 Gastrointestinal and Hepatic Manifestations of Coronavirus (COVID-19)
Gastrointestinal and Hepatic Manifestations of Coronavirus (COVID-19)
Introduction
COVID-19, the illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a highly contagious viral illness and was declared a global pandemic after the first cases of an atypical acute respiratory illness were initially reported in China in December 2019 and spread to more than 200 countries worldwide. This viral infection readily spreads from person to person via respiratory droplets, mucosal contact, and contaminated surfaces. SARS-CoV-2 primarily affects the respiratory system but can also affect other major organ systems, including the gastrointestinal (GI) tract, liver, cardiovascular system, central nervous system, and kidneys (see Image. Mechanisms of Gastrointestinal Injury With COVID-19). Emerging data indicate that patients with COVID-19 infection may present with isolated gastrointestinal symptoms in the absence of respiratory symptoms. Patients with any primary GI-related symptoms are at increased risk of hospitalization compared to patients without GI symptoms.[1][2][3]
SARS-CoV-2 RNA can be detected in fecal samples of asymptomatic patients who tested negative for COVID-19 by nasopharyngeal swab. Continued fecal shedding in symptomatic COVID-19 patients for days after clinical recovery for an extended period has been reported, which is concerning for possible fecal-oral transmission of this virus. Some laboratories have reported isolating live fecal SARS-CoV-2, suggesting that the GI tract is a primary site of infection rather than merely a location for viral shedding.[4][5]
COVID-19 is also frequently associated with elevated liver biochemistries in patients with or without clinical symptoms. In addition, patients with COVID-19 are increasingly being recognized as being at risk of developing prothrombotic complications such as acute mesenteric ischemia and portal vein thrombosis. This activity will review the effect of SARS-CoV-2 on the GI tract and liver in adult patients.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Coronaviruses are enveloped positive-sense single-stranded ribonucleic acid viruses. Based on their genomic structure, they are classified into 4 different categories as follows:
- Alphacoronavirus
- Betacoronavirus
- Gammacoronavirus
- Deltacoronavirus [6]
SARS-CoV-2 is a betacoronavirus belonging to the same subgenus as the severe acute respiratory syndrome coronavirus (SARS-CoV) and the Middle East Respiratory Syndrome Coronavirus, which have been previously implicated in epidemics with mortality rates up to 10% and 35%, respectively. Genomic characterization of the 2019 novel coronavirus demonstrated 89% nucleotide identity with bat SARS-like CoV and 82% with human SARS-CoV.[7] Throughout the COVID-19 pandemic, SARS-CoV-2 has undergone frequent mutations, resulting in new viral variants. The GI tract and the liver were frequently involved in both the SARS-CoV and MERS-CoV outbreaks, with symptoms similar to those reported with SARS-CoV-2.
Epidemiology
Since the first reported cases of COVID-19 from Wuhan, China, in December 2019 and the subsequent declaration of COVID-19 as a global pandemic by the World Health Organization, this highly contagious infectious disease has spread to more than 200 countries so far, with more than 701 million cases, and more than 6.9 million deaths reported globally. Patients aged older than 65 and patients with specific underlying medical comorbidities (eg, severe obesity, hypertension, chronic kidney disease, diabetes, chronic lung disease, positive smoking status, use of chronic immunosuppressants) are at increased risk of developing severe COVID-19 infection. Based on the results of a meta-analysis of 50 studies from the United States and the United Kingdom, it was noted that patients of Black and Asian ethnic minority groups were at increased risk of contracting COVID-19 infection compared to White patients. In addition, Asian patients may be at increased risk of intensive care unit admission and death, which has significant global public health implications.[8]
Pathophysiology
Effect of SARS-CoV-2 on the Gastrointestinal Tract
The pathogenesis of GI tract involvement in SARS-CoV-2 is likely multifactorial. Several hypotheses have been described, including direct angiotensin-converting enzyme 2-mediated viral cytotoxicity of the intestinal mucosa, cytokine-induced inflammation, gut dysbiosis, and vascular abnormalities. SARS-CoV-2 gains entry into the host cells by binding the SARS-CoV-2 spike protein to the angiotensin-converting enzyme 2 (ACE2) receptors present on the respiratory epithelium, followed by priming of the spike protein by the host transmembrane serine protease 2 that facilitates cell entry and subsequent viral replication.[9] The ACE2 receptor is abundantly expressed in enterocytes of the GI tract, primarily in epithelial cells, and human organoid models have demonstrated active viral replication.[10][11]
SARS-CoV-2 was detected in endoscopic biopsy specimens of the esophagus, stomach, duodenum, and rectum from several patients.[12] Given the reported propensity of SARS-CoV-2 to spread via the fecal-oral route, many studies have reported evidence of cytokine-induced inflammatory response of the intestinal mucosa in patients with COVID-19, characterized by elevation of fecal calprotectin, a calcium- and zinc-binding protein which has been studied extensively as a marker of intestinal mucosal damage in inflammatory bowel disease.[13][14] Several studies have also hypothesized that intestinal infection with SARS-CoV-2 alters the fecal microbiota, potentially damaging enterocytes and causing diarrhea.[15] A study evaluating the effect of SARS-CoV-2 on the GI tract and gut microbiome reported increased infective competence and alteration of the gut microbiome in patients diagnosed with COVID-19.[16] Recent studies have highlighted the oral cavity's role as a portal for viral entry and replication (see Image. Mechanisms of Gastrointestinal Injury With COVID-19).[17]
