutton-fat keratic precipitates
- Iris nodules, including Busacca nodules on the iris surface, Koeppe nodules at the pupillary margins, and Berlin nodules at the angle of the anterior chamber
- Chronic or insidious onset of inflammation
- Choroidal granulomas or nodular lesions in the posterior segment.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Various causes of granulomatous uveitis have been published in the literature. Common etiologies include the following:
Infectious Causes
Bacterial infections:
- Mycobacterium tuberculosis: Tuberculosis is a classic cause, particularly in endemic areas, and may present with mutton-fat keratic precipitates, choroidal granulomas, and other features.[4][5]
- Syphilis: Syphilis is known as the great masquerader and can cause diverse granulomatous presentations. Please see StatPearls' companion reference, "Syphilis Ocular Manifestations," for further information.
- Lyme disease: Lyme disease is caused by Borrelia burgdorferi and is typically transmitted by ticks.[6]
- Cutibacterium acnes (previously Propionibacterium acnes): Chronic postsurgical endophthalmitis can mimic granulomatous uveitis. Please see StatPearls' companion reference, "Endophthalmitis," for further information.
- Poststreptococcal uveitis: Although poststreptococcal uveitis is classically described as bilateral nongranulomatous anterior uveitis, poststreptococcal uveitis can occasionally manifest with unilateral or bilateral granulomatous features. Poststreptococcal uveitis is presumed to be a type III or IV delayed hypersensitivity reaction (immune-mediated) rather than a direct intraocular infection.[7][8]
- Leprosy (Hansen disease): Leprosy is a less common cause characterized by iris pearls.[9]
- Nontuberculous mycobacterial infections: These infections can occasionally mimic ocular tuberculosis, causing granulomatous intraocular inflammation.[10]
Fungal infections:
- Histoplasmosis: Disseminated histoplasmosis can manifest as granulomatous choroiditis, particularly in patients with immunocompromise due to AIDS.[11]
- Cryptococcus: Disseminated Cryptococcus infection can manifest with multiple choroidal granulomas.[12]
Viral infections:
- Herpesviruses, including herpes simplex virus, varicella-zoster virus, and cytomegalovirus, may cause anterior uveitis, which manifests as granulomatous keratic precipitates. Cytomegalovirus anterior uveitis is typically associated with coin-shaped keratic precipitates.[13][14]
Parasitic infections:
- Toxoplasmosis: Toxoplasmosis is often nongranulomatous but can present with granulomatous features in chronic or severe cases.[15]
- Toxocariasis: Typical patterns of ocular toxocariasis include chronic endophthalmitis, posterior pole granuloma, and peripheral granuloma. Please see StatPearls' companion reference, "Ocular Toxocariasis," for further information.
- Trematode-associated uveitis: Granulomatous intermediate uveitis has been described, especially in endemic areas such as India and Egypt.[16]
Systemic Disorders
- Sarcoidosis: Sarcoidosis is a common cause of granulomatous uveitis characterized by large iris nodules and mutton-fat keratic precipitates. Posterior segment manifestations may be noted, including choroidal granulomas and optic disc granuloma.[17]
- Vogt-Koyanagi-Harada (VKH) disease: VKH disease causes bilateral diffuse granulomatous choroiditis. Patients with pigmented skin may be more frequently affected.[18]
- Chronic granulomatous disease: Chronic granulomatous disease can cause granulomatous uveitis.[19]
- Common variable immunodeficiency: Common variable immunodeficiency has also been associated with granulomatous uveitis.[19]
- Juvenile idiopathic arthritis: Certain cases of juvenile idiopathic arthritis may show granulomatous uveitis, though nongranulomatous uveitis is more common.[20]
- Granuloma annulare: Granuloma annulare can be rarely associated with bilateral granulomatous anterior uveitis, along with typical skin lesions.[21]
- Tubulointerstitial nephritis and uveitis syndrome: Although tubulointerstitial nephritis and uveitis syndrome is usually associated with nongranulomatous uveitis, granulomatous forms have been rarely reported.[22]
Genetic Causes
- Blau syndrome: An autosomal dominant familial autoinflammatory disorder caused by a mutation in the NOD2 gene (CARD15), resulting in dermatitis, arthritis, and uveitis in pediatric patients.[23]
- Several other genetic associations have been identified as relevant to granulomatous uveitis. Relevant associations include HLA-DRB1*04, which is associated with Vogt-Koyanagi-Harada disease.[24][25]
Ocular-Specific Disorders
- Sympathetic ophthalmia: Sympathetic ophthalmia is another cause of bilateral diffuse granulomatous choroiditis, typically following penetrating eye trauma.[26]
- Lens-induced uveitis: Phacoantigenic uveitis, a reaction to retained lens protein, may be associated with granulomatous keratic precipitates. Please see StatPearls' companion reference, "Lens-Induced Inflammation," for further information.
- Postoperative causes: High-density silicone oil injected into the vitreous cavity can cause a granulomatous reaction.[27] Intraocular implants and suture material can also predispose to granulomatous inflammation.[28] Intraocular foreign bodies, including metallic, wooden, and plant materials, can cause a granulomatous reaction.
Drug-Induced
- Brimonidine can cause granulomatous anterior uveitis characterized by multiple large, pigmented keratic precipitates. Brimonidine-associated uveitis typically resolves after stopping brimonidine.[29]
- Other drugs associated with granulomatous uveitis include:
Masquerade Syndromes
Malignant neoplasms, including intraocular lymphoma, systemic lymphoma with intraocular involvement, uveal melanoma, and metastasis, can present with granulomatous uveitis. Histiocytic disorders, including Langerhans cell histiocytosis and Rosai-Dorfman disease, may be associated with granulomatous ocular inflammation.[33]
Miscellaneous
Tattoo-associated granulomatous uveitis: Bilateral granulomatous uveitis can occur after a tattoo.[34]
Idiopathic
Idiopathic granulomatous uveitis is a diagnosis of exclusion applied when a patient presents with classic granulomatous features, such as mutton-fat keratic precipitates, Busacca or Koeppe nodules, or choroidal granulomas, but exhaustive clinical, laboratory, and radiologic testing fails to identify an underlying infectious or systemic cause.[35] Results from studies suggested that a significant portion of uveitis cases initially labeled as idiopathic are later reclassified as specific entities, particularly sarcoidosis or tuberculosis, when systemic symptoms manifest over time.[17] Overall, sarcoidosis is the most frequent identifiable cause of granulomatous uveitis in developed countries, whereas tuberculosis remains a major cause in South Asia and India.[17][36] Although granulomatous uveitis is more common in adults, pediatric presentation is highly suggestive of specific genetic or infectious conditions outlined above, including Blau syndrome, juvenile idiopathic arthritis, ocular toxocariasis, and Vogt-Koyanagi-Harada disease.
Epidemiology
The prevalence of uveitis is approximately 38 to 204 cases per 100,000 people globally.[37] The incidence is approximately 17 to 52 cases per 100,000 person-years.[37] The epidemiology of granulomatous uveitis varies by cause, geography, and ethnicity, among other factors. In areas where tuberculosis is more common, such as resource-limited countries, tuberculosis is a common cause of granulomatous uveitis. Tuberculosis and VKH disease are more common causes in South Asia.[38] Additionally, VKH disease is common in East Asia, accounting for 5% to 8% of uveitis cases, and in Latin American populations.[39][40] Sarcoidosis-related granulomatous uveitis is more common in high-income regions such as Europe and the US and accounts for 3% to 7% of uveitis cases.[41] However, results from recent studies in Japan have shown rising rates of sarcoidosis.[42] Idiopathic cases are difficult to characterize.[43]
Pathophysiology
Because of the wide variation in the etiologies of granulomatous uveitis, the pathophysiology likely varies by specific cause. In general, granulomas form when the innate immune system fails to clear antigens.[44] The immune system activates antigen-presenting cells, such as macrophages and dendritic cells, to respond to both infectious and noninfectious triggers. Antigen-presenting cells present antigen to CD4+ T cells via major histocompatibility complex class II molecules.[45] These CD4+ cells differentiate and produce cytokines, triggering a cascade that activates other immune cells, amplifies the inflammatory response, and ultimately leads to granuloma formation. Furthermore, macrophage polarization into a proinflammatory M1 state and persistent signaling within cytokine networks explain how these granulomas are maintained over time.[46] Key immune pathways involved in this maintenance include T-helper 1 responses mediated by interferon γ, T helper-17 pathways involving IL-17 and IL-23, and tumor necrosis factor α, which plays a central role in granuloma stability.[44]
Histopathology
In general, granulomas are composed of macrophages, epithelioid cells, and multinucleated giant cells. Ocular granulomas can affect any part of the uvea. Various etiologies of granulomatous uveitis can present with distinct histopathologic findings. Intraocular tuberculosis infection is characterized by granulomatous inflammation with central caseous necrosis.[47] Furthermore, sarcoidosis typically causes noncaseating epithelioid giant cell granulomas in tissues, as demonstrated by immunohistochemical staining for CD68+ and CD163+ cells.[17] Moreover, VKH disease primarily presents with panuveitis and diffuse thickening of the uveal tract due to nonnecrotizing granulomatous inflammation.[48] The greasy appearance of mutton fat keratic precipitates is due to the accumulation of large, aggregated clusters of macrophages and epithelioid cells on the corneal endothelium.
History and Physical
Granulomatous uveitis, like other forms of uveitis, can be idiopathic or associated with systemic conditions; therefore, a general review of systems is critical. History should focus on autoimmune conditions, such as sarcoidosis, and infections, such as tuberculosis, although the absence of systemic conditions does not rule out this diagnosis.[49] Joint pain, fatigue, dyspnea, dry cough, and rashes can warrant chest radiography and further evaluation for sarcoidosis. Cough, night sweats, weight loss, or travel history can suggest tuberculosis. A sexual history can also warrant additional laboratory studies for syphilis and other sexually transmitted infections. Targeted systemic review questions can guide further evaluation and assist in diagnosis. Patients with uveitis usually present with ocular symptoms of pain, photophobia, redness, floaters, and decreased vision.
A physical examination should start with visual acuity and intraocular pressure measurements, followed by a pupil examination, a slit-lamp examination, and a dilated fundus examination. In granulomatous uveitis, findings can be present in both the anterior and posterior segments of the eye. Anterior segment examination findings include mutton-fat keratic precipitates on the corneal endothelium (see Image. Mutton-Fat Keratic Precipitates), anterior chamber cells, and iris nodules (see Image. Busacca Nodules in Granulomatous Uveitis). Posterior segment examination findings can include vitreous cells, snowballs, retinal vasculitis, and focal or diffuse choroidal lesions.[50] Choroidal tuberculosis may manifest as small tubercles (see Image. Choroidal Tubercle), larger nodular lesions (choroidal tuberculoma, see Image. Tubercular Choroidal Granuloma), and subretinal abscess (see Image. Choroidal Tuberculosis Abscess). Please see StatPearls' companion reference, "Ocular Tuberculosis," for further information. Typical posterior segment findings of ocular sarcoidosis include choroidal granuloma, retinal vasculitis with candle wax dripping (see Image. Retinal Vasculitis with Candle-Wax Dripping Exudates) or taches de bougie, optic disc granuloma (see Image. Optic Disc Edema and Chorioretinal Granuloma in Granulomatous Uveitis), and retinal arterial macroaneurysms in an inflamed eye. Please see StatPearls' companion references, "Ocular Sarcoidosis" and "Retinal Macroaneurysm," for more information.
