 Doppler Abdominal Aorta Assessment, Protocols, and Interpretation
Doppler Abdominal Aorta Assessment, Protocols, and Interpretation
Introduction
Doppler ultrasound is a valuable, noninvasive modality for evaluating the abdominal aorta, providing insights into systemic flow and perfusion. This procedure is convenient and cost-effective, eliminating the need for contrast administration, radiation exposure, and the limited availability associated with computed tomography and magnetic resonance imaging.[1][2][3] Integrating Doppler ultrasound into abdominal aorta assessment protocols can help identify conditions such as stenosis and aneurysms, as well as monitor vascular grafts following endovascular aneurysm repair.[4][5][6]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Doppler Ultrasound Anatomy
On grayscale ultrasound, the abdominal aorta appears as a thin-walled, tubular structure on sagittal view and as a rounded structure on axial view. The abdominal aorta is located in the retroperitoneum, in the prevertebral space to the left of the inferior vena cava, the second largest vessel in this anatomic space. Initially, it lies in the midline in the upper abdomen, opposite to the T12 vertebral body. The aorta gradually shifts leftward as it descends to the level of the L4 vertebral body, opposite the umbilicus, where it bifurcates into its distal main branches, the right and left common iliac arteries. As it descends, it gives off multiple single and paired branches, and its diameter gradually narrows; females have narrower aortic diameters than males. The abdominal aorta gives origin to 4 unpaired branches—the celiac artery at the T12 level, the superior mesenteric artery at the L1 level, the inferior mesenteric artery at the L3 level, and the median sacral artery. In addition, 5 paired arterial branches are present—the inferior phrenic, middle suprarenal, and renal arteries at the L1-2 levels, gonadal arteries between the L2 and L3 levels, and lumbar arteries. The aorta terminates by bifurcating into the right and left common iliac arteries at the L4 level.
Color Doppler ultrasound examination reveals internal blood flow, whereas spectral sampling demonstrates a high-resistance multiphasic flow pattern.
Doppler Concept
Doppler imaging visualizes and measures blood flow by analyzing the interaction of ultrasound pulses with moving blood elements. As an extension of B-mode ultrasound, it is based on the same pulse-echo principle. Rapidly moving targets, such as red blood cells, produce distinct echoes that can be displayed as a color flow map (color Doppler) or a wave pattern (spectral Doppler).[3][7]
Ultrasound Doppler enhances and supplements other vascular imaging methods by providing functional data. Color Doppler ultrasound provides information about the presence or absence of flow, mean velocity, and flow direction within a selected region of interest, ie, the color box. Spectral Doppler imaging extends these functional data by tracing moving blood velocities over time, enabling quantitative assessment of absolute blood flow velocities and analysis of flow patterns.[2][3][7][8][9]
Indications
Doppler assessment of the abdominal aorta is critical for diagnosing and monitoring aortic pathologies, providing essential information for treatment decisions and follow-up. This modality is commonly used for the following:
- Diagnosis, screening, and follow-up of aortic aneurysms and pulsatile abdominal masses.[4][5][6]
- Evaluation of hypertensive patients: Initial diagnostic modality in the young population and handy follow-up modality for high-risk chronic patients to diagnose aortic wall hematomas, thrombi, and dissection.[10]
- Assistance in the diagnosis of some peri-aortic diseases, such as mid-aortic syndrome and retroperitoneal fibrosis.[11][12]
- Assessment of abdominal aortic involvement during screening and follow-up of large-vessel vasculitides, such as Takayasu arteritis.[13][14]
- Post-procedural surveillance of patients following endovascular aneurysm repair.[15]
Contraindications
Although there are no absolute contraindications, the effectiveness of Doppler ultrasound may be reduced in individuals with obesity, significant bowel gas, ascites, large ventral hernias, subcutaneous emphysema, or extensive aortic wall calcification.[13][16]
Equipment
Transducer Selection and Orientation
Low-frequency transducers with high penetration are essential for obtaining clear diagnostic images. Adult patients typically require operating frequencies ranging from 2.5 to 5.0 MHz, whereas pediatric patients may require frequencies up to 10 MHz. Adjusting the transducer frequency during the examination is essential to achieve optimal image quality based on the patient's body habitus. An effective Doppler ultrasound examination of the abdominal aorta requires selecting a transducer appropriate to the patient's body type and optimizing the balance between ultrasound penetration and image resolution. Low-frequency transducers, typically 2.5 to 5.0 MHz, provide sufficient penetration for adult patients, whereas high-frequency transducers, up to 10 MHz, offer higher resolution suitable for pediatric patients. Additionally, frequency adjustments should be made during the procedure to ensure the highest image quality.[17][18][19][17]
Personnel
Trained and qualified ultrasound technicians perform most peripheral ultrasound examinations in radiology and vascular labs. However, well-trained healthcare personnel can also provide point-of-care ultrasound triaging at the forefront of healthcare services.
Radiologists with adequate knowledge and qualifications interpret Doppler studies.
Practice Guidelines and Technical Considerations
Key practice parameters are essential for performing high-yield diagnostic and screening ultrasound examinations of the abdominal aorta:[20]
- Examination should be conducted by qualified personnel following standardized protocols to ensure precise results.
- The examination should assess the entire length of the abdominal aorta from various angles, extending from its diaphragmatic aperture (through a midline subcostal window) to the distal aortic bifurcation (about an inch below the umbilicus) with a global evaluation of the common iliac arteries.
- The interpretation of the findings should consider the patient's medical history and relevant risk factors.
