Introduction
Doppler liver ultrasonography is an effective, noninvasive method for evaluating the hepatic vasculature. Understanding the normal and abnormal waveforms of the primary hepatic vessels and their characteristic patterns can help diagnose specific diseases that have characteristic effects on these patterns. Understanding how an abnormal hepatic artery, hepatic vein, or portal vein manifests on Doppler sonography can help identify or confirm liver diseases.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The liver plays a vital role in the body's metabolic functions and is composed of a relatively complex vascular architecture.[1] One-quarter of the cardiac output goes to the liver.[2] The liver is divided into various hepatic segments, and each hepatic lobule receives a branch of the portal vein, hepatic artery, and biliary tract, collectively called the portal triad.[3] These branches involve the following anatomic structures:
- Portal vein: The portal vein constitutes 75% of the hepatic blood supply. The blood from the portal vein is deoxygenated and carries mainly nutrients. The portal vein is formed by the confluence of the superior mesenteric and the splenic veins. The portal vein drains all the upper and middle parts of the gastrointestinal tract, pancreas, gallbladder, and spleen.[4] Within the liver, the portal is divided into 2 branches: the left and the right portal veins. The left supplies segments II, III, and IV, while the right portal vein supplies segments V, VIII, VI, and VII. Variants of the portal venous system are not uncommon.[5]
- Hepatic veins: The hepatic veins are 3 branches (right, left, and middle) that drain blood into the inferior vena cava (IVC).[6] The most common hepatic venous morphology includes a right hepatic vein and a common trunk for the middle and left hepatic veins.[7]
- Hepatic artery: The hepatic artery supplies 25% of the hepatic blood flow and constitutes the main bulk of oxygenated blood to the liver.[2] Frequent variations of the origin of the hepatic artery exist, with the most common type constituting the common hepatic artery arising from the celiac artery in 70% of patients.[8]
- Inferior vena cava: The IVC represents the confluence of the right and left common iliac veins and is the retroperitoneal draining vessel to the hepatic veins. The IVC subsequently empties deoxygenated blood to the right heart.[9]
Hepatopetal and Hepatofugal Flow
Hepatopetal flow refers to blood flow towards the liver (from the portal hepatis to the liver periphery). Hepatopetal flow is typically used to describe the normal blood flow direction in the portal vein.[10] This occurs in a normal liver and allows it to detoxify the blood entering it after it absorbs nutrients from the intestine via the portal vein.
Hepatofugal flow refers to blood flow away from the liver in the portal vein and is sometimes referred to as "retrograde" flow. In other words, the portal venous blood flow pattern is from the periphery of the liver towards the porta hepatis.[10] This occurs when the portal venous pressure is high in the case of portal hypertension (see Image. Portal Hypertension). Thus, portosystemic shunts are reopened, with additional findings including a more narrowed portal vein and prominence of the hepatic artery.[11] Occasionally, a to-and-fro bidirectional blood flow pattern alternating between hepatopetal and hepatofugal flow can be seen in the portal vein before the onset of frank hepatofugal flow.[12]
While HVPG (hepatic venous pressure gradient) is the gold standard for measuring portal and hepatic venous pressures, it requires catheterization of the hepatic vessels.[13] On the other hand, Doppler ultrasound is a noninvasive procedure and can evaluate for abnormal physiology of the hepatic vasculature.