Effect of SARS-CoV-2 on the Liver and Pancreatobiliary System
Elevations in liver biochemistries are frequently observed in 14% to 53% of patients with COVID-19 infection.[18] The severity of the liver injury depends on the severity of the illness, with hepatic dysfunction occurring more frequently in patients with severe COVID-19 illness. Viral hepatitis classically manifests with a hepatocellular injury that is alanine transaminase predominant; however, hepatocellular injury in patients with COVID-19 infection appears to be aspartate aminotransferase predominant.[19] Because ACE2 receptors are expressed in cholangiocytes, mild elevations in alkaline phosphatase and gamma-glutamyl transferase are not uncommon in patients with COVID-19.[20]
The pathogenesis of liver injury is likely multifactorial and is explained by various hypotheses, including ACE2-mediated viral replication in the liver and its resulting cytotoxicity, hypoxic or ischemic injury, immune-mediated inflammatory response, drug-induced liver injury, and worsening of preexisting liver disease.[21] Severe cytokine-induced systemic inflammation and associated hemodynamic compromise could also contribute to the abnormal liver functions noted in patients with severe COVID-19 infection. Liver enzyme abnormalities can also be attributed to drug-induced liver injury secondary to newer antiviral agents such as remdesivir or concurrent medication use with hepatotoxic potential.
The role of preexisting liver disease in the pathogenesis of COVID-19-associated liver injury is not well studied. Based on data from 2 international registries involving 745 patients with chronic liver disease (with and without cirrhosis) and COVID-19 infection, the mortality rate was significantly higher in patients with cirrhosis at 32% compared to 8% in patients without cirrhosis. Moreover, mortality rates differed by underlying Child-Pugh Class (CPC) score: 19% in CPC A, 25% in CPC B, and 51% in CPC C.[22] Patients with chronic liver disease diagnosed with COVID-19 are at an increased risk of poor clinical outcomes.[22][23][24]
In addition to luminal GI tract cells, ACE2 is expressed in pancreatic islet cells and in pericytes of the pancreatic microvasculature. Literature describing the effect of SARS-CoV-2 on the pancreas, manifesting as acute pancreatitis, is limited. Hyperlipasemia has been reported in a minority of COVID-19 patients, but it is not specific to pancreatitis and does not reflect severe infection or poor clinical outcome.[25][26] However, a single-center prospective clinicopathologic case series reported focal pancreatitis with necrosis of the pancreatic parenchyma and adjacent adipose tissue, as well as calcifications, in 4 patients.[27]
Prothrombotic State
ACE2 binding to SARS-CoV-2 is thought to cause endothelial damage, thereby promoting inflammation and hypercoagulation. There is likely a complex interplay among endothelial damage, proinflammatory cytokines, and underlying coagulopathy caused by sepsis/severe disease. This can cause a hypercoagulable state, leading to conditions such as mesenteric ischemia or portal vein thrombosis, as well as microvascular thrombi in the GI and other systems.[4]
Histopathology
Histopathology Examination of the Gastrointestinal Tract
Histopathological examination of the endoscopic specimens demonstrates positive staining of the viral nucleocapsid protein in the gastric, duodenal, and rectal epithelium cytoplasm. Numerous infiltrating plasma cells and lymphocytes with interstitial edema were seen in the lamina propria of the stomach, duodenum, and rectum. Histopathological examination of the small bowel in a patient admitted with mesenteric ischemia suggested prominent endothelial inflammation of the submucosal vessels and apoptotic bodies.[28]
Histopathology Examination of the Liver
Post-mortem histopathological examination of liver tissue in a deceased patient with COVID-19 infection demonstrated nonspecific findings of moderate macrovesicular steatosis without any intracytoplasmic or intranuclear inclusions commonly associated with underlying nonalcoholic fatty liver disease, sepsis, or secondary to drug-induced liver injury.[29] A prospective single-center clinicopathologic case series study involving the post-mortem histopathological exam of major organs of 11 deceased patients with COVID-19 (mean age 81 years) reported findings of hepatic steatosis in all patients. The liver specimens of 73% of patients demonstrated chronic congestion. Different forms of hepatocyte necrosis were noted in 4 patients. Seventy percent of patients demonstrated nodular proliferation.[27]
History and Physical
Treating clinicians must obtain a detailed clinical history of the onset and duration of symptoms, travel history, exposure to individuals with COVID-19, underlying comorbidities, and medication history. Patients with typical clinical signs suspicious of COVID-19, such as fever, cough, sore throat, loss of taste or smell, malaise, and myalgias, should be tested for SARS-CoV-2. Patients presenting with isolated GI symptoms such as diarrhea, nausea, vomiting, and abdominal pain, or with incidental findings of elevated serum transaminases, should also be tested for SARS-CoV-2 in a high COVID-19-prevalence setting.[30] Patients with SARS-CoV-2 infection can experience many clinical manifestations ranging from no symptoms to critical illness associated with respiratory failure, septic shock, or multiple organ failure.