Adherence to these guidelines is associated with a comprehensive and effective Doppler evaluation of the abdominal aorta.[8]
Preparation
No special preparation is required for Doppler ultrasound of the abdominal aorta in individuals with average body habitus and weight. However, for individuals with larger body habitus and obesity, minimizing bowel gas is important. Bowel gas reduction can be achieved by fasting overnight and avoiding activities that lead to air swallowing, such as smoking or chewing gum.[4][16]
Technique or Treatment
Understanding the protocols for performing Doppler assessment of the abdominal aorta and interpreting the results is crucial for accurate diagnosis and patient care.
Image Optimization
The greyscale ultrasound image depth should be adjusted to visualize the vertebral body behind the aorta, with the spine and aorta on the patient's left and the inferior vena cava on the patient's right. Bowel gas may impede image acquisition; techniques such as steady pressure or lateral decubitus can help displace it.[21]
To ensure unbiased Doppler analysis, the examiner must fine-tune the Doppler gain to achieve optimal diagnostic color and spectral signal saturation. This adjustment helps to avoid artifactual aliasing, a spectral ambiguity caused by disparities in the radiofrequency pulse of the Doppler source and the received flow velocities. On color Doppler, it manifests as patches of noisy, interwoven color hues. In spectral Doppler, it shifts the flow wave apex to the opposite side of the baseline.[7][21][22]
Examination Technique
The examination begins with greyscale scanning of the aorta in the axial plane, followed by complementary evaluation in the sagittal plane. Accurate measurement of the aorta and iliac artery segments—from the anterior leading edge to the posterior leading edge—should be obtained in both transverse and longitudinal planes. When an endograft is present, its attachment sites should be carefully documented.
Measurements of aortic diameter obtained by ultrasound can vary among practitioners, leading to inconsistent results. The cardiac cycle phase further impacts the assessment of aortic measurements. The vessel's complex geometry and surrounding tissue conditions are other confounding factors.[23] Recent research suggests that the most reliable method is to measure the aortic diameter using calipers from the outer wall to the outer wall or from the inner wall to the inner wall in both axial and sagittal planes.[24] For abdominal aortic aneurysm (AAA) surveillance, assigning a single trained observer to perform follow-up ultrasound Doppler imaging is recommended to ensure measurement consistency and reproducibility, highlighting the importance of examiner expertise.[25]
Following the greyscale scan, color and spectral Doppler should be used to assess the aorta, aneurysmal sac (if any), and any endografts in place. Color Doppler is deployed to address the luminal patency of the abdominal aorta qualitatively. Similarly, it assesses graft patency and detects abnormal blood flow patterns. Spectral Doppler should be employed to obtain samples from different aortic segments by placing a sample gate/window on the desired vascular segment to be assessed, ensuring the angle of insonation (the Doppler angle) is less than 60° for precise velocity measurements. Appropriate Doppler angle alignment can be achieved using a heel-to-toe maneuver, in which the transducer is gently tilted or angled along its long axis.[1][3][8][7][9]
Examination Extent
The Doppler examination of the abdominal aorta should begin with a gray-scale assessment that covers the entire length of the abdominal aorta and extends to the common iliac arteries. The scanning process typically commences in the midline from the substernal window to just below the umbilicus to include the iliac arteries as thoroughly as possible. The celiac and superior mesenteric arteries are important reference points for the proximal abdominal aorta, and the bifurcation of the common iliac arteries concludes the terminal abdominal aorta. Excessive transducer pressure should be avoided during abdominal aortic scanning to prevent potentially serious complications, including aneurysm rupture and patient injury.[1][2][3][7][9]
In an ideal world, both cine clips and still images of the greyscale and Doppler samplings of the abdominal aorta at different levels should be obtained. Nonetheless, diagnostic static image captures can be satisfactory if cine clips cannot be stored.
Complications
The ultrasound Doppler examination procedure is generally safe, with minimal known complications. Of note, as mentioned earlier, the examiner should avoid exerting excessive pressure during the abdominal aortic scan to prevent potentially serious complications such as aneurysm rupture.
Clinical Significance
Normal Abdominal Aorta Doppler Signature
The abdominal aorta's diameter decreases from the diaphragm's level to its bifurcation, with females having smaller aortic diameters.[26] The typical Doppler flow pattern in the aorta is antegrade and plug flow (characterized by constant velocity across the vessel) throughout the cardiac cycle, reflecting the bio-elastic buffering effect of the thoracic aorta during ventricular contraction and the characteristics of the vascular bed it supplies.[27][28][29]
The spectral trace above the inferior mesenteric artery branching off point displays a rapid systolic upstroke, followed by a swift return to baseline, brisk yet short early diastolic reverse, and low-velocity forward flow for the remainder of diastole, resulting in a triphasic pattern. This flow trace mirrors the low-resistive vascular beds of the splanchnic circulation, which require continuous perfusion.[30][31][32] In contrast, below the inferior mesenteric artery origin, the Doppler spectrum shows a relative decrease in the systolic flow peak, an increase in the volume of the early diastolic flow reversal, and a decrease or absence of late diastolic flow, resulting in a high-resistive biphasic pattern. This high-resistance flow trace reflects the capillaries' high resistance in the lower limbs' muscular beds (see Image. Normal Abdominal Aorta Doppler).[2][32]
In adolescents, normal peak systolic velocities in the abdominal aorta range from 110 to 120 cm/s.[2][30] With increasing age, these velocities decrease and typically range from 70 to 100 cm/s (see Image. Color and Spectral Ultrasound Doppler Images of Normal Abdominal Aortic Flow Pattern).[8][33][34]
Abnormal Abdominal Aortic Doppler
The abdominal aorta plays a crucial role in the functioning of abdominal organs and the lower body. Abnormalities in the abdominal aorta and its branches can lead to various acute or chronic conditions and align with patterns in the broader vascular system. Atherosclerosis, aneurysm, dissection, and arteritis are common issues.