Evaluation
Evaluation begins by identifying the anatomic location (anterior, intermediate, or posterior) and the course (acute versus chronic) of uveitis. Certain diseases often present in a specific pattern; for example, panuveitis in a young adult with Vogt-Koyanagi-Harada disease or granulomatous anterior uveitis in a middle-aged individual with sarcoidosis.[43][51] Although laboratory testing is guided by clinical suspicion, important baseline tests such as complete blood count, erythrocyte sedimentation rate, and C-reactive protein are useful for assessing inflammation. Common laboratory tests for infectious causes include a tuberculin skin test (purified protein derivative) or interferon-γ release assay, nontreponemal tests including Venereal Disease Research Laboratory and rapid plasma reagin testing, and fluorescent treponemal antibody absorption testing, serologic IgM and IgG testing for Borrelia burgdorferi, Toxoplasma gondii, herpes simplex virus, varicella-zoster virus, cytomegalovirus, and antigen and antibody tests for Histoplasma organisms and Cryptococcus organisms if suspected.[4] For noninfectious etiologies, testing for serum angiotensin-converting enzyme, calcium, human leukocyte antigen (HLA)-B27, and, in younger patients, HLA-DR15 and HLA-A29 is often sufficient when birdshot chorioretinopathy is suspected.[51] Clinicians should recognize that HLA-B27–associated etiologies and birdshot chorioretinopathy usually present with nongranulomatous uveitis.[43][51] Nonlaboratory diagnostics can also play an important role in evaluating granulomatous uveitis. These modalities often include systemic imaging, tissue biopsy, ocular fluid analysis, and ocular imaging.
Systemic Imaging
Chest radiography and, if findings are abnormal, chest CT are more sensitive for diagnosing sarcoidosis.[17] Lumbar puncture to look for oligoclonal bands or pleocytosis in the cerebrospinal fluid can be performed in patients with suspected multiple sclerosis or VKH disease, respectively.[52] In younger patients, brain and spine MRI can also help diagnose uveitis associated with multiple sclerosis, central nervous system lymphoma, or VKH disease.[53] Fluorodeoxyglucose positron emission tomography (FDG-PET) and echocardiography can also play a role in diagnosing unclear causes of granulomatous uveitis or in cases of suspected cardiac involvement.[54]
Tissue Biopsy
Although not always feasible, obtaining a biopsy can be crucial for diagnosing and managing granulomatous uveitis.[55] Conjunctival biopsy is a safe procedure that can detect noncaseating granulomas in 20% to 60% of patients with sarcoidosis.[56] If lymphoma is suspected, a vitreous or chorioretinal biopsy can identify malignant cells.[55][57] Lastly, a biopsy of an accessible site, such as lymph nodes, is often performed when tuberculosis or sarcoidosis is suspected.[58] A biopsy should be pursued when the results would significantly impact treatment and when a biopsy can be performed safely.[58]
Ocular Fluid Analysis
In cases of suspected intraocular infection or masquerade, an anterior chamber paracentesis, vitreous tap, or vitrectomy can be performed to detect microbial DNA or RNA, calculate the Goldmann-Witmer coefficient, or obtain an IL-10 to IL-6 ratio.[59] The Goldmann-Witmer coefficient compares intraocular antibody concentrations with corresponding serum levels for organisms such as Toxoplasma or Borrelia species.[59] The IL-10 to IL-6 ratio can be an important test in older patients with longstanding uveitis because an elevated ratio may indicate intraocular lymphoma.[59]
Ocular Imaging
Fluorescein angiography: As the gold standard for assessing the blood-retinal barrier, fluorescein angiography is essential for identifying retinal vasculitis and inflammatory optic nerve involvement.[60] In sarcoidosis, fluorescein angiography frequently reveals segmental periphlebitis, often termed candle-wax drippings, and disc hyperfluorescence.[61] In cases of intraocular tuberculosis, fluorescein angiography delineates multifocal serpiginoid choroiditis lesions that characteristically show early hypofluorescence with late hyperfluorescence along active borders.[62][63] Fluorescein angiography is also the primary modality for identifying cystoid macular edema, which appears as a petaloid leakage pattern on late-phase images.[64]
Indocyanine green angiography: As a more effective modality for visualizing choroidal stroma, indocyanine green angiography can detect deeper granulomas invisible on fluorescein angiography.[20][65] A hallmark finding in sarcoidosis, VKH disease, and sympathetic ophthalmia is the presence of hypofluorescent dark dots, which represent localized granulomatous infiltrates. The persistence or disappearance of these spots serves as a critical marker for monitoring therapeutic response.[20][65]
Enhanced-depth imaging optical coherence tomography: This imaging modality enables precise measurement of subfoveal choroidal thickness, a quantifiable biomarker of inflammation in multiple uveitic conditions.[66] In the acute phase of VKH disease, enhanced-depth imaging optical coherence tomography reveals massive choroidal thickening and may reveal septa or fluid-filled compartments (bacillary layer detachment).[67] Although enhanced-depth imaging optical coherence tomography excels at quantifying choroidal thickness and detecting structural changes, combining it with fluorescein angiography, indocyanine green angiography, fundus autofluorescence, and optical coherence tomography angiography provides a comprehensive assessment of structural and vascular alterations in uveitis.[68]
Fundus autofluorescence: Fundus autofluorescence patterns distinguish between active and chronic metabolic stress in the retinal pigment epithelium. Active inflammatory lesions often manifest as hyperautofluorescent areas, whereas healed or atrophic lesions transition to hypoautofluorescence.[69] For example, in VKH disease, fundus autofluorescence patterns evolve with the clinical phase and timing of treatment, shifting from uniform hyperautofluorescence in the early acute stages to mottled or granular patterns when treatment is delayed. In the chronic phase, hypoautofluorescent lesions indicate loss of the retinal pigment epithelium, whereas hyperautofluorescent areas suggest proliferation or edema.[70] In sarcoidosis, fundus autofluorescence is recommended as part of the ancillary imaging toolkit for monitoring posterior segment inflammation.[71] Sarcoid choroidal granulomas, which characteristically appear as multiple, small (mean ± SD, 2.7 ± 4.5 mm), yellow lesions, can be monitored with fundus autofluorescence for retinal pigment epithelium changes overlying the granulomas.[71]
Optical coherence tomography angiography: Optical coherence tomography angiography provides noninvasive, depth-resolved visualization of vascular and structural changes in granulomatous uveitis, enabling detection of neovascularization, assessment of choroidal granulomas, and monitoring of disease activity without intravenous dye administration.[72] Optical coherence tomography angiography can show neovascularization in granulomatous disease of the retina or choroid that may not be visible on traditional imaging. This modality is particularly valuable for distinguishing inflammatory choroidal neovascularization, a sight-threatening complication of infectious and noninfectious uveitis, from avascular inflammatory material in the outer retina.[73] Type 1 subretinal pigment epithelium choroidal neovascularization is particularly well visualized on optical coherence tomography angiography in inflammatory conditions, where these findings may be missed on conventional fluorescein angiography and optical coherence tomography. Optical coherence tomography angiography enables detection by visualizing the neovascular network in the outer retina to the choriocapillaris slab, often appearing as low-lying pigment epithelial detachments on structural optical coherence tomography.[74]
Pediatric Uveitis
The diagnostic evaluation of pediatric granulomatous uveitis is complicated by a silent, asymptomatic presentation that frequently leads to late diagnosis; approximately 46% of children present with established complications, including cataracts (36%) and posterior synechiae (31%).[75][76] Although juvenile idiopathic arthritis is classically nongranulomatous, clinicians must recognize that 28% to 32% of cases exhibit granulomatous features, such as mutton-fat keratic precipitates, especially in antinuclear antibody-positive, oligoarticular juvenile idiopathic arthritis.[20] Consequently, the evaluation for juvenile idiopathic arthritis requires a formal slit-lamp examination rather than general vision screening, with antinuclear antibody testing to guide screening intervals of 3 to 6 months.[20] For the pediatric triad of uveitis, dermatitis, and arthritis, NOD2 genetic sequencing is the definitive diagnostic test for Blau syndrome, supplemented by physical examination for boggy joint swelling and camptodactyly.[75][76]
A systematic, 2-step diagnostic strategy is validated to optimize yield in children, beginning with mandatory screening: complete blood cell count, inflammatory markers (erythrocyte sedimentation rate and C-reactive protein), syphilis serology, tuberculosis testing, serum angiotensin-converting enzyme levels, and chest imaging.[75][76] In the first step of the Uveitis: Clinical and Diagnostic Evaluation study, the tuberculin skin test was the most contributory investigation, aiding diagnosis in 17.1% of children.[50] Second-step testing should be highly specific: measurement of urinary β2-microglobulin for tubulointerstitial nephritis and uveitis syndrome, and Toxoplasma or Toxocara serology for posterior granulomatous lesions.[77][78] Rare monogenic syndromes, such as Mendelian susceptibility to mycobacterial disease, should be considered when STAT1 or IFNGR1 immune defects are suspected.[77][78]
Step-Wise Approach
For vision-threatening or atypical cases, intraocular fluid analysis is highly recommended because it can offer a negative predictive value of approximately 95% for ruling out infectious pathogens.[79][80] Multimodal imaging remains essential: optical coherence tomography identifies subclinical choroidal granulomas and macular edema, whereas fluorescein angiography evaluates retinal vasculitis. Because delayed referral is a primary predictor of long-term blindness, particularly in VKH disease, interdisciplinary collaboration among ophthalmology, rheumatology, and infectious diseases is mandatory to prevent irreversible structural damage.[81] In summary, the following stepwise approach can be used to evaluate a suspected case of granulomatous uveitis. First, determine the primary site of inflammation: anterior (iris or ciliary body), intermediate (vitreous or pars plana), posterior (choroid or retina), or panuveitis.[43] Anatomical patterns often narrow the differential diagnosis; for example, VKH disease typically presents as panuveitis, whereas sarcoidosis frequently involves the anterior and intermediate segments.[43]
Second, identify granulomatous features, such as mutton-fat keratic precipitates, Koeppe and Busacca iris nodules, choroidal granulomas, or a chronic rather than acute clinical course.[43] Third, exclude infectious etiologies with serology or ocular fluid testing. The 3 major infections to exclude are syphilis, tuberculosis, and herpesviruses.
