Introduction
Approximately 4.9 million people worldwide have bilateral blindness secondary to corneal disease, accounting for 12% of total global blindness.[1][2] Common causes include anterior corneal pathologies such as trachoma, infectious keratitis, ocular trauma, and chemical injuries, with high prevalence in developing countries.[3] Advances in corneal transplantation have dramatically improved visual rehabilitation; in non-complex eyes, primary corneal transplantation, either lamellar or penetrating keratoplasty, demonstrates excellent outcomes, with reported graft survival rates of 87% to 93% at 1 year and 72% to 73% at 5 years.[4] However, graft survival declines significantly with repeat transplantation and in complex ocular surface disease, despite refinements in surgical technique and tissue selectivity.[5][6]
High-risk factors include recurrent or chronic ocular surface inflammation, glaucoma, and corneal vascularisation. Globally, the availability of donor corneal tissue can be limited by donor supply and the need for eye banking facilities. Modern lamellar corneal transplantation techniques aim to replace the non-functional or diseased part of the cornea. An artificial cornea transplant can be considered for end-stage corneal diseases such as multiple graft failures or inflammatory ocular surface disease.
Bioengineered corneal endothelial therapies aim to restore native corneal physiology by replacing or regenerating dysfunctional endothelium using cell-based constructs, biomimetic scaffolds, or synthetic membranes.[7] These approaches preserve the host cornea, maintain immune privilege, and integrate with established lamellar techniques such as DMEK (descemet membrane endothelial keratoplasty), offering the potential for lower complication rates and more physiological outcomes.[8][9] In contrast, traditional keratoprostheses were developed to address end-stage corneal blindness where grafting fails, relying on rigid artificial optics that bypass biological integration. Although keratoprostheses provide vision in severe cases, they are associated with significant long-term complications, including glaucoma, infection, extrusion, and lifelong surveillance.[10][11] Overall, bioengineered endothelial strategies represent a regenerative, tissue-preserving evolution, whereas keratoprostheses remain a salvage solution for complex corneal disease.
Numerous artificial corneal transplant devices have been proposed, including keratoprosthesis (KPro). Pellier de Quengsy first described the initial concept in 1789.[12] These devices generally have a central, clear optic with either hard skirt plates that sandwich donor corneal tissue or a soft optic and skirt in a one-piece integrated design. The importance of a suitable skirt material with good tissue incorporation was made clear from earlier models made from rubber, milk protein, Dacron, crystal, glass, and celluloid, which resulted in device extrusion after implantation.[4] The successful introduction of cadaveric corneal transplantation resulted in decreased interest in artificial corneal transplantation. However, the discovery of polymethylmethacrylate enabled the implantation of a biocompatible device, and earlier devices have been described by Choyce and Stone.[13][14]
More recently, soft polymers have been used to simulate the natural cornea. Poly-2-hydroxyethyl methacrylate was used for the AlphaCor, which gained FDA approval in 2003.[15] After 1 and 2 years, retention rates were 80% and 62%, respectively, and stromal melt occurred in 27% of cases, many of which required explantation.[15] A similar design using polytetrafluoroethylene (Legeais BioKPro-III) had worse outcomes, with 86% of devices failing after implantation.[16] This review focuses on the indications and management of the most commonly used artificial cornea transplants currently in practice—the Boston KPro type 1 and the osteo-odonto-Keratoprosthesis (OOKP).
Keratoprostheses
Boston keratoprosthesis type I: The Boston KPro type 1 is the most widely implanted artificial cornea. First introduced by Dohlman in 1965, the device was approved by the FDA in 1992.[17] The use of Boston KPro type 1 began to increase at the beginning of the 21st century, and to date, more than 19,000 devices have been implanted worldwide. The design consists of a front plate with a central optical stem, a backplate, and a corneal donor button sandwiched in between. The front plate and optic are made from polymethylmethacrylate, and the optical power is determined by the radius of curvature. Originally, the backplate was screwed into place; this was refined with a titanium locking ring in 2003 and a threadless stem in 2007.[17] The backplate is available in polymethylmethacrylate and titanium, both of which are well-tolerated biologically. No difference in the frequency of retroprosthetic membrane formation between the 2 materials was reported at 12 months.[18]
Osteo-odonto-keratoprosthesis: The OOKP uses an autologous tooth root-alveolar bone complex as the keratoprosthesis skirt material for better tissue integration. Originally invented by Strampelli and later modified by Falcinelli et al, the OOKP procedure involves bypassing the diseased ocular surface with a buccal mucous membrane patch and replacing the anterior segment structures with the OOKP.[19] The mucous membrane patch can tolerate dry environmental conditions and some level of inflammation. Good tissue integration ensures that OOKP can be retained for several decades.[20] Long-term anatomical retention of OOKP is favorable, with 81% reported retention rates of 81% over 5 years in 36 eyes, 98% over 20 years in 85 patients, and 80% over 18 years in 224 eyes.[19][21][22]
Keratoprostheses in Development
Several alternative keratoprostheses are currently in development.[23][24] Studies have found that 5-year survival, both for anatomical retention and functional recovery, was higher with the Boston type 1 KPro than with the Aurolab keratoprosthesis; however, these differences were not statistically significant.[25][26] Therefore, the Aurolab keratoprosthesis can be an alternative to the Boston type 1 KPro when affordability or availability is limited. The Lucia keratoprosthesis is a modified version of the Boston Type 1 KPro to improve affordability. [27] Machinist time was reduced by changing the locking interface between the front and backplates. Photoetching was used instead of using a lathe, and the round holes in the backplate were replaced with petaloid radial slits. Anodised titanium enabled colour changes to the backplate for improved cosmesis.
Several different keratoprostheses for eyes with defective blinking, dry eyes, or cicatrization are being evaluated. The Lux keratoprosthesis consists of a cone-shaped polymethylmethacrylate cylinder, a titanium sleeve, and a 7.8 mm titanium backplate. A donor cornea is double trephined, with a central trephination at 3 mm and a peripheral trephination at 7.5 mm. The polymethylmethacrylate cylinder is secured in the titanium sleeve and placed through the central 3 mm opening in the donor cornea. The backplate is secured and sutured into place in the host after the patient's cornea is removed, using interrupted nylon sutures. A mucous membrane graft is sutured over with an opening for the polymethylmethacrylate cylinder optic. Short-term results with good retention and functional outcomes have been reported.[23]
Improvements in skirt materials may further enhance the development of keratoprosthesis. The OOKP is at risk of bone resorption, and a synthetic substitute comprising a hydrogel composite of nano-crystalline hydroxyapatite–coated poly(lactic-co-glycolic acid) microspheres has been evaluated in laboratory studies. A graphene oxide titania-based biomaterial has been implanted in vivo in rabbit corneas without causing an immune or inflammatory reaction, suggesting potential as a novel skirt material for keratoprostheses.[28]
Eyes considered high-risk for graft failure commonly exhibit recurrent or chronic ocular surface inflammation, corneal neovascularization, glaucoma, limbal stem cell deficiency, or severe cicatrization. In addition, global donor corneal shortages and the dependence on well-developed eye banking infrastructure further limit access to conventional keratoplasty in many regions. Although modern lamellar techniques aim to selectively replace diseased corneal layers while preserving host tissue, these approaches may still fail in eyes with severe surface pathology or repeated immunologic rejection. In such end-stage corneal diseases, artificial corneal transplantation (keratoprosthesis) represents a critical alternative for visual rehabilitation.[29]
Parallel to the development of keratoprosthesis, bioengineered corneal endothelial therapies have emerged as a regenerative strategy to restore native corneal physiology. These strategies include cell-based endothelial replacement, biomimetic scaffolds, and synthetic membranes designed to integrate with host tissue while maintaining immune privilege. When combined with lamellar approaches such as DMEK, these therapies offer the potential for lower complication rates and more physiological outcomes. However, their applicability remains limited to eyes with relatively preserved corneal architecture and ocular surface stability. In contrast, keratoprostheses were specifically designed for end-stage corneal blindness, where biological integration is no longer feasible. While they can provide dramatic visual recovery, they are associated with substantial long-term risks, including glaucoma progression, infection, extrusion, and the need for lifelong surveillance. Thus, regenerative endothelial therapies represent an evolution toward tissue preservation, whereas keratoprostheses remain a salvage solution for the most complex corneal disease.[30]
The concept of artificial corneal transplantation dates back to Pellier de Quengsy in 1789, marking one of the earliest attempts to replace opaque corneal tissue with a synthetic optical substitute. Most keratoprostheses consist of a central transparent optic combined with a surrounding skirt that anchors the device to host tissue, either by sandwiching donor cornea or by direct tissue integration. Early devices fabricated from materials such as rubber, glass, crystal, milk protein, Dacron, and celluloid failed due to poor biocompatibility and high extrusion rates, underscoring the importance of selecting the skirt material. With the success of cadaveric corneal transplantation, interest in artificial corneas declined temporarily until the advent of polymethylmethacrylate enabled the development of more biocompatible devices, including early designs by Choyce and Stone.[31]
Subsequent innovations explored soft polymer optics to better simulate the natural cornea. Poly-2-hydroxyethyl methacrylate, used in the AlphaCor device (approved by the Food and Drug Administration (FDA) in 2003), demonstrated retention rates of 80% at 1 year and 62% at 2 years but was limited by stromal melt in 27% of cases, often necessitating explantation. Other designs, such as the Legeais BioKPro-III using polytetrafluoroethylene, showed even poorer outcomes, with failure rates as high as 86%.[15] As a result, contemporary practice has largely converged on two established devices—the Boston KPro type I and the OOKP.[32]
The Boston KPro type I, first introduced by Dohlman in 1965 and FDA approved in 1992, is currently the most widely implanted keratoprosthesis, with over 19,000 devices implanted worldwide. The modular design of Boston KPro type I—consisting of a polymethylmethacrylate front plate with optical stem, a backplate, and an intervening donor corneal button—has undergone iterative refinements, including the introduction of a titanium locking ring and a threadless stem to improve stability and reduce complications. Both polymethylmethacrylate and titanium backplates demonstrate good biocompatibility, with no significant difference in retroprosthetic membrane formation at 1 year.[7]
The OOKP represents a fundamentally different approach, using an autologous tooth root-alveolar bone complex as the skirt material to achieve superior tissue integration. Originally described by Strampelli and later refined by Falcinelli, the OOKP bypasses the diseased ocular surface using a buccal mucous membrane graft and replaces the anterior segment with a biologically integrated optical system. The ability of OOKP to tolerate severe dryness and inflammation has led to exceptional long-term retention, with reported anatomical survival rates of 80% to 98% over follow-up periods up to 20 years.[30]
Beyond these established devices, multiple keratoprostheses remain under development, including the Aurolab, Lucia, and Lux keratoprostheses, which aim to improve affordability, accessibility, and performance in resource-limited settings. Innovations in skirt materials, such as nano-crystalline hydroxyapatite–coated polymers and graphene oxide-titania composites, show promise in enhancing tissue integration while reducing inflammatory responses, potentially addressing longstanding limitations of keratoprosthesis design. Collectively, artificial corneal transplantation occupies a unique and indispensable role in modern corneal surgery, bridging the gap between regenerative approaches and irreversible corneal blindness. Continued refinement of device design, patient selection, and multidisciplinary postoperative care is essential to optimize outcomes in this challenging patient population.[1]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Classification of Keratoprostheses
Keratoprostheses can be classified based on design and method of fixation:
- Collar-stud keratoprostheses consist of 2 skirt plates that sandwich a donor corneal button between them. Examples include Boston KPro and Auralab KPro.
- Soft optic and skirt devices, typically made from polymers, are secured intracorneally within the stromal layers. Examples include Legeais, AlphaCor, and KeraKlear.
- Externally secured keratoprostheses are fixed to the external cornea and sclera and incorporate a central clear optical core. The OOKP is the primary example of this design.
Major Keratoprosthesis Types
Boston keratoprosthesis type I: Early Boston KPro models had a solid backplate, leading to higher rates of corneal melt at follow-up. This complication was due to reduced aqueous flow, reduced penetration of the donor carrier cornea tissue, and reduced nutrient delivery, leading to tissue necrosis, device extrusion or leakage, and endophthalmitis. Therefore, the backplate was modified to include holes, and the bandage contact lens was changed at regular intervals to prevent ocular surface desiccation during long-term prophylactic topical vancomycin administration. This increased biointegration of the KPro with the donor cornea reduces the rates of leakage of pathogenic microbes into the eye.
Osteo-odonto-Keratoprosthesis: Previously, porous and nonbiological KPro skirt materials have been trialed, including Teflon, ceramic, Dacron, polytetrafluoroethylene, hydrogel, and hydroxyapatite.[33] All of these had issues with longevity and tissue integration. The OOKP uses a tooth root-alveolar bone complex, originally described by Strampelli, as a biological substitute for the KPro skirt. Nowadays, the tibial bone is sometimes used as an alternative in patients with no teeth (edentulism). The modern-day OOKP is the modified type improved by Falcinelli et al and standardized in the Rome-Vienna protocol.[34] The patient's ocular surface is bypassed with a buccal mucosal membrane graft, and the anterior segment structures are replaced with an osteo-odonto-acrylic lamina. The buccal mucosal membrane can tolerate drying and some inflammation, and the alveo-dental lamina integrates with the ocular tissues and can last for several decades. The surgery is performed in stages by oral and ophthalmic surgeons.
Artificial corneal transplantation, commonly referred to as keratoprosthesis (KPro) implantation, is designed to restore optical clarity and visual function in eyes where conventional corneal grafting is unlikely to succeed. Unlike biological keratoplasty, which relies on donor tissue integration and host immune tolerance, keratoprostheses bypass or replace the native corneal anatomy using synthetic or composite constructs. A detailed understanding of normal corneal anatomy and physiology, and how these are altered or substituted by artificial devices, is essential for appropriate patient selection, surgical planning, and postoperative management.
Normal Corneal Anatomy: Functional Overview
The human cornea is a transparent, avascular, multilayered structure approximately 500 to 550 µm thick centrally and serves as the primary refractive surface of the eye. The cornea is composed of 5 principal layers:
- Corneal epithelium—A stratified squamous epithelium providing barrier protection, a smooth optical surface, and rapid regenerative capacity.
- Bowman's layer—An acellular collagenous layer contributing to corneal rigidity.
- Corneal stroma—Constituting nearly 90% of corneal thickness, composed of regularly arranged collagen lamellae and keratocytes, responsible for transparency and tensile strength.
- Descemet membrane—The basement membrane of the endothelium.
- Corneal endothelium—A monolayer of hexagonal cells essential for maintaining corneal deturgescence through active ion transport.
Physiologically, corneal transparency depends on stromal dehydration, precise collagen alignment, intact epithelial barrier function, and endothelial pump activity. Disruption of any of these components—through infection, inflammation, trauma, or immune-mediated damage—leads to corneal opacity and visual loss.[35]
Rationale for Artificial Corneal Replacement
In end-stage corneal disease, especially in eyes with severe ocular surface pathology, limbal stem cell deficiency, multiple graft failures, or chronic inflammation, normal corneal anatomy cannot be reliably restored. Artificial corneal transplantation is therefore designed to replace optical function while bypassing biological dependence on corneal epithelium, stroma, and endothelium. Rather than restoring corneal physiology in a regenerative manner, keratoprostheses substitute optical transparency mechanically, while relying on surrounding host tissues for structural support and device retention.[36]
Anatomy of Keratoprosthesis Devices
Although multiple designs exist, most keratoprostheses share common anatomical components:
Optical cylinder (central optic): The central optic serves as an artificial corneal window, providing a clear refractive pathway for light. The optic is typically made of polymethylmethacrylate or other optically inert polymers.