Abdominal Aortic Aneurysm
An aneurysm is a focal enlargement of an artery, with an expansion of at least 50% beyond the vessel's usual diameter. An AAA is diagnosed when a dilated aorta with a diameter of 30 mm or greater is detected on imaging.[4][5][6][35][36] Diameters between 25 and 29 mm are considered sub-aneurysmal aortic diameters.[36] Academic discourse is increasingly focused on enhancing AAA screening effectiveness, specifically addressing sex-specific differences in rupture risk at smaller diameters, the necessity for inclusive protocols for women, particularly those with a smoking history, and the implications of population-based screening programs in non-Western countries, including Asia.[37][36][38][39][40]
Ultrasound is the preferred modality for screening and monitoring AAAs, as it eliminates the need for repeated exposure to radiation and contrast media used in computed tomography angiography (CTA).[4][5][6][35][36] Additionally, the ultrasound can effectively detect complications such as dissection, chronic rupture, and stent occlusions and exclude coexistent iliac artery aneurysms.
Individuals at higher risk for AAA should undergo diameter-adjusted interval screening to reduce morbidity and mortality.[36] High-risk groups primarily include males aged 65 or older; individuals with a family history of AAA; those with a history of smoking, hypertension, hypercholesterolemia, coronary artery disease, or peripheral arterial disease; and individuals with a first-degree relative with an AAA diagnosis.[41][42][43][44][45]
As stated earlier, Doppler ultrasound is used to diagnose an AAA when a segment of the infrarenal abdominal aneurysm has a diameter of 30 mm or greater. The dilation may be fusiform (in line with the main aorta) or saccular (eccentric segment dilation). A mural echogenic thrombus or intimal calcifications are typically detected (see Image. Greyscale Ultrasound of an Abdominal Aortic Aneurysm).
Color Doppler imaging typically shows swirling arterial flow (Yin-Yang/ Korean flag sign) within the aortic aneurysmal sac (See Image. Color and Spectral Ultrasound Doppler Images of an Abdominal Aortic Aneurysm)
AAAs are associated with serious complications such as dissections and ruptures. In acute or chronic vascular dissections, greyscale images reveal an intraluminal linear echogenic intimal flap that syncs with arterial pulsations. Additionally, color Doppler imaging delineates 2 distinct flow channels on each flap side during diastole, indicating the true and false lumens.[46][47] Suspicion of a silent ruptured aneurysm arises when there is an intimal defect or ulceration between the lumen wall and an adjacent thrombus, asymmetrical or unilateral hypoechogenicity near the aorta, and varying amounts of free fluid in the peritoneal cavities. In addition, color Doppler interrogation shows no color flow.[48][49][50]
Ultrasound Doppler is commonly used to monitor post-endovascular aortic repair complications, such as graft limb stenosis and endoleaks. Careful attention to Doppler settings is needed to detect extra-stent flow and differentiate true endoleak flow from artifactual apparent flow.[15][51]
Three-dimensional ultrasound technology has emerged as an alternative to CTA for measuring AAA diameter and for monitoring post-endovascular aortic repair. Three-dimensional ultrasound involves the concurrent acquisition of multiplanar two-dimensional ultrasound image data, enabling analysis in transverse, coronal, and sagittal planes similar to computed tomography images while obviating the need for contrast administration and reducing radiation exposure.[52][53]
Doppler of Endoleaks
Endovascular aneurysm repair is a safe and widely adopted management approach that is increasingly favored for treating high-risk patients with AAA, particularly older individuals with multiple comorbidities.[36][54]
Endoleak, a peri-graft flow into the aneurysm sac, is the most common complication after endovascular aneurysm repair. Endoleaks are commonly classified into 5 common types (see Table. Types of Endoleaks and Their Standard Criteria).[55]
Table 1. Types of Endoleaks and Their Standard Criteria
|
Endoleak |
Definition/Descriptor |
|
Type I |
Attachment site leak-proximal or distal The most common early post-intervention complication |
|
Type II |
Collateral vessel-leak The most common overall type Aneurysm sac fills with blood from the aortic branches |
|
Type III |
Graft failure Stent junctions may fracture due to arterial pulsation and aneurysm pressure |
|
Type IV |
Graft wall porosity caused by inherent stent material deficiencies |
|
Type V |
Endotension Aneurysm sac growing on its own. Reason unknown. |
Endovascular aneurysmal repair requires a strict imaging surveillance protocol to identify potential complications, including endoleak, potential stent re-occlusion, or the development of a para-anastomotic aneurysm.[51][55][36] Doppler ultrasound is the preferred modality, as it reduces radiation exposure, avoids contrast-related risks, and is more cost-effective compared to CTA.[56][57][58][54] Furthermore, Doppler ultrasound offers a significant advantage compared to CTA by identifying the flow direction in endoleaks.[59] Reports indicate that duplex ultrasound scans showing endoleak nidus velocities exceeding 100 cm/s are unlikely to close independently.[60][61]
On color Doppler ultrasound, type I endoleaks are identified by color flow at the graft's landing zones. On the other hand, type II endoleaks show retrograde flow in the inferior mesenteric and lumbar arteries, with to-and-fro flow in the excluded sac. In type III endoleaks, a color flow is detected in the sac around the graft in a central position.[62] In types IV and V, serial imaging shows increasing sac diameter.