Fourth, use body and ocular imaging to look further for signs of common etiologies. Modalities include chest radiography or CT for sarcoidosis, B-scan ultrasonography, fluorescein angiography, indocyanine green angiography, optical coherence tomography, enhanced-depth imaging optical coherence tomography, and optical coherence tomography angiography. To standardize this process for ocular sarcoidosis, some clinicians use the Revised International Workshop on Ocular Sarcoidosis criteria, which classify cases into definite, presumed, or probable.[82] The framework helps clinicians differentiate sarcoidosis from other mimics by clustering clinical signs, such as mutton-fat keratic precipitates, with systemic findings, such as bilateral hilar lymphadenopathy or elevated serum markers.[82] Finally, if the inflammation is persistent or atypical, or occurs in an older patient, the possibility of intraocular lymphoma should be evaluated by performing a tissue biopsy or measuring the IL-10 to IL-6 ratio.[43]
Treatment / Management
Treating granulomatous uveitis involves assessing the severity and the underlying causes to determine the appropriate therapy. The first branch of decision-making is determining whether uveitis is infectious or noninfectious.[43] If an infectious source is identified (eg, chest lesions suggestive of tuberculosis, syphilis serology results that are positive, polymerase chain reaction evidence of herpes simplex virus), specific antimicrobial therapy is initiated promptly.[43][83] To prevent exacerbation of the underlying infectious agent, corticosteroids, as anti-inflammatory agents, are initiated either concomitantly with or after a brief delay following appropriate antimicrobial therapy.[83] For noninfectious etiologies, immunosuppression is the treatment of choice.[43] Interdisciplinary treatment is crucial in most cases, for example, involving pulmonology for sarcoidosis or infectious disease for tuberculosis.[43][83][84] Sarcoidosis is widely recognized as the most common noninfectious cause of granulomatous uveitis, whereas tuberculosis is the leading infectious cause globally, especially in endemic areas. Treatment of the underlying condition is crucial for controlling uveitis.(B3)
In addition to appropriate antimicrobial agents for infectious causes, the initial treatment for granulomatous uveitis involves topical and systemic corticosteroids, depending on severity.[43][83] Prednisolone acetate 1% eye drops every 1 to 6 hours are often the treatment of choice for most cases of benign or moderate anterior uveitis; however, systemic corticosteroids are often recommended for severe, posterior, or bilateral disease.[43][83][85] Oral prednisone 60 to 100 mg/d (1 to 1.5 mg/kg/d) with a slow taper, or intravenous methylprednisolone 1 g daily for 3 days in fulminant cases, is often a reasonable starting point.[43][83][85] Periocular or intravitreal corticosteroids, such as sub-Tenon or intravitreal triamcinolone injections, can also be used for local control in these cases.[85] The use of cycloplegics is often crucial for reducing pain and preventing synechiae formation.[43] These medications can be contraindicated in patients with primary angle closure glaucoma or patients with known hypersensitivities or allergies to such medications.[43]
Transition to corticosteroid-sparing therapy in cases of systemic use is often crucial to prevent long-term adverse effects. Most guidelines recommend controlling inflammation and symptoms with oral corticosteroids for no longer than 6 to 12 weeks.[86][87][88] If tapering prednisone to less than 10 to 15 mg/d by 12 weeks in unsuccessful, or in cases of recurrent disease, corticosteroid-sparing agents may be initiated.[43][86][87] First-line agents include antimetabolites such as methotrexate (10 to 15 mg once weekly initially), azathioprine (1 to 3 mg/kg/d), or mycophenolate mofetil (1 to 2 g/d).[43][86][87] Second-line and third-line agents and biologics can play vital roles in immunosuppression for patients with granulomatous uveitis, depending on the context. Please see StatPearls' companion reference, "Fluorescein Angiography," for further information.[68][89](A1)
Clinicians should recognize that children are at a higher risk for amblyopia due to vision-obscuring complications such as cataracts or vitreous haze.[90] Additionally, pediatric patients are more prone to corticosteroid-induced ocular hypertension, and systemic growth suppression occurs with oral corticosteroids.[91][92] Therefore, the threshold to initiate corticosteroid-sparing antimetabolites is significantly lower in children than in adults.[93] Table 1 summarizes treatment modalities for noninfectious uveitis after exclusion of infectious causes.(A1)
Table 1. Treatment of Noninfectious Uveitis
Abbreviations: CBC, complete blood count; GI; gastrointestinal; JIA, juvenile idiopathic arthritis; LFTs, liver function tests; VKH, Vogt-Koyanagi-Harada disease;
References for the table:[86][87][88][94][95](A1)
|
Class |
Drug |
Indication |
Advantages |
Limitations and monitoring |
|
Antimetabolites (first-line) |
Methotrexate |
Anterior/intermediate uveitis, JIA, sarcoid |
Weekly dosing, low cost, long safety record |
Slow onset (6–8 wks), hepatotoxicity, cytopenias; monitor CBC, LFTs |
|
|
Mycophenolate mofetil |
Posterior uveitis, panuveitis (VKH, birdshot, sarcoid) |
Well tolerated, effective posteriorly |
GI upset, leukopenia; monitor CBC |
|
|
Azathioprine |
Panuveitis, Behçet disease |
Oral, effective for vasculitis |
Myelosuppression, hepatotoxicity; check thiopurine methyltransferase, nudix hydrolase 15 (NUDT15) before use |
|
Calcineurin inhibitors (second-line/ adjuncts) |
Cyclosporine |
Posterior uveitis, birdshot, VKH, cystoid macular edema |
Potent for retinal/choroidal inflammation |
Nephrotoxicity, hypertension; monitor blood pressure, renal function, drug levels |
|
|
Tacrolimus |
Same as cyclosporine, sometimes better tolerated |
More potent than cyclosporine, oral or topical (rare) |
Similar renal/hypertension issues, neurotoxicity |
|
Alkylating agents (last-resort) |
Cyclophosphamide |
Severe, sight-threatening refractory disease (sympathetic ophthalmia, necrotizing scleritis) |
Very potent, can induce long-term remission |
Risk of malignancy, cytopenias, infertility; reserved for refractory cases |
|
|
Chlorambucil |
Same as cyclophosphamide |
Oral, effective |
High toxicity, risk of leukemia, and gonadal failure |
|
Biologics |
Adalimumab (US Food and Drug Administration approved) |
Behçet disease, JIA, VKH, birdshot, sarcoid |
Subcutaneous injection, good safety/efficacy, rapid |
Expensive, tuberculosis reactivation, infection risk → screen for tuberculosis, hepatits B virus |
|
|
Infliximab |
Behçet disease with vasculitis, refractory sarcoid |
Intravenous infusion, rapid effect |
Infusion reactions, immunogenicity, infection risk |
|
|
Tocilizumab |
Highly effective for refractory uveitic macular edema that has failed TNF-α inhibitors |
Risk of serious infections and gastrointestinal perforation (rare) |
Baseline and periodic CBC (neutrophils/platelets) and LFTs, as well as screening for baseline latent tuberculosis. |
|
|
Janus kinase inhibitors, including tofacitinib and baricitinib |
Oral administration (no needles/infusions), which improves patient adherence |
Increased risk of herpes zoster (shingles) reactivation. Potential for deep vein thrombosis or pulmonary embolism (especially in high-risk patients) |
Regular CBC, LFTs, and renal function.
|
|
Corticteroids |
Dexamethasone intravitreal implant (eg, Ozurdex [Allergan]) |
Excellent for the rapid resolution of acute vitritis and macular edema |
Relatively short duration of action (requires repeat injections every 4 to 6 months) |
Intraocular pressure checks at 2 weeks and 4–6 weeks postinjection |
|
|
Fluocinolone acetonide implants (eg, Retisert [Bausch & Lomb, Inc], Yutiq [Alimera Sciences, Inc]) |
Long-term control of chronic, smoldering posterior uveitis |
High incidence of cataracts; nearly all patients will eventually require cataract surgery; risk of glaucoma |
Frequent, lifelong monitoring of intraocular pressure |
Differential Diagnosis
Clinicians should distinguish granulomatous uveitis from other causes of a red, inflamed eye, as treatment can often differ. Important differential diagnoses to consider include:
- Nongranulomatous uveitis: This class of uveitis, typically idiopathic or HLA-B27–associated anterior uveitis, presents with smaller keratic precipitates, more acute onset, greater pain, and often lacks iris nodules and the classic mutton-fat deposits associated with granulomatous uveitis.[43] Clinicians should recognize that iris nodules, including pupillary nodules or Koeppe nodules, may be noted in nongranulomatous uveitides such as Fuchs uveitis. Please see StatPearls' companion reference, "Amsler Sign," and "Fuchs Uveitis Syndrome," for further information.
- Conjunctivitis, keratitis, or scleritis: Conjunctivitis often presents with more diffuse conjunctival injection rather than perilimbal injection seen with uveitis, does not present with cells in the anterior chamber, and often leads to discharge.[96] Keratitis or corneal ulcers often cause corneal stromal opacities or epithelial defects, both of which are absent in uveitis aside from keratic precipitates. Keratitis often has an identifiable risk factor, such as trauma or contact lens wear, and does not present with significant cell or flare in the anterior chamber unless secondary to inflammation.[97] Scleritis can also coexist with autoimmune diseases; however, scleritis often presents with deep aching pain, pain with eye movement, areas of scleral edema, and nonblanching dilation of scleral vessels.[98] However, scleritis can not only coexist with uveitis but also cause secondary uveitis, particularly in necrotizing scleritis.[99] Clinicians should recognize that scleritis can coexist with uveitis and cause secondary uveitis, particularly in necrotizing scleritis.[100] Furthermore, results from studies suggested that up to 42% of patients with scleritis can develop anterior uveitis.[99]
- Fuchs heterochromic iridocyclitis: Fuchs heterochromic iridocyclitis is currently believed to have a multifactorial etiology that remains poorly understood. However, Fuchs heterochromic iridocyclitis can present with inflammation, keratic precipitates, and iris atrophy that could mimic uveitis.[101][102] This condition is almost always unilateral, presents with low-grade, nonrelapsing inflammation, features fine diffuse keratic precipitates, and is identified by diffuse iris atrophy and heterochromia.[101][102] In contrast, granulomatous uveitis can be unilateral or bilateral, often presents with localized mutton-fat keratic precipitates, and, although possible, granulomatous uveitis is not defined by iris atrophy. Lastly, uveitis responds well to corticosteroids, whereas Fuchs heterochromic iridocyclitis responds poorly to corticosteroids.[101][102] Hemorrhage from the angle of the anterior chamber may occur during paracentesis in eyes with Fuchs heterochromic iridocyclitis, known as the Amsler sign.[103]
- Acute angle-closure glaucoma: Acute angle-closure glaucoma typically presents with a poorly reactive, mid-dilated pupil, a cloudy cornea, and very high intraocular pressure, often greater than 40 mm Hg.[104] Acute angle-closure glaucoma is an ocular emergency requiring immediate reduction in intraocular pressure and can be easily differentiated from uveitis by tonometry and assessment of the iridocorneal angle.[104] After angle closure, posterior synechia may form.
- Endophthalmitis: Defined as a purulent infection inside the eye, endophthalmitis can deceptively look similar to severe granulomatous uveitis due to evidence of intense inflammation.[105][106] Both conditions can present with dense anterior chamber cells and flare, hypopyon, granulomatous keratic precipitates, and vitritis.[106] Disproportionate pain, lid edema, chemosis, rapid vision decline, dense vitritis, and the presence of recent ocular trauma, surgical procedure, or injection are signs favoring endophthalmitis.[106] Diagnostic aqueous or vitreous sampling can help when the diagnosis is unclear.[106]
- Masquerade syndromes: Certain intraocular tumors, such as primary vitreoretinal lymphoma, uveal melanoma, retinoblastoma, or metastatic tumors, can mimic granulomatous uveitis by presenting with anterior chamber cell and flare and vitritis.[107] Very high levels of IL-10 in vitreous, persistent symptoms despite corticosteroid therapy, the presence of a focal mass, or subretinal infiltrates can be a clue to masquerade syndromes.[107] A detailed fundus examination, MRI, and ultrasonography can help identify such masquerades.[107]
Pertinent Studies and Ongoing Trials
Several key landmark clinical trials and studies have shaped the treatment of uveitis:
Multicenter Uveitis Steroid Treatment (MUST) trial: This National Eye Institute-funded trial compared systemic therapy, including corticosteroids and immunosuppressants, with fluocinolone acetonide intravitreal implants.[108] Although the implant provided slightly better control of inflammation, long-term visual outcomes remained similar between the groups.[108] Because systemic therapy has a lower risk of ocular complications such as glaucoma, systemic therapy remains the primary standard of care.[108]
VISUAL I and VISUAL II trials: These phase 3 trials demonstrated that adalimumab, a tumor necrosis factor α inhibitor, effectively treats active and inactive noninfectious uveitis.[54] The results showed that patients receiving adalimumab had a significantly longer time to treatment failure than patients receiving a placebo.[54] Beyond clinical metrics, adalimumab also led to meaningful improvements in patient-reported visual functioning.[54]
First-Line Antimetabolites as Steroid-Sparing Therapy trial (FAST): This study investigated whether mycophenolate mofetil was superior to methotrexate as an initial corticosteroid-sparing agent.[109] The study results showed that methotrexate is noninferior to mycophenolate mofetil, making methotrexate a reasonable first-line choice.[109] The findings suggested that methotrexate might even be more effective in specific cases involving posterior uveitis or panuveitis.[109]
Periocular Versus Intravitreal Corticosteroids for Uveitic Macular Edema trial (POINT): This trial compared 3 regional corticosteroid delivery methods to treat macular edema and the results showed that periocular injections were superior to intravitreal injections in reducing swelling.[100] Consequently, the intravitreal groups achieved significantly greater gains in visual acuity during the first 8 weeks of treatment.[100]
Macular Edema Ranibizumab Versus Intravitreal Steroids Versus Methotrexate (MERIT) trial: Building on previous findings, this trial compared local injections of dexamethasone, methotrexate, and ranibizumab for persistent edema. The dexamethasone implant was the most effective at resolving fluid and improving vision compared to the other 2 treatments.[110] In contrast, intravitreal methotrexate showed very little benefit for this specific indication.[110] The study results established intravitreal corticosteroids as the most effective treatment for persistent uveitic macular edema compared with methotrexate and anti–vascular endothelial growth factor injection.[110]
Toxicity and Adverse Effect Management
Frequent follow-up visits, every 1 to 2 weeks during the active phase, are often crucial for assessing inflammation, detecting complications, and monitoring intraocular pressure, given the frequent use of corticosteroids.[43][84] Preventative measures, such as the use of intraocular pressure-lowering drops, calcium and vitamin D supplementation, and gastric protection, are crucial if corticosteroids are started and prolonged use is required.[43][111] Additional adverse effects include hyperglycemia, hypertension, weight gain, and mood changes. Additionally, periodic laboratory monitoring is often required for patients transitioning to corticosteroid-sparing immunosuppressants.[43][111] Table 1 summarizes the major adverse effects associated with these medications.