Most patients present with clinical symptoms such as fever, cough, sore throat, shortness of breath, anosmia, dysgeusia, malaise, and myalgia. However, COVID-19 can present with GI manifestations alone or concur with the other symptoms described earlier. In a meta-analysis of 1992 patients, 1052 (53%) experienced GI symptoms, with diarrhea (34%), nausea (27%), vomiting (16%), and abdominal pain (11%) being the most commonly reported.[31] Loss of appetite is also a commonly reported symptom in patients with COVID-19. A case report described the incidence of hemorrhagic colitis demonstrated endoscopically and was attributed to SARS-CoV-2 after all other etiologies, including ischemic injury, were ruled out.[32]
Evaluation
Initial laboratory assessment should include a complete blood count, a comprehensive metabolic panel with renal and liver function testing, a coagulation panel, and serum lipase at presentation. Viral ribonucleic acid can be isolated from stool specimens of COVID-19 patients, as evidenced by results of a meta-analysis of 23 published and 6 preprint studies involving 4805 patients; fecal tests were positive for SARS-CoV-2 in 8 studies, and viral ribonucleic acid shedding was detected in 41% of patients, implying transmission of SARS-CoV-2 via the possible fecal-oral route, in addition to respiratory droplet transmission.[33]
COVID-19 is also frequently associated with elevations in liver biochemistries in 14% to 53% of patients.[18] Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are generally elevated 1 to 2 times the upper limit of normal, with normal to mildly elevated total bilirubin. Hepatic dysfunction occurs more frequently in severe COVID-19 illness compared to patients with mild illness. Patients with liver injury at presentation had a considerably higher risk of intensive care unit admission and death.[20][31]
Due to the expression of ACE2 receptors in the cholangiocytes, it is not uncommon to see a mild elevation of alkaline phosphatase and gamma-glutamyl transferase in patients with COVID-19.[20] Infectious etiologies, particularly Clostridium difficile and other viral and bacterial enteric infections, should be excluded in patients presenting with isolated symptoms of acute diarrhea and abdominal pain.[34] A troponin level and an electrocardiogram should be performed to rule out cardiac injury, especially in patients with liver abnormalities, with AST significantly greater than ALT. Measuring inflammatory markers such as C-reactive protein, calprotectin, D-dimer, and ferritin can also be considered.
Patients with COVID-19 and elevated liver biochemistries should be evaluated for etiologies unrelated to COVID-19, which must include checking a comprehensive hepatitis panel to rule out other viruses such as hepatitis A, B, and C.[35] In patients with autoimmune hepatitis (AIH) and orthotopic liver transplant (OLT) recipients with active COVID-19, disease flare or acute cellular rejection should not be presumed without a biopsy confirmation indicating the same.[34] Patients with COVID-19 are also increasingly being recognized as being at risk of developing prothrombotic complications, manifesting as acute mesenteric ischemia and portal vein thrombosis.[36].This is likely attributed to a hypercoagulable state associated with this viral illness. If clinically indicated, initial imaging may include a chest x-ray, ultrasound, computerized tomography, or magnetic resonance imaging/magnetic resonance cholangiopancreatography. Endoscopic evaluation should be considered when clinically indicated, with appropriate personal protective equipment as recommended by the American Society for Gastrointestinal Endoscopy, given that endoscopy procedures are associated with a high risk of viral transmission.
Treatment / Management
Managing COVID-19 depends on the severity of illness at presentation, and patients should be appropriately triaged based on clinical symptoms. Asymptomatic patients or patients with mild illness can be managed in the ambulatory setting with supportive care and self-quarantine recommendations. However, patients with moderate-to-severe illness or patients at risk of developing severe illness should be clinically monitored in the hospital setting and managed as outlined in the updated National Institute of Health guidelines. As with other viral enteric infections, GI symptoms such as nausea and vomiting should be managed conservatively with intravenous fluids, antiemetic medications, and close monitoring of serum electrolytes.
Remdesivir is the first Food and Drug Administration-approved drug that has been indicated for use in adults and pediatric patients to treat hospitalized patients with COVID-19. Liver biochemistries must be performed at baseline and regularly monitored during initiation of remdesivir and throughout treatment. Potential hepatotoxic agents must be identified early and, if possible, avoided in patients with elevated liver biochemistries.
Nirmatrelvir/ritonavir (Paxlovid) was approved in December 2021 for use in patients with mild-to-moderate COVID-19 symptoms who are at high risk of complications from COVID-19. Nirmatrelvir is an antiviral that prevents intracellular replication of SARS-CoV-2, and ritonavir inhibits cytochrome P450 3A to increase nirmatrelvir concentrations. This medication is most effective when given within the first 5 days of symptom onset. See StatPearls' companion reference, "Nirmatrelvir-ritonavir," for more information.