Indications
Liver Posttransplantation Assessment
Hepatic Doppler is used for the early detection of vascular occlusion or graft rejection and is the preferred follow-up method due to its low cost and noninvasiveness.[14] Sonographic assessment of a posttransplant liver includes a gray-scale evaluation of the hepatic parenchyma and the hepatic biliary tree. Doppler evaluation of the hepatic vasculature involves both gray-scale and Doppler assessment. Evaluation of strictures can reveal varying degrees of vessel narrowing.[15]
Thrombus formation in the portal vein and IVC can be evaluated with both gray-scale and Doppler imaging (see Image. Portal Vein Thrombosis). A normal hepatic artery will demonstrate a rapid systolic upstroke lasting up to 80 milliseconds. The resistive index of the hepatic artery, calculated as the ratio of peak systemic velocity minus peak diastolic velocity divided by peak systolic velocity, should be between 0.5 and 0.7.[15] In the setting of posttransplant evaluation, the portal vein should demonstrate a continuous hepatopetal flow pattern with only mild velocity variations on inspiration and expiration. Hepatic veins and the IVC should demonstrate a phasic flow pattern corresponding to the cardiac cycle.[15]
Diagnosis of Portal Hypertension and Patency of Collaterals
Cirrhosis and alterations in portal hemodynamics ultimately increase the portal venous pressure gradient, leading to abnormal portal venous blood flow away from the liver.[16] Doppler ultrasonography can assess blood flow direction and evaluate the presence of collateral vessels. Doppler indices include portal and splenic venous velocities, flow directions, and resistive/pulsatility indices of the arterial vasculature.[17]
Additional strengths of Doppler assessment include real-time observation, while limitations include a poor detection of slow blood flow and a reduced frame rate.[18] Other useful parameters in the diagnosis of cirrhosis include liver and spleen size, evaluation of liver echotexture, and evaluation of the bluntness of the liver edge.[19] The normal portal vein pressure is less than 6 mm Hg. Portal hypertension is clinically manifested when this pressure exceeds 12 mm Hg.
Diagnosis of Budd Chiari Syndrome
Budd-Chiari syndrome is an outflow obstruction of the hepatic veins, most commonly secondary to a prothrombotic disorder.[20] Doppler in Budd-Chiari syndrome is diagnosed by occlusion of hepatic venous outflow, either by stenosis or thrombosis of the hepatic veins or the higher-draining inferior vena cava. Doppler in Budd-Chiari syndrome is performed by measuring the flow direction and velocity, as well as the vessel diameter.[21]
Nonvisualization of the hepatic venous vasculature is often noted on Doppler color ultrasound. A fibrous cord, a luminal thrombus, and stenosis are present.[22] Collaterals can also be seen in a spiderweb morphology, often extending to the inferior vena cava or other hepatic veins.
Diagnosis and Follow-Up of Thrombosis
Chronic thrombus formation can occur in the portal veins, hepatic veins, or the inferior vena cava. Thrombosis appears as an absent signal on color Doppler evaluation. The gold standard for diagnosing vessel thrombosis is angiography of the suspected vessel, but angiography is an invasive procedure.[23] In chronic thrombosis, collaterals begin to form alongside recanalization of the obstructed vessel. Portal vein thrombosis could be due to benign obstruction of the portal vein (caused by the over-coagulable state, slow blood flow, or vascular injury) or malignant obstruction (caused by infiltration of the endovascular lining of the vessel).[24]
Evaluation of a Transjugular Intrahepatic Portosystemic Shunt Stent
The transjugular intrahepatic portosystemic shunt (TIPS) procedure is a treatment option for patients with cirrhosis or noncirrhotic total hypertension. TIPS shunts function to treat those who suffer from refractory ascites and variceal bleeding.[25] TIPS dysfunction has a high incidence and can be secondary to malpositioning, thrombosis, and pseudointimal hyperplasia.[26] Ultrasound can assess TIPS velocities (typically 90 to 190 cm/s), portal venous blood velocity before entering the shunt (normal is around 30 cm/s), waveforms, and the presence of stenosis.[27]
Assessment of Hemodynamics of Hepatic Focal Lesions
Doppler evaluation can be used in the assessment of benign hemangiomas and telangiectasia.[28] Hypoechoic hepatic focal lesions may be detected during screening of high-risk populations for hepatocellular carcinoma. The lesions may be associated with enlarged portal hepatic lymph nodes or para-aortic lymph nodes in metastasis. The vascular flow on color Doppler around the focal lesion can be evaluated for neovascularization.[29][30]
Hemodynamics in Heart Failure
Doppler ultrasound can also be utilized to assess heart failure. Heart failure can result in hepatic venous congestion and retrograde flow, inferior vena cava congestion with dilated diameters of the vessels, and increased portal vein pulsatility.[31]
Contraindications
Doppler ultrasound of the liver is a noninvasive procedure that has no contraindications.