- The optic replaces the epithelium, stroma, and endothelium in the visual axis.
- Optical power is pre-calculated based on axial length and keratometry equivalents.
- Unlike the natural cornea, the optic does not remodel, hydrate, or heal.[37]
Front Plate: The front plate supports the optic and interfaces with the tear film or mucosal surface. In devices such as the Boston KPro, the front plate lies anterior to the donor corneal button and contributes to mechanical stability.
Back Plate: The back plate lies posterior to the donor corneal tissue and distributes pressure evenly across the graft-host interface. Common materials include polymethylmethacrylate or titanium, both of which are biocompatible and biodegradable.
Skirt or Supporting Structure: The skirt is the most critical anatomical component for long-term retention.
- In Boston KPro, the skirt function is performed by a donor corneal button that integrates with host tissue.
- In OOKP, the skirt consists of autologous tooth root and alveolar bone, offering exceptional biointegration.
- Emerging devices explore synthetic or bioactive skirts to promote vascularized tissue ingrowth.[29]
Physiology of Vision Through an Artificial Cornea
Artificial corneal transplantation fundamentally alters normal corneal physiology:
Optical transmission: Light passes directly through the rigid optic without dependence on corneal hydration, epithelial smoothness, or endothelial pump function. This design eliminates corneal edema as a cause of visual degradation but introduces optical challenges such as glare and reduced contrast sensitivity.[38]
Tear film and surface physiology: Normal tear film dynamics are disrupted. Many devices require lifelong bandage contact lens wear to protect peri-prosthetic tissue, maintain hydration, and reduce epithelial breakdown. In OOKP, the optic protrudes through a mucous membrane graft rather than a tear film–dependent ocular surface.[39]
Aqueous humor dynamics: The presence of a rigid optic alters anterior chamber anatomy and may interfere with aqueous outflow, contributing to the high incidence of secondary glaucoma following keratoprosthesis implantation. Unlike natural corneas, intraocular pressure (IOP) measurement becomes unreliable, necessitating indirect assessment methods.[40]
Immune privilege: Although the cornea is normally immunoprecipitated, keratoprostheses partially bypass immune-mediated graft rejection. However, the surrounding donor tissue or host interface remains vulnerable to inflammation, infection, and sterile melt.
Host-device integration and biological response: Successful artificial corneal transplantation depends on a delicate balance between mechanical stability and biological tolerance.
- Excessive inflammation leads to tissue necrosis and device extrusion.
- Inadequate integration predisposes to leakage and infection.
- Chronic exposure to synthetic materials increases the risk of biofilm formation.
Physiologically, the eye adapts to the prosthesis by encapsulating it in fibrous tissue, a process that must be carefully controlled to avoid obstruction of the visual axis or extrusion.[41]
Anatomical Differences Between Major Keratoprostheses
- Boston KPro type I preserves some elements of corneal anatomy via a donor button and requires a relatively stable ocular surface.
- OOKP completely bypasses corneal and conjunctival anatomy, replacing it with mucosal tissue and bone-based support, making it suitable for the most severe cicatrizing diseases.
Summary
Artificial corneal transplantation replaces the complex biological architecture of the cornea with a mechanical optical system, restoring vision in eyes otherwise deemed untreatable. Although it successfully substitutes corneal transparency and refractive function, it does not replicate normal corneal physiology, necessitating lifelong surveillance and multidisciplinary care. Understanding the altered anatomy and physiology underlying keratoprosthesis implantation is fundamental to optimizing outcomes and minimizing complications.[42]
Indications
Patients with severe corneal opacity who are bilaterally blind, where otherwise conventional corneal and stem cell transplantation fails, can be considered for an artificial corneal transplant in 1 eye if that eye has a reasonable retina optic disc. The degree of ocular surface scarring or keratinization and inflammation, any shortening of the fornices, baseline tear secretion, blink reflex, and lid abnormalities need to be assessed. These factors influence the surgical approach and the choice of keratoprosthesis.
Boston Keratoprosthesis Type I
Patients considered for KPro type I should have an adequate blink reflex and sufficient tear production, with a minimum Schirmer I test result of 5 mm. Any type of anterior segment pathology can be acceptable. However, the severity and type of posterior segment disease impact suitability and clinical outcomes. Examples include previous multiple failed grafts; corneal opacities with extensive vascularisation; certain conditions, such as aniridia, corneal dystrophies, and herpetic keratitis; and previous corneal infections. Patients must be able to apply and retain a soft contact lens if type I KPro is being considered.[27] Boston type II KPro may be suitable for patients who do not meet these criteria and are not suitable for OOKP due to poor dentition or edentulism.
Osteo-Odonto-Keratoprosthesis
Patients with dry eyes, defective blinking, eyelid abnormalities, keratinization, and ocular surface inflammatory disorders may be candidates for OOKP surgery. Indications include conditions such as Sjogren's syndrome, graft-versus-host disease, Stevens-Johnson syndrome, mucous membrane pemphigoid (stage 3 and 4), chemical burns, Lyell syndrome, and trachoma (stage C0 World Health Organization classification) with at least light perception vision.
Artificial corneal transplantation is primarily indicated in eyes with end-stage corneal blindness where conventional penetrating or lamellar keratoplasty is unlikely to succeed or has already failed. Unlike biological corneal transplantation, a keratoprosthesis bypasses host-dependent epithelial healing, endothelial function, and immune tolerance, making it a valuable option in complex ocular surface disease.[29]
The decision to proceed with a keratoprosthesis requires careful consideration of ocular surface integrity, inflammatory status, glaucoma control, posterior segment health, and patient compliance, as long-term success depends on meticulous postoperative care and surveillance.
Major Indications for Keratoprosthesis
Multiple failed corneal grafts: Repeated failure of penetrating keratoplasty remains the most common indication for artificial corneal transplantation. Each subsequent graft carries a progressively lower survival rate due to immune sensitization, corneal vascularization, and chronic inflammation. In eyes with 2 or more failed grafts, especially when vascularized host beds are present, keratoprosthesis offers a more predictable visual outcome.[43]
Severe ocular surface disease: Eyes with chronic ocular surface inflammation or cicatrization often lack the biological environment necessary for donor corneal survival. Examples include:
- Stevens-Johnson syndrome
- Toxic epidermal necrolysis
- Ocular cicatricial pemphigoid
- Severe chemical or thermal burns
In such conditions, epithelial instability, tear film deficiency, and limbal stem cell loss lead to inevitable graft failure, making keratoprosthesis—particularly OOKP—a preferred option.[44]
Limbal stem cell deficiency: Total or near-total limbal stem cell deficiency results in conjunctivalization of the cornea, persistent epithelial defects, and stromal scarring. Although limbal stem cell transplantation may be attempted in selected cases, advanced or bilateral limbal stem cell deficiency with stromal opacification often necessitates keratoprosthesis implantation.[45]
Severe corneal neovascularization: Dense, deep stromal neovascularization significantly increases the risk of immune rejection following traditional keratoplasty. Artificial corneal transplantation circumvents immune rejection mechanisms by eliminating donor endothelium and minimizing antigen exposure.[46]
Autoimmune and inflammatory keratopathies: Eyes with underlying autoimmune disease frequently exhibit persistent inflammation and poor wound healing. Keratoprosthesis is considered when inflammation is medically controlled, but structural corneal failure persists.[47]
Congenital or developmental corneal opacities: In rare cases, artificial corneal transplantation may be considered for congenital corneal opacity or anterior segment dysgenesis when standard keratoplasty is anatomically or biologically unfeasible, particularly in older children or adults.[48]
Infectious keratitis with structural sequelae: End-stage corneal scarring following severe infectious keratitis—especially fungal or acanthamoeba keratitis—may warrant keratoprosthesis if the eye is otherwise stable and infection-free.[49]
Specific device-based indications:
- Boston KPro type I: Eyes with adequate tear film, eyelid function, and relatively stable ocular surface.
- OOKP: Eyes with severe dry eye, cicatrization, and keratinized ocular surfaces where conventional devices fail.[40]
Table 1. Indications for Artificial Corneal Transplantation
|
Clinical Scenario |
Rationale for Keratoprosthesis |
Preferred Device |
|
Two or more failed corneal grafts |
High risk of further immune rejection |
Boston KPro type I |
|
Severe chemical/thermal burns |
Poor epithelial healing, limbal stem cell deficiency |
OOKP |
|
Stevens-Johnson syndrome/toxic epidermal necrolysis |
Extreme dry eye, cicatrization |
OOKP |
|
Ocular cicatricial pemphigoid |
Progressive conjunctival scarring |
OOKP |
|
Total limbal stem cell deficiency |
Conjunctivalization of the cornea |
Boston KPro/OOKP |
|
Dense corneal neovascularization |
Loss of immune privilege |
Boston KPro |
|
End-stage infectious corneal scarring |
Structural opacity with a stable posterior segment |
Boston KPro |
|
Congenital corneal opacity (selected cases) |
Failed or unsuitable keratoplasty |
Boston KPro |
Abbreviations: KPro, keratoprosthesis; OOKP, osteo-odonto-Keratoprosthesis.
Contraindications
Boston Keratoprosthesis Type I
Contraindications include the absence of a blink reflex; tear production; posterior segment pathologies, such as retinal detachment; vision worse than light perception; abnormal lid anatomy; and forniceal shortening with the inability to retain a soft contact lens. Patients with no light perception vision, phthisis bulbi, or who have unrealistic expectations are not suitable for either type I or type II KPros. Patients with lagophthalmos require an oculoplastic consultation to minimize exposure risks.[30]
Boston KPro implantation has previously been performed in pediatric patients due to perceived advantages over penetrating keratoplasty, including reduced rejection, rapid visual recovery (lack of postoperative suture-related astigmatism), and fewer examinations under anesthesia. However, recent experience has demonstrated high complication rates and progression to phthisis; hence, it is no longer recommended.[50][51]
Osteo-Odonto-Keratoprosthesis
Advanced glaucoma is considered a relative contraindication.[4] OOKP is contraindicated in patients younger than 18 due to their high bone turnover, as well as in eyes with no light perception or phthisis bulbi. Patients with a detached retina or other posterior segment pathology that results in low visual potential are contraindicated for an OOKP. Other relative contraindications include inability to complete the follow-up program andpoor mental health.
Artificial corneal transplantation, including keratoprosthesis implantation, is primarily indicated for end-stage corneal blindness where conventional keratoplasty is unlikely to succeed. However, careful patient selection is essential, as several ocular, systemic, and psychosocial factors can significantly compromise anatomical retention, visual outcomes, and long-term safety. Contraindications may be absolute or relative, depending on the severity of disease, availability of adjunctive procedures, and the ability to ensure rigorous lifelong follow-up.[29]
Ocular Contraindications
Severe and uncontrolled ocular surface inflammation remains one of the most important contraindications to artificial corneal transplantation. Active autoimmune cicatrizing disorders, such as uncontrolled ocular cicatricial pemphigoid or Stevens-Johnson syndrome without adequate surface stabilization, markedly increase the risk of extrusion, infection, and stromal melt. Profound limbal stem cell deficiency with severe dry eye and absent tear film further compromises epithelialization and device integration, particularly for Boston type I keratoprosthesis. Advanced posterior segment disease represents another major contraindication. Eyes with irreversible optic nerve damage, advanced glaucomatous optic neuropathy, end-stage retinal disease, or no light perception vision are unlikely to derive functional benefit despite successful keratoprosthesis retention. Similarly, uncontrolled glaucoma or eyes with poor potential for IOP monitoring and management pose significant long-term risks following artificial corneal transplantation.[52]
Systemic and Patient-Related Contraindications
Systemic conditions that impair wound healing or increase infection risk—such as uncontrolled diabetes mellitus, severe immunosuppression, or active systemic infections—may adversely affect postoperative outcomes. Poor patient compliance is a critical contraindication, as artificial corneal transplantation requires lifelong surveillance, continuous topical antibiotics, and strict adherence to follow-up schedules. Patients unable or unwilling to comply with long-term care are at increased risk of catastrophic complications, including endophthalmitis and device extrusion.[53]
Psychosocial and Environmental Factors
Limited access to specialized ophthalmic care and inability to attend frequent follow-up visits significantly reduce the safety profile of artificial corneal transplantation. Poor hygiene, high-risk occupational exposure, or unstable social circumstances may also influence candidacy. In such cases, alternative visual rehabilitation strategies should be considered.[54]
Procedure-Specific Considerations
Certain contraindications are device-specific. Boston KPro type I is relatively contraindicated in eyes with severe ocular surface dryness and lid abnormalities, whereas OOKP may be contraindicated in patients with inadequate dentition, severe maxillofacial disease, or inability to tolerate multi-stage surgery.[55]
Table 2. Contraindications to Artificial Corneal Transplantation
|
Category |
Contraindication |
Rationale |
|
Ocular (Absolute) |
No light perception vision |
No functional visual potential |
|
Advanced optic nerve or retinal disease |
Poor visual prognosis |
|
|
Uncontrolled glaucoma |
High risk of irreversible vision loss |
|
|
Ocular (Relative) |
Active ocular surface inflammation |
Risk of extrusion and melt |
|
Severe dry eye/limbal stem cell deficiency |
Poor epithelialization |
|
|
Active intraocular infection |
Risk of endophthalmitis |
|
|
Systemic |
Uncontrolled diabetes mellitus or immunosuppression |
Impaired healing, infection risk |
|
Active systemic infection |
Increased postoperative morbidity |
|
|
Patient-related |
Poor compliance |
Lifelong care mandatory |
|
Inability to attend follow-up |
High risk of late complications |
|
|
Procedure-specific |
Inadequate dentition (OOKP) |
Inability to construct osteodental lamina |
|
Severe lid abnormalities (Boston KPro type I) |
Exposure and device failure |
Abbreviations: KPro, keratoprosthesis; OOKP, osteo-odonto-Keratoprosthesis.
Key Clinical Pearl
Artificial corneal transplantation should only be undertaken when visual potential exists and when both ocular surface stability and lifelong postoperative surveillance can be assured.
Equipment
Boston Keratoprosthesis Type I
Required equipment includes cornea donor tissue, trephine, 9/10.0 nylon sutures, soft bandage contact lens, intraocular lens (if combining with lens removal), corneal graft surgical tray, oculoplastic surgical tray, vitrectomy tray, and glaucoma drainage device.[40]
Osteo-Odonto-Keratoprosthesis
Surgical requirements include a corneal graft surgical tray, cautery, bone saw retractors, diamond-coated flywheel, drill, optic cylinder, fliering ring, trephine, silk traction suture, and 10.0 nylon sutures.