Type I and III endoleaks require prompt intervention, whereas type II endoleaks may resolve spontaneously and often require only regular follow-up.[15][55][36]
Aortic Coarctation
In some cases, a chest x-ray may identify localized aortic indentation and rib notching, suggesting a diagnosis of coarctation of the aorta.[63] However, Doppler spectral flow in the abdominal aorta provides greater insight into the condition of the descending thoracic aorta. The presence of significantly reduced systolic spectral velocities, a lack of early diastolic reverse flow, and a strong diastolic phase that allows for continuous forward flow—known as the tardus parvus pattern (tardus means "delayed acceleration" and parvus refers "low velocity")—may indicate a severe proximal stenotic lesion, such as aortic coarctation, necessitating further cross-sectional vascular imaging.
A clear interpretation of a precise spectral wave pattern requires consideration of the patient's clinical history and previous diagnostic tests to avoid misinterpretation due to confounding factors such as obstruction length, the presence of a patent ductus arteriosus, collateral circulation status, and decreased cardiac output in severe coarctation. Importantly, end-diastolic reversal effectively rules out significant aortic coarctation.[64]
Uncommon forms of aortic coarctation affecting the abdominal aorta include congenital developmental anomalies of the aorta;[65][66][65] inflammatory conditions, such as Takayasu arteritis;[65] and non-inflammatory conditions, such as fibromuscular dysplasia.[66] Contemporary literature generally considers these conditions under the umbrella of the mid-aortic syndrome.
Middle Aortic Syndrome
Middle aortic syndrome is a sub-isthmic coarctation of the distal thoracic or proximal abdominal aorta and its major splanchnic branches. Collateral pathways, such as the internal mammary artery or the arc of Riolan, may become enlarged to bypass the stenotic segment.[67][66] Sonographic findings of middle aortic syndrome include segmental narrowing of the abdominal aorta, turbulent flow (color Doppler aliasing), and focal peak systolic velocities (>200 cm/s) in the stenotic segment. Furthermore, the depiction of the tardus parvus spectral Doppler trace in vessels distal to the stenotic area (eg, the superior mesenteric and renal arteries) is an indirect sign of significant upstream stenosis. The tardus parvus describes a spectral trace showing reduced peak systolic and elevated end-diastolic flow velocities, with an overall prolonged flow time due to the loss of pulsatile energy from the proximal stenosis.[11][68][69][70][71]
Doppler ultrasound is a valuable tool for identifying potential causes of mild smooth stenosis of the abdominal aorta. This tool can identify slab- or strip-like isoechoic lesions around the aorta with minimal blood flow signal in retroperitoneal fibrosis or visualize the thickening of the vascular wall and perivascular halo in vasculitis. Furthermore, it can evaluate collateral circulation in response to stenosis.[12][72]. Further angiographic imaging using CTA or MRA may be warranted.[11][73]
Large-Vessel Vasculitis/Takayasu Aortitis
Large vessel vasculitides are divided into 2 main types—Takayasu arteritis and giant cell arteritis. Takayasu arteritis primarily affects young females and involves large central arteries such as the aorta and pulmonary arteries. In contrast, giant cell arteritis is less common in individuals younger than 50, shows a higher prevalence in males, and most frequently involves the superficial temporal artery and other large peripheral arteries.[74][75]
Takayasu arteritis, also known as pulseless disease, is a chronic inflammatory pan-aortitis involving an intricate interplay of immune processes, genetic factors, and vascular remodeling. This disease often initially presents in children and adolescents with systemic symptoms such as malaise, fever, night sweats, weight loss, and joint pain, accompanied by anemia and elevated inflammatory markers. In the early phases, imaging shows a thickening of the arterial wall. As the condition progresses into a late-quiescent phase, the inflammatory changes subside, leading to stenosis, thrombosis, and aneurysm formation. In this phase, patients often experience complications leading to symptoms such as limb ischemia or renovascular hypertension.[75][76]
Ultrasound is crucial for screening and diagnosing large-vessel vasculitis. Fast-tracking adults and pediatric patients with suspected large-vessel vasculitis or fever of unknown origin is recommended to detect Takayasu arteritis at an early stage.[14][77] The primary focus is the identification of intima-medial and adventitial wall thickening due to inflammation, which leads to segmental or diffuse abdominal aortic lumen narrowing on greyscale imaging, giving the halo sign of vasculitis. Color Doppler may show increased peri-aortic adventitial vascularity in active phases and disappear in remission.[78][79] Doppler interrogation typically reveals abnormally elevated systolic velocity and a shift from the triphasic to monophasic forward flow pattern in patients with Takayasu arteritis.[3][8][13][80] Doppler ultrasound is a valuable tool for detecting complications, such as vascular dissections.[81][82]