Equipment
Doppler ultrasound for abdominal examination includes 2 modalities: pulsed Doppler and color Doppler. Continuous Doppler, commonly used to evaluate high-frequency flow in cardiac valves and vascular structures, is not well suited for assessing the portal veins, hepatic veins, or inferior vena cava.
Personnel
Usually, Doppler ultrasound is performed by an experienced sonographer, either a radiologist or a gastroenterologist.
Preparation
Fasting is preferred (4 to 6 hours before the examination) to reduce gaseous distension and abdominal fluid, thereby increasing the visibility of the vessels.[32] Before starting the examination, adjusting the device's gain, frequency, and depth is crucial.[33][34]
Technique or Treatment
General Doppler Ultrasound Technique
Incorporating hepatic Doppler ultrasound into a standard abdominal ultrasound enhances operator proficiency by improving probe manipulation and facilitating clearer visualization of hepatic vasculature. The combined use of abdominal ultrasound and hepatic Doppler does not substantially increase examination time.
Patient breath-holding may improve image quality during vascular assessment.[35] On most ultrasound systems, red color coding indicates blood flow toward the probe, while blue indicates flow away from the probe. The portal vein demonstrates a thick fibrous wall, appearing as an echogenic line surrounding the vessel, whereas hepatic vein walls remain thin and often not visualized. Portal vein diameter typically ranges from 7 to 15 mm, hepatic vein diameter from 5 to 7 mm, and inferior vena cava diameter from 13 to 22 mm, with normal collapsibility under pressure.[36][37]
Optimal patient positioning includes supine or left lateral decubitus positioning. Initial scanning in the right subcostal region enables visualization of the portal vein, with the confluence of the splenic and superior mesenteric veins identified as the probe is moved left toward the midline. Substernal scanning allows visualization of the inferior vena cava, which should appear compressible, along with the aorta in the midline using a posteriorly directed probe in longitudinal or transverse orientation. Hepatic veins are best assessed from the right intercostal approach with medial probe orientation to evaluate drainage of all 3 hepatic veins into the inferior vena cava. Additional visualization of the hepatic veins may be achieved via the subcostal approach with a posterior probe orientation, while the left and middle hepatic veins are optimally assessed from the substernal window.
Limitations
Obesity may limit visualization of vessel flow and velocity during Doppler assessment. Postprandial states may increase portal pressure and widen the vessel diameter, while ingested contents and associated gaseous distension can further impede clear visualization of hepatic vessels. Fasting for at least 4 to 6 hours before Doppler examination improves imaging quality and diagnostic accuracy.
Incorrect device settings, including improper adjustment of gain and frequency, may lead to inaccurate interpretation of hepatic hemodynamics. Low-frequency settings may lead to false-positive identification of portal vein thrombosis. Inadequate breath-holding capacity may also hinder vessel visualization; however, synchronization of probe movement with patient inhalation can help mitigate this limitation and improve image acquisition.