Artificial corneal transplantation is a technically demanding procedure that requires specialized surgical instrumentation, implant-specific components, and long-term postoperative adjuncts. The equipment used spans preoperative assessment, intraoperative keratoprosthesis implantation, and postoperative monitoring and maintenance. Appropriate availability and familiarity with these tools are essential to ensure anatomical retention, visual rehabilitation, and the prevention of complications.[56]
Core Keratoprosthesis Components
The central equipment for artificial corneal transplantation is the keratoprosthesis device itself, which varies depending on the model used. The Boston KPro type I consists of a polymethylmethacrylate front plate with an optical stem, a donor corneal button, a backplate (polymethylmethacrylate or titanium), and a locking ring. The OOKP requires additional dental and maxillofacial surgical equipment for harvesting and shaping the osteodental lamina, as well as specialized storage and implantation tools.[57]
Standard Ophthalmic Surgical Instruments
Artificial corneal transplantation requires a full set of microsurgical corneal instruments, including trephines, corneal scissors, forceps, needle holders, and vitreoretinal instruments. Precision trephination of both donor and host cornea is critical for proper device alignment. In combined procedures, vitrectomy systems and glaucoma drainage device instrumentation may be required.[58]
Operating Microscope and Visualization Systems
A high-resolution operating microscope with coaxial illumination is mandatory for accurate device placement. Intraoperative anterior segment optical coherence tomography, when available, helps assess device alignment, corneal thickness, and posterior segment status during complex cases.[59]
Adjunctive Intraoperative Equipment
Additional equipment includes vitrectomy machines, endolaser probes, and glaucoma shunt systems, as many artificial corneal transplantation cases require combined posterior segment surgery or glaucoma management. Bandage contact lenses, typically large-diameter soft lenses, are essential for protecting the ocular surface during Boston KPro implantation.[60]
Postoperative and Long-Term Monitoring Equipment
Long-term success of artificial corneal transplantation depends on careful surveillance. Equipment such as tonometers adapted for keratoprosthesis eyes, B-scan ultrasonography, and posterior segment imaging systems is necessary to monitor IOP, retinal status, and device integrity. Continuous access to topical antibiotics and antifungals is also a critical component of postoperative equipment planning.[61]
Table 3. Equipment Required for Artificial Corneal Transplantation
|
Category |
Equipment |
Purpose |
|
Keratoprosthesis components |
Boston KPro type I (front plate, backplate, and locking ring) |
Artificial optical device |
|
Donor corneal button |
Structural support |
|
|
OOKP osteodental lamina |
Biological skirt for integration |
|
|
Surgical instruments |
Corneal trephines |
Host and donor corneal trephination |
|
Microsurgical forceps and scissors |
Tissue handling |
|
|
Needle holders and sutures (9-0 and 10-0 nylon) |
Device fixation |
|
|
Visualization |
Operating microscope |
High-precision surgery |
|
Anterior segment OCT (optional) |
Intraoperative assessment |
|
|
Adjunctive systems |
Vitrectomy machine |
Posterior segment management |
|
Endolaser system |
Retinal treatment |
|
|
Glaucoma drainage devices |
IOP control |
|
|
Ocular surface protection |
Large-diameter bandage contact lens |
Prevent desiccation and exposure |
|
Postoperative monitoring |
B-scan ultrasonography |
Posterior segment evaluation |
|
Specialized tonometry devices |
IOP monitoring |
|
|
Fundus imaging systems |
Retinal surveillance |
|
|
Pharmacologic adjuncts |
Topical antibiotics and antifungals |
Infection prophylaxis |
|
Lubricants and anti-inflammatory agents |
Surface protection |
Abbreviations: KPro, keratoprosthesis; OOKP, osteo-odonto-Keratoprosthesis; OCT, optical coherence tomography; IOP, intraocular pressure.
Key Clinical Point
Successful artificial corneal transplantation requires not only the keratoprosthesis device but also a comprehensive infrastructure of surgical, imaging, and postoperative monitoring equipment to ensure long-term visual and anatomical success.
Personnel
Ophthalmologists—including subspecialists in cornea and anterior segment, glaucoma, vitreoretinal, oculoplastics—oral-dental surgeons, anesthetists, clinicians, and clinical psychologists are essential for achieving optimum outcomes. Psychological and social support, along with access to hospital facilities for planned and emergency follow-up care, are necessary components of the service. The care pathway should also provide access to patient support groups and educational resources, such as leaflets or multimedia materials, to inform patients about the procedure and aftercare.[6]
Artificial corneal transplantation is a complex, high-risk ophthalmic procedure that requires a multidisciplinary and interprofessional team to achieve optimal anatomical retention, visual rehabilitation, and long-term patient safety. Unlike standard corneal transplantation, artificial corneal transplantation demands specialized surgical expertise, meticulous perioperative coordination, and lifelong postoperative surveillance, making the role of each team member critical.[29]
Core Surgical Team
The corneal surgeon with expertise in keratoprosthesis implantation leads the procedure and is responsible for patient selection, surgical planning, and intraoperative execution. In many cases, especially those with advanced ocular surface disease or glaucoma, collaboration with a vitreoretinal surgeon and glaucoma specialist is essential. For OOKP procedures, additional involvement of oral and maxillofacial surgeons and otolaryngologists is required for harvesting and preparing the osteodental lamina.[62]
Anesthesia and Perioperative Support
Artificial corneal transplantation procedures are typically lengthy and technically demanding, necessitating the expertise of an anesthesiologist experienced in ophthalmic and prolonged surgeries. Anesthesia teams must account for patient comorbidities; airway considerations, especially in OOKP; and perioperative pain management. Operating room nurses and technicians play a vital role in instrument handling, maintaining sterility, and coordinating specialized equipment.[63]
Postoperative and Long-Term Care Team
Postoperative care extends well beyond the operating room. Ophthalmic nurses and optometrists are integral in wound care, contact lens management, visual rehabilitation, and patient education. Low-vision rehabilitation specialists assist patients in maximizing functional vision outcomes, particularly in bilateral or end-stage disease. Long-term follow-up often requires coordination with infectious disease specialists for antimicrobial prophylaxis and ocular surface specialists for management of chronic inflammation or epithelial instability.[64]
Patient Education and Psychosocial Support
Given the lifelong commitment required after artificial corneal transplantation, counselors and rehabilitation therapists support patient adherence, expectation management, and quality-of-life optimization. Effective communication among all personnel ensures early detection of complications such as glaucoma, retroprosthetic membrane formation, infection, and device extrusion.[43]
Table 4. Core Personnel in Artificial Corneal Transplantation
|
Personnel |
Primary Role |
|
Corneal surgeon |
Patient selection and keratoprosthesis implantation |
|
Vitreoretinal surgeon |
Vitrectomy and retinal management |
|
Glaucoma specialist |
IOP control and glaucoma surgery |
|
Oral and maxillofacial surgeon (OOKP) |
Osteodental lamina harvesting |
|
Anesthesiologist |
Perioperative anesthesia and monitoring |
|
Operating room nurses |
Instrument handling and surgical support |
|
Surgical technicians |
Equipment preparation and maintenance |
Abbreviations: OOKP, osteo-odonto-Keratoprosthesis; IOP, intraocular pressure.
Table 5. Postoperative and Supportive Care Personnel
|
Personnel |
Responsibilities |
|
Ophthalmic nurse |
Postoperative care and medication administration |
|
Optometrist |
Visual rehabilitation and refraction |
|
Low-vision specialist |
Functional vision optimization |
|
Infectious disease specialist |
Antimicrobial prophylaxis and infection management |
|
Ocular surface specialist |
Chronic surface disease management |
|
Rehabilitation counselor |
Patient education and adherence |
Key Clinical Insight
The success of artificial corneal transplantation relies equally on coordinated multidisciplinary personnel and surgical technique, highlighting the importance of team-based care for achieving long-term visual outcomes.
Preparation
Boston KPro Type 1
Generally, patients have already received maximal medical and surgical management, and KPro type 1 surgery is the only option for vision preservation and improvement. Baseline best-corrected visual function should be documented, including evidence of glaucoma surgeries, previous corneal grafts, history of steroid response, and posterior segment disease. Biometry should be performed if open-sky cataract extraction is planned. Risk factors such as herpetic disease and active ocular surface inflammation should be optimized before surgery.[65]
Osteo-Odonto-Keratoprosthesis
During the preoperative assessment, baseline visual acuity of at least light perception in the eye is necessary to proceed to OOKP. Ultrasonography, A-scan biometry, and electrodiagnostics also help predict postoperative visual potential. IOP can be challenging to measure, and it may sometimes need to be recorded subjectively via digital estimation. A thorough ocular surface examination and documentation of dryness, along with assessment of the patient's oral health, are needed. Sometimes radiological imaging of the patient's teeth is necessary to choose a suitable donor tooth.
The patient is started on an antiseptic and antifungal mouthwash a day before stage I surgery. During this stage, a buccal mucosal membrane is harvested from the patient and grafted to the ocular surface bed. The prepared osteo-odonto-acrylic lamina is implanted into a subcutaneous pouch in the contralateral lower lid. Preparation for the second stage involves careful monitoring of mucosal complications, including thinning, ulceration, and infection, as well as infection or extrusion of the implanted lamina.[29]
Preparation for artificial corneal transplantation is a multistage, multidisciplinary process that begins well before the day of surgery and continues through meticulous intraoperative planning. Given the high-risk nature of keratoprosthesis implantation, appropriate preparation is critical to minimize complications such as infection, glaucoma progression, device extrusion, and retinal morbidity.
Preoperative Clinical Assessment
Comprehensive ocular evaluation is essential and includes assessment of visual potential, ocular surface stability, lid anatomy, tear film adequacy, IOP, and posterior segment status. B-scan ultrasonography is mandatory when media opacity precludes fundus visualization. Glaucoma evaluation—including gonioscopy, optic nerve assessment, and baseline imaging—is crucial, as glaucoma remains the leading cause of long-term vision loss after artificial corneal transplantation.[30]
Systemic Evaluation and Optimization
Patients often have systemic comorbidities such as autoimmune disease, diabetes mellitus, or connective tissue disorders that can adversely affect healing. Systemic conditions should be optimized in collaboration with internists, rheumatologists, or anesthesiologists. In OOKP candidates, dental and maxillofacial assessments are mandatory to evaluate tooth and alveolar bone suitability.[6]
Infection Control and Ocular Surface Preparation
Preoperative eradication of ocular surface infection and inflammation is mandatory. Management includes aggressive treatment of blepharitis, conjunctivitis, and chronic surface inflammation. Long-term topical antibiotics, lubricants, and anti-inflammatory agents are initiated well in advance. Patients should be counseled regarding lifelong prophylactic antibiotic use following artificial corneal transplantation.[66]
Surgical Planning and Device Selection
Selection of keratoprosthesis type (eg, Boston KPro type I and OOKP) is individualized based on ocular surface status, blink function, tear film, and prior surgical history. Device sizing, optical power calculation, backplate material, and contact lens planning are finalized preoperatively. Coordination with the eye bank is required if donor corneal tissue is used as a carrier.
Patient Counseling and Consent
Patients must receive detailed counseling regarding realistic visual expectations, lifelong follow-up, need for chronic medications, and risk of severe complications, including glaucoma, infection, retinal detachment, and device loss. Written informed consent should explicitly address the salvage nature of the procedure in many cases.[67]
Table 6. Preoperative Preparation Checklist for Artificial Corneal Transplantation
|
Domain |
Key Components |
|
Ocular assessment |
Visual acuity, slit-lamp examination, IOP, B-scan, and glaucoma evaluation |
|
Ocular surface |
Identification and treatment of infection or inflammation; lid hygiene |
|
Posterior segment |
Retinal status; vitrectomy planning |
|
Systemic workup |
Medical clearance; autoimmune screening |
|
Dental evaluation (OOKP) |
Tooth and alveolar bone assessment |
|
Device planning |
KPro type, size, optical power |
|
Patient counseling |
Expectations, risks, lifelong care |
Abbreviations: KPro, keratoprosthesis; OOKP, osteo-odonto-Keratoprosthesis; IOP, intraocular pressure.
Table 7. Medications and Interventions During Preparation
|
Category |
Purpose |
|
Topical antibiotics |
Reduce ocular surface microbial load |
|
Lubricants |
Improve epithelial health |
|
Topical steroids |
Control inflammation |
|
Antiglaucoma meds |
Optimize baseline IOP |
|
Systemic antibiotics |
Selected high-risk cases |
|
Immunosuppression |
Autoimmune or inflammatory disease |
Abbreviation: IOP, intraocular pressure.
Clinical Pearl
Meticulous preoperative preparation and patient selection are the most important determinants of long-term keratoprosthesis retention and visual success.
Technique or Treatment
Artificial corneal transplantation, commonly referred to as keratoprosthesis (KPro) surgery, is a salvage surgical intervention for patients with end-stage corneal blindness in whom conventional keratoplasty has failed or is unlikely to succeed. The goal of artificial corneal transplantation is to restore optical clarity and visual function by replacing the diseased cornea with a synthetic optical device while ensuring long-term anatomical stability and ocular surface integrity. The technique varies depending on the type of keratoprosthesis, most commonly Boston KPro type I and OOKP.
General Principles of Artificial Corneal Transplantation Surgery
Artificial corneal transplantation surgery is based on 3 core principles:
- Creation of a stable optical pathway using a transparent artificial optic
- Secure integration of the device with host tissues to prevent extrusion
- Control of inflammation, infection, and glaucoma postoperatively
Meticulous patient selection, preoperative optimization, and lifelong postoperative care are critical to success.[4]
Surgical Technique: Boston Keratoprosthesis Type I
Preoperative Preparation
- Preoperative evaluation includes a comprehensive ocular evaluation, including glaucoma assessment, posterior segment imaging, and ocular surface examination.
- Eyelid position, tear film stability, and inflammation must be optimized before surgery.
- Appropriate backplate size and optical power should be selected.
Key Surgical Steps
- Donor cornea preparation
- A donor corneal button is trephined, and a central hole is created to accommodate the KPro optic.
- Assembly of the device
- The polymethylmethacrylate optic is passed through the donor cornea and secured with a titanium or polymethylmethacrylate backplate.
- Host cornea trephination
- The diseased host cornea is excised, similar to penetrating keratoplasty.
- Implantation
- The assembled KPro-donor cornea complex is sutured into the host bed using interrupted or continuous nylon sutures.
- Adjunctive procedures
- Lens extraction or vitrectomy may be performed if required.
- Bandage contact lens placement
- A permanent bandage contact lens is applied to protect the ocular surface.[67]
Postoperative Management
Postoperative care includes:
- Lifelong topical antibiotics and steroids
- Regular glaucoma monitoring
- Surveillance for retroprosthetic membrane, infection, and melt
Boston Keratoprosthesis Type I
- Thickened corneal epithelium is removed to aid visualization.
- The corneal center is marked with gentian violet. An RK marker can be used to aid suture placement later.
- If a concurrent pars plana vitrectomy is planned, the ports can be pre-placed. A core anterior vitrectomy is generally performed in aphakic patients.
- In phakic patients, lens extraction is performed, with or without intraocular lens implantation.
- KPro is assembled before the patient's cornea is trephined. The donor cornea is trephined to a diameter of 8.5 to 9.0 mm. A central 3 mm hole is trephined on the donor corneal button. This step can be performed before the outer diameter punch is used. The front plate is placed face down. The donor button is placed over the front plate stem, with the backplate resting on the corneal endothelium. This construct is secured in place with the titanium locking ring.