Prognosis
Key factors in prognostication include the underlying etiology, duration of inflammation before treatment, response to therapy, patient adherence, and treatment of complications.[112] Sarcoid uveitis often responds well to therapy; conversely, Behçet disease can be explosive and recurrent.[9][113] Vogt-Koyanagi-Harada disease, syphilis, and tuberculosis can respond well to therapy if treated early, but delayed treatment can cause irreversible damage.[43][84] Eyes that present with chronic, smoldering inflammation may already have complications such as posterior synechiae, band-shaped keratopathy, cataracts, vitreous debris or opacity, macular edema, epiretinal membrane, choroidal neovascular membrane, glaucoma, or optic nerve damage due to other causes.[112][114] If the presenting eye responds well to available first-line therapies, the prognosis is often excellent.[43] If the presentation is refractory to multiple lines of therapy, the risk of complications and vision loss increases substantially.[43] As previously discussed, uveitis treatment often requires long-term therapies with frequent appointments; patients who are not regularly evaluated can develop additional preventable complications. Lastly, results from studies showed that up to 60% or more of patients with uveitis will develop at least 1 ocular complication over the course of the disease.[114] However, with modern treatments, most complications can be treated. Results from one large study found that 80% of patients with uveitis had 20/40 or better vision in at least 1 eye at 5-year follow-up.[114]
Complications
Chronic granulomatous uveitis can affect every structure in the eye, leading to numerous complications. Important and common complications include cataract, particularly posterior subcapsular cataract; anterior and posterior synechiae, which in turn could lead to pupillary block and angle-closure glaucoma; open-angle glaucoma resulting from debris clogging the trabecular meshwork or from corticosteroid-induced ocular hypertension; calcific band keratopathy; hypotony and phthisis bulbi from chronic ciliary body inflammation and formation of a cyclitic membrane; cystoid macular edema; epiretinal membrane; choroidal neovascularization; vasculitis; ischemia; vitreous hemorrhage; chronic papilledema and optic nerve damage; amblyopia; and many other complications.[43][84] As previously discussed, prognosis is often favorable. However, educating patients about the importance of adhering to therapy and close follow-up is essential to prevent or address such serious complications.[84] Complications of therapy, including adverse effects of antitubercular therapy, corticosteroids, and immunomodulatory drugs, should also be considered. The underlying systemic disease may also cause manifestations that require treatment.
Deterrence and Patient Education
Results from numerous studies in reputable journals over the years showed that well-informed patients who understand their disease and the rationale behind treatment have higher adherence, fewer complications, and better quality of life.[115][116] Regarding granulomatous uveitis, patients should understand that granulomatous uveitis is an intraocular inflammatory condition that can lead to severe vision loss if not adequately treated.[84] Explaining the chronic nature of granulomatous uveitis can help patients prepare for the long course of treatment and follow-up. Explaining to patients that many complications, such as high intraocular pressure, are silent could help patients present for follow-up appointments. Describing the red-flag symptoms that warrant prompt evaluation can help detect complications early. Ultimately, early recognition and treatment will help prevent long-term visual impairment.[84]
Pearls and Other Issues
Granulomatous uveitis is a clinical pattern defined by mutton-fat keratic precipitates and iris nodules, signaling an underlying systemic disease rather than a single entity. Clinicians must rule out syphilis and tuberculosis before initiating treatment, because corticosteroids alone can worsen these underlying infections. Sarcoidosis and VKH disease are the most frequent noninfectious causes; for sarcoidosis, chest imaging provides a higher diagnostic yield and specificity than serum angiotensin-converting enzyme levels.
Multimodal imaging, such as fluorescein angiography for vascular leakage, indocyanine green angiography for choroidal granulomas, and optical coherence tomography for cystoid macular edema, is essential for comprehensive treatment. Guidelines recommend transitioning to corticosteroid-sparing agents if control requires more than 10 to 15 mg/d of prednisone for longer than 12 weeks. Persistent or refractory inflammation should immediately prompt an evaluation for masquerade syndromes, such as intraocular lymphoma.
Enhancing Healthcare Team Outcomes
As stressed in this article, patients with granulomatous uveitis require timely diagnosis and coordinated long-term treatment to prevent severe visual complications. Given the systemic nature of uveitis, an interprofessional interdisciplinary approach to care is essential.[116] While ophthalmologists treat the ocular presentation of granulomatous uveitis, pulmonologists, infectious disease clinicians, rheumatologists, and nephrologists often contribute expertise in evaluating or treating underlying conditions, symptoms, or syndromes that may arise or lead to granulomatous uveitis. Nurses and advanced practitioners play a key role in educating patients and triaging and monitoring ocular and systemic symptoms. Pharmacists also play a key role in ensuring the safety and effectiveness of commonly used medications such as corticosteroids, immunosuppressants, and antimicrobials. Pharmacists can also play a pivotal role in facilitating access to high-cost emerging biologics used in the treatment of this disease.
Media
(Click Image to Enlarge)
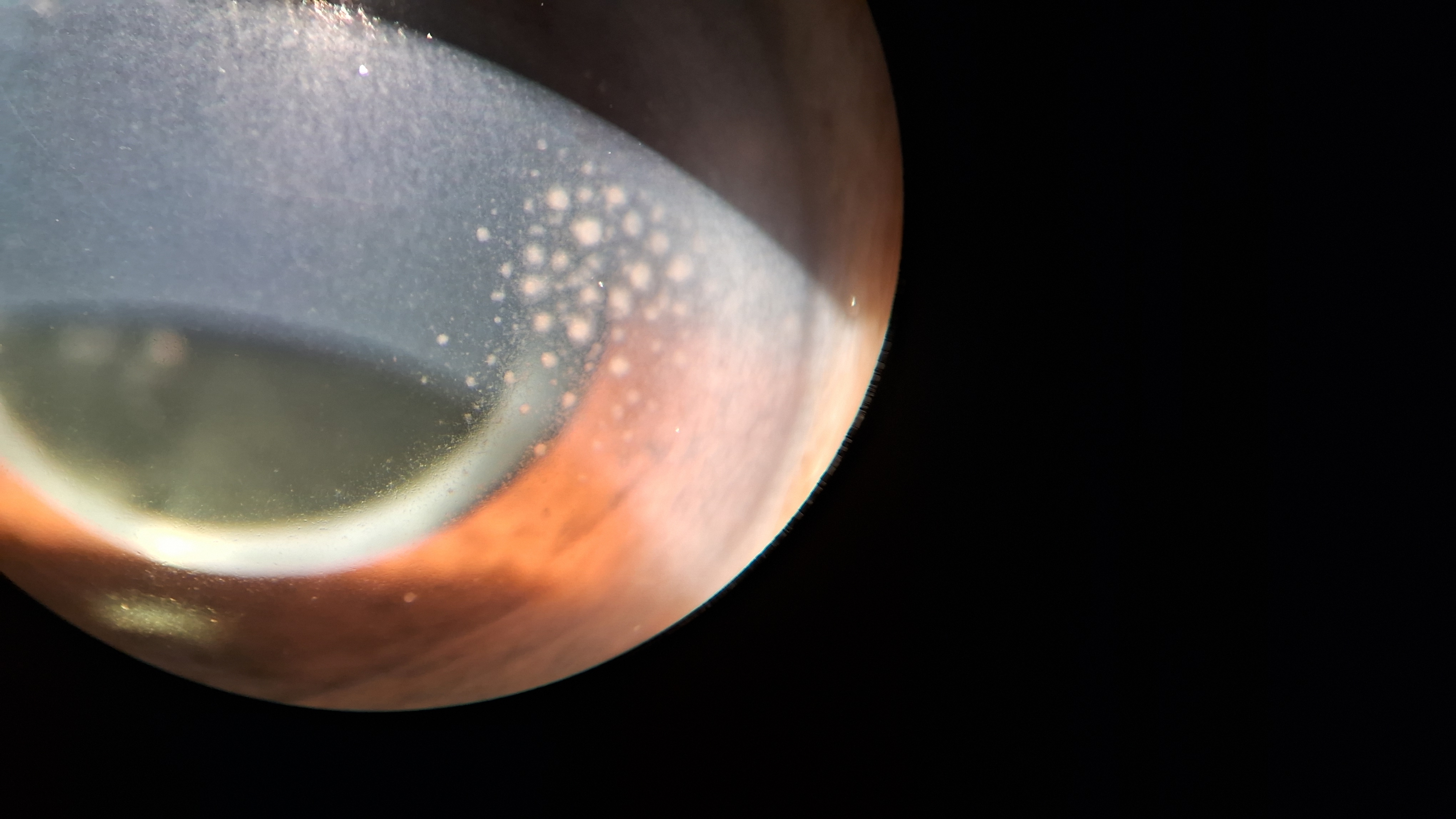
Mutton-Fat Keratic Precipitates. This slit-lamp photograph illustrates large, greasy-appearing "mutton-fat" keratic precipitates on the posterior corneal endothelium, a hallmark clinical finding indicative of granulomatous uveitis.
Contributed by K Tripathy, MD
(Click Image to Enlarge)
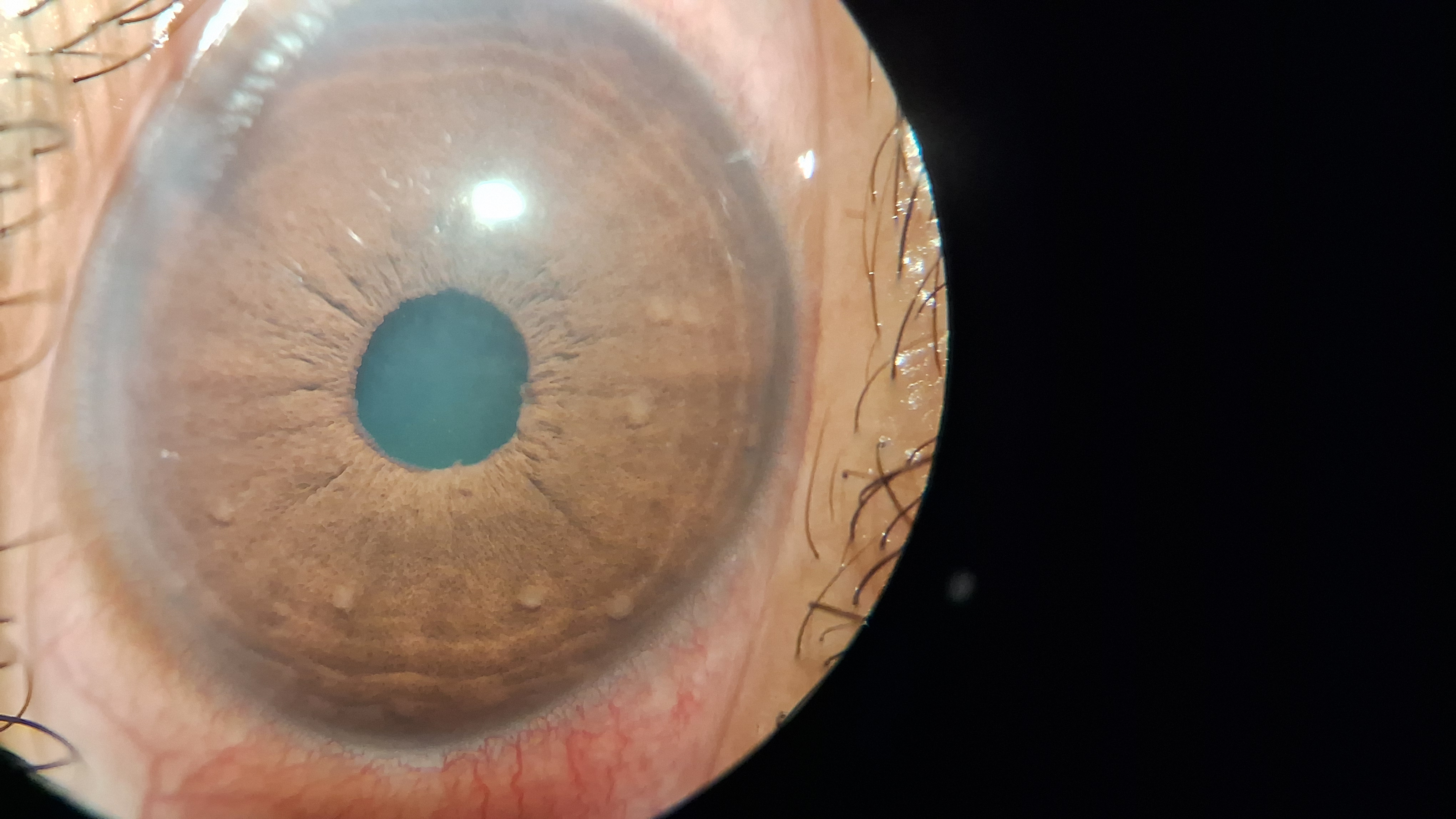
Busacca Nodules in Granulomatous Uveitis. Multiple small, pale inflammatory aggregates on the anterior iris surface, known as Busacca nodules, are a characteristic feature of granulomatous uveitis.