Clinical Significance
Hepatic Doppler ultrasound is a noninvasive investigative tool that can help clinicians, especially when added to an abdominal ultrasound exam. The procedure is cost-effective and has no complications. Doppler ultrasound is the preferred imaging modality for assessing the vascular condition in the following diseases:
- Portal hypertension associated with cirrhosis
- Portal or hepatic vein thrombosis (see Image. Ultrasound of Portal Vein Thrombosis) [38]
- Vascularity of the hepatic focal lesions [39]
- Follow-up after TIPS or liver transplantation [40]
- Measuring the hepatic vein and artery patency, blood velocity, and direction
Referral to other invasive investigative or treatment procedures, eg, hepatic venous pressure gradient HVPG, angiography, transjugular intrahepatic portosystemic shunt TIPS, and other procedures, depends on initial assessment on Doppler ultrasound. In a study comparing rats with fatty liver disease to normal rats, no significant difference was observed between the 2 groups in portal vein diameter and flow, and a normal increase in diameter in both groups with meals was observed.[41]
Furthermore, a study on 120 patients found that portal vein diameter and splenic area were inversely correlated to the platelet count, where the platelet count is a strong indicator of liver fibrosis as shown by histopathological score (Ishak score) [42] A recent meta-analysis and a systematic review found that on comparing hepatic vein resistive index versus hepatic artery resistive index, that the former had a higher diagnostic accuracy in detecting liver fibrosis of F2 or greater (indicating liver fibrosis stage of moderate scarring in the liver, with bands of scar tissue forming but no cirrhosis) as diagnosed by liver biopsy.[43]
A study on 94 patients with hepatitis B virus infection showed that as the liver inflammation increased, the diameter of the portal vein increased while its velocity decreased; moreover, as the degree of liver fibrosis increased, the diameter of the portal vein increased, while its velocity decreased, associated with decreased velocity of the superior mesenteric and splenic veins. A flat or unidirectional flow of the hepatic veins accompanies this. Thus, Doppler ultrasound of the liver may be more useful than conventional abdominal ultrasound for noninvasive assessment of the degree of liver fibrosis.[44]
Enhancing Healthcare Team Outcomes
Doppler liver ultrasonography serves as a noninvasive, cost-effective modality for evaluating hepatic vascular anatomy, blood flow direction, and hemodynamic abnormalities associated with liver disease. Assessment of portal venous, hepatic venous, hepatic arterial, and inferior vena cava waveforms assists in diagnosing portal hypertension, portal or hepatic vein thrombosis, Budd-Chiari syndrome, hepatic congestion from heart failure, and complications following liver transplantation or TIPS placement. Recognition of hepatopetal and hepatofugal flow patterns, vessel patency, resistive indices, and abnormal waveform morphology improves diagnostic accuracy and supports timely intervention. Doppler ultrasonography also aids in evaluating focal hepatic lesions, monitoring progression of fibrosis, and guiding referral for invasive procedures such as angiography, hepatic venous pressure gradient measurement, or TIPS revision. Technical factors, including patient positioning, fasting status, respiratory motion, obesity, and equipment settings, significantly influence image quality and interpretation.
Interprofessional collaboration strengthens diagnostic precision, patient safety, and longitudinal management of hepatic vascular disorders. Radiologists, hepatologists, gastroenterologists, transplant surgeons, primary care clinicians, and advanced practitioners coordinate evaluation, interpretation of Doppler findings, and selection of appropriate follow-up testing or intervention. Nurses reinforce patient preparation instructions, monitor procedural tolerance, and facilitate communication across care teams. Pharmacists assist with anticoagulation management, medication reconciliation, and prevention of drug-related hepatic complications. Sonographers optimize image acquisition and recognize abnormal flow patterns requiring urgent escalation. Shared decision-making promotes patient understanding of diagnostic findings, surveillance strategies, transplant follow-up, and risk reduction measures, while timely referral and coordinated monitoring reduce complications such as graft failure, progressive portal hypertension, and thrombotic events.
Media
(Click Image to Enlarge)

Portal Hypertension. B-mode ultrasound demonstrating a main portal vein diameter of 15.1 millimeters. This finding is suggestive of portal hypertension.