- A paracentesis is made, and viscoelastic is injected into the anterior chamber. The patient's recipient cornea is trephinated. Typically, the diameter is 0.5 mm less than the donor cornea graft. At this point, any additional procedures are undertaken to improve visualization, eg, lens extraction, intraocular lens implantation/removal, open-sky anterior vitrectomy, and trimming of glaucoma drainage devices.
- The donor button with KPro is sutured with interrupted 10.0 nylon (9.0 nylon can also be used) and checked for integrity.
- A pars plana core vitrectomy is sometimes performed after suturing is complete, especially if there is posterior segment pathology, such as hemorrhage, retinal detachment, and epiretinal membrane. Long-term patients who have had combined pars plana core vitrectomy and KPro had fewer complications.[68]
- Intracameral antibiotics and a soft contact lens are placed at the end of the procedure.
Surgical Technique: Osteo-Odonto-Keratoprosthesis
OOKP is reserved for severe ocular surface disease, such as Stevens-Johnson syndrome and chemical burns.
Two-Stage Procedure
Stage 1
- Harvesting of the tooth-alveolar bone complex
- Placement of polymethylmethacrylate optic within the tooth lamina
- Buccal mucosal graft applied over the ocular surface
Stage 2
- Implantation of the osteo-odonto lamina into the eye
- Central optic exposed through the mucosa
Advantages
- Excellent long-term retention
- Superior tissue integration
- Suitable for dry and cicatrized eyes
Adjunctive and Supportive Treatments
- Glaucoma management (medical or surgical)
- Vitrectomy for posterior segment access
- Management of retroprosthetic membrane with YAG laser or surgery
- Systemic immunomodulation in selected inflammatory cases [29]
Osteo-Odonto-Keratoprosthesis
Stage I
- The mucous membrane covering needs to be harvested. A preoperative oral hygiene regimen is started after the decision to operate is taken. The removed mucous membrane graft is approximately 3 to 4 mm in diameter, covering the anterior surface of the globe to the recti muscle insertions. The parotid duct opening is preserved, and hemostasis and sutured closure of the graft site are performed.
- All remaining limbal stem cells, corneal epithelium, and Bowman's layer covering the globe must be removed. The conjunctiva is recessed up to the recti muscles with the use of minimal cautery. Tenon's capsule is used to cover a non-vascularised cornea.
- The mucous membrane graft is sutured onto the episclera with interrupted or running suture close to the recti insertions without overstretching.
- The tooth chosen should have the largest root. The gingiva is dissected, and the tooth with root and surrounding alveolar bone is harvested with a bone saw. The ideal size of the dentoalveolar lamina is 15 to 16 mm in length and at least 3 mm in thickness. The gingiva is removed, and extensive rinsing with povidone-iodine is performed to reduce bacterial contamination.
- A diamond-coated flywheel is used to remove half of the root. All tissues from the dental pulp canal are also removed.
- An opening for the optic cylinder is drilled in the dentine at a perpendicular angle, ideally centered or where there is more bone tissue.
- The optic cylinder power is calculated (50-60 diopters for an aphakic eye) and cemented into the opening after the dentine is dried with oxygen.
- The tooth crown is removed, and the osteoodontoacrylic lamina implant is inserted into a subcutaneous pouch for 3 months to aid revascularisation and growth of connective tissues, typically in the orbitozygomatic area inferior to the lower lid of the contralateral eye.[69]
Stage II
- The osteoodontoacrylic lamina is explanted from the subcutaneous pouch and assessed for integrity and bone absorption.
- The connective tissue is removed from the dentine surface, which makes contact with the corneal surface.
- The mucous membrane graft is partially lifted off the anterior globe, and a flap is fashioned, with the inferior limbus base attached to retain the blood supply.
- A Flieringa ring is sutured to the sclera with traction sutures at 3 and 9 o'clock, pre-placed to lift the ring at the time of lamina insertion.
- The center of the cornea is trephined to the same diameter as the posterior optical cylinder. Decentration here can cause a visual field decentration.
- Removal of the iris, lens, and anterior vitreous is necessary to avoid postoperative secondary glaucoma or severe inflammatory membranes.
- Pre-placed sutures around the prosthesis are positioned before inserting the optical cylinder into the cornea, with the dentine surface facing the cornea. Air is injected into the globe through a 30-G needle for inflation. Interrupted sutures fix the prosthesis to the corneoscleral surface.
- More sterile air is injected to seal the cornea trephination. The patient should lie on their back for 4 to 5 days after the operation.
- The buccal mucosa flap is replaced to cover the lamina after central trephination, thereby exposing the optical cylinder.
- Lifelong topical antibiotic therapy and aseptic sterile cleaning of the optical cylinder are advised. Eye ointment should be used if there is lagophthalmos present. A scleral shield can be worn to reduce dehydration and for improved cosmesis.[34]
Table 8. Summary of Artificial Corneal Transplantation Techniques
|
Aspect |
Boston KPro Type I |
OOKP |
|
Indication |
Failed grafts, wet ocular surface |
Severe dry/cicatrized surface |
|
Surgical stages |
Single-stage |
Two-stage |
|
Skirt material |
Donor cornea |
Autologous tooth-bone |
|
Retention |
Good (with surveillance) |
Excellent (long-term) |
|
Technical complexity |
Moderate |
High |
|
Follow-up |
Lifelong |
Lifelong |
Abbreviations: KPro, keratoprosthesis; OOKP, osteo-odonto-keratoprosthesis.
Key Takeaways
- Artificial corneal transplantation is a vision-restoring but high-maintenance procedure.
- Surgical success depends on technique, device selection, and postoperative vigilance.
- Boston KPro is most commonly used, whereas OOKP remains the gold standard for extreme ocular surface disease.
- Artificial corneal transplantation should be performed in specialized tertiary centers with multidisciplinary expertise.
Complications
Complications can arise from failure of the KPro to biocolonise (non-epithelization) and biointegrate (corneal melt around the optic). Ongoing inflammation in the anterior chamber and the formation of retroprosthetic membranes are common complications. Corneal melt can lead to leakage and endophthalmitis, which can be repaired with corneal regrafting and autologous cartilage.[70] Higher-risk eyes are those affected by underlying autoimmune conditions. In the United States, the incidence of endophthalmitis with the Boston keratoprosthesis ranges from 1% to 12.5%, whereas internationally it can reach 17%.[71] This condition can lead to complete vision loss.
After successful artificial corneal transplantation (all types), glaucoma is the most common complication and can even affect the eyes during late follow-up. High preoperative intraocular pressure and autoimmune diseases, such as mucous membrane pemphigoid and Stevens-Johnson syndrome, lead to a higher risk for glaucoma development and progression. In a recent single-center study of 140 eyes following Boston KPro type I implantation, 24% of eyes developed de novo glaucoma postoperatively.[72] Long-term monitoring for glaucoma development and progression is challenging due to the gross anatomical changes. Anterior segment optical coherence tomography can detect changes associated with glaucoma, such as angle narrowing, and, if the patient has reasonable vision, standard visual field testing can still be performed.[73][74] Several studies have shown that implanting glaucoma drainage devices before or at the time of KPro surgery reduces the risk of glaucoma progression.[75][76]
Combined KPro-vitrectomy eyes show a lower incidence of retroprosthetic membrane formation and more stable long-term vision than non-vitrectomised eyes.[77] Incidents of corneal melt, endophthalmitis, and glaucoma requiring surgical intervention increase with follow-up time, and there is a paucity of published data on medium- to long-term outcomes.[78] Complete repeat KPro appears to offer a reduced risk of recurrent melt for the Boston KPro, with localized repair a temporizing measure, and is the only option in cases of device extrusion or severe infection.[79]
The OOKP is fully biocompatible when using the patient's tooth; however, significant complications may still occur. These complications include oral (buccal mucosa harvesting), oculoplastic, secondary glaucoma, posterior segment, and device extrusion. Vitreoretinal complications include retinal detachment, vitritis, retroprosthetic membrane, vitreous hemorrhage, choroidal detachment, and endophthalmitis.[80][81] Primary vitrectomy during OOKP surgery is sometimes performed to reduce these complications. Mucosal melt and ulceration can lead to exposure of the lamina, necessitating repair with mucosal grafting. Poor oral health and buccal mucosa scarring increase the risk of mucosal ulcers and thinning. Laminar resorption can occur in the setting of anatomical failure and is more pronounced in allografts. Detection is achieved through clinical examination and confirmed with CT imaging.[82] Patients with Stevens-Johnson syndrome are at increased risk of laminar resorption.[83]
Artificial corneal transplantation, although vision-restoring in end-stage corneal disease, is associated with a distinct, often higher, complication profile compared to conventional keratoplasty. Complications may be early or late, ocular or device-related, and typically require lifelong surveillance and multidisciplinary management. Many complications are interrelated and may significantly impact long-term visual and anatomical outcomes if not detected early.
The most clinically significant complications include glaucoma progression, retroprosthetic membrane formation, infectious keratitis or endophthalmitis, sterile corneal melt, and device extrusion. Artificial corneal transplantation alters normal ocular anatomy and physiology, including aqueous dynamics, ocular surface defense mechanisms, and immune privilege, predisposing patients to these events. Visual rehabilitation may also be limited by posterior segment complications such as retinal detachment, cystoid macular edema, or optic nerve damage. Long-term success of artificial corneal transplantation depends not only on surgical technique but also on strict adherence to prophylactic medications, regular follow-up, and prompt intervention when complications arise.
Table 9. Complications of Artificial Corneal Transplantation
|
Category |
Complication |
Description/Mechanism |
Clinical Impact |
|
Anterior segment |
Retroprosthetic membrane |
Fibrocellular proliferation behind the optic due to inflammation |
Reduced vision may require a YAG laser or surgery |
|
Sterile corneal melt |
Enzymatic stromal degradation around the device |
Risk of extrusion and vision loss |
|
|
Infectious keratitis |
Compromised ocular surface defenses |
May progress to endophthalmitis |
|
|
Epithelial defects |
Poor tear film, exposure, and reduced healing |
Infection risk and discomfort |
|
|
Device-related |
Device extrusion |
Progressive tissue loss or infection |
Catastrophic failure and globe loss |
|
Device tilt or malposition |
Improper alignment or tissue instability |
Optical distortion and vision loss |
|
|
Backplate exposure |
Thinning or necrosis of the surrounding tissue |
Infection and extrusion risk |
|
|
Posterior segment |
Glaucoma/glaucoma progression |
Altered aqueous outflow and steroid response |
Leading cause of irreversible vision loss |
|
Retinal detachment |
Vitreoretinal traction or inflammation |
Severe visual morbidity |
|
|
Cystoid macular edema |
Chronic inflammation |
Reduced central vision |
|
|
Infectious |
Endophthalmitis |
Direct microbial entry or surface colonization |
Vision-threatening emergency |
|
Optic nerve |
Optic atrophy |
Chronic elevated IOP or inflammation |
Permanent visual loss |
|
Systemic/long-term |
Lifelong medication dependence |
Continuous antibiotic and steroid use |
Adherence challenges and toxicity |
|
Need for repeat interventions |
Retroprosthetic membrane removal, glaucoma surgery, and revision artificial corneal transplantation |
Increased morbidity and cost |
Key Clinical Pearls
- Glaucoma is the most common cause of late vision loss after artificial corneal transplantation and is often difficult to detect due to unreliable IOP measurements.
- Retroprosthetic membrane formation is common and should be anticipated rather than viewed as a failure.
- Infection risk persists lifelong, necessitating continuous topical antibiotic prophylaxis.
- Successful artificial corneal transplantation requires patient selection, education, and rigorous long-term follow-up.
Clinical Significance
Corneal opacities are one of the leading causes of worldwide blindness, along with cataracts, glaucoma, and macular degeneration. Access to corneal transplantation varies worldwide and is limited by a lack of infrastructure and donor tissue supply.[84][85][86] Advances in keratoprosthesis design have led to the development of more stable and biocompatible artificial corneal devices. To date, there is no equivalence between conventional corneal and artificial cornea keratoprosthesis transplantation. Keratoprostheses remain a viable option for patients where conventional cornea transplantation is not possible in the context of scarring and vascularisation.[85]
The increasing number of newer artificial corneal keratoprostheses requires adequate study and evaluation. Recent guidelines on consensus and reporting standards across all groups researching artificial cornea devices have been developed to improve data collection and comparative analysis.[87] Considering factors such as preoperative ocular surface status, eyelid anatomy, presence of systemic or autoimmune disease, and patient-related socioeconomic limitations can aid in decision-making.[40]
Artificial corneal transplantation, commonly performed using keratoprosthesis devices, represents a vision-restoring intervention of critical clinical importance for patients with end-stage corneal blindness who are poor candidates for conventional keratoplasty. Artificial corneal transplantation is particularly significant in eyes with multiple graft failures, severe ocular surface disease, limbal stem cell deficiency, chemical injuries, autoimmune cicatrizing disorders, or extensive corneal vascularization—scenarios in which standard corneal transplantation has unacceptably low success rates.[29]
From a clinical standpoint, artificial corneal transplantation bypasses host corneal pathology and provides a clear optical pathway, often resulting in rapid and meaningful visual rehabilitation in otherwise untreatable eyes. In many patients, it restores ambulatory vision, improves independence, and significantly enhances quality of life. The procedure has transformed the management paradigm of complex corneal disease, shifting the goal from palliative care to functional visual restoration.[88]
Artificial corneal transplantation also has importance as a salvage procedure, preserving vision and preventing progression to phthisis bulbi or enucleation in severely diseased eyes. Long-term data, particularly with Boston KPro type I and OOKP, demonstrate durable anatomical retention and sustained visual benefit when patients are carefully selected and closely monitored.[89]
However, the clinical significance of artificial corneal transplantation extends beyond visual outcomes alone. The procedure requires lifelong surveillance, interdisciplinary care, and meticulous management of complications, including glaucoma, infection, retroprosthetic membrane formation, and device extrusion. Thus, artificial corneal transplantation underscores the importance of comprehensive patient counseling, adherence to follow-up, and coordinated interprofessional care.[57]
Enhancing Healthcare Team Outcomes
Artificial corneal transplantation with keratoprostheses is a complex, multi-stage procedure that requires expertise, multidisciplinary teams, and resources. The ophthalmologist serves as the primary point of patient assessment, evaluating surgical suitability, identifying risk factors that may influence outcomes, and providing detailed counseling to the patient and family. When assessing suitability for OOKP, consultation with an oral and maxillofacial surgeon is essential. Clinicians can assess the patient's general systemic health. Clinical psychologists can investigate for psychological morbidity, the patient's coping mechanisms, expectations, adaptation to blindness, and the availability of social support in place. Ophthalmology specialty nurses can assist with the procedure and postoperative care. Such interprofessional team coordination contributes to improved outcomes from this procedure.[4]
Artificial corneal transplantation is a complex, high-risk, vision-restorative procedure that demands robust interprofessional collaboration to optimize patient outcomes, minimize complications, and ensure long-term device retention. Effective healthcare team performance hinges on clearly defined roles, advanced clinical skills, ethical practice, structured communication, and coordinated longitudinal care.