Atherosclerosis and Occlusive Arterial Disease
Atherosclerosis is a systemic, multifactorial disorder that affects medium- and large-sized arteries. This disease is characterized by thickening of the vessel wall, especially the intima, with the formation of degenerative plaques and subendothelial deposits of low-density lipoprotein cholesterol. Ultrasound has been used to visualize and quantify atherosclerotic plaques as potential prognostic markers of future cardiovascular events.[83]
Atherosclerosis is characterized by focal irregularities and calcifications on the inner surface of the AA, whereas the adjacent inferior vena cava has a smooth inner surface.[84][85] These vascular changes often lead to peripheral arterial aneurysms, especially popliteal artery aneurysms, which are strongly associated with AAAs.[86][87] Doppler ultrasound detects the total plaque area or volume. Furthermore, it assesses aortic arterial stiffness, providing crucial data for planning surgical or interventional treatments by estimating blood flow and velocity, correlating with stenosis severity.[84][85] Patients with proximal peripheral arterial disease and severe stenosis or occlusion of the distal abdominal aorta and iliac arteries often display a mid-systolic notch in the Doppler spectrum of the descending aorta. This finding is attributed to a reflected backward pressure wave at the stenotic site that dampens the systolic peak.[88]
Leriche syndrome is an unusual form of chronic occlusive atherosclerosis that primarily affects the aorta and iliac arteries. This syndrome is often linked to risk factors such as smoking, high cholesterol, and high blood pressure.[89][90] Most patients are asymptomatic because collateral blood vessels develop to supply the lower limbs, reducing the risk of acute ischemic events.[89][90][91] Ultrasound Doppler imaging typically shows limited color flow in a highly narrowed vessel, often with large, hypoechoic atherosclerotic plaques in the affected area.[91] When conducting examinations, it is crucial to carefully adjust parameters to avoid missing low-velocity flow by increasing the Doppler gain and adjusting the color scale.[7] A monophasic waveform and reduced peak systolic velocities in the common femoral arteries downstream of the blockage can confirm proximal iliac artery occlusion.[91] Currently, angioplasty and stenting are the primary treatments for Leriche syndrome, with open surgery being reserved as an alternative for extensive disease and in cases of failed endovascular intervention.[92][93]
Enhancing Healthcare Team Outcomes
Doppler ultrasound plays a critical role in assessing the abdominal aorta, identifying stenosis, aneurysms, and complications, and monitoring vascular grafts. However, its effectiveness as a screening tool is limited by operator dependency, and additional angiographic imaging with CTA or MRA is often warranted when abnormal findings are detected in a clinically suspicious setting.
To ensure high-quality outcomes, the treating teams must collaborate, emphasizing patient-centered care. Clinicians requesting Doppler evaluations should have the qualifications and skills to understand the impact of aortic diseases and provide comprehensive clinical information justifying the necessity of the assessment. Radiology services should provide qualified personnel capable of conducting satisfactory diagnostic examinations and interpreting findings accurately, considering the patient's medical history and relevant risk factors to ensure the reliability of the results. Another essential strategy is to incorporate point-of-care ultrasound into healthcare training programs for healthcare providers at all levels. This approach can expedite the identification and management of critical abdominal aortic emergencies, thereby improving patient outcomes. Point-of-care ultrasound is a dependable, cost-effective diagnostic tool used in emergency departments, underserved areas, and budget-constrained health systems to detect abdominal aortic abnormalities, especially aneurysms, and their complications. These efforts significantly advance patient-centered care and play a vital role in optimizing outcomes within the broader healthcare system.
Media
(Click Image to Enlarge)
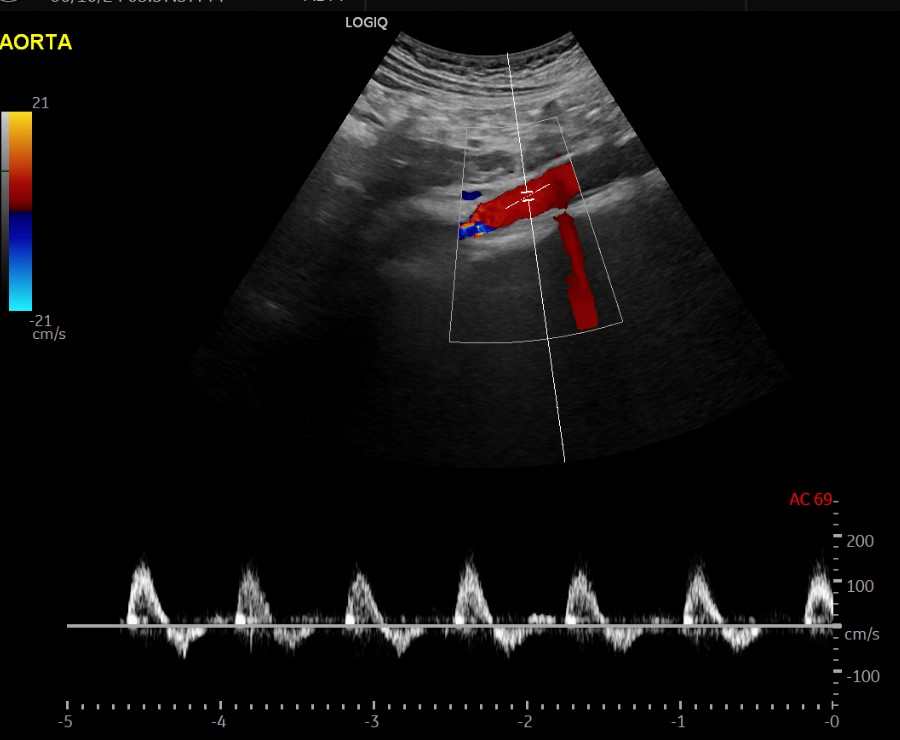
Normal Abdominal Aorta Doppler. Longitudinal color and spectral Doppler images show normal abdominal aorta color saturation and spectral triphasic pattern.