Contributed by K Tripathy, MD
(Click Image to Enlarge)

Choroidal Tubercle. Choroidal tubercle (marked with <) in a patient with miliary tuberculosis.
Contributed by K Tripathy, MD
(Click Image to Enlarge)
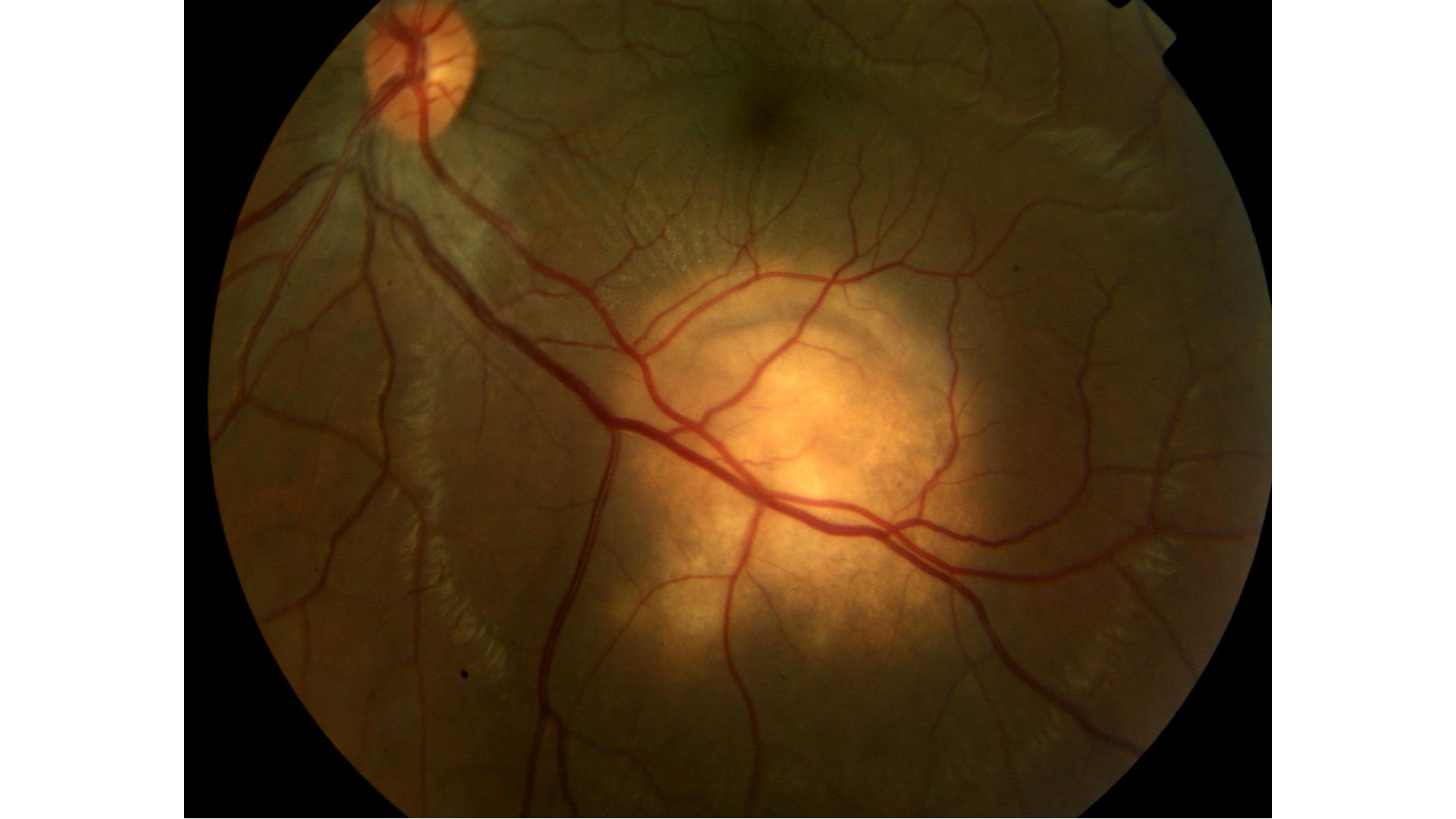
Tubercular Choroidal Granuloma. Large choroidal granuloma with subretinal fluid reaching the macula in a patient with tuberculosis choroiditis.
Contributed by AB Sallam, MD, PhD, FRCOphth
(Click Image to Enlarge)

Choroidal Tuberculosis Abscess. Image of a subretinal abscess in choroidal tuberculosis.
Contributed by K Tripathy, MD
(Click Image to Enlarge)

Retinal Vasculitis with Candle-Wax Dripping Exudates. This fundus photograph shows multifocal, yellowish-white perivascular exudates, known as candle-wax dripping, a classic clinical sign of retinal vasculitis frequently associated with systemic sarcoidosis.
Contributed by KB Murthy, MRCOphth
(Click Image to Enlarge)
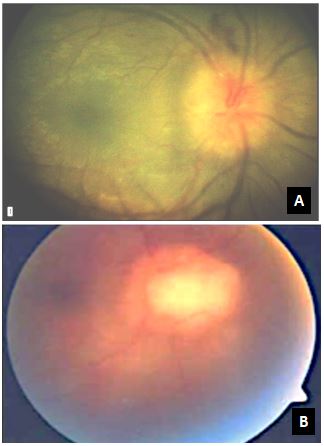
Optic Disc Edema and Chorioretinal Granuloma in Granulomatous Uveitis. These fundus photographs illustrate significant optic nerve head swelling with blurred margins (A) and a large, elevated yellowish-white chorioretinal granuloma in the posterior pole (B), classic posterior segment manifestations of ocular sarcoidosis.
Contributed by KB Murthy, MRCOphth
References
Miserocchi E, Fogliato G, Modorati G, Bandello F. Review on the worldwide epidemiology of uveitis. European journal of ophthalmology. 2013 Sep-Oct:23(5):705-17. doi: 10.5301/ejo.5000278. Epub 2013 May 3 [PubMed PMID: 23661536]
Dick AD, Tundia N, Sorg R, Zhao C, Chao J, Joshi A, Skup M. Risk of Ocular Complications in Patients with Noninfectious Intermediate Uveitis, Posterior Uveitis, or Panuveitis. Ophthalmology. 2016 Mar:123(3):655-62. doi: 10.1016/j.ophtha.2015.10.028. Epub 2015 Dec 19 [PubMed PMID: 26712559]
Bertrand PJ, Jamilloux Y, Ecochard R, Richard-Colmant G, Gerfaud-Valentin M, Guillaud M, Denis P, Kodjikian L, Sève P. Uveitis: Autoimmunity… and beyond. Autoimmunity reviews. 2019 Sep:18(9):102351. doi: 10.1016/j.autrev.2019.102351. Epub 2019 Jul 16 [PubMed PMID: 31323361]
Miller JM, Binnicker MJ, Campbell S, Carroll KC, Chapin KC, Gonzalez MD, Harrington A, Jerris RC, Kehl SC, Leal SM Jr, Patel R, Pritt BS, Richter SS, Robinson-Dunn B, Snyder JW, Telford S 3rd, Theel ES, Thomson RB Jr, Weinstein MP, Yao JD. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2024 Mar 5:():. pii: ciae104. doi: 10.1093/cid/ciae104. Epub 2024 Mar 5 [PubMed PMID: 38442248]
Cunningham ET Jr, Rathinam SR, Albini TA, Chee SP, Zierhut M. Tuberculous uveitis. Ocular immunology and inflammation. 2015 Feb:23(1):2-6. doi: 10.3109/09273948.2014.1004016. Epub [PubMed PMID: 25615806]
Bernard A, Seve P, Abukhashabh A, Roure-Sobas C, Boibieux A, Denis P, Broussolle C, Mathis T, Kodjikian L. Lyme-associated uveitis: Clinical spectrum and review of literature. European journal of ophthalmology. 2020 Sep:30(5):874-885. doi: 10.1177/1120672119856943. Epub 2019 Jun 26 [PubMed PMID: 31238716]
Abderrahim K, Chebil A, Falfoul Y, Bouladi M, El Matri L. Granulomatous uveitis and reactive arthritis as manifestations of post-streptococcal syndrome. International ophthalmology. 2015 Oct:35(5):641-3. doi: 10.1007/s10792-012-9626-1. Epub 2012 Sep 18 [PubMed PMID: 22986580]
Besada E, Frauens BJ. Unilateral granulomatous post-streptococcal uveitis with elevated tension. Optometry and vision science : official publication of the American Academy of Optometry. 2008 Nov:85(11):E1110-5. doi: 10.1097/OPX.0b013e31818b9622. Epub [PubMed PMID: 18981915]
Level 3 (low-level) evidenceDana MR, Merayo-Lloves J, Schaumberg DA, Foster CS. Prognosticators for visual outcome in sarcoid uveitis. Ophthalmology. 1996 Nov:103(11):1846-53 [PubMed PMID: 8942880]
Level 2 (mid-level) evidenceChu HS, Chang SC, Shen EP, Hu FR. Nontuberculous mycobacterial ocular infections--comparing the clinical and microbiological characteristics between Mycobacterium abscessus and Mycobacterium massiliense. PloS one. 2015:10(1):e0116236. doi: 10.1371/journal.pone.0116236. Epub 2015 Jan 12 [PubMed PMID: 25581038]
Klintworth GK, Hollingsworth AS, Lusman PA, Bradford WD. Granulomatous choroiditis in a case of disseminated histoplasmosis. Histologic demonstration of Histoplasma capsulatum in choroidal lesions. Archives of ophthalmology (Chicago, Ill. : 1960). 1973 Jul:90(1):45-8 [PubMed PMID: 4714795]
Level 3 (low-level) evidenceAndreola C, Ribeiro MP, de Carli CR, Gouvea AL, Curi AL. Multifocal choroiditis in disseminated Cryptococcus neoformans infection. American journal of ophthalmology. 2006 Aug:142(2):346-8 [PubMed PMID: 16876530]
Kardeş E, Bozkurt K, Sezgin Akçay Bİ, Ünlü C, Aydoğan Gezginaslan T, Ergin A. Clinical Features and Prognosis of Herpetic Anterior Uveitis. Turkish journal of ophthalmology. 2016 Jun:46(3):109-113 [PubMed PMID: 27800272]
Alfawaz A. Cytomegalovirus-related corneal endotheliitis: A review article. Saudi journal of ophthalmology : official journal of the Saudi Ophthalmological Society. 2013 Jan:27(1):47-9. doi: 10.1016/j.sjopt.2011.10.001. Epub 2011 Oct 10 [PubMed PMID: 23964187]
Hall BR, Oliver GE, Wilkinson M. A presentation of longstanding toxoplasmosis chorioretinitis. Optometry (St. Louis, Mo.). 2009 Jan:80(1):23-8. doi: 10.1016/j.optm.2008.03.007. Epub [PubMed PMID: 19111254]
Level 3 (low-level) evidenceAmin RH, Abdullatif AM. Management of presumed trematode-induced granulomatous intermediate uveitis. Eye (London, England). 2023 Aug:37(11):2299-2304. doi: 10.1038/s41433-022-02336-4. Epub 2022 Dec 7 [PubMed PMID: 36477731]
Giorgiutti S, Jacquot R, El Jammal T, Bert A, Jamilloux Y, Kodjikian L, Sève P. Sarcoidosis-Related Uveitis: A Review. Journal of clinical medicine. 2023 Apr 29:12(9):. doi: 10.3390/jcm12093194. Epub 2023 Apr 29 [PubMed PMID: 37176633]
O'Keefe GA, Rao NA. Vogt-Koyanagi-Harada disease. Survey of ophthalmology. 2017 Jan-Feb:62(1):1-25. doi: 10.1016/j.survophthal.2016.05.002. Epub 2016 May 27 [PubMed PMID: 27241814]
Level 3 (low-level) evidenceSmith JA, Mackensen F, Sen HN, Leigh JF, Watkins AS, Pyatetsky D, Tessler HH, Nussenblatt RB, Rosenbaum JT, Reed GF, Vitale S, Smith JR, Goldstein DA. Epidemiology and course of disease in childhood uveitis. Ophthalmology. 2009 Aug:116(8):1544-51, 1551.e1. doi: 10.1016/j.ophtha.2009.05.002. Epub [PubMed PMID: 19651312]
Papasavvas I, Herbort CP Jr. Granulomatous Features in Juvenile Idiopathic Arthritis-Associated Uveitis is Not a Rare Occurrence. Clinical ophthalmology (Auckland, N.Z.). 2021:15():1055-1059. doi: 10.2147/OPTH.S299436. Epub 2021 Mar 8 [PubMed PMID: 33727787]
Reddy HS, Khurana RN, Rao NA, Chopra V. Granuloma annulare anterior uveitis. Ocular immunology and inflammation. 2008 Jan-Feb:16(1):55-7. doi: 10.1080/09273940801899814. Epub [PubMed PMID: 18379945]
Level 3 (low-level) evidenceBograd A, Heiligenhaus A, Reuter S, Tappeiner C. A Comprehensive Review of Tubulointerstitial Nephritis and Uveitis (TINU) Syndrome. Biomedicines. 2025 Jan 26:13(2):. doi: 10.3390/biomedicines13020300. Epub 2025 Jan 26 [PubMed PMID: 40002713]
Takada S, Saito MK, Kambe N. Blau Syndrome: NOD2-related systemic autoinflammatory granulomatosis. Giornale italiano di dermatologia e venereologia : organo ufficiale, Societa italiana di dermatologia e sifilografia. 2020 Oct:155(5):537-541. doi: 10.23736/S0392-0488.19.06524-6. Epub 2020 Jul 2 [PubMed PMID: 32618442]
Sarup V, Foster CS. HLA associations in chronic vision threatening uveitis. Seminars in ophthalmology. 2013 Sep-Nov:28(5-6):333-6. doi: 10.3109/08820538.2013.825282. Epub [PubMed PMID: 24138042]
Kuiper JJW, Venema WJ. HLA-A29 and Birdshot Uveitis: Further Down the Rabbit Hole. Frontiers in immunology. 2020:11():599558. doi: 10.3389/fimmu.2020.599558. Epub 2020 Nov 11 [PubMed PMID: 33262772]
Pleyer U, Dutescu M. [Sympathetic ophthalmia]. Der Ophthalmologe : Zeitschrift der Deutschen Ophthalmologischen Gesellschaft. 2009 Feb:106(2):167-75; quiz 176. doi: 10.1007/s00347-008-1911-z. Epub [PubMed PMID: 19198848]
Wickham L, Asaria RH, Alexander R, Luthert P, Charteris DG. Immunopathology of intraocular silicone oil: enucleated eyes. The British journal of ophthalmology. 2007 Feb:91(2):253-7 [PubMed PMID: 17005543]
Koura Y, Fukushima A, Nishino K, Ishida W, Nakakuki T, Sento M, Yamazoe K, Yamaguchi T, Misyoshi T, Ueno H. Inflammatory reaction following cataract surgery and implantation of acrylic intraocular lens in rabbits with endotoxin-induced uveitis. Eye (London, England). 2006 May:20(5):606-10 [PubMed PMID: 15999134]