Patients with COVID-19 are associated with a hypercoagulable state, which puts them at risk of developing prothrombotic complications such as arterial and venous thrombosis. Clinicians should maintain a high index of suspicion for these complications and consider initiating appropriate systemic anticoagulation, provided there are no other contraindications to its initiation. Given that SARS-CoV-2 is an airborne pathogen, the aerosol-generating nature of endoscopy, and the potential for fecal-oral transmission, gastroenterologists, medical staff, and endoscopy staff are at increased risk of contracting or transmitting the virus. Implementing the precautions described below can prevent or reduce viral transmission.[37]
Precautions Against COVID-19 in the Endoscopy Suite
- Because endoscopy is an aerosol-generating procedure, all endoscopists, endoscopy staff, and anesthesia providers must wear full personal protective equipment (PPE): gowns, National Institute for Occupational Safety and Health (NIOSH)-approved N95 masks, and face shields for all endoscopies, and, preferably, a powered air-purifying respirator for positive COVID-19 cases.
- All endoscopies must be performed in negative-pressure rooms if available.
- All endoscopy unit staff must be trained in PPE donning/doffing and in the proper storage of PPE equipment.
- Placement of NIOSH-approved air filters in endoscopy rooms should be considered if possible.
- Before and after examination, frequent handwashing with soap and water for at least 20 seconds must be performed.
Differential Diagnosis
Although the GI symptoms are well-defined in patients with active COVID-19 infection, clinicians evaluating the patient must rule out other common etiologies of GI tract and liver disorders, including the following:
- GI tract etiologies that can cause similar symptoms include infectious diarrhea, ischemic colitis, inflammatory bowel disease, irritable bowel syndrome, small-bowel intestinal overgrowth, acute pancreatitis, chronic pancreatitis, acute cholecystitis, choledocholithiasis, and peptic ulcer disease.
- Hepatic etiologies that can cause elevated liver enzymes include acetaminophen toxicity, viral hepatitis (A, B, and C), drug-induced liver injury, ischemic hepatitis, primary biliary cholangitis, Budd-Chiari syndrome, sepsis-related hypotension, autoimmune hepatitis, cytomegalovirus, Epstein-Barr virus, or herpes simplex virus infections, and muscle-related disorders, such as polymyositis or rhabdomyolysis.
Prognosis
The prognosis of COVID-19 largely depends on various factors, including the severity of illness at presentation, associated comorbidities, and treatment response. Based on a large cohort study from China involving 44,415 patients, most (81%) were diagnosed with mild illness and had a favorable clinical course. The other 19% were diagnosed with severe to critical illness requiring hospitalization, of which 5% developed critical illness characterized by respiratory failure and multiorgan dysfunction.[38]
Many studies have reported that patients with COVID-19 infection who presented with primary GI-related symptoms or concurrent symptoms were at increased risk of hospitalization compared to those without GI symptoms.[1][2][3] However, this has not been comprehensively assessed, and more studies are needed. Acute liver failure is uncommon in patients with COVID-19. However, COVID-19 patients with liver injury on presentation are at significantly higher risk of admission to the intensive care unit and death.[20][31]
Complications
Considering the involvement of many major organ systems, COVID-19 can be regarded as a systemic viral illness. The complications of COVID-19 are likely due to progressive or sudden clinical deterioration leading to acute respiratory failure, acute respiratory distress syndrome, and multiorgan failure. Patients with COVID-19 illness are also increasingly being recognized as at risk of developing prothrombotic complications. Acute mesenteric ischemia is a life-threatening abdominal emergency associated with poor clinical outcomes.[36]
Results from a study found bowel wall abnormalities in 31% of abdominal computed tomography scans (mostly in patients in the intensive care unit), including pneumatosis and portal venous gas. Laparotomy and pathology confirmed small bowel ischemia in some of these patients, which was thought to be due to small vessel thrombosis.[4] These prothrombotic complications are likely attributable to the hypercoagulable state associated with this viral illness. Other complications, such as severe hepatitis, hemorrhagic colitis, and pancreatic necrosis, could be multifactorial in the setting of hypoxia, cytokine-induced inflammation, and hypoperfusion.[27][32]
Deterrence and Patient Education
Deterrence and prevention strategies are pivotal in mitigating the GI and hepatic manifestations of COVID-19. Patients should be advised to stay updated on the COVID-19 vaccination and get appropriate boosters as needed. Primary efforts should focus on public health education to enhance awareness of the virus's diverse presentations, including isolated GI symptoms. Emphasizing the importance of early reporting and seeking medical attention for such symptoms can aid in timely diagnosis and intervention. Given that the effectiveness of nirmatrelvir/ritonavir diminishes with more time elapsed since symptom onset, at-risk patients should be advised to seek medical care as soon as possible. Implementation of rigorous screening protocols, particularly for high-risk populations, can help identify cases early on.