Contributed by B Covello, MD
(Click Image to Enlarge)
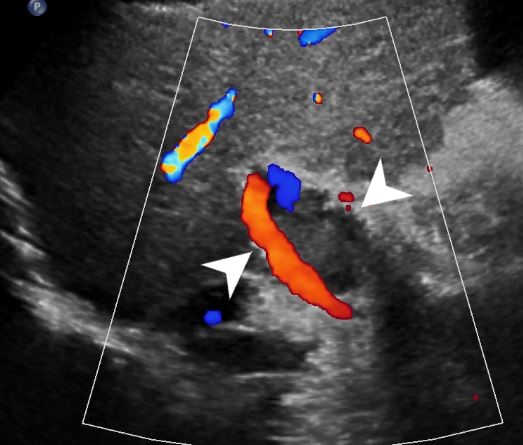
Ultrasound of Portal Vein Thrombosis. Ultrasound imaging demonstrating thrombosis of the portal vein.
Contributed by D Tafti, MD
(Click Image to Enlarge)
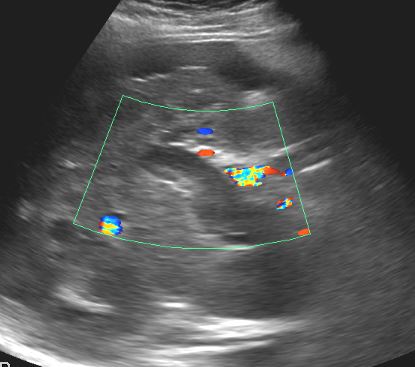
Portal Vein Thrombosis. Thrombus formation in the portal vein and IVC can be evaluated on both gray-scale and Doppler assessments.
Contributed by D Tafti, MD
References
Torres Rojas AM, Lorente S, Hautefeuille M, Sanchez-Cedillo A. Hierarchical Modeling of the Liver Vascular System. Frontiers in physiology. 2021:12():733165. doi: 10.3389/fphys.2021.733165. Epub 2021 Nov 16 [PubMed PMID: 34867439]
Eipel C, Abshagen K, Vollmar B. Regulation of hepatic blood flow: the hepatic arterial buffer response revisited. World journal of gastroenterology. 2010 Dec 28:16(48):6046-57 [PubMed PMID: 21182219]
Couinaud C. Liver anatomy: portal (and suprahepatic) or biliary segmentation. Digestive surgery. 1999:16(6):459-67 [PubMed PMID: 10805544]
Level 3 (low-level) evidenceCarneiro C, Brito J, Bilreiro C, Barros M, Bahia C, Santiago I, Caseiro-Alves F. All about portal vein: a pictorial display to anatomy, variants and physiopathology. Insights into imaging. 2019 Mar 21:10(1):38. doi: 10.1186/s13244-019-0716-8. Epub 2019 Mar 21 [PubMed PMID: 30900187]
Level 3 (low-level) evidenceSchmidt S, Demartines N, Soler L, Schnyder P, Denys A. Portal vein normal anatomy and variants: implication for liver surgery and portal vein embolization. Seminars in interventional radiology. 2008 Jun:25(2):86-91. doi: 10.1055/s-2008-1076688. Epub [PubMed PMID: 21326549]
Hardy KJ. The hepatic veins. The Australian and New Zealand journal of surgery. 1972 Aug:42(1):11-4 [PubMed PMID: 4512537]
Fang CH, You JH, Lau WY, Lai EC, Fan YF, Zhong SZ, Li KX, Chen ZX, Su ZH, Bao SS. Anatomical variations of hepatic veins: three-dimensional computed tomography scans of 200 subjects. World journal of surgery. 2012 Jan:36(1):120-4. doi: 10.1007/s00268-011-1297-y. Epub [PubMed PMID: 21976007]
Marchal G, Kint E, Nijssens M, Baert AL. Variability of the hepatic arterial anatomy: a sonographic demonstration. Journal of clinical ultrasound : JCU. 1981 Sep:9(7):377-81 [PubMed PMID: 6792236]
Tucker WD, Shrestha R, Burns B. Anatomy, Abdomen and Pelvis: Inferior Vena Cava. StatPearls. 2026 Jan:(): [PubMed PMID: 29493975]
McNaughton DA, Abu-Yousef MM. Doppler US of the liver made simple. Radiographics : a review publication of the Radiological Society of North America, Inc. 2011 Jan-Feb:31(1):161-88. doi: 10.1148/rg.311105093. Epub [PubMed PMID: 21257940]
Ralls PW. Color Doppler sonography of the hepatic artery and portal venous system. AJR. American journal of roentgenology. 1990 Sep:155(3):517-25 [PubMed PMID: 2117348]