Contributed by M Ahmed, MD
(Click Image to Enlarge)
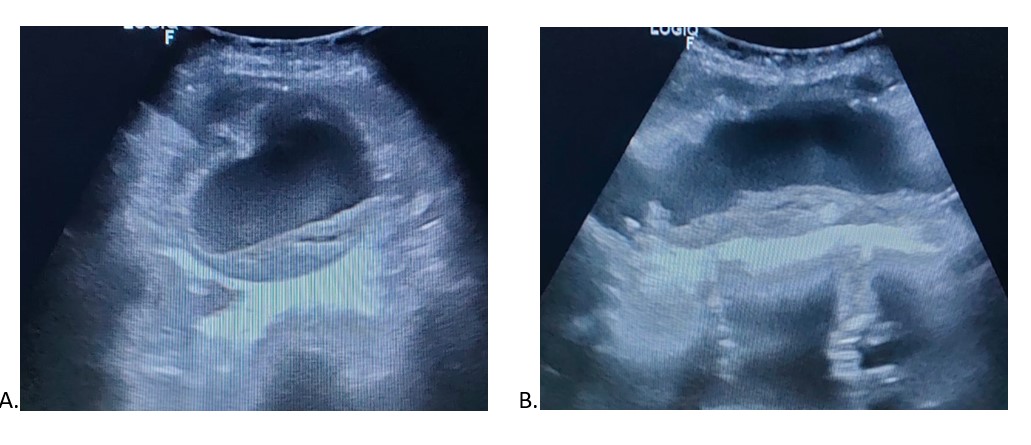
Color and Spectral Ultrasound Doppler Images of Normal Abdominal Aortic Flow Pattern. Abdominal aortic aneurysm. Axial (A) and sagittal (B) scans. Note the eccentric, echogenic mural thrombus.
Contributed by H Ibrahim, MD
(Click Image to Enlarge)
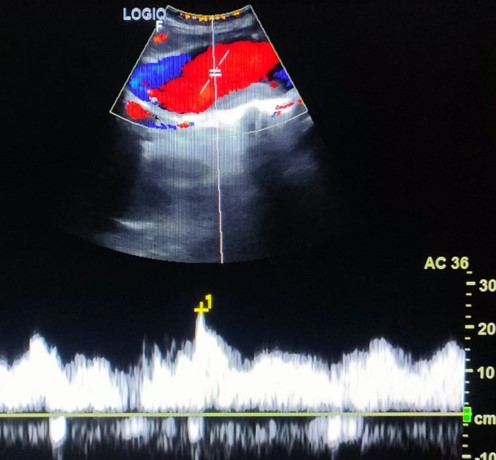
Greyscale Ultrasound of an Abdominal Aortic Aneurysm. Longitudinal color and spectral Doppler images show turbulent bidirectional color saturation within the aneurysm (Korean flag sign) with echogenic mural thrombus and a low-resistance, bidirectional waveform.
Contributed by M Amer, MD
(Click Video to Play)
Color and Spectral Ultrasound Doppler Images of an Abdominal Aortic Aneurysm. This ultrasound video demonstrates the inferior vena cava—the collapsible vessel located posteriorly and to the patient’s right (appearing on the left side of the screen)—and the abdominal aorta, which remains round and lies anteriorly and to the patient’s left (appearing on the right side of the screen).
Contributed by R Gibbons, MD, FAAEM
References
Fadel BM, Bakarman H, Al-Admawi M, Bech-Hanssen O, Di Salvo G. Pulse-wave Doppler interrogation of the abdominal aorta: a window to the left heart and vasculature. Echocardiography (Mount Kisco, N.Y.). 2014 Apr:31(4):543-7. doi: 10.1111/echo.12531. Epub 2014 Feb 7 [PubMed PMID: 24702564]
Chavhan GB, Parra DA, Mann A, Navarro OM. Normal Doppler spectral waveforms of major pediatric vessels: specific patterns. Radiographics : a review publication of the Radiological Society of North America, Inc. 2008 May-Jun:28(3):691-706. doi: 10.1148/rg.283075095. Epub [PubMed PMID: 18480479]
Gupta P, Lyons S, Hedgire S. Ultrasound imaging of the arterial system. Cardiovascular diagnosis and therapy. 2019 Aug:9(Suppl 1):S2-S13. doi: 10.21037/cdt.2019.02.05. Epub [PubMed PMID: 31559150]
Chaikof EL, Dalman RL, Eskandari MK, Jackson BM, Lee WA, Mansour MA, Mastracci TM, Mell M, Murad MH, Nguyen LL, Oderich GS, Patel MS, Schermerhorn ML, Starnes BW. The Society for Vascular Surgery practice guidelines on the care of patients with an abdominal aortic aneurysm. Journal of vascular surgery. 2018 Jan:67(1):2-77.e2. doi: 10.1016/j.jvs.2017.10.044. Epub [PubMed PMID: 29268916]
Level 1 (high-level) evidenceO'Donnell TFX, Schermerhorn ML. Abdominal aortic aneurysm screening guidelines: United States Preventative Services Task Force and Society for Vascular Surgery. Journal of vascular surgery. 2020 May:71(5):1457-1458. doi: 10.1016/j.jvs.2020.01.054. Epub [PubMed PMID: 32334726]
Kapila V, Jetty P, Wooster D, Vucemilo V, Dubois L, Canadian Society for Vascular Surgery. Screening for abdominal aortic aneurysms in Canada: 2020 review and position statement of the Canadian Society for Vascular Surgery. Canadian journal of surgery. Journal canadien de chirurgie. 2021 Sep 1:64(5):E461-E466. doi: 10.1503/cjs.009120. Epub 2021 Sep 1 [PubMed PMID: 34467750]
Revzin MV, Imanzadeh A, Menias C, Pourjabbar S, Mustafa A, Nezami N, Spektor M, Pellerito JS. Optimizing Image Quality When Evaluating Blood Flow at Doppler US: A Tutorial. Radiographics : a review publication of the Radiological Society of North America, Inc. 2019 Sep-Oct:39(5):1501-1523. doi: 10.1148/rg.2019180055. Epub 2019 Aug 9 [PubMed PMID: 31398088]
Level 2 (mid-level) evidenceFadel BM, Mohty D, Kazzi BE, Alamro B, Arshi F, Mustafa M, Echahidi N, Aboyans V. Ultrasound Imaging of the Abdominal Aorta: A Comprehensive Review. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2021 Nov:34(11):1119-1136. doi: 10.1016/j.echo.2021.06.012. Epub 2021 Jul 2 [PubMed PMID: 34224827]
Meola M, Ibeas J, Lasalle G, Petrucci I. Basics for performing a high-quality color Doppler sonography of the vascular access. The journal of vascular access. 2021 Nov:22(1_suppl):18-31. doi: 10.1177/11297298211018060. Epub 2021 Jul 28 [PubMed PMID: 34320855]