Clinician and Advanced Practitioner Roles
Corneal surgeons lead patient selection, surgical execution, and long-term clinical oversight, applying evidence-based criteria to identify appropriate candidates and manage complications such as infection, glaucoma, retroprosthetic membrane formation, and device extrusion. Advanced practitioners support perioperative assessment, continuity of care, and early detection of complications, ensuring adherence to standardized follow-up protocols. Subspecialist collaboration with glaucoma and retina specialists is essential for proactive surveillance and timely intervention in posterior segment or intraocular pressure–related complications.[90]
Nursing Contributions
Ophthalmic nurses play a critical role in patient-centered care delivery, emphasizing medication adherence, ocular surface care, and early recognition of adverse events. Nursing responsibilities include postoperative monitoring, reinforcement of infection-prevention strategies, contact lens maintenance, and patient education regarding warning symptoms that require urgent evaluation. Nurses also facilitate communication between patients and the broader care team, improving responsiveness and safety.
Pharmacist Responsibilities
Clinical pharmacists enhance outcomes through medication optimization and antimicrobial stewardship, particularly in patients requiring lifelong topical antibiotics and adjunctive systemic therapy. Pharmacists assess drug interactions, counsel patients on correct administration techniques, and monitor for medication-related toxicity, thereby improving adherence and reducing preventable adverse events.[91]
Allied Health and Rehabilitation Professionals
Optometrists and low-vision specialists focus on functional rehabilitation, visual optimization, and quality-of-life enhancement. Their involvement ensures realistic visual expectations, appropriate visual aids, and adaptation strategies for patients with partial visual recovery. Social workers and rehabilitation counselors address psychosocial challenges, access to care, and long-term compliance with follow-up schedules.
Interprofessional Communication and Ethics
Structured interprofessional communication—using shared documentation, standardized protocols, and regular case reviews—reduces care fragmentation and enhances patient safety. Ethical responsibilities include informed consent, realistic counseling regarding risks and lifelong surveillance, and equitable access to advanced corneal care. Transparent communication fosters trust, shared decision-making, and sustained patient engagement.
Outcome Optimization
By integrating surgical expertise, vigilant nursing care, pharmacologic oversight, rehabilitative support, and ethical coordination, the interprofessional healthcare team improves anatomical retention, visual outcomes, patient satisfaction, and overall safety in artificial corneal transplantation.[92]
Nursing, Allied Health, and Interprofessional Team Interventions
Artificial corneal transplantation requires coordinated, protocol-driven interventions by an interprofessional healthcare team to reduce morbidity, preserve vision, and ensure long-term device retention. Given the chronic nature of care following keratoprosthesis implantation, team-based interventions extend from the perioperative period through lifelong follow-up.[93]
Nursing Interventions
Ophthalmic nurses are central to perioperative care, patient education, and longitudinal monitoring. Preoperatively, nurses verify surgical readiness, reinforce ocular hygiene, ensure proper administration of preoperative antibiotics, and educate patients regarding postoperative expectations. Postoperatively, nursing interventions focus on wound assessment, contact lens positioning, medication adherence, and early detection of complications, including infection, inflammation, device instability, or increased ocular discomfort. Nurses also serve as the first point of contact for patients reporting visual changes or ocular symptoms, facilitating timely referral to the surgical team.[94]
Allied Health Interventions
Optometrists and vision care specialists contribute significantly to functional rehabilitation and surface maintenance. Their interventions include visual acuity monitoring, refractive assessment when applicable, therapeutic contact lens fitting, and evaluation of optic clarity. Low-vision specialists provide adaptive strategies and visual aids to enhance the quality of life, particularly in patients with limited visual recovery or bilateral disease.[62]
Clinician-Led Interprofessional Interventions
Corneal surgeons oversee surgical planning, postoperative management, and the mitigation of complications. Glaucoma specialists implement proactive intraocular pressure control strategies, recognizing the limitations of conventional tonometry in keratoprosthesis eyes. Retina specialists intervene early for posterior segment complications, including retinal detachment, vitreous opacities, or endophthalmitis, using B-scan ultrasonography and targeted interventions.[95]
Pharmacist-Driven Interventions
Clinical pharmacists optimize medication safety and adherence, particularly for lifelong topical antibiotic prophylaxis and systemic immunosuppressive therapy when indicated. Pharmacists identify drug interactions, counsel patients on correct dosing schedules, and support antimicrobial stewardship to reduce resistance and toxicity.[96]
Psychosocial and Rehabilitation Interventions
Social workers and rehabilitation professionals address barriers to care, including access to medications, transportation for frequent follow-up, and psychosocial stress related to chronic ocular disease. Counseling and vision rehabilitation services support patient adaptation and adherence to long-term care plans.[92]
Key Interprofessional Intervention Principle
Timely, coordinated interventions across nursing, allied health, and clinician teams are essential to prevent complications, optimize visual outcomes, and ensure durable success following artificial corneal transplantation.[97]
Nursing, Allied Health, and Interprofessional Team Monitoring
Artificial corneal transplantation requires lifelong, structured monitoring by an interprofessional healthcare team due to the high risk of vision-threatening complications such as infection, glaucoma, retroprosthetic membrane formation, retinal detachment, and device extrusion. Effective collaboration among ophthalmologists, nurses, optometrists, pharmacists, and allied health professionals is essential to ensure patient safety, optimize outcomes, and maintain long-term device retention.[98]
Nursing Monitoring and Responsibilities
Ophthalmic nurses play a central role in perioperative and long-term surveillance. Preoperatively, nurses reinforce ocular hygiene, medication adherence, and patient education. Postoperatively, they monitor for early warning signs, including ocular pain, redness, discharge, contact lens displacement, or sudden visual decline. Nurses ensure correct administration of topical antibiotics, steroids, and lubricants, and assess compliance with lifelong prophylactic regimens. Prompt escalation of abnormal findings to the surgical team is critical.[31]
Optometrists and Vision Care Specialists
Optometrists are integral to long-term visual rehabilitation and surveillance, particularly for patients with Boston KPro type I. Their responsibilities include visual acuity monitoring, refraction when applicable, contact lens fitting and maintenance, and early detection of surface complications or device instability. Regular assessment of optic clarity and functional vision aids early identification of retroprosthetic membrane formation.[99]
Glaucoma and Retina Team Monitoring
Given the high incidence of glaucoma progression after artificial corneal transplantation, glaucoma specialists monitor intraocular pressure using alternative techniques, such as digital palpation and transpalpebral tonometry, and manage medical or surgical intervention as needed. Retina specialists perform serial posterior segment evaluations using B-scan ultrasonography and fundus examination when feasible to detect retinal detachment, vitreoretinal traction, or endophthalmitis.[100]
Pharmacist and Medication Oversight
Clinical pharmacists support medication reconciliation, counsel patients on long-term antibiotic prophylaxis, identify drug interactions, particularly with systemic immunosuppressants, and reinforce adherence. Their involvement is especially valuable in complex cases requiring systemic therapy.
Allied Health and Psychosocial Support
Low-vision therapists, rehabilitation specialists, and counselors assist patients in adapting to visual limitations and the psychological burden of chronic ocular disease. Social workers facilitate access to medications, follow-up care, and transportation, particularly for patients requiring lifelong surveillance.[101]
Table 10. Interprofessional Team Roles in Artificial Corneal Transplantation Monitoring
|
Team Member |
Key Monitoring Responsibilities |
|
Ophthalmic nurse |
Medication adherence, surface assessment, and early complication detection |
|
Optometrist |
Visual acuity monitoring, contact lens care, and optic clarity |
|
Glaucoma specialist |
IOP control and glaucoma progression |
|
Retina specialist |
Posterior segment surveillance |
|
Pharmacist |
Medication safety, adherence, and interactions |
|
Allied health professional |
Vision rehabilitation and psychosocial support |
Abbreviation: IOP, intraocular pressure.
Key Interprofessional Principle
Early recognition of complications and seamless communication among team members are the cornerstones of long-term success following artificial corneal transplantation.