Agarwal M, Dutta Majumder P, Babu K, Konana VK, Goyal M, Touhami S, Stanescu-Segall D, Bodaghi B. Drug-induced uveitis: A review. Indian journal of ophthalmology. 2020 Sep:68(9):1799-1807. doi: 10.4103/ijo.IJO_816_20. Epub [PubMed PMID: 32823396]
Warwar RE, Bullock JD, Ballal D. Cystoid macular edema and anterior uveitis associated with latanoprost use. Experience and incidence in a retrospective review of 94 patients. Ophthalmology. 1998 Feb:105(2):263-8 [PubMed PMID: 9479285]
Level 2 (mid-level) evidenceFraunfelder FW, Fraunfelder FT. Bisphosphonates and ocular inflammation. The New England journal of medicine. 2003 Mar 20:348(12):1187-8 [PubMed PMID: 12646685]
Gkiozos I, Kopitopoulou A, Kalkanis A, Vamvakaris IN, Judson MA, Syrigos KN. Sarcoidosis-Like Reactions Induced by Checkpoint Inhibitors. Journal of thoracic oncology : official publication of the International Association for the Study of Lung Cancer. 2018 Aug:13(8):1076-1082. doi: 10.1016/j.jtho.2018.04.031. Epub 2018 May 12 [PubMed PMID: 29763666]
Coupland SE, Heimann H, Bechrakis NE. Primary intraocular lymphoma: a review of the clinical, histopathological and molecular biological features. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2004 Nov:242(11):901-13 [PubMed PMID: 15565454]
Ostheimer TA, Burkholder BM, Leung TG, Butler NJ, Dunn JP, Thorne JE. Tattoo-associated uveitis. American journal of ophthalmology. 2014 Sep:158(3):637-43.e1. doi: 10.1016/j.ajo.2014.05.019. Epub 2014 May 27 [PubMed PMID: 24875002]
Level 2 (mid-level) evidenceKanavi MR, Soheilian M, Naghshgar N. Confocal scan of keratic precipitates in uveitic eyes of various etiologies. Cornea. 2010 Jun:29(6):650-4. doi: 10.1097/ICO.0b013e3181c2967e. Epub [PubMed PMID: 20458232]
Parchand S, Tandan M, Gupta V, Gupta A. Intermediate uveitis in Indian population. Journal of ophthalmic inflammation and infection. 2011 Jun:1(2):65-70. doi: 10.1007/s12348-011-0020-3. Epub 2011 Feb 23 [PubMed PMID: 21484178]
Tsirouki T, Dastiridou A, Symeonidis C, Tounakaki O, Brazitikou I, Kalogeropoulos C, Androudi S. A Focus on the Epidemiology of Uveitis. Ocular immunology and inflammation. 2018:26(1):2-16. doi: 10.1080/09273948.2016.1196713. Epub 2016 Jul 28 [PubMed PMID: 27467180]
Biswas J, Narain S, Das D, Ganesh SK. Pattern of uveitis in a referral uveitis clinic in India. International ophthalmology. 1996-1997:20(4):223-8 [PubMed PMID: 9112191]
Ohguro N, Sonoda KH, Takeuchi M, Matsumura M, Mochizuki M. The 2009 prospective multi-center epidemiologic survey of uveitis in Japan. Japanese journal of ophthalmology. 2012 Sep:56(5):432-5. doi: 10.1007/s10384-012-0158-z. Epub 2012 Jul 3 [PubMed PMID: 22752308]
Level 2 (mid-level) evidenceSukavatcharin S, Tsai JH, Rao NA. Vogt-Koyanagi-Harada disease in Hispanic patients. International ophthalmology. 2007 Apr-Jun:27(2-3):143-8 [PubMed PMID: 17380271]
Herbort CP, Rao NA, Mochizuki M, members of Scientific Committee of First International Workshop on Ocular Sarcoidosis. International criteria for the diagnosis of ocular sarcoidosis: results of the first International Workshop On Ocular Sarcoidosis (IWOS). Ocular immunology and inflammation. 2009 May-Jun:17(3):160-9. doi: 10.1080/09273940902818861. Epub [PubMed PMID: 19585358]
Morimoto T, Azuma A, Abe S, Usuki J, Kudoh S, Sugisaki K, Oritsu M, Nukiwa T. Epidemiology of sarcoidosis in Japan. The European respiratory journal. 2008 Feb:31(2):372-9 [PubMed PMID: 17959635]
Maghsoudlou P, Epps SJ, Guly CM, Dick AD. Uveitis in Adults: A Review. JAMA. 2025 Aug 5:334(5):419-434. doi: 10.1001/jama.2025.4358. Epub [PubMed PMID: 40434762]
Ito T, Connett JM, Kunkel SL, Matsukawa A. The linkage of innate and adaptive immune response during granulomatous development. Frontiers in immunology. 2013:4():10. doi: 10.3389/fimmu.2013.00010. Epub 2013 Jan 31 [PubMed PMID: 23386849]
Co DO, Hogan LH, Il-Kim S, Sandor M. T cell contributions to the different phases of granuloma formation. Immunology letters. 2004 Mar 29:92(1-2):135-42 [PubMed PMID: 15081537]
Level 3 (low-level) evidenceMarino S, Cilfone NA, Mattila JT, Linderman JJ, Flynn JL, Kirschner DE. Macrophage polarization drives granuloma outcome during Mycobacterium tuberculosis infection. Infection and immunity. 2015 Jan:83(1):324-38. doi: 10.1128/IAI.02494-14. Epub 2014 Nov 3 [PubMed PMID: 25368116]
Basu S, Wakefield D, Biswas J, Rao NA. Pathogenesis and Pathology of Intraocular Tuberculosis. Ocular immunology and inflammation. 2015 Aug:23(4):353-357. doi: 10.3109/09273948.2015.1056536. Epub [PubMed PMID: 29265968]
Rao NA. Pathology of Vogt-Koyanagi-Harada disease. International ophthalmology. 2007 Apr-Jun:27(2-3):81-5 [PubMed PMID: 17435969]
Mehta H, Sim DA, Keane PA, Zarranz-Ventura J, Gallagher K, Egan CA, Westcott M, Lee RW, Tufail A, Pavesio CE. Structural changes of the choroid in sarcoid- and tuberculosis-related granulomatous uveitis. Eye (London, England). 2015 Aug:29(8):1060-8. doi: 10.1038/eye.2015.65. Epub 2015 May 29 [PubMed PMID: 26021867]
Grumet P, Kodjikian L, de Parisot A, Errera MH, Sedira N, Heron E, Pérard L, Cornut PL, Schneider C, Rivière S, Ollé P, Pugnet G, Cathébras P, Manoli P, Bodaghi B, Saadoun D, Baillif S, Tieulie N, Andre M, Chiambaretta F, Bonin N, Bielefeld P, Bron A, Mouriaux F, Bienvenu B, Vicente S, Bin S, Labetoulle M, Broussolle C, Jamilloux Y, Decullier E, Sève P, ULISSE group. Contribution of diagnostic tests for the etiological assessment of uveitis, data from the ULISSE study (Uveitis: Clinical and medicoeconomic evaluation of a standardized strategy of the etiological diagnosis). Autoimmunity reviews. 2018 Apr:17(4):331-343. doi: 10.1016/j.autrev.2017.10.018. Epub 2018 Feb 7 [PubMed PMID: 29427823]
Jabs DA, Busingye J. Approach to the diagnosis of the uveitides. American journal of ophthalmology. 2013 Aug:156(2):228-36. doi: 10.1016/j.ajo.2013.03.027. Epub 2013 May 10 [PubMed PMID: 23668682]
Bernier R, Gavoille A, Chirpaz N, Jamilloux Y, Kodjikian L, Mathis T, Sève P. Diagnostic value of lumbar puncture for the etiological assessment of uveitis: a retrospective cohort of 188 patients. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2022 May:260(5):1651-1662. doi: 10.1007/s00417-021-05514-4. Epub 2022 Jan 6 [PubMed PMID: 34988612]
Level 2 (mid-level) evidenceLi CQ, Cho AA, Edward NJ, Edward DP, Fajardo RG, Mafee MF. Magnetic resonance imaging of uveitis. Neuroradiology. 2015 Aug:57(8):825-32. doi: 10.1007/s00234-015-1531-7. Epub 2015 Apr 24 [PubMed PMID: 25903430]
Sheppard J, Joshi A, Betts KA, Hudgens S, Tari S, Chen N, Skup M, Dick AD. Effect of Adalimumab on Visual Functioning in Patients With Noninfectious Intermediate Uveitis, Posterior Uveitis, and Panuveitis in the VISUAL-1 and VISUAL-2 Trials. JAMA ophthalmology. 2017 Jun 1:135(6):511-518. doi: 10.1001/jamaophthalmol.2017.0603. Epub [PubMed PMID: 28426849]
Patnaik G, Annamalai R, Biswas J. Intraocular biopsy in uveitis. Indian journal of ophthalmology. 2020 Sep:68(9):1838-1843. doi: 10.4103/ijo.IJO_1325_20. Epub [PubMed PMID: 32823400]
Korkmaz Ekren P, Mogulkoc N, Toreyin ZN, Egrilmez S, Veral A, Akalın T, Bacakoglu F. Conjunctival Biopsy as a First Choice to Confirm a Diagnosis of Sarcoidosis. Sarcoidosis, vasculitis, and diffuse lung diseases : official journal of WASOG. 2016 Oct 7:33(3):196-200 [PubMed PMID: 27758983]
Johnston RL, Tufail A, Lightman S, Luthert PJ, Pavesio CE, Cooling RJ, Charteris D. Retinal and choroidal biopsies are helpful in unclear uveitis of suspected infectious or malignant origin. Ophthalmology. 2004 Mar:111(3):522-8 [PubMed PMID: 15019330]
Level 3 (low-level) evidenceCrouser ED, Maier LA, Wilson KC, Bonham CA, Morgenthau AS, Patterson KC, Abston E, Bernstein RC, Blankstein R, Chen ES, Culver DA, Drake W, Drent M, Gerke AK, Ghobrial M, Govender P, Hamzeh N, James WE, Judson MA, Kellermeyer L, Knight S, Koth LL, Poletti V, Raman SV, Tukey MH, Westney GE, Baughman RP. Diagnosis and Detection of Sarcoidosis. An Official American Thoracic Society Clinical Practice Guideline. American journal of respiratory and critical care medicine. 2020 Apr 15:201(8):e26-e51. doi: 10.1164/rccm.202002-0251ST. Epub [PubMed PMID: 32293205]