Promoting hygienic practices and infection control measures remains crucial in preventing the spread of the virus, considering the potential for fecal-oral transmission. Given the possible fecal-oral transmission of SARS-CoV-2, clinical providers must educate and inform the patients and their close contacts about the fecal shedding of the virus and advise them to maintain contact precautions to prevent the spread of the virus. Patients must be educated about frequent handwashing with soap and water for at least 20 seconds when they come in contact with potentially contaminated surfaces. Collaborative efforts between healthcare professionals, public health agencies, and communities are essential to establish a comprehensive approach, ensuring effective deterrence and prevention of GI and hepatic complications associated with COVID-19.
Enhancing Healthcare Team Outcomes
Prevention and management of this highly contagious viral illness require a holistic, interprofessional approach that includes physicians across specialties, nurses, pharmacists, public health experts, and government authorities. The interprofessional team caring for individuals with COVID-19 on the front lines should consider assessing for gastrointestinal symptoms when evaluating patients suspected of COVID-19. Patients should be educated about the benefits of vaccination against the latest COVID-19 variants, in accordance with the National Institutes of Health/Centers for Disease Control guidelines.
The interprofessional team must educate patients and their close contacts about fecal shedding and maintain contact precautions to prevent viral spread. Healthcare systems must adopt the most up-to-date national infection control guidelines when treating patients in this group with atypical symptoms. Such a multi-pronged approach enhances patient care and outcomes while reducing the burden of hospitalizations that could strain healthcare resources. Such measures could significantly change the dynamics of healthcare infrastructure, go a long way toward eradicating this virus, and limit its devastating effects on socioeconomic and healthcare conditions globally.
Media
(Click Image to Enlarge)
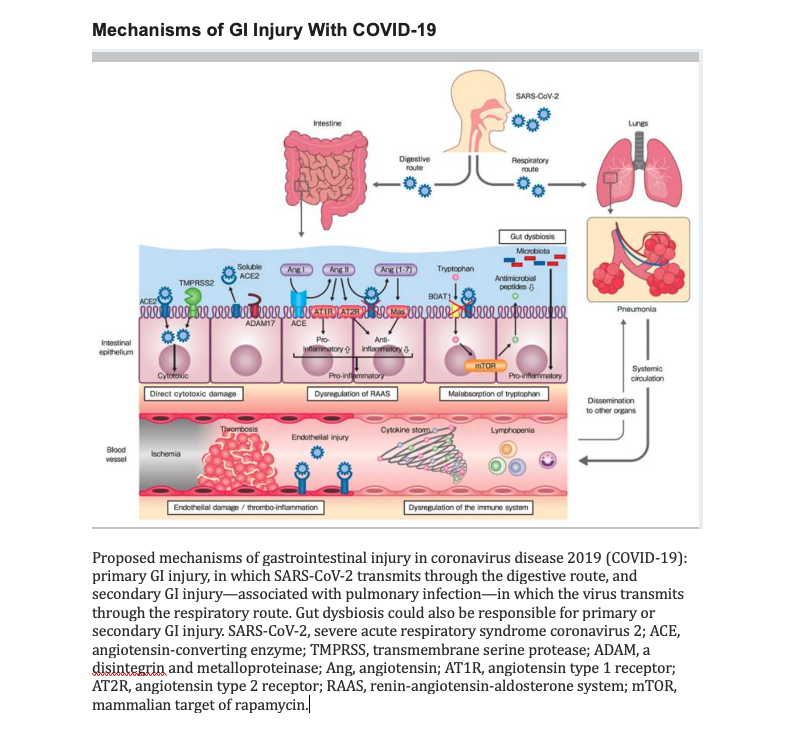
Mechanisms of Gastrointestinal Injury With COVID-19. Proposed mechanisms of GI injury in coronavirus disease 2019. The illustration depicts the primary GI injury, in which SARS-CoV-2 transmits through the digestive route, and the secondary GI injury—associated with pulmonary infection—in which the virus transmits through the respiratory route.