Media
(Click Image to Enlarge)
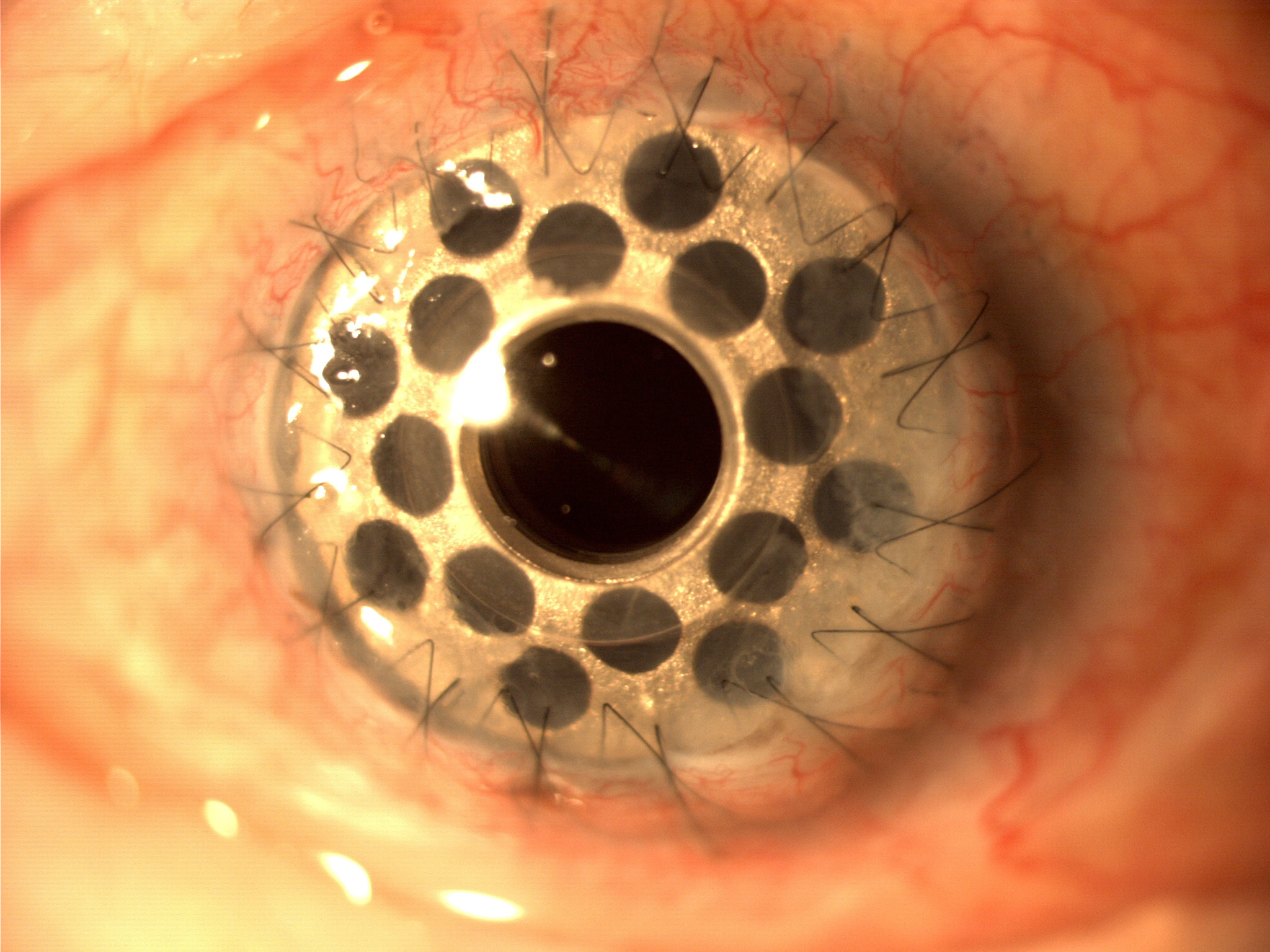
Boston KPro Type 1 with titanium posterior plate. Contributed by Wikimedia User: Mariagessa (CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0/deed.en)
(Click Image to Enlarge)
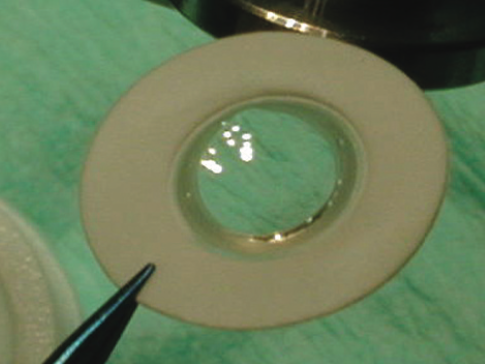
Example of a soft KPro (Legeais BioKPro-III) Contributed with Permission from Emma J Hollick, BM, BA, BCH (HONS OXON), MD
(Click Image to Enlarge)
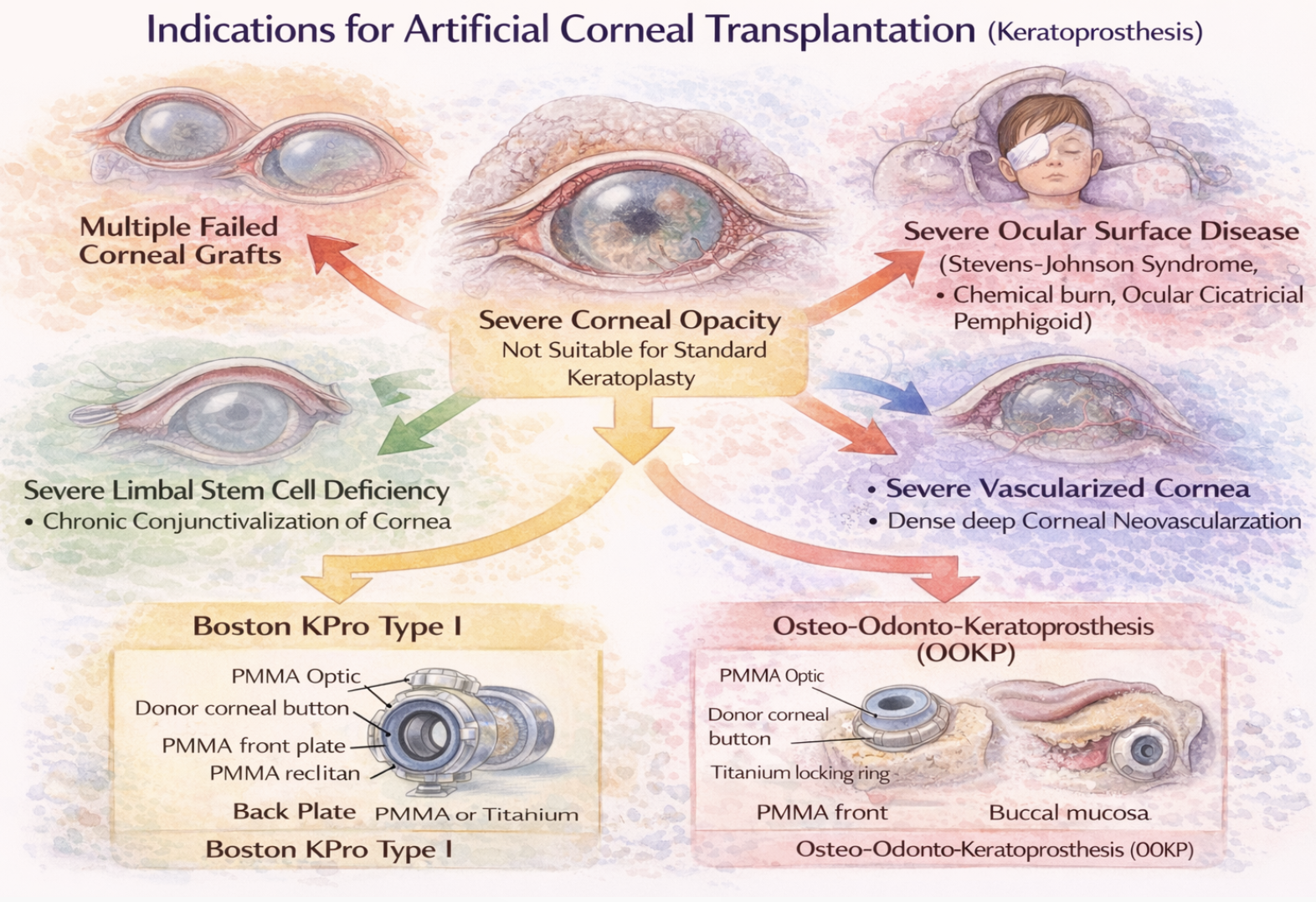
Schematic diagram depicting indications for artificial corneal transplantation
Bharat Gurnani, MD
(Click Image to Enlarge)
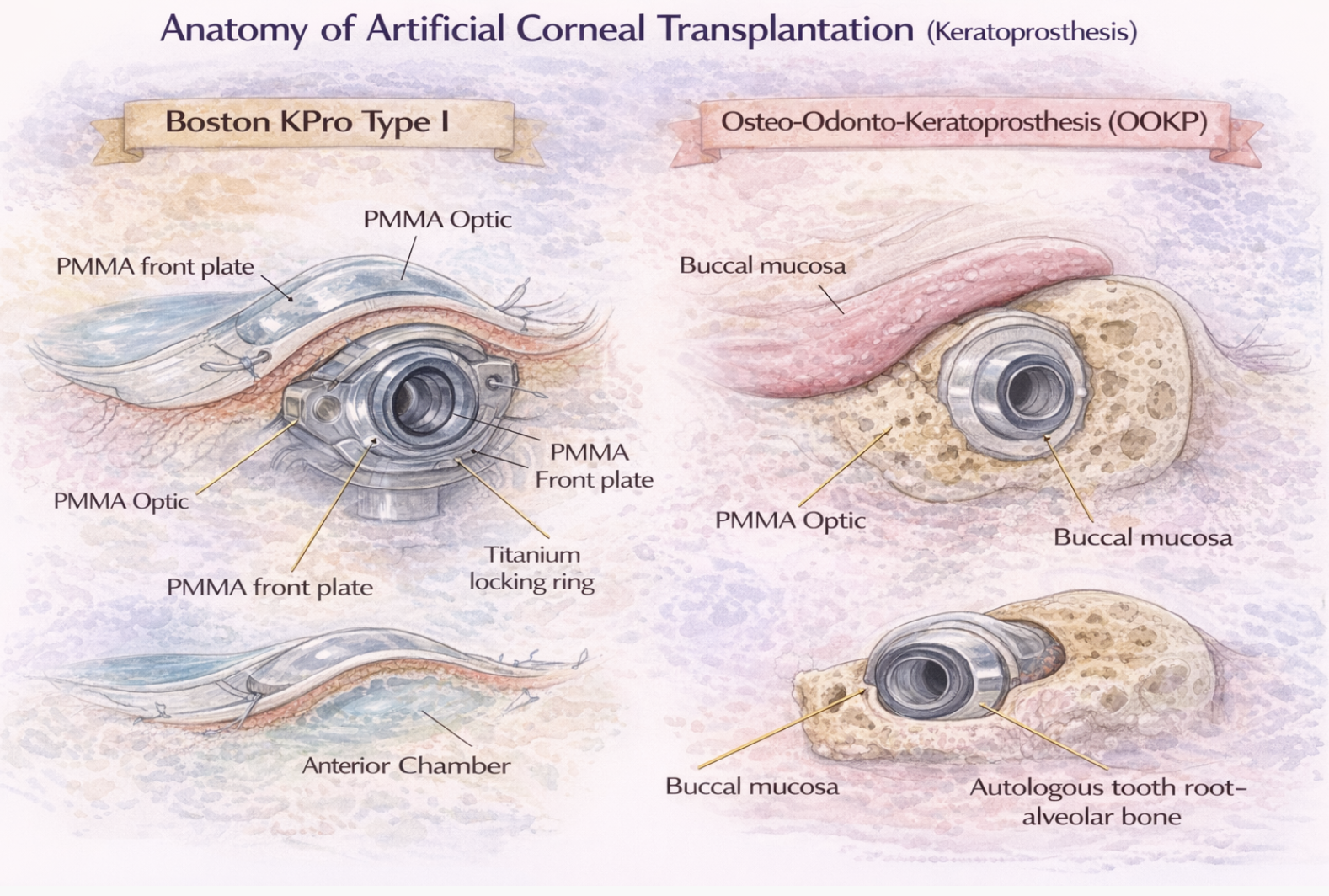
Schematic diagram depicting anatomy of artificial corneal transplantation
Bharat Gurnani, MD
(Click Image to Enlarge)
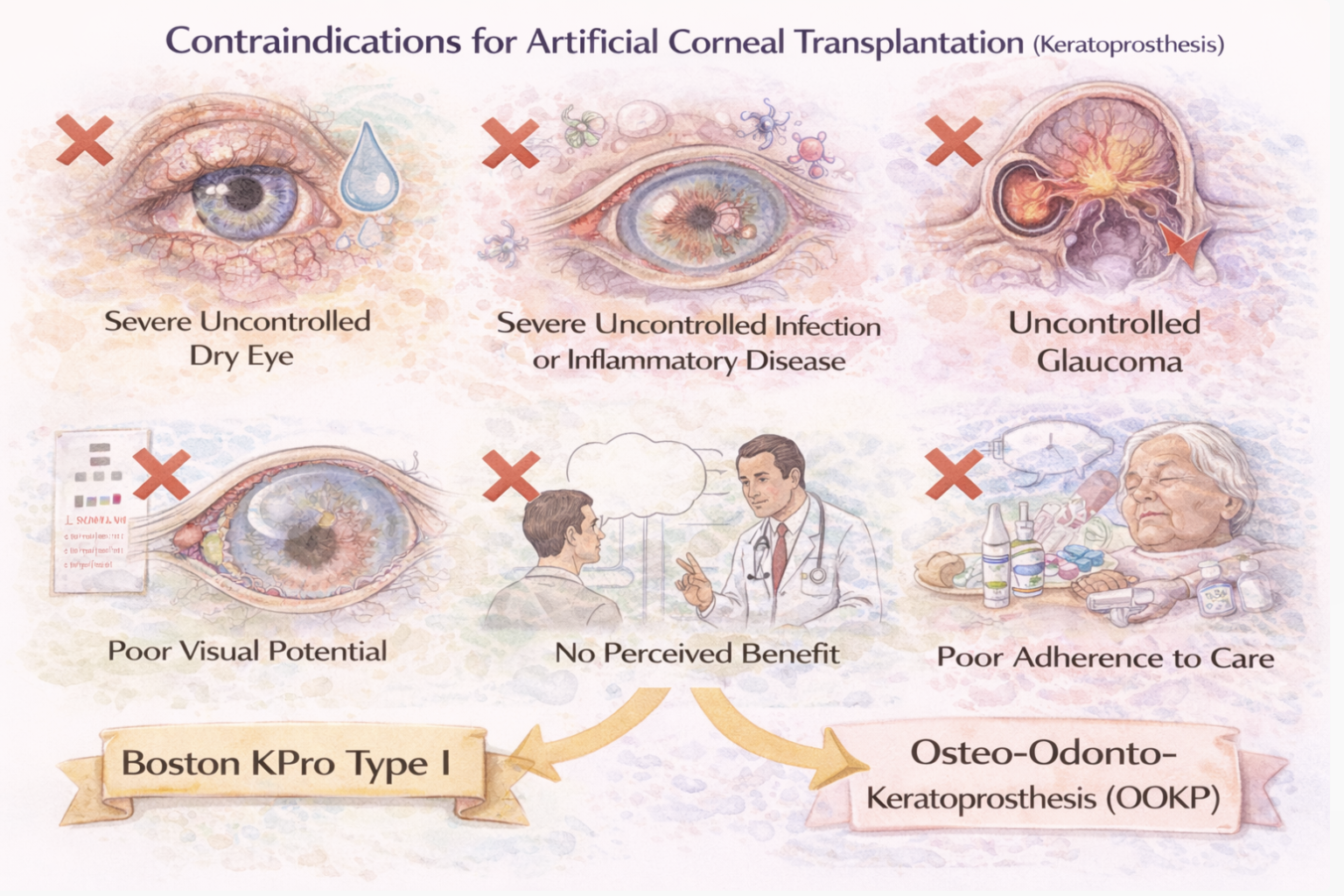
Schematic diagram depicting contraindications of artificial corneal transplantation
Bharat Gurnani, MD
References
Tóth G, Liu S, Li S, Váncsa S, Paczkó M, Kói T, Hegyi P, Szentmáry N. Outcomes of Penetrating Keratoplasty and Boston Type 1 Keratoprosthesis in Aniridia-Associated Keratopathy: A Systematic Review and Meta-Analysis. American journal of ophthalmology. 2026 Feb:282():405-415. doi: 10.1016/j.ajo.2025.11.027. Epub 2025 Nov 21 [PubMed PMID: 41276206]
Level 1 (high-level) evidencePascolini D, Mariotti SP. Global estimates of visual impairment: 2010. The British journal of ophthalmology. 2012 May:96(5):614-8. doi: 10.1136/bjophthalmol-2011-300539. Epub 2011 Dec 1 [PubMed PMID: 22133988]
Level 1 (high-level) evidenceMathews PM, Lindsley K, Aldave AJ, Akpek EK. Etiology of Global Corneal Blindness and Current Practices of Corneal Transplantation: A Focused Review. Cornea. 2018 Sep:37(9):1198-1203. doi: 10.1097/ICO.0000000000001666. Epub [PubMed PMID: 29912039]
Avadhanam VS, Smith HE, Liu C. Keratoprostheses for corneal blindness: a review of contemporary devices. Clinical ophthalmology (Auckland, N.Z.). 2015:9():697-720. doi: 10.2147/OPTH.S27083. Epub 2015 Apr 16 [PubMed PMID: 25945031]
Mitry D, Bhogal M, Patel AK, Lee BS, Chai SM, Price MO, Price FW Jr, Jun AS, Aldave AJ, Mehta JS, Busin M, Allan BD. Descemet stripping automated endothelial keratoplasty after failed penetrating keratoplasty: survival, rejection risk, and visual outcome. JAMA ophthalmology. 2014 Jun:132(6):742-9. doi: 10.1001/jamaophthalmol.2014.352. Epub [PubMed PMID: 24763830]
Level 2 (mid-level) evidenceMemmi B, Wu Q, Borderie V, Allain JM. Assessment of Human Corneal Biomechanical Properties After Refractive Surgery With Inflation Test Using Optical Coherence Tomography. Journal of refractive surgery (Thorofare, N.J. : 1995). 2026 Jan:42(1):e64-e70. doi: 10.3928/1081597X-20251202-03. Epub 2026 Jan 1 [PubMed PMID: 41525093]
Fu L, Perez AV, Maqsood S, Kopsachilis N, Foti R, D'Esposito F, Musa M, Tognetto D, Gagliano C, Zeppieri M. Artificial and Bioengineered Therapeutic Options for Corneal Endothelial Disease. Bioengineering (Basel, Switzerland). 2025 Sep 30:12(10):. doi: 10.3390/bioengineering12101064. Epub 2025 Sep 30 [PubMed PMID: 41155063]
Parikumar P, Haraguchi K, Senthilkumar R, Abraham SJ. Human corneal endothelial cell transplantation with nanocomposite gel sheet preserves corneal stability in post-corneal transplant bullous keratopathy: a 16-year follow-up. American journal of stem cells. 2024:13(3):162-168. doi: 10.62347/CBYH7014. Epub 2024 Jun 15 [PubMed PMID: 39021374]
Hernández J, Santos N, Ahumada M. Advances in 3D Bioprinting for Corneal Regeneration. Gels (Basel, Switzerland). 2025 May 31:11(6):. doi: 10.3390/gels11060422. Epub 2025 May 31 [PubMed PMID: 40558721]
Level 3 (low-level) evidenceChen KG, Starnes TW, Kravets S, Ghosh S, de la Cruz J, Cortina MS. Recurrent retroprosthetic membranes in Boston Keratoprosthesis Type I: Incidence, risk factors, and complications. The ocular surface. 2025 Oct:38():424-430. doi: 10.1016/j.jtos.2025.11.002. Epub 2025 Nov 12 [PubMed PMID: 41232600]
Bernstein A, Gheth Y, Nassrallah W, Berkache M, Haagdorens M, Harissi-Dagher M. Long-term outcomes of the Boston keratoprosthesis: a 15-year follow-up. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2025 Sep 1:():. pii: S0008-4182(25)00362-X. doi: 10.1016/j.jcjo.2025.08.005. Epub 2025 Sep 1 [PubMed PMID: 40876808]
Giles CL, Henderson JW. Keratoprosthesis: current status. The American journal of the medical sciences. 1967 Feb:253(2):239-42 [PubMed PMID: 5334643]
STONE W Jr. Alloplasty in surgery of the eye. The New England journal of medicine. 1958 Mar 6:258(10):486-90 contd [PubMed PMID: 13517505]
Barnham JJ, Roper-Hall MJ. Keratoprosthesis: a long-term review. The British journal of ophthalmology. 1983 Jul:67(7):468-74 [PubMed PMID: 6860613]
Hicks CR, Crawford GJ, Dart JK, Grabner G, Holland EJ, Stulting RD, Tan DT, Bulsara M. AlphaCor: Clinical outcomes. Cornea. 2006 Oct:25(9):1034-42 [PubMed PMID: 17133049]
Level 2 (mid-level) evidenceHollick EJ, Watson SL, Dart JK, Luthert PJ, Allan BD. Legeais BioKpro III keratoprosthesis implantation: long term results in seven patients. The British journal of ophthalmology. 2006 Sep:90(9):1146-51 [PubMed PMID: 16929061]
Nonpassopon M, Niparugs M, Cortina MS. Boston Type 1 Keratoprosthesis: Updated Perspectives. Clinical ophthalmology (Auckland, N.Z.). 2020:14():1189-1200. doi: 10.2147/OPTH.S219270. Epub 2020 Apr 29 [PubMed PMID: 32425503]
Level 3 (low-level) evidenceTalati RK, Hallak JA, Karas FI, de la Cruz J, Cortina MS. Retroprosthetic Membrane Formation in Boston Keratoprosthesis: A Case-Control-Matched Comparison of Titanium Versus PMMA Backplate. Cornea. 2018 Feb:37(2):145-150. doi: 10.1097/ICO.0000000000001462. Epub [PubMed PMID: 29140862]
Level 2 (mid-level) evidenceFalcinelli G, Falsini B, Taloni M, Colliardo P, Falcinelli G. Modified osteo-odonto-keratoprosthesis for treatment of corneal blindness: long-term anatomical and functional outcomes in 181 cases. Archives of ophthalmology (Chicago, Ill. : 1960). 2005 Oct:123(10):1319-29 [PubMed PMID: 16219722]
Level 3 (low-level) evidenceTan A, Tan DT, Tan XW, Mehta JS. Osteo-odonto keratoprosthesis: systematic review of surgical outcomes and complication rates. The ocular surface. 2012 Jan:10(1):15-25. doi: 10.1016/j.jtos.2012.01.003. Epub 2012 Jan 8 [PubMed PMID: 22330056]
Level 1 (high-level) evidenceLiu C, Okera S, Tandon R, Herold J, Hull C, Thorp S. Visual rehabilitation in end-stage inflammatory ocular surface disease with the osteo-odonto-keratoprosthesis: results from the UK. The British journal of ophthalmology. 2008 Sep:92(9):1211-7. doi: 10.1136/bjo.2007.130567. Epub 2008 May 29 [PubMed PMID: 18511541]
Level 2 (mid-level) evidenceMarchi V, Ricci R, Pecorella I, Ciardi A, Di Tondo U. Osteo-odonto-keratoprosthesis. Description of surgical technique with results in 85 patients. Cornea. 1994 Mar:13(2):125-30 [PubMed PMID: 8156783]
Bakshi SK, Graney J, Paschalis EI, Agarwal S, Basu S, Iyer G, Liu C, Srinivasan B, Chodosh J. Design and Outcomes of a Novel Keratoprosthesis: Addressing Unmet Needs in End-Stage Cicatricial Corneal Blindness. Cornea. 2020 Apr:39(4):484-490. doi: 10.1097/ICO.0000000000002207. Epub [PubMed PMID: 31724985]
Fariselli C, Toprak I, Al-Shymali O, Alio Del Barrio JL, Alio JL. Corneal transplantation outcomes after the extrusion of an intrastromal keratoprosthesis: a pilot study. Eye and vision (London, England). 2020:7():26. doi: 10.1186/s40662-020-00193-4. Epub 2020 May 8 [PubMed PMID: 32411808]
Level 3 (low-level) evidenceBasu S, Serna-Ojeda JC, Senthil S, Pappuru RR, Bagga B, Sangwan V. The Aurolab Keratoprosthesis (KPro) versus the Boston Type I Kpro: 5-year Clinical Outcomes in 134 Cases of Bilateral Corneal Blindness. American journal of ophthalmology. 2019 Sep:205():175-183. doi: 10.1016/j.ajo.2019.03.016. Epub 2019 Mar 22 [PubMed PMID: 30905723]
Level 2 (mid-level) evidenceShanbhag SS, Senthil S, Mohamed A, Basu S. Outcomes of the Boston type 1 and the Aurolab keratoprosthesis in eyes with limbal stem cell deficiency. The British journal of ophthalmology. 2021 Apr:105(4):473-478. doi: 10.1136/bjophthalmol-2020-316369. Epub 2020 Jun 17 [PubMed PMID: 32554443]
Gomaa A, Comyn O, Liu C. Keratoprostheses in clinical practice - a review. Clinical & experimental ophthalmology. 2010 Mar:38(2):211-24. doi: 10.1111/j.1442-9071.2010.02231.x. Epub [PubMed PMID: 20398109]
Tan XW, Thompson B, Konstantopoulos A, Goh TW, Setiawan M, Yam GH, Tan D, Khor KA, Mehta JS. Application of Graphene as Candidate Biomaterial for Synthetic Keratoprosthesis Skirt. Investigative ophthalmology & visual science. 2015 Oct:56(11):6605-11. doi: 10.1167/iovs.15-17306. Epub [PubMed PMID: 26465888]
Ficoń H, Zniszczoł S, Morawiec T, Orzechowska-Wylęgała B, Balicz A. Osteo-odonto-keratoprosthesis: a surgical procedure for treating advanced corneal diseases. The Saudi dental journal. 2026 Jan 8:38(1):4. doi: 10.1007/s44445-025-00102-2. Epub 2026 Jan 8 [PubMed PMID: 41501589]
Razavi P, Vingopoulos F, Dohlman TH, Starr CE. Keratoprosthesis Indications, Outcomes, and Future Directions. Cornea. 2026 Jan 1:45(1):130-135. doi: 10.1097/ICO.0000000000004005. Epub 2025 Oct 2 [PubMed PMID: 41251419]
Level 3 (low-level) evidenceGurnani B, Kaur K. Post-market surveillance of ophthalmic implants: role of real-world evidence. Expert review of medical devices. 2025 Dec:22(12):1303-1308. doi: 10.1080/17434440.2025.2579578. Epub 2025 Oct 24 [PubMed PMID: 41123186]
Suffo S, Abdin AD, Daas L, Seitz B, Abu Dail Y. When the Keratoprosthesis Is Too Small: Homburger Corneal Gap Bridging Surgical Technique for Combined Vitreoretinal Surgery and Large-Diameter Keratoplasty. Cornea. 2026 Jan 1:45(1):112-115. doi: 10.1097/ICO.0000000000003999. Epub 2025 Oct 23 [PubMed PMID: 41247281]