Level 2 (mid-level) evidenceWachsberg RH, Bahramipour P, Sofocleous CT, Barone A. Hepatofugal flow in the portal venous system: pathophysiology, imaging findings, and diagnostic pitfalls. Radiographics : a review publication of the Radiological Society of North America, Inc. 2002 Jan-Feb:22(1):123-40 [PubMed PMID: 11796903]
Suk KT. Hepatic venous pressure gradient: clinical use in chronic liver disease. Clinical and molecular hepatology. 2014 Mar:20(1):6-14. doi: 10.3350/cmh.2014.20.1.6. Epub 2014 Mar 26 [PubMed PMID: 24757653]
Kimura Y, Tapia Sosa R, Soto-Trujillo D, Kimura Sandoval Y, Casian C. Liver Transplant Complications Radiologist Can't Miss. Cureus. 2020 Jun 5:12(6):e8465. doi: 10.7759/cureus.8465. Epub 2020 Jun 5 [PubMed PMID: 32642371]
Crossin JD, Muradali D, Wilson SR. US of liver transplants: normal and abnormal. Radiographics : a review publication of the Radiological Society of North America, Inc. 2003 Sep-Oct:23(5):1093-114 [PubMed PMID: 12975502]
Kim MY, Jeong WK, Baik SK. Invasive and non-invasive diagnosis of cirrhosis and portal hypertension. World journal of gastroenterology. 2014 Apr 21:20(15):4300-15. doi: 10.3748/wjg.v20.i15.4300. Epub [PubMed PMID: 24764667]
Baik SK. Haemodynamic evaluation by Doppler ultrasonography in patients with portal hypertension: a review. Liver international : official journal of the International Association for the Study of the Liver. 2010 Nov:30(10):1403-13. doi: 10.1111/j.1478-3231.2010.02326.x. Epub 2010 Aug 19 [PubMed PMID: 20731772]
Maruyama H, Yokosuka O. Ultrasonography for Noninvasive Assessment of Portal Hypertension. Gut and liver. 2017 Jul 15:11(4):464-473. doi: 10.5009/gnl16078. Epub [PubMed PMID: 28267700]
Colli A, Fraquelli M, Andreoletti M, Marino B, Zuccoli E, Conte D. Severe liver fibrosis or cirrhosis: accuracy of US for detection--analysis of 300 cases. Radiology. 2003 Apr:227(1):89-94 [PubMed PMID: 12601199]
Level 3 (low-level) evidenceBargalló X, Gilabert R, Nicolau C, García-Pagán JC, Ayuso JR, Brú C. Sonography of Budd-Chiari syndrome. AJR. American journal of roentgenology. 2006 Jul:187(1):W33-41 [PubMed PMID: 16794137]
Valla DC. Budd-Chiari syndrome/hepatic venous outflow tract obstruction. Hepatology international. 2018 Feb:12(Suppl 1):168-180. doi: 10.1007/s12072-017-9810-5. Epub 2017 Jul 6 [PubMed PMID: 28685257]
Chaubal N, Dighe M, Hanchate V, Thakkar H, Deshmukh H, Rathod K. Sonography in Budd-Chiari syndrome. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2006 Mar:25(3):373-9 [PubMed PMID: 16495498]
Manzano-Robleda Mdel C, Barranco-Fragoso B, Uribe M, Méndez-Sánchez N. Portal vein thrombosis: what is new? Annals of hepatology. 2015 Jan-Feb:14(1):20-7 [PubMed PMID: 25536638]
Chawla YK, Bodh V. Portal vein thrombosis. Journal of clinical and experimental hepatology. 2015 Mar:5(1):22-40. doi: 10.1016/j.jceh.2014.12.008. Epub 2015 Jan 6 [PubMed PMID: 25941431]