Mitsuyama K, Tsuruta K, Takedatsu H, Yoshioka S, Morita M, Niwa M, Matsumoto S. Clinical features and pathogenic mechanisms of gastrointestinal injury in COVID-19. J Clin Med. 2020;9(11):3630. doi: 10.3390/jcm9113630. (CC license 4.0)
References
Pan L, Mu M, Yang P, Sun Y, Wang R, Yan J, Li P, Hu B, Wang J, Hu C, Jin Y, Niu X, Ping R, Du Y, Li T, Xu G, Hu Q, Tu L. Clinical Characteristics of COVID-19 Patients With Digestive Symptoms in Hubei, China: A Descriptive, Cross-Sectional, Multicenter Study. The American journal of gastroenterology. 2020 May:115(5):766-773. doi: 10.14309/ajg.0000000000000620. Epub [PubMed PMID: 32287140]
Level 2 (mid-level) evidenceCholankeril G, Podboy A, Aivaliotis VI, Pham EA, Spencer SP, Kim D, Ahmed A. Association of Digestive Symptoms and Hospitalization in Patients With SARS-CoV-2 Infection. The American journal of gastroenterology. 2020 Jul:115(7):1129-1132. doi: 10.14309/ajg.0000000000000712. Epub [PubMed PMID: 32618665]
Mao R, Qiu Y, He JS, Tan JY, Li XH, Liang J, Shen J, Zhu LR, Chen Y, Iacucci M, Ng SC, Ghosh S, Chen MH. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: a systematic review and meta-analysis. The lancet. Gastroenterology & hepatology. 2020 Jul:5(7):667-678. doi: 10.1016/S2468-1253(20)30126-6. Epub 2020 May 12 [PubMed PMID: 32405603]
Level 2 (mid-level) evidenceMitsuyama K, Tsuruta K, Takedatsu H, Yoshioka S, Morita M, Niwa M, Matsumoto S. Clinical Features and Pathogenic Mechanisms of Gastrointestinal Injury in COVID-19. Journal of clinical medicine. 2020 Nov 11:9(11):. doi: 10.3390/jcm9113630. Epub 2020 Nov 11 [PubMed PMID: 33187280]
Pegoraro F, Trapani S, Indolfi G. Gastrointestinal, hepatic and pancreatic manifestations of COVID-19 in children. Clinics and research in hepatology and gastroenterology. 2022 Apr:46(4):101818. doi: 10.1016/j.clinre.2021.101818. Epub 2021 Oct 2 [PubMed PMID: 34607068]
Yuki K, Fujiogi M, Koutsogiannaki S. COVID-19 pathophysiology: A review. Clinical immunology (Orlando, Fla.). 2020 Jun:215():108427. doi: 10.1016/j.clim.2020.108427. Epub 2020 Apr 20 [PubMed PMID: 32325252]
Chan JF, Kok KH, Zhu Z, Chu H, To KK, Yuan S, Yuen KY. Genomic characterization of the 2019 novel human-pathogenic coronavirus isolated from a patient with atypical pneumonia after visiting Wuhan. Emerging microbes & infections. 2020:9(1):221-236. doi: 10.1080/22221751.2020.1719902. Epub 2020 Jan 28 [PubMed PMID: 31987001]
Sze S, Pan D, Nevill CR, Gray LJ, Martin CA, Nazareth J, Minhas JS, Divall P, Khunti K, Abrams KR, Nellums LB, Pareek M. Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine. 2020 Dec:29():100630. doi: 10.1016/j.eclinm.2020.100630. Epub 2020 Nov 12 [PubMed PMID: 33200120]
Level 2 (mid-level) evidenceHoffmann M, Kleine-Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, Müller MA, Drosten C, Pöhlmann S. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell. 2020 Apr 16:181(2):271-280.e8. doi: 10.1016/j.cell.2020.02.052. Epub 2020 Mar 5 [PubMed PMID: 32142651]
Xiao F, Tang M, Zheng X, Liu Y, Li X, Shan H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology. 2020 May:158(6):1831-1833.e3. doi: 10.1053/j.gastro.2020.02.055. Epub 2020 Mar 3 [PubMed PMID: 32142773]
Zou X, Chen K, Zou J, Han P, Hao J, Han Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Frontiers of medicine. 2020 Apr:14(2):185-192. doi: 10.1007/s11684-020-0754-0. Epub 2020 Mar 12 [PubMed PMID: 32170560]
Lin L, Jiang X, Zhang Z, Huang S, Zhang Z, Fang Z, Gu Z, Gao L, Shi H, Mai L, Liu Y, Lin X, Lai R, Yan Z, Li X, Shan H. Gastrointestinal symptoms of 95 cases with SARS-CoV-2 infection. Gut. 2020 Jun:69(6):997-1001. doi: 10.1136/gutjnl-2020-321013. Epub 2020 Apr 2 [PubMed PMID: 32241899]
Level 3 (low-level) evidenceEffenberger M, Grabherr F, Mayr L, Schwaerzler J, Nairz M, Seifert M, Hilbe R, Seiwald S, Scholl-Buergi S, Fritsche G, Bellmann-Weiler R, Weiss G, Müller T, Adolph TE, Tilg H. Faecal calprotectin indicates intestinal inflammation in COVID-19. Gut. 2020 Aug:69(8):1543-1544. doi: 10.1136/gutjnl-2020-321388. Epub 2020 Apr 20 [PubMed PMID: 32312790]