Zarei-Ghanavati M, Avadhanam V, Vasquez Perez A, Liu C. The osteo-odonto-keratoprosthesis. Current opinion in ophthalmology. 2017 Jul:28(4):397-402. doi: 10.1097/ICU.0000000000000388. Epub [PubMed PMID: 28441214]
Level 3 (low-level) evidenceHille K, Grabner G, Liu C, Colliardo P, Falcinelli G, Taloni M, Falcinelli G. Standards for modified osteoodontokeratoprosthesis (OOKP) surgery according to Strampelli and Falcinelli: the Rome-Vienna Protocol. Cornea. 2005 Nov:24(8):895-908 [PubMed PMID: 16227830]
Level 2 (mid-level) evidenceWróbel-Dudzińska D, Ćwiklińska-Haszcz A, Kosior-Jarecka E, Żarnowski T. Difficulties in management of ocular surface in the late phase of toxic epidermal necrolysis - a rare case report. Annals of agricultural and environmental medicine : AAEM. 2025 Sep 18:32(3):424-427. doi: 10.26444/aaem/202806. Epub 2025 Mar 28 [PubMed PMID: 41025191]
Level 3 (low-level) evidenceGurnani B, Kaur K, Lalgudi VG, Kundu G, Mimouni M, Liu H, Jhanji V, Prakash G, Roy AS, Shetty R, Gurav JS. Role of artificial intelligence, machine learning and deep learning models in corneal disorders - A narrative review. Journal francais d'ophtalmologie. 2024 Sep:47(7):104242. doi: 10.1016/j.jfo.2024.104242. Epub 2024 Jul 15 [PubMed PMID: 39013268]
Level 3 (low-level) evidenceAouimeur I, Coulomb L, Fraine S, He Z, Bonnet G, Sagnial T, Travers G, Xxx S, Mauclair C, Moisan A, Gain P, Thuret G, Maurin C. Tissue-Engineered Endothelial Keratoplasty with Controlled Cell Density: Toward Super TEEKs. Tissue engineering. Part A. 2025 Sep 23:():. doi: 10.1177/19373341251381346. Epub 2025 Sep 23 [PubMed PMID: 40986463]
Kurihara T, Eguchi H, Hotta F, Mano F, Iwahashi C, Kusaka S. Short-term perfluoro-n-octane tamponade for combined penetrating keratoplasty and pars plana vitrectomy. Retinal cases & brief reports. 2025 Nov 18:():. doi: 10.1097/ICB.0000000000001845. Epub 2025 Nov 18 [PubMed PMID: 41481907]
Level 3 (low-level) evidenceMorcos DM, Dohlman TH, Durand ML. Incidence and Microbiology of Endophthalmitis in Eyes With a Type 1 Boston Keratoprosthesis: A Systematic Review and Meta-Analysis. Cornea. 2025 Dec 2:():. doi: 10.1097/ICO.0000000000004061. Epub 2025 Dec 2 [PubMed PMID: 41474942]
Level 1 (high-level) evidenceAgarwal S, Bhambhani V, Rajarajan M, Chodosh J. Decision-Making in Keratoprosthesis: Navigating Device Selection in Complex Ocular Scenarios. Turkish journal of ophthalmology. 2025 Dec 25:55(6):341-349. doi: 10.4274/tjo.galenos.2025.33802. Epub [PubMed PMID: 41447022]
Geoffrion D, Akl C, Harissi-Dagher M. Bandage contact lens wear in Boston keratoprosthesis type 1 surgery. European journal of ophthalmology. 2025 Dec 22:():11206721251407013. doi: 10.1177/11206721251407013. Epub 2025 Dec 22 [PubMed PMID: 41428757]
Natarajan S, Bayram-Suverza M, Aguilar-Valdez I, González-Suriel ML. Endophthalmitis with keratitis-how to manage severe cases? : A narrative review. Die Ophthalmologie. 2025 Dec 1:():. doi: 10.1007/s00347-025-02357-w. Epub 2025 Dec 1 [PubMed PMID: 41326823]
Level 3 (low-level) evidenceMurra S, Wiedemann J, Schlereth S, Cursiefen C, Bachmann B. Management and Histological Analysis of a Retroprosthetic Membrane as a Novel Complication After EndoArt Implantation. Cornea. 2025 Dec 23:():. doi: 10.1097/ICO.0000000000004076. Epub 2025 Dec 23 [PubMed PMID: 41474960]
Sawires K, Tao BK, Nithianandan H, Menant-Tay L, O'Connor M, Yan P, Arjmand P. Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review of Ophthalmic Management and Treatment. Vision (Basel, Switzerland). 2025 Sep 11:9(3):. doi: 10.3390/vision9030078. Epub 2025 Sep 11 [PubMed PMID: 40981321]
Level 1 (high-level) evidenceMeshko B, Volatier T, Cursiefen C, Notara M. Limbal Epithelial Stem Cells in Review: Immune and Lymphangiogenic Privilege and Their Clinical Relevance. Cells. 2026 Jan 5:15(1):. doi: 10.3390/cells15010091. Epub 2026 Jan 5 [PubMed PMID: 41511374]
Gurnani B, Czyz CN, Mahabadi N, Havens SJ. Corneal Graft Rejection. StatPearls. 2025 Jan:(): [PubMed PMID: 30085585]
Gurnani B, Feroze KB, Patel BC. Neurotrophic Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 28613758]
Gurnani B, Kaur K, Chaudhary S, Kaur RP, Nayak S, Mishra D, Balakrishnan H, Parkash RO, Morya AK, Porwal A. Pediatric corneal transplantation: techniques, challenges, and outcomes. Therapeutic advances in ophthalmology. 2024 Jan-Dec:16():25158414241237906. doi: 10.1177/25158414241237906. Epub 2024 Mar 25 [PubMed PMID: 38533487]
Level 3 (low-level) evidenceAtighehchian M, Latifi A, Nozarian Z, Amoli FA, Zarei-Ghanavati M. Fungal keratitis complicating the diagnosis of Acanthamoeba keratitis. Medical mycology case reports. 2025 Mar:47():100687. doi: 10.1016/j.mmcr.2024.100687. Epub 2024 Dec 7 [PubMed PMID: 39811097]
Level 3 (low-level) evidenceColby K. Pediatric Keratoprosthesis: A Promise Unfulfilled. Ophthalmology. 2018 Feb:125(2):147-149. doi: 10.1016/j.ophtha.2017.10.030. Epub [PubMed PMID: 29389402]
Fung SSM, Jabbour S, Harissi-Dagher M, Tan RRG, Hamel P, Baig K, Ali A. Visual Outcomes and Complications of Type I Boston Keratoprosthesis in Children: A Retrospective Multicenter Study and Literature Review. Ophthalmology. 2018 Feb:125(2):153-160. doi: 10.1016/j.ophtha.2017.07.009. Epub 2017 Aug 12 [PubMed PMID: 28807636]
Level 2 (mid-level) evidenceChen E, Reynolds HH, Graham LV. Ocular cicatricial pemphigoid treated with intramuscular corticotropin injections. JAAD case reports. 2020 May:6(5):450-452. doi: 10.1016/j.jdcr.2020.02.034. Epub 2020 Apr 30 [PubMed PMID: 32382644]
Level 3 (low-level) evidenceSpampinato SF, Caruso GI, De Pasquale R, Sortino MA, Merlo S. The Treatment of Impaired Wound Healing in Diabetes: Looking among Old Drugs. Pharmaceuticals (Basel, Switzerland). 2020 Apr 1:13(4):. doi: 10.3390/ph13040060. Epub 2020 Apr 1 [PubMed PMID: 32244718]
Wu JH, Varkhedi V, Radha Saseendrakumar B, Acuff K, Weinreb RN, Baxter SL. Social and Health Care Utilization Factors Associated With Ophthalmic Visit Nonadherence in Glaucoma: An All of Us Study. Journal of glaucoma. 2023 Dec 1:32(12):1029-1037. doi: 10.1097/IJG.0000000000002300. Epub 2023 Aug 29 [PubMed PMID: 37671531]
Avadhanam VS, Liu CS. A brief review of Boston type-1 and osteo-odonto keratoprostheses. The British journal of ophthalmology. 2015 Jul:99(7):878-87. doi: 10.1136/bjophthalmol-2014-305359. Epub 2014 Oct 27 [PubMed PMID: 25349081]
Visioli G, Alisi L, Armentano M, Mastromarino D, Iannetti L. Our experience in optical cylinder preservation in osteo-odonto-keratoprosthesis (OOKP). European journal of ophthalmology. 2025 Sep 25:():11206721251380933. doi: 10.1177/11206721251380933. Epub 2025 Sep 25 [PubMed PMID: 40997248]
Kruoch Z, Choo AY, Kemp A, Gonzales M, Yim TW, McCann P, Liu SH, Ting DSJ, Kuo IC. Medical and surgical interventions for neurotrophic keratopathy. The Cochrane database of systematic reviews. 2025 Dec 5:12(12):CD015723. doi: 10.1002/14651858.CD015723.pub2. Epub 2025 Dec 5 [PubMed PMID: 41347649]
Level 1 (high-level) evidenceCox I, Stevens S. Care of ophthalmic surgical instruments. Community eye health. 2000:13(35):40-1 [PubMed PMID: 17491960]
Tao YK. Intraoperative optical coherence tomography in ophthalmology: Technologies and applications. Taiwan journal of ophthalmology. 2025 Jul-Sep:15(3):378-388. doi: 10.4103/tjo.TJO-D-25-00076. Epub 2025 Sep 5 [PubMed PMID: 40995326]
Jacobson A, Besirli CG, Bohnsack BL. Outcomes of combined endoscopic vitrectomy and posteriorly placed glaucoma drainage devices in pediatric patients. BMC ophthalmology. 2022 Apr 1:22(1):149. doi: 10.1186/s12886-022-02373-3. Epub 2022 Apr 1 [PubMed PMID: 35365117]
Tas AY, Abay B, Muftuoglu O. Clinical outcomes and significance of postoperative ultrasound biomicroscopy in patients with Boston type 1 keratoprosthesis. Arquivos brasileiros de oftalmologia. 2024:88(1):e20230160. doi: 10.5935/0004-2749.2023-0160. Epub 2024 Aug 2 [PubMed PMID: 39109743]
Level 2 (mid-level) evidenceHüfner L, Augustin VA, Auffarth GU, Friedrich M, Son HS. [New tissue-additive procedures to improve vision in keratoconus]. Die Ophthalmologie. 2026 Feb:123(2):104-110. doi: 10.1007/s00347-025-02370-z. Epub 2026 Jan 3 [PubMed PMID: 41483160]
Zhang WP, Lv HJ, Pan AP, Zhang WX, Shao X, Qu YZ, Li AS, Chen LH, Zeng SQ, Yu AY. Femtosecond lasers in ophthalmology: Mechanisms, clinical breakthroughs, and multidisciplinary frontiers. Progress in retinal and eye research. 2026 Jan:110():101431. doi: 10.1016/j.preteyeres.2025.101431. Epub 2025 Dec 6 [PubMed PMID: 41360298]
Gamage GP, Lovegrove J, Seneviratne S, Tobiano G, Gillespie B. Postoperative Wound Care Practices of Acute Care Nurses: An Integrative Review. International wound journal. 2025 Nov:22(11):e70781. doi: 10.1111/iwj.70781. Epub [PubMed PMID: 41192409]
Adamovich-Zeitlin R, Ramakrishnan MS, Zhu D, Ritterband D, Barile G, Schiff W, Seedor J, Cheela I, Tirsi A, Baghdasaryan E, Kaden TR. Clinical Outcomes of Boston Type 1 Keratoprosthesis with and without Endophthalmitis During the Covid-19 Pandemic. Ocular immunology and inflammation. 2025 Nov:33(9):2109-2114. doi: 10.1080/09273948.2025.2562357. Epub 2025 Sep 23 [PubMed PMID: 40985885]
Level 2 (mid-level) evidenceStapleton F, Abad JC, Barabino S, Burnett A, Iyer G, Lekhanont K, Li T, Liu Y, Navas A, Obinwanne CJ, Qureshi R, Roshandel D, Sahin A, Shih K, Tichenor A, Jones L. TFOS lifestyle: Impact of societal challenges on the ocular surface. The ocular surface. 2023 Apr:28():165-199. doi: 10.1016/j.jtos.2023.04.006. Epub 2023 Apr 14 [PubMed PMID: 37062429]