Level 1 (high-level) evidenceDe Groot-Mijnes JD, Rothova A, Van Loon AM, Schuller M, Ten Dam-Van Loon NH, De Boer JH, Schuurman R, Weersink AJ. Polymerase chain reaction and Goldmann-Witmer coefficient analysis are complimentary for the diagnosis of infectious uveitis. American journal of ophthalmology. 2006 Feb:141(2):313-8 [PubMed PMID: 16458686]
Level 3 (low-level) evidenceLittlewood R, Mollan SP, Pepper IM, Hickman SJ. The Utility of Fundus Fluorescein Angiography in Neuro-Ophthalmology. Neuro-ophthalmology (Aeolus Press). 2019 Aug:43(4):217-234. doi: 10.1080/01658107.2019.1604764. Epub 2019 Aug 21 [PubMed PMID: 31528186]
O'Keefe GAD, Rao NA. Progress in the diagnosis of ocular sarcoidosis. Indian journal of ophthalmology. 2022 Apr:70(4):1121-1129. doi: 10.4103/ijo.IJO_2830_21. Epub [PubMed PMID: 35325997]
Bansal R, Basu S, Gupta A, Rao N, Invernizzi A, Kramer M. Imaging in tuberculosis-associated uveitis. Indian journal of ophthalmology. 2017 Apr:65(4):264-270. doi: 10.4103/ijo.IJO_464_16. Epub [PubMed PMID: 28513488]
Bansal R, Gupta V. Tubercular serpiginous choroiditis. Journal of ophthalmic inflammation and infection. 2022 Nov 9:12(1):37. doi: 10.1186/s12348-022-00312-3. Epub 2022 Nov 9 [PubMed PMID: 36352169]
Naseripour M, Hemmati S, Chaibakhsh S, Gordiz A, Miri L, Abdi F. Cystoid macular oedema without leakage in fluorescein angiography: a literature review. Eye (London, England). 2023 Jun:37(8):1519-1526. doi: 10.1038/s41433-022-02230-z. Epub 2022 Sep 10 [PubMed PMID: 36088420]
Herbort CP Jr, Tugal-Tutkun I, Mantovani A, Neri P, Khairallah M, Papasavvas I. Advances and potential new developments in imaging techniques for posterior uveitis Part 2: invasive imaging methods. Eye (London, England). 2021 Jan:35(1):52-73. doi: 10.1038/s41433-020-1072-0. Epub 2020 Aug 10 [PubMed PMID: 32778739]
Level 3 (low-level) evidenceBehdad B, Rahmani S, Montahaei T, Soheilian R, Soheilian M. Enhanced depth imaging OCT (EDI-OCT) findings in acute phase of sympathetic ophthalmia. International ophthalmology. 2015 Jun:35(3):433-9. doi: 10.1007/s10792-015-0058-6. Epub 2015 Mar 15 [PubMed PMID: 25772275]
Level 3 (low-level) evidenceGanesh SK, Mistry S, Nair N. Role of Swept source optical coherence tomography in management of acute Vogt-Koyanagi-Harada's disease. Indian journal of ophthalmology. 2022 Jul:70(7):2458-2463. doi: 10.4103/ijo.IJO_1944_21. Epub [PubMed PMID: 35791133]
Agarwal A, Pichi F, Invernizzi A, Grewal DS, Singh RB, Upadhyay A. Stepwise approach for fundus imaging in the diagnosis and management of posterior uveitis. Survey of ophthalmology. 2023 May-Jun:68(3):446-480. doi: 10.1016/j.survophthal.2023.01.006. Epub 2023 Jan 29 [PubMed PMID: 36724831]
Level 3 (low-level) evidenceMauschitz MM, Zeller M, Sagar P, Biswal S, Guzman G, Terheyden JH, Meyer CH, Holz FG, Heinz C, Pleyer U, Finger RP, Wintergerst MWM. Fundus Autofluorescence in Posterior and Panuveitis-An Under-Estimated Imaging Technique: A Review and Case Series. Biomolecules. 2024 Apr 25:14(5):. doi: 10.3390/biom14050515. Epub 2024 Apr 25 [PubMed PMID: 38785922]
Level 2 (mid-level) evidenceKoizumi H, Maruyama K, Kinoshita S. Blue light and near-infrared fundus autofluorescence in acute Vogt-Koyanagi-Harada disease. The British journal of ophthalmology. 2010 Nov:94(11):1499-505. doi: 10.1136/bjo.2009.164665. Epub 2009 Dec 3 [PubMed PMID: 19965835]
Belperio JA, Shaikh F, Abtin F, Fishbein MC, Saggar R, Tsui E, Lynch JP 3rd. Extrapulmonary sarcoidosis with a focus on cardiac, nervous system, and ocular involvement. EClinicalMedicine. 2021 Jul:37():100966. doi: 10.1016/j.eclinm.2021.100966. Epub 2021 Jun 27 [PubMed PMID: 34258571]
Pichi F, Sarraf D, Arepalli S, Lowder CY, Cunningham ET Jr, Neri P, Albini TA, Gupta V, Baynes K, Srivastava SK. The application of optical coherence tomography angiography in uveitis and inflammatory eye diseases. Progress in retinal and eye research. 2017 Jul:59():178-201. doi: 10.1016/j.preteyeres.2017.04.005. Epub 2017 Apr 29 [PubMed PMID: 28465249]
Pichi F, Hay S. Use of optical coherence tomography angiography in the uveitis clinic. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2023 Jan:261(1):23-36. doi: 10.1007/s00417-022-05763-x. Epub 2022 Jul 16 [PubMed PMID: 35841398]
Aggarwal K, Agarwal A, Sharma A, Sharma K, Gupta V, OCTA Study Group. DETECTION OF TYPE 1 CHOROIDAL NEOVASCULAR MEMBRANES USING OPTICAL COHERENCE TOMOGRAPHY ANGIOGRAPHY IN TUBERCULAR POSTERIOR UVEITIS. Retina (Philadelphia, Pa.). 2019 Aug:39(8):1595-1606. doi: 10.1097/IAE.0000000000002176. Epub [PubMed PMID: 29689028]
Maleki A, Anesi SD, Look-Why S, Manhapra A, Foster CS. Pediatric uveitis: A comprehensive review. Survey of ophthalmology. 2022 Mar-Apr:67(2):510-529. doi: 10.1016/j.survophthal.2021.06.006. Epub 2021 Jun 25 [PubMed PMID: 34181974]
Level 3 (low-level) evidenceNguyen AT, Koné-Paut I, Dusser P. Diagnosis and Management of Non-Infectious Uveitis in Pediatric Patients. Paediatric drugs. 2024 Jan:26(1):31-47. doi: 10.1007/s40272-023-00596-5. Epub 2023 Oct 4 [PubMed PMID: 37792254]
Sarli WM, Quaranta F, Canessa C, Lodi L, Pisano L, Buccoliero AM, Oranges T, Sieni E, Simonini G, Bartolini L, Venturini E, Galli L, Azzari C, Ricci S. Uncovering hidden immune defects in childhood granulomatous disorders: a case report. Frontiers in immunology. 2025:16():1634661. doi: 10.3389/fimmu.2025.1634661. Epub 2025 Jul 18 [PubMed PMID: 40755768]
Level 3 (low-level) evidenceHettinga YM, Scheerlinck LM, Lilien MR, Rothova A, de Boer JH. The value of measuring urinary β2-microglobulin and serum creatinine for detecting tubulointerstitial nephritis and uveitis syndrome in young patients with uveitis. JAMA ophthalmology. 2015 Feb:133(2):140-5. doi: 10.1001/jamaophthalmol.2014.4301. Epub [PubMed PMID: 25356569]
Miller JM, Binnicker MJ, Campbell S, Carroll KC, Chapin KC, Gilligan PH, Gonzalez MD, Jerris RC, Kehl SC, Patel R, Pritt BS, Richter SS, Robinson-Dunn B, Schwartzman JD, Snyder JW, Telford S 3rd, Theel ES, Thomson RB Jr, Weinstein MP, Yao JD. A Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2018 Update by the Infectious Diseases Society of America and the American Society for Microbiology. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2018 Aug 31:67(6):e1-e94. doi: 10.1093/cid/ciy381. Epub [PubMed PMID: 29955859]
Pardo I, Finamor LPS, Marra PS, Ferreira JMG, Gutfreund MC, Hsieh MK, Li Y, Pinho JRR, Rizzo LV, Kobayashi T, Diekema DJ, Edmond MB, Bispo PJM, Marra AR. Metagenomic Next-Generation Sequencing for the Diagnosis of Infectious Uveitis: A Comprehensive Systematic Review. Viruses. 2025 May 26:17(6):. doi: 10.3390/v17060757. Epub 2025 May 26 [PubMed PMID: 40573347]
Level 1 (high-level) evidenceReiff A. Clinical Presentation, Management, and Long-Term Outcome of Pars Planitis, Panuveitis, and Vogt-Koyanagi-Harada Disease in Children and Adolescents. Arthritis care & research. 2020 Nov:72(11):1589-1596. doi: 10.1002/acr.24056. Epub [PubMed PMID: 31444859]
Mochizuki M, Smith JR, Takase H, Kaburaki T, Acharya NR, Rao NA, International Workshop on Ocular Sarcoidosis Study Group. Revised criteria of International Workshop on Ocular Sarcoidosis (IWOS) for the diagnosis of ocular sarcoidosis. The British journal of ophthalmology. 2019 Oct:103(10):1418-1422. doi: 10.1136/bjophthalmol-2018-313356. Epub 2019 Feb 23 [PubMed PMID: 30798264]
Clarke SLN, Maghsoudlou P, Guly CM, Dick AD, Ramanan AV. The management of adult and paediatric uveitis for rheumatologists. Nature reviews. Rheumatology. 2024 Dec:20(12):795-808. doi: 10.1038/s41584-024-01181-x. Epub 2024 Nov 6 [PubMed PMID: 39506056]
Kim L, Li A, Angeles-Han S, Yeh S, Shantha J. Update on the management of uveitis in children: an overview for the clinician. Expert review of ophthalmology. 2019:14(4-5):211-218. doi: 10.1080/17469899.2019.1663731. Epub 2019 Sep 19 [PubMed PMID: 32831897]
Level 3 (low-level) evidenceValdes LM, Sobrin L. Uveitis Therapy: The Corticosteroid Options. Drugs. 2020 Jun:80(8):765-773. doi: 10.1007/s40265-020-01314-y. Epub [PubMed PMID: 32350761]
Branford JA, Bodaghi B, Ferreira LB, McCluskey PJ, Thorne JE, Matthews JM, International Study Group for Systemic Immunomodulatory Drug Treatment of Non‐Infectious Uveitis, Smith JR. Use of immunomodulatory treatment for non-infectious uveitis: an International Ocular Inflammation Society report of real-world practice. The British journal of ophthalmology. 2025 Mar 20:109(4):482-489. doi: 10.1136/bjo-2024-326239. Epub 2025 Mar 20 [PubMed PMID: 39472042]