Foshager MC, Ferral H, Nazarian GK, Castañeda-Zúñiga WR, Letourneau JG. Duplex sonography after transjugular intrahepatic portosystemic shunts (TIPS): normal hemodynamic findings and efficacy in predicting shunt patency and stenosis. AJR. American journal of roentgenology. 1995 Jul:165(1):1-7 [PubMed PMID: 7785564]
Cura M, Cura A, Suri R, El-Merhi F, Lopera J, Kroma G. Causes of TIPS dysfunction. AJR. American journal of roentgenology. 2008 Dec:191(6):1751-7. doi: 10.2214/AJR.07.3534. Epub [PubMed PMID: 19020247]
Benito A, Bilbao J, Hernández T, Martinez-Cuesta A, Larrache J, González I, Vivas I. Doppler ultrasound for TIPS: does it work? Abdominal imaging. 2004 Jan-Feb:29(1):45-52 [PubMed PMID: 15160753]
Naganuma H, Ishida H, Kuroda H, Suzuki Y, Ogawa M. Hereditary hemorrhagic telangiectasia: how to efficiently detect hepatic abnormalities using ultrasonography. Journal of medical ultrasonics (2001). 2020 Jul:47(3):421-433. doi: 10.1007/s10396-020-01022-w. Epub 2020 May 10 [PubMed PMID: 32390074]
Kang HJ, Lee JM, Jeon SK, Ryu H, Yoo J, Lee JK, Han JK. Microvascular Flow Imaging of Residual or Recurrent Hepatocellular Carcinoma after Transarterial Chemoembolization: Comparison with Color/Power Doppler Imaging. Korean journal of radiology. 2019 Jul:20(7):1114-1123. doi: 10.3348/kjr.2018.0932. Epub [PubMed PMID: 31270975]
Maruyama H, Yoshikawa M, Yokosuka O. Current role of ultrasound for the management of hepatocellular carcinoma. World journal of gastroenterology. 2008 Mar 21:14(11):1710-9 [PubMed PMID: 18350602]
Jefkins M, Chan B. Hepatic and portal vein Dopplers in the clinical management of patients with right-sided heart failure: two case reports. The ultrasound journal. 2019 Nov 12:11(1):30. doi: 10.1186/s13089-019-0146-3. Epub 2019 Nov 12 [PubMed PMID: 31748951]
Level 3 (low-level) evidenceAfif AM, Chang JP, Wang YY, Lau SD, Deng F, Goh SY, Pwint MK, Ooi CC, Venkatanarasimha N, Lo RH. A sonographic Doppler study of the hepatic vein, portal vein and hepatic artery in liver cirrhosis: Correlation of hepatic hemodynamics with clinical Child Pugh score in Singapore. Ultrasound (Leeds, England). 2017 Nov:25(4):213-221. doi: 10.1177/1742271X17721265. Epub 2017 Aug 3 [PubMed PMID: 29163657]
Carovac A, Smajlovic F, Junuzovic D. Application of ultrasound in medicine. Acta informatica medica : AIM : journal of the Society for Medical Informatics of Bosnia & Herzegovina : casopis Drustva za medicinsku informatiku BiH. 2011 Sep:19(3):168-71. doi: 10.5455/aim.2011.19.168-171. Epub [PubMed PMID: 23408755]
Kurzweil A, Martin J. Transabdominal Ultrasound. StatPearls. 2026 Jan:(): [PubMed PMID: 30521234]