Williamson SL, Cortina MS. Boston type 1 keratoprosthesis from patient selection through postoperative management: a review for the keratoprosthetic surgeon. Clinical ophthalmology (Auckland, N.Z.). 2016:10():437-43. doi: 10.2147/OPTH.S83677. Epub 2016 Mar 14 [PubMed PMID: 27041986]
Lim JI, Machen L, Arteaga A, Karas FI, Hyde R, Cao D, Niec M, Vajaranant TS, Cortina MS. COMPARISON OF VISUAL AND ANATOMICAL OUTCOMES OF EYES UNDERGOING TYPE I BOSTON KERATOPROSTHESIS WITH COMBINATION PARS PLANA VITRECTOMY WITH EYES WITHOUT COMBINATION VITRECTOMY. Retina (Philadelphia, Pa.). 2018 Sep:38 Suppl 1(Suppl 1):S125-S133. doi: 10.1097/IAE.0000000000002036. Epub [PubMed PMID: 29370031]
Kaur J. Osteo-odonto keratoprosthesis: Innovative dental and ophthalmic blending. Journal of Indian Prosthodontic Society. 2018 Apr-Jun:18(2):89-95. doi: 10.4103/jips.jips_283_17. Epub [PubMed PMID: 29692560]
Huang Y, Dong Y, Wang L, Du G, Yu J, Song J, Chiang HH. Long-term outcomes of MICOF keratoprosthesis in the end stage of autoimmune dry eyes: an experience in China. The British journal of ophthalmology. 2012 Jan:96(1):28-33. doi: 10.1136/bjo.2010.193029. Epub 2011 Mar 31 [PubMed PMID: 21454379]
Level 2 (mid-level) evidenceBehlau I, Martin KV, Martin JN, Naumova EN, Cadorette JJ, Sforza JT, Pineda R 2nd, Dohlman CH. Infectious endophthalmitis in Boston keratoprosthesis: incidence and prevention. Acta ophthalmologica. 2014 Nov:92(7):e546-55. doi: 10.1111/aos.12309. Epub 2014 Jan 25 [PubMed PMID: 24460594]
Level 2 (mid-level) evidenceGeoffrion D, Harissi-Dagher M. Glaucoma Risk Factors and Outcomes Following Boston Keratoprosthesis Type 1 Surgery. American journal of ophthalmology. 2021 Jun:226():56-67. doi: 10.1016/j.ajo.2021.01.006. Epub 2021 Jan 22 [PubMed PMID: 33493469]
Nascimento E Silva R, Taniguchi EV, Cruzat A, Paschalis EI, Pasquale LR, Colby KA, Dohlman CH, Chodosh J, Shen LQ. Angle Anatomy and Glaucoma in Patients With Boston Keratoprosthesis. Cornea. 2020 Jun:39(6):713-719. doi: 10.1097/ICO.0000000000002216. Epub [PubMed PMID: 31764284]
Quercia AZF, Silva LD, de Oliveira F, Teixeira SH, de Sousa LB, de Oliveira LA. Visual Field Characteristics of Type I Boston Keratoprosthesis Patients Without Glaucoma. Journal of glaucoma. 2021 Jun 1:30(6):532-536. doi: 10.1097/IJG.0000000000001737. Epub [PubMed PMID: 33149106]
Samarawickrama C, Strouthidis N, Wilkins MR. Boston keratoprosthesis type 1: outcomes of the first 38 cases performed at Moorfields Eye Hospital. Eye (London, England). 2018 Jun:32(6):1087-1092. doi: 10.1038/s41433-018-0016-4. Epub 2018 Feb 14 [PubMed PMID: 29440740]
Level 3 (low-level) evidenceVajaranant TS, Liu J, Wilensky J, Cortina MS, Aref AA. Innovative approaches to glaucoma management of Boston keratoprosthesis type 1. Current ophthalmology reports. 2016 Sep:4(3):147-153. doi: 10.1007/s40135-016-0102-3. Epub 2016 Jul 26 [PubMed PMID: 28529825]
Kanu LN, Niparugs M, Nonpassopon M, Karas FI, de la Cruz JM, Cortina MS. Predictive factors of Boston Type I Keratoprosthesis outcomes: A long-term analysis. The ocular surface. 2020 Oct:18(4):613-619. doi: 10.1016/j.jtos.2020.07.012. Epub 2020 Jul 21 [PubMed PMID: 32702418]
Priddy J, Bardan AS, Tawfik HS, Liu C. Systematic Review and Meta-Analysis of the Medium- and Long-Term Outcomes of the Boston Type 1 Keratoprosthesis. Cornea. 2019 Nov:38(11):1465-1473. doi: 10.1097/ICO.0000000000002098. Epub [PubMed PMID: 31403526]
Level 1 (high-level) evidenceDaoud R, Sabeti S, Harissi-Dagher M. Management of corneal melt in patients with Boston Keratoprosthesis Type 1: Repair versus repeat. The ocular surface. 2020 Oct:18(4):713-717. doi: 10.1016/j.jtos.2020.07.005. Epub 2020 Aug 7 [PubMed PMID: 32777438]
Rishi P, Rishi E, Agarwal V, Nair S, Iyer G, Srinivasan B, Agarwal S. Vitreoretinal Complications and Outcomes in 92 Eyes Undergoing Surgery for Modified Osteo-Odonto-Keratoprosthesis: A 10-Year Review. Ophthalmology. 2018 Jun:125(6):832-841. doi: 10.1016/j.ophtha.2017.12.003. Epub 2018 Jan 17 [PubMed PMID: 29342438]
Elsliger S, Sebag M, Nassrallah WB, Berkache M, Bernstein A, Geoffrion D, Tolba R, Elkader AA, Harissi-Dagher M. The Risk of Retinal Detachment Following Boston Keratoprosthesis Type 1 Implantation: Insights From a Retrospective Case Review. American journal of ophthalmology. 2026 Jan:281():1-9. doi: 10.1016/j.ajo.2025.09.007. Epub 2025 Sep 5 [PubMed PMID: 40915518]
Level 2 (mid-level) evidenceAvadhanam VS, Smith J, Poostchi A, Chervenkoff J, Al Raqqad N, Francis I, Liu CS. Detection of laminar resorption in osteo-odonto-keratoprostheses. The ocular surface. 2019 Jan:17(1):78-82. doi: 10.1016/j.jtos.2018.09.004. Epub 2018 Sep 15 [PubMed PMID: 30227262]
Iyer G, Srinivasan B, Agarwal S, Rachapalle SR. Laminar resorption in modified osteo-odonto-keratoprosthesis procedure: a cause for concern. American journal of ophthalmology. 2014 Aug:158(2):263-269.e2. doi: 10.1016/j.ajo.2014.03.004. Epub 2014 Mar 12 [PubMed PMID: 24631477]
Level 2 (mid-level) evidenceJeng BH, Ahmad S. In Pursuit of the Elimination of Corneal Blindness: Is Establishing Eye Banks and Training Surgeons Enough? Ophthalmology. 2021 Jun:128(6):813-815. doi: 10.1016/j.ophtha.2020.06.042. Epub 2020 Jul 29 [PubMed PMID: 32739177]
Gain P, Jullienne R, He Z, Aldossary M, Acquart S, Cognasse F, Thuret G. Global Survey of Corneal Transplantation and Eye Banking. JAMA ophthalmology. 2016 Feb:134(2):167-73. doi: 10.1001/jamaophthalmol.2015.4776. Epub [PubMed PMID: 26633035]
Level 3 (low-level) evidenceThuret G, Courrier E, Poinard S, Gain P, Baud'Huin M, Martinache I, Cursiefen C, Maier P, Hjortdal J, Sanchez Ibanez J, Ponzin D, Ferrari S, Jones G, Griffoni C, Rooney P, Bennett K, Armitage WJ, Figueiredo F, Nuijts R, Dickman M. One threat, different answers: the impact of COVID-19 pandemic on cornea donation and donor selection across Europe. The British journal of ophthalmology. 2022 Mar:106(3):312-318. doi: 10.1136/bjophthalmol-2020-317938. Epub 2020 Nov 26 [PubMed PMID: 33243832]
Belin MW, Güell JL, Grabner G. Suggested Guidelines for Reporting Keratoprosthesis Results: Consensus Opinion of the Cornea Society, Asia Cornea Society, EuCornea, PanCornea, and the KPRO Study Group. Cornea. 2016 Feb:35(2):143-4. doi: 10.1097/ICO.0000000000000703. Epub [PubMed PMID: 26619387]
Level 3 (low-level) evidenceNavarro-Naranjo PI, Hernandez-Chavarria C. De Wit-Carter G, Hernandez-Chavarria C, Navarro-Naranjo PI, et al. Boston keratoprosthesis type 1 (KPro) without contact lens wearing in end-stage corneal disease: The APEC Experience. European Journal of Ophthalmology. 2024 Jul;34(4):1063-1070. European journal of ophthalmology. 2026 Jan 2:():11206721251407008. doi: 10.1177/11206721251407008. Epub 2026 Jan 2 [PubMed PMID: 41481496]
Lu TC, Huang CH, Lin IC. Artificial Intelligence Application in Cornea and External Diseases. Diagnostics (Basel, Switzerland). 2025 Dec 15:15(24):. doi: 10.3390/diagnostics15243199. Epub 2025 Dec 15 [PubMed PMID: 41464203]
Hashemian MN, Zia MJ, Khorrami-Nejad M, Abed QS, Hashemian H. Long-term outcomes of corneal transplantation: a review of 8,378 patients. BMC ophthalmology. 2025 Jan 22:25(1):39. doi: 10.1186/s12886-024-03826-7. Epub 2025 Jan 22 [PubMed PMID: 39844058]
Hadavand MB, Heidary F, Heidary R, Gharebaghi R. Role of ophthalmic nurses in prevention of ophthalmic diseases. Medical hypothesis, discovery & innovation ophthalmology journal. 2013 Winter:2(4):92-5 [PubMed PMID: 24822227]
van Nispen RM, Virgili G, Hoeben M, Langelaan M, Klevering J, Keunen JE, van Rens GH. Low vision rehabilitation for better quality of life in visually impaired adults. The Cochrane database of systematic reviews. 2020 Jan 27:1(1):CD006543. doi: 10.1002/14651858.CD006543.pub2. Epub 2020 Jan 27 [PubMed PMID: 31985055]
Level 1 (high-level) evidenceGurnani B, Kaur K. Renaissance of an Emerging Pathogen-Pythium insidiosum Keratitis: An Indian Perspective. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4811-4830. doi: 10.2147/OPTH.S568552. Epub 2025 Dec 18 [PubMed PMID: 41446894]
Level 3 (low-level) evidenceGurnani B, Kaur K. Immune Camouflage in Pythium insidiosum Keratitis: A Hypothesis on Molecular Mimicry and Host Pattern Recognition Receptor Evasion. Clinical ophthalmology (Auckland, N.Z.). 2025:19():4855-4873. doi: 10.2147/OPTH.S560311. Epub 2025 Dec 19 [PubMed PMID: 41446892]
Gurnani B, Kaur K. Corneal cross-linking for keratoconus: a global economic and clinical perspective. Journal of medical economics. 2025 Dec:28(1):2119-2124. doi: 10.1080/13696998.2025.2587416. Epub 2025 Nov 30 [PubMed PMID: 41320236]
Level 3 (low-level) evidenceHall WA, Gurnani B. Compressive Optic Neuropathy. StatPearls. 2026 Jan:(): [PubMed PMID: 32809418]
Gurnani B, Patel BC. Photorefractive Keratectomy. StatPearls. 2026 Jan:(): [PubMed PMID: 31751077]
Nishant P, Gurnani B, Singh P, Sinha S, Kaur K, Kumar A, Sinha RK. Current concepts and recent trends in endothelial keratoplasty. World journal of transplantation. 2025 Jun 18:15(2):102507. doi: 10.5500/wjt.v15.i2.102507. Epub [PubMed PMID: 40535500]
Gurnani B, Kaur K. Advancing diagnostics in Pythium insidiosum keratitis: the emerging role of point-of-care imaging and biosensor-based detection devices. Expert review of medical devices. 2025 Dec:22(12):1287-1292. doi: 10.1080/17434440.2025.2582616. Epub 2025 Nov 2 [PubMed PMID: 41147335]
Gurnani B, Kaur K. Pythium Keratitis. StatPearls. 2026 Jan:(): [PubMed PMID: 34424645]
Shaker HO, Sabry AAF, Salah A, Ragab GM, Sedik NA, Ali Z, Magdy D, Alkafafy AM. The impact of clinical pharmacists' medication reconciliation upon patients' admission to reduce medication discrepancies in the emergency department: a prospective quasi-interventional study. International journal of emergency medicine. 2023 Dec 15:16(1):89. doi: 10.1186/s12245-023-00568-z. Epub 2023 Dec 15 [PubMed PMID: 38102544]