Edwards Mayhew RG, Li T, McCann P, Leslie L, Strong Caldwell A, Palestine AG. Non-biologic, steroid-sparing therapies for non-infectious intermediate, posterior, and panuveitis in adults. The Cochrane database of systematic reviews. 2022 Oct 31:10(10):CD014831. doi: 10.1002/14651858.CD014831.pub2. Epub 2022 Oct 31 [PubMed PMID: 36315029]
Level 1 (high-level) evidenceAgrawal R, Goh YY, Rojas-Carabali W, Cifuentes-González C, Sanjay S, Yu-Hor Thong B, de-la-Torre A, Samson CM, Biswas J, Finger RP, Kempen JH. Immunomodulatory therapy in non-infectious Uveitis: Current landscape, gaps, and future directions. Progress in retinal and eye research. 2025 Sep:108():101380. doi: 10.1016/j.preteyeres.2025.101380. Epub 2025 Jun 21 [PubMed PMID: 40550324]
Level 3 (low-level) evidenceEbrahimiadib N, Maleki A, Fadakar K, Manhapra A, Ghassemi F, Foster CS. Vascular abnormalities in uveitis. Survey of ophthalmology. 2021 Jul-Aug:66(4):653-667. doi: 10.1016/j.survophthal.2020.12.006. Epub 2021 Jan 5 [PubMed PMID: 33412171]
Level 3 (low-level) evidenceWong AM. Amblyopia (lazy eye) in children. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2014 Mar 4:186(4):292. doi: 10.1503/cmaj.130666. Epub 2013 Nov 4 [PubMed PMID: 24190990]
Kwok AK, Lam DS, Ng JS, Fan DS, Chew SJ, Tso MO. Ocular-hypertensive response to topical steroids in children. Ophthalmology. 1997 Dec:104(12):2112-6 [PubMed PMID: 9400772]
Level 1 (high-level) evidenceAllen DB, Mullen M, Mullen B. A meta-analysis of the effect of oral and inhaled corticosteroids on growth. The Journal of allergy and clinical immunology. 1994 Jun:93(6):967-76 [PubMed PMID: 8006318]
Level 1 (high-level) evidenceSchatz CS, Uzel JL, Leininger L, Danner S, Terzic J, Fischbach M. Immunosuppressants used in a steroid-sparing strategy for childhood uveitis. Journal of pediatric ophthalmology and strabismus. 2007 Jan-Feb:44(1):28-34. doi: 10.3928/01913913-20070101-03. Epub [PubMed PMID: 17274332]
Sangwan VS, Pearson PA, Paul H, Comstock TL. Use of the Fluocinolone Acetonide Intravitreal Implant for the Treatment of Noninfectious Posterior Uveitis: 3-Year Results of a Randomized Clinical Trial in a Predominantly Asian Population. Ophthalmology and therapy. 2015 Jun:4(1):1-19. doi: 10.1007/s40123-014-0027-6. Epub 2014 Dec 12 [PubMed PMID: 25502122]
Level 1 (high-level) evidenceBertin L, Savarino EV. JAK Inhibitors: A Double-Edged Sword in Immune-Mediated Diseases Management. United European gastroenterology journal. 2025 May:13(4):505-507. doi: 10.1002/ueg2.12716. Epub 2024 Nov 29 [PubMed PMID: 39611749]
Roy H. The red eye. Comprehensive therapy. 2006 Spring:32(1):43-6 [PubMed PMID: 16785582]
Bourcier T, Koestel E, Bertret C, Yaïci R, Borderie V, Bouheraoua N. [Bacterial keratitis: Retrospective and prospective 2024]. Journal francais d'ophtalmologie. 2024 Dec:47(10):104335. doi: 10.1016/j.jfo.2024.104335. Epub 2024 Oct 24 [PubMed PMID: 39454484]
Level 2 (mid-level) evidenceMurthy SI, Sabhapandit S, Balamurugan S, Subramaniam P, Sainz-de-la-Maza M, Agarwal M, Parvesio C. Scleritis: Differentiating infectious from non-infectious entities. Indian journal of ophthalmology. 2020 Sep:68(9):1818-1828. doi: 10.4103/ijo.IJO_2032_20. Epub [PubMed PMID: 32823398]
Sainz de la Maza M, Foster CS, Jabbur NS. Scleritis-associated uveitis. Ophthalmology. 1997 Jan:104(1):58-63 [PubMed PMID: 9022105]
Level 3 (low-level) evidenceThorne JE, Sugar EA, Holbrook JT, Burke AE, Altaweel MM, Vitale AT, Acharya NR, Kempen JH, Jabs DA, Multicenter Uveitis Steroid Treatment Trial Research Group. Periocular Triamcinolone vs. Intravitreal Triamcinolone vs. Intravitreal Dexamethasone Implant for the Treatment of Uveitic Macular Edema: The PeriOcular vs. INTravitreal corticosteroids for uveitic macular edema (POINT) Trial. Ophthalmology. 2019 Feb:126(2):283-295. doi: 10.1016/j.ophtha.2018.08.021. Epub 2018 Sep 27 [PubMed PMID: 30269924]
Muhaya M, Calder V, Towler HM, Shaer B, McLauchlan M, Lightman S. Characterization of T cells and cytokines in the aqueous humour (AH) in patients with Fuchs' heterochromic cyclitis (FHC) and idiopathic anterior uveitis (IAU). Clinical and experimental immunology. 1998 Jan:111(1):123-8 [PubMed PMID: 9472671]
Jones NP. Fuchs' heterochromic uveitis: an update. Survey of ophthalmology. 1993 Jan-Feb:37(4):253-72 [PubMed PMID: 8441952]
Level 3 (low-level) evidenceTripathy K, Salini B. Amsler Sign. StatPearls. 2026 Jan:(): [PubMed PMID: 30844165]
Nüssle S, Reinhard T, Lübke J. Acute Closed-Angle Glaucoma-an Ophthalmological Emergency. Deutsches Arzteblatt international. 2021 Nov 12:118(Forthcoming):771-80. doi: 10.3238/arztebl.m2021.0264. Epub 2021 Nov 12 [PubMed PMID: 34551857]
Simakurthy S, Tripathy K. Endophthalmitis. StatPearls. 2026 Jan:(): [PubMed PMID: 32644505]
Durand ML. Endophthalmitis. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2013 Mar:19(3):227-34. doi: 10.1111/1469-0691.12118. Epub [PubMed PMID: 23438028]
Lin ML, Hall AJ. Uveitis masquerade syndromes: An approach to diagnosis. Clinical & experimental ophthalmology. 2024 Jan-Feb:52(1):91-105. doi: 10.1111/ceo.14328. Epub 2023 Nov 23 [PubMed PMID: 37997019]
Multicenter Uveitis Steroid Treatment (MUST) Trial Research Group, Kempen JH, Altaweel MM, Drye LT, Holbrook JT, Jabs DA, Sugar EA, Thorne JE. Benefits of Systemic Anti-inflammatory Therapy versus Fluocinolone Acetonide Intraocular Implant for Intermediate Uveitis, Posterior Uveitis, and Panuveitis: Fifty-four-Month Results of the Multicenter Uveitis Steroid Treatment (MUST) Trial and Follow-up Study. Ophthalmology. 2015 Oct:122(10):1967-75. doi: 10.1016/j.ophtha.2015.06.042. Epub 2015 Aug 20 [PubMed PMID: 26298715]
Rathinam SR, Gonzales JA, Thundikandy R, Kanakath A, Murugan SB, Vedhanayaki R, Lim LL, Suhler EB, Al-Dhibi HA, Doan T, Keenan JD, Rao MM, Ebert CD, Nguyen HH, Kim E, Porco TC, Acharya NR, FAST Research Group. Effect of Corticosteroid-Sparing Treatment With Mycophenolate Mofetil vs Methotrexate on Inflammation in Patients With Uveitis: A Randomized Clinical Trial. JAMA. 2019 Sep 10:322(10):936-945. doi: 10.1001/jama.2019.12618. Epub [PubMed PMID: 31503307]
Level 1 (high-level) evidenceMulticenter Uveitis Steroid Treatment Trial (MUST) Research Group, Writing Committee:, Acharya NR, Vitale AT, Sugar EA, Holbrook JT, Burke AE, Thorne JE, Altaweel MM, Kempen JH, Jabs DA. Intravitreal Therapy for Uveitic Macular Edema-Ranibizumab versus Methotrexate versus the Dexamethasone Implant: The MERIT Trial Results. Ophthalmology. 2023 Sep:130(9):914-923. doi: 10.1016/j.ophtha.2023.04.011. Epub 2023 Jun 13 [PubMed PMID: 37318415]
Foster CS, Kothari S, Anesi SD, Vitale AT, Chu D, Metzinger JL, Cerón O. The Ocular Immunology and Uveitis Foundation preferred practice patterns of uveitis management. Survey of ophthalmology. 2016 Jan-Feb:61(1):1-17. doi: 10.1016/j.survophthal.2015.07.001. Epub 2015 Jul 9 [PubMed PMID: 26164736]
Level 3 (low-level) evidenceKempen JH, Van Natta ML, Altaweel MM, Dunn JP, Jabs DA, Lightman SL, Thorne JE, Holbrook JT, Multicenter Uveitis Steroid Treatment (MUST) Trial Research Group. Factors Predicting Visual Acuity Outcome in Intermediate, Posterior, and Panuveitis: The Multicenter Uveitis Steroid Treatment (MUST) Trial. American journal of ophthalmology. 2015 Dec:160(6):1133-1141.e9. doi: 10.1016/j.ajo.2015.09.017. Epub 2015 Sep 18 [PubMed PMID: 26386159]
Joubert M, Desbois AC, Domont F, Ghembaza A, Le Joncour A, Mirouse A, Maalouf G, Leclercq M, Touhami S, Cacoub P, Bodaghi B, Saadoun D. Behçet's Disease Uveitis. Journal of clinical medicine. 2023 May 24:12(11):. doi: 10.3390/jcm12113648. Epub 2023 May 24 [PubMed PMID: 37297843]
Tomkins-Netzer O, Talat L, Bar A, Lula A, Taylor SR, Joshi L, Lightman S. Long-term clinical outcome and causes of vision loss in patients with uveitis. Ophthalmology. 2014 Dec:121(12):2387-92. doi: 10.1016/j.ophtha.2014.07.007. Epub 2014 Aug 30 [PubMed PMID: 25178807]
Level 2 (mid-level) evidenceAremu TO, Oluwole OE, Adeyinka KO, Schommer JC. Medication Adherence and Compliance: Recipe for Improving Patient Outcomes. Pharmacy (Basel, Switzerland). 2022 Aug 28:10(5):. doi: 10.3390/pharmacy10050106. Epub 2022 Aug 28 [PubMed PMID: 36136839]
Religioni U, Barrios-Rodríguez R, Requena P, Borowska M, Ostrowski J. Enhancing Therapy Adherence: Impact on Clinical Outcomes, Healthcare Costs, and Patient Quality of Life. Medicina (Kaunas, Lithuania). 2025 Jan 17:61(1):. doi: 10.3390/medicina61010153. Epub 2025 Jan 17 [PubMed PMID: 39859135]
Level 2 (mid-level) evidence