Ojetti V, Saviano A, Covino M, Acampora N, Troiani E, Franceschi F, GEMELLI AGAINST COVID‐19 group. COVID-19 and intestinal inflammation: Role of fecal calprotectin. Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2020 Nov:52(11):1231-1233. doi: 10.1016/j.dld.2020.09.015. Epub 2020 Sep 22 [PubMed PMID: 33060042]
Vodnar DC, Mitrea L, Teleky BE, Szabo K, Călinoiu LF, Nemeş SA, Martău GA. Coronavirus Disease (COVID-19) Caused by (SARS-CoV-2) Infections: A Real Challenge for Human Gut Microbiota. Frontiers in cellular and infection microbiology. 2020:10():575559. doi: 10.3389/fcimb.2020.575559. Epub 2020 Dec 9 [PubMed PMID: 33363049]
de Nies L, Galata V, Martin-Gallausiaux C, Despotovic M, Busi SB, Snoeck CJ, Delacour L, Budagavi DP, Laczny CC, Habier J, Lupu PC, Halder R, Fritz JV, Marques T, Sandt E, O'Sullivan MP, Ghosh S, Satagopam V, CON-VINCE Consortium, Krüger R, Fagherazzi G, Ollert M, Hefeng FQ, May P, Wilmes P. Altered infective competence of the human gut microbiome in COVID-19. Microbiome. 2023 Mar 9:11(1):46. doi: 10.1186/s40168-023-01472-7. Epub 2023 Mar 9 [PubMed PMID: 36894986]
Hoffmann D. The role of the oral cavity in SARS-CoV-2- and other viral infections. Clinical oral investigations. 2023 Jun:27(Suppl 1):15-22. doi: 10.1007/s00784-023-05078-z. Epub 2023 Jun 13 [PubMed PMID: 37310513]
Xu L, Liu J, Lu M, Yang D, Zheng X. Liver injury during highly pathogenic human coronavirus infections. Liver international : official journal of the International Association for the Study of the Liver. 2020 May:40(5):998-1004. doi: 10.1111/liv.14435. Epub 2020 Mar 30 [PubMed PMID: 32170806]
Bloom PP, Meyerowitz EA, Reinus Z, Daidone M, Gustafson J, Kim AY, Schaefer E, Chung RT. Liver Biochemistries in Hospitalized Patients With COVID-19. Hepatology (Baltimore, Md.). 2021 Mar:73(3):890-900. doi: 10.1002/hep.31326. Epub 2020 Nov 4 [PubMed PMID: 32415860]
Zhang C, Shi L, Wang FS. Liver injury in COVID-19: management and challenges. The lancet. Gastroenterology & hepatology. 2020 May:5(5):428-430. doi: 10.1016/S2468-1253(20)30057-1. Epub 2020 Mar 4 [PubMed PMID: 32145190]
Li J, Fan JG. Characteristics and Mechanism of Liver Injury in 2019 Coronavirus Disease. Journal of clinical and translational hepatology. 2020 Mar 28:8(1):13-17. doi: 10.14218/JCTH.2020.00019. Epub 2020 Mar 30 [PubMed PMID: 32274341]
Marjot T, Moon AM, Cook JA, Abd-Elsalam S, Aloman C, Armstrong MJ, Pose E, Brenner EJ, Cargill T, Catana MA, Dhanasekaran R, Eshraghian A, García-Juárez I, Gill US, Jones PD, Kennedy J, Marshall A, Matthews C, Mells G, Mercer C, Perumalswami PV, Avitabile E, Qi X, Su F, Ufere NN, Wong YJ, Zheng MH, Barnes E, Barritt AS 4th, Webb GJ. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. Journal of hepatology. 2021 Mar:74(3):567-577. doi: 10.1016/j.jhep.2020.09.024. Epub 2020 Oct 6 [PubMed PMID: 33035628]
Level 2 (mid-level) evidenceÖzdemir Ö, Arsoy HEM. Commentary on COVID-19-induced liver injury in various age and risk groups. World journal of virology. 2023 Jan 25:12(1):44-52. doi: 10.5501/wjv.v12.i1.44. Epub [PubMed PMID: 36743662]
Level 3 (low-level) evidenceLiptak P, Nosakova L, Rosolanka R, Skladany L, Banovcin P. Acute-on-chronic liver failure in patients with severe acute respiratory syndrome coronavirus 2 infection. World journal of hepatology. 2023 Jan 27:15(1):41-51. doi: 10.4254/wjh.v15.i1.41. Epub [PubMed PMID: 36744167]
McNabb-Baltar J, Jin DX, Grover AS, Redd WD, Zhou JC, Hathorn KE, McCarty TR, Bazarbashi AN, Shen L, Chan WW. Lipase Elevation in Patients With COVID-19. The American journal of gastroenterology. 2020 Aug:115(8):1286-1288. doi: 10.14309/ajg.0000000000000732. Epub [PubMed PMID: 32496339]
Fignani D, Licata G, Brusco N, Nigi L, Grieco GE, Marselli L, Overbergh L, Gysemans C, Colli ML, Marchetti P, Mathieu C, Eizirik DL, Sebastiani G, Dotta F. SARS-CoV-2 Receptor Angiotensin I-Converting Enzyme Type 2 (ACE2) Is Expressed in Human Pancreatic β-Cells and in the Human Pancreas Microvasculature. Frontiers in endocrinology. 2020:11():596898. doi: 10.3389/fendo.2020.596898. Epub 2020 Nov 13 [PubMed PMID: 33281748]