Level 2 (mid-level) evidenceMohr-Kahaly S, Erbel R, Kearney P, Puth M, Meyer J. Aortic intramural hemorrhage visualized by transesophageal echocardiography: findings and prognostic implications. Journal of the American College of Cardiology. 1994 Mar 1:23(3):658-64 [PubMed PMID: 8113549]
Yan L, Li HY, Ye XJ, Xu RQ, Chen XY. Doppler ultrasonographic and clinical features of middle aortic syndrome. Journal of clinical ultrasound : JCU. 2019 Jan:47(1):22-26. doi: 10.1002/jcu.22634. Epub 2018 Oct 14 [PubMed PMID: 30318593]
Chen SJ, Qin L, Xie YJ, Zhu JP, Zhang Q, Chen M. Ultrasonography for Preoperative Diagnosis of Retroperitoneal Fibrosis. Ultrasound quarterly. 2017 Jun:33(2):162-166. doi: 10.1097/RUQ.0000000000000293. Epub [PubMed PMID: 28538448]
Level 2 (mid-level) evidenceBardi M, Diamantopoulos AP. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice summary. La Radiologia medica. 2019 Oct:124(10):965-972. doi: 10.1007/s11547-019-01058-0. Epub 2019 Jun 28 [PubMed PMID: 31254221]
Nozawa H, Ogura M, Miyasaka M, Suzuki H, Ishikura K, Ishiguro A, Ito S. Ultrasonography as a Diagnostic Support Tool for Childhood Takayasu Arteritis Referred to as Fever of Unknown Origin: Case Series and Literature Review. JMA journal. 2021 Oct 15:4(4):358-366. doi: 10.31662/jmaj.2020-0115. Epub 2021 Sep 13 [PubMed PMID: 34796290]
Level 2 (mid-level) evidenceZierler RE. Duplex ultrasound follow-up after fenestrated and branched endovascular aneurysm repair (FEVAR and BEVAR). Seminars in vascular surgery. 2020 Dec:33(3-4):60-64. doi: 10.1053/j.semvascsurg.2020.05.006. Epub 2020 May 23 [PubMed PMID: 33308597]
Goldschmidt E, Al-Embideen S, Abbas J, Russell T, Paolini D, Al-Balbissi L, Lurie F. The Effect of Patient Oral Intake Status on Abdominal Aortic Ultrasound Visualization. Annals of vascular surgery. 2021 Jul:74():204-208. doi: 10.1016/j.avsg.2020.12.035. Epub 2021 Feb 5 [PubMed PMID: 33556518]
Hwang M, Piskunowicz M, Darge K. Advanced Ultrasound Techniques for Pediatric Imaging. Pediatrics. 2019 Mar:143(3):. doi: 10.1542/peds.2018-2609. Epub [PubMed PMID: 30808770]
Magee P. Essential notes on the physics of Doppler ultrasound. BJA education. 2020 Apr:20(4):112-113. doi: 10.1016/j.bjae.2020.01.003. Epub 2020 Feb 20 [PubMed PMID: 33456938]
Lieu D. Ultrasound fundamentals and their clinical implications for interventional cytopathologists. Cytopathology : official journal of the British Society for Clinical Cytology. 2025 Jul:36(4):356-374. doi: 10.1111/cyt.13382. Epub 2024 Apr 18 [PubMed PMID: 38635297]
. AIUM Practice Parameter for the Performance of Diagnostic and Screening Ultrasound Examinations of the Abdominal Aorta in Adults. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2021 May:40(5):E34-E38. doi: 10.1002/jum.15668. Epub 2021 Mar 5 [PubMed PMID: 33665858]
Ramaswami G, Al-Kutoubi A, Nicolaides AN, Dhanjil S, Griffin M, Belcaro G, Coen LD. The role of duplex scanning in the diagnosis of lower limb arterial disease. Annals of vascular surgery. 1999 Sep:13(5):494-500 [PubMed PMID: 10466993]
Oglat AA, Matjafri MZ, Suardi N, Oqlat MA, Abdelrahman MA, Oqlat AA. A Review of Medical Doppler Ultrasonography of Blood Flow in General and Especially in Common Carotid Artery. Journal of medical ultrasound. 2018 Jan-Mar:26(1):3-13. doi: 10.4103/JMU.JMU_11_17. Epub 2018 Mar 28 [PubMed PMID: 30065507]
Grøndal N, Bramsen MB, Thomsen MD, Rasmussen CB, Lindholt JS. The cardiac cycle is a major contributor to variability in size measurements of abdominal aortic aneurysms by ultrasound. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2012 Jan:43(1):30-3. doi: 10.1016/j.ejvs.2011.09.025. Epub 2011 Oct 21 [PubMed PMID: 22018525]
Hill BG, Holloway R, Lim J, Clifford K, Lesche S, Letts J, Krysa J. The correlation between different ultrasound planes and computed tomography measures of abdominal aortic aneurysms. Australasian journal of ultrasound in medicine. 2023 Feb:26(1):5-12. doi: 10.1002/ajum.12319. Epub 2022 Oct 12 [PubMed PMID: 36960142]