Macnaught F, Campbell-Rogers N. The liver: how we do it. Australasian journal of ultrasound in medicine. 2009 Aug:12(3):44-47. doi: 10.1002/j.2205-0140.2009.tb00061.x. Epub 2015 Dec 31 [PubMed PMID: 28191063]
Geleto G, Getnet W, Tewelde T. Mean Normal Portal Vein Diameter Using Sonography among Clients Coming to Radiology Department of Jimma University Hospital, Southwest Ethiopia. Ethiopian journal of health sciences. 2016 May:26(3):237-42 [PubMed PMID: 27358544]
Patil S, Jadhav S, Shetty N, Kharge J, Puttegowda B, Ramalingam R, Cholenahally MN. Assessment of inferior vena cava diameter by echocardiography in normal Indian population: A prospective observational study. Indian heart journal. 2016 Dec:68 Suppl 3(Suppl 3):S26-S30. doi: 10.1016/j.ihj.2016.06.009. Epub 2016 Jul 1 [PubMed PMID: 28038721]
Level 2 (mid-level) evidenceFrancoz C, Valla D, Durand F. Portal vein thrombosis, cirrhosis, and liver transplantation. Journal of hepatology. 2012 Jul:57(1):203-12. doi: 10.1016/j.jhep.2011.12.034. Epub 2012 Mar 21 [PubMed PMID: 22446690]
Tanaka H. Current role of ultrasound in the diagnosis of hepatocellular carcinoma. Journal of medical ultrasonics (2001). 2020 Apr:47(2):239-255. doi: 10.1007/s10396-020-01012-y. Epub 2020 Mar 13 [PubMed PMID: 32170489]
Ricci P, Cantisani V, Lombardi V, Alfano G, D'Ambrosio U, Menichini G, Marotta E, Drudi FM. Is color-Doppler US a reliable method in the follow-up of transjugular intrahepatic portosystemic shunt (TIPS)? Journal of ultrasound. 2007 Mar:10(1):22-7. doi: 10.1016/j.jus.2007.02.005. Epub 2007 Apr 16 [PubMed PMID: 23396711]
Alqawasmi M, Lin H, Kanagy N, Birg A. Detecting Portal Venous Blood Flow in Metabolic Dysfunction-Associated Fatty Liver Disease Using Non-Invasive Doppler Ultrasound. Cureus. 2025 Jul:17(7):e88446. doi: 10.7759/cureus.88446. Epub 2025 Jul 21 [PubMed PMID: 40842749]
Boccatonda A, Garlisi MC, Brighenti A, Musmeci M, Masi L, Bakken SM, Serra C. Platelet and Doppler ultrasound signatures of histological fibrosis in chronic liver disease: a correlation study based on Ishak staging. Journal of ultrasound. 2026 Jun:29(2):317-323. doi: 10.1007/s40477-026-01126-y. Epub 2026 Feb 22 [PubMed PMID: 41724905]
Nmai RA, Wiafe YA, Donkor A, Anyitey-Kokor IC, Adu-Bredu TK, Antwi SO, Roberts LR. Diagnostic accuracy of Doppler Sonography of hepatic blood vessels in the detection of significant liver fibrosis: a systematic review and meta-analysis. Journal of ultrasound. 2026 Mar:29(1):13-24. doi: 10.1007/s40477-026-01121-3. Epub 2026 Feb 13 [PubMed PMID: 41686401]
Level 1 (high-level) evidenceTian L, Tang S, Wang N, Deng H, Zhang Q, Shi T. Hepatic and portal vein Doppler ultrasounds in assessing liver inflammation and fibrosis in chronic HBV infection with a normal ALT level. Frontiers in medicine. 2023:10():1178944. doi: 10.3389/fmed.2023.1178944. Epub 2023 May 25 [PubMed PMID: 37305137]