Lax SF, Skok K, Zechner P, Kessler HH, Kaufmann N, Koelblinger C, Vander K, Bargfrieder U, Trauner M. Pulmonary Arterial Thrombosis in COVID-19 With Fatal Outcome : Results From a Prospective, Single-Center, Clinicopathologic Case Series. Annals of internal medicine. 2020 Sep 1:173(5):350-361. doi: 10.7326/M20-2566. Epub 2020 May 14 [PubMed PMID: 32422076]
Level 2 (mid-level) evidenceVarga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, Zinkernagel AS, Mehra MR, Schuepbach RA, Ruschitzka F, Moch H. Endothelial cell infection and endotheliitis in COVID-19. Lancet (London, England). 2020 May 2:395(10234):1417-1418. doi: 10.1016/S0140-6736(20)30937-5. Epub 2020 Apr 21 [PubMed PMID: 32325026]
Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, Liu S, Zhao P, Liu H, Zhu L, Tai Y, Bai C, Gao T, Song J, Xia P, Dong J, Zhao J, Wang FS. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. The Lancet. Respiratory medicine. 2020 Apr:8(4):420-422. doi: 10.1016/S2213-2600(20)30076-X. Epub 2020 Feb 18 [PubMed PMID: 32085846]
Dorrell RD, Dougherty MK, Barash EL, Lichtig AE, Clayton SB, Jensen ET. Gastrointestinal and hepatic manifestations of COVID-19: A systematic review and meta-analysis. JGH open : an open access journal of gastroenterology and hepatology. 2021 Jan:5(1):107-115. doi: 10.1002/jgh3.12456. Epub 2020 Nov 21 [PubMed PMID: 33363257]
Level 1 (high-level) evidenceHajifathalian K, Krisko T, Mehta A, Kumar S, Schwartz R, Fortune B, Sharaiha RZ, WCM-GI research group∗. Gastrointestinal and Hepatic Manifestations of 2019 Novel Coronavirus Disease in a Large Cohort of Infected Patients From New York: Clinical Implications. Gastroenterology. 2020 Sep:159(3):1137-1140.e2. doi: 10.1053/j.gastro.2020.05.010. Epub 2020 May 8 [PubMed PMID: 32389667]
Carvalho A, Alqusairi R, Adams A, Paul M, Kothari N, Peters S, DeBenedet AT. SARS-CoV-2 Gastrointestinal Infection Causing Hemorrhagic Colitis: Implications for Detection and Transmission of COVID-19 Disease. The American journal of gastroenterology. 2020 Jun:115(6):942-946. doi: 10.14309/ajg.0000000000000667. Epub [PubMed PMID: 32496741]
Parasa S, Desai M, Thoguluva Chandrasekar V, Patel HK, Kennedy KF, Roesch T, Spadaccini M, Colombo M, Gabbiadini R, Artifon ELA, Repici A, Sharma P. Prevalence of Gastrointestinal Symptoms and Fecal Viral Shedding in Patients With Coronavirus Disease 2019: A Systematic Review and Meta-analysis. JAMA network open. 2020 Jun 1:3(6):e2011335. doi: 10.1001/jamanetworkopen.2020.11335. Epub 2020 Jun 1 [PubMed PMID: 32525549]
Level 1 (high-level) evidenceFix OK, Hameed B, Fontana RJ, Kwok RM, McGuire BM, Mulligan DC, Pratt DS, Russo MW, Schilsky ML, Verna EC, Loomba R, Cohen DE, Bezerra JA, Reddy KR, Chung RT. Clinical Best Practice Advice for Hepatology and Liver Transplant Providers During the COVID-19 Pandemic: AASLD Expert Panel Consensus Statement. Hepatology (Baltimore, Md.). 2020 Jul:72(1):287-304. doi: 10.1002/hep.31281. Epub [PubMed PMID: 32298473]
Level 3 (low-level) evidenceSultan S, Altayar O, Siddique SM, Davitkov P, Feuerstein JD, Lim JK, Falck-Ytter Y, El-Serag HB, AGA Institute. Electronic address: ewilson@gastro.org. AGA Institute Rapid Review of the Gastrointestinal and Liver Manifestations of COVID-19, Meta-Analysis of International Data, and Recommendations for the Consultative Management of Patients with COVID-19. Gastroenterology. 2020 Jul:159(1):320-334.e27. doi: 10.1053/j.gastro.2020.05.001. Epub 2020 May 11 [PubMed PMID: 32407808]
Level 1 (high-level) evidenceParry AH, Wani AH, Yaseen M. Acute Mesenteric Ischemia in Severe Coronavirus-19 (COVID-19): Possible Mechanisms and Diagnostic Pathway. Academic radiology. 2020 Aug:27(8):1190. doi: 10.1016/j.acra.2020.05.016. Epub 2020 May 23 [PubMed PMID: 32475635]
Thompson CC, Shen L, Lee LS. COVID-19 in endoscopy: Time to do more? Gastrointestinal endoscopy. 2020 Aug:92(2):435-439. doi: 10.1016/j.gie.2020.03.3848. Epub 2020 Mar 29 [PubMed PMID: 32234312]
Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020 Apr 7:323(13):1239-1242. doi: 10.1001/jama.2020.2648. Epub [PubMed PMID: 32091533]
Level 3 (low-level) evidence