Matthews EO, Pinchbeck J, Elmore K, Jones RE, Moxon JV, Golledge J. The reproducibility of measuring maximum abdominal aortic aneurysm diameter from ultrasound images. The ultrasound journal. 2021 Feb 26:13(1):13. doi: 10.1186/s13089-021-00211-z. Epub 2021 Feb 26 [PubMed PMID: 33646456]
Trihan JE, Perez-Martin A, Guillaumat J, Lanéelle D. Normative and pathological values of hemodynamic and Doppler ultrasound arterial findings in children. VASA. Zeitschrift fur Gefasskrankheiten. 2020 Jun:49(4):264-274. doi: 10.1024/0301-1526/a000860. Epub 2020 Apr 23 [PubMed PMID: 32323630]
London GM, Guerin AP. Influence of arterial pulse and reflected waves on blood pressure and cardiac function. American heart journal. 1999 Sep:138(3 Pt 2):220-4 [PubMed PMID: 10467216]
Wood MM, Romine LE, Lee YK, Richman KM, O'Boyle MK, Paz DA, Chu PK, Pretorius DH. Spectral Doppler signature waveforms in ultrasonography: a review of normal and abnormal waveforms. Ultrasound quarterly. 2010 Jun:26(2):83-99. doi: 10.1097/RUQ.0b013e3181dcbf67. Epub [PubMed PMID: 20498564]
Addetia K, Therrien J. Spot diagnosis using pulse wave Doppler interrogation of the abdominal aorta. Journal of cardiovascular ultrasound. 2012 Jun:20(2):112-3. doi: 10.4250/jcu.2012.20.2.112. Epub 2012 Jun 25 [PubMed PMID: 22787531]
Voges I, Jerosch-Herold M, Hedderich J, Pardun E, Hart C, Gabbert DD, Hansen JH, Petko C, Kramer HH, Rickers C. Normal values of aortic dimensions, distensibility, and pulse wave velocity in children and young adults: a cross-sectional study. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2012 Nov 14:14(1):77. doi: 10.1186/1532-429X-14-77. Epub 2012 Nov 14 [PubMed PMID: 23151055]
Level 2 (mid-level) evidenceOsada T, Murase N, Kime R, Shiroishi K, Shimomura K, Nagata H, Katsumura T. Arterial blood flow of all abdominal-pelvic organs using Doppler ultrasound: range, variability and physiological impact. Physiological measurement. 2007 Oct:28(10):1303-16 [PubMed PMID: 17906396]
Osada T, Nagata H, Murase N, Shimomura K, Kime R, Shiroishi K, Nakagawa N, Katsumura T. Hemodynamic relationships among upper-abdominal aorta and femoral arteries: basis for measurement of arterial blood flow to abdominal-pelvic organs. Medical science monitor : international medical journal of experimental and clinical research. 2009 Jul:15(7):CR332-40 [PubMed PMID: 19564822]
Maier SE, Meier D, Boesiger P, Moser UT, Vieli A. Human abdominal aorta: comparative measurements of blood flow with MR imaging and multigated Doppler US. Radiology. 1989 May:171(2):487-92 [PubMed PMID: 2649924]
Level 2 (mid-level) evidenceVieli A, Moser U, Maier S, Meier D, Boesiger P. Velocity profiles in the normal human abdominal aorta: a comparison between ultrasound and magnetic resonance data. Ultrasound in medicine & biology. 1989:15(2):113-9 [PubMed PMID: 2658233]
Lin J, Chen S, Yao Y, Yan M. Status of diagnosis and therapy of abdominal aortic aneurysms. Frontiers in cardiovascular medicine. 2023:10():1199804. doi: 10.3389/fcvm.2023.1199804. Epub 2023 Jul 28 [PubMed PMID: 37576107]
Wanhainen A, Van Herzeele I, Bastos Goncalves F, Bellmunt Montoya S, Berard X, Boyle JR, D'Oria M, Prendes CF, Karkos CD, Kazimierczak A, Koelemay MJW, Kölbel T, Mani K, Melissano G, Powell JT, Trimarchi S, Tsilimparis N, ESVS Guidelines Committee, Antoniou GA, Björck M, Coscas R, Dias NV, Kolh P, Lepidi S, Mees BME, Resch TA, Ricco JB, Tulamo R, Twine CP, Document Reviewers, Branzan D, Cheng SWK, Dalman RL, Dick F, Golledge J, Haulon S, van Herwaarden JA, Ilic NS, Jawien A, Mastracci TM, Oderich GS, Verzini F, Yeung KK. Editor's Choice -- European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2024 Feb:67(2):192-331. doi: 10.1016/j.ejvs.2023.11.002. Epub 2024 Jan 23 [PubMed PMID: 38307694]
Level 1 (high-level) evidenceMola AG, Díaz CT, Martins GG, Sari XT, Montoya SB. Editor's Choice - Systematic Review and Meta-Analysis of Normal Infrarenal Aortic Diameter in the General Worldwide Population and Changes in Recent Decades. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2022 Jul:64(1):4-14. doi: 10.1016/j.ejvs.2022.04.014. Epub 2022 Apr 26 [PubMed PMID: 35483578]
Li K, Zhang K, Li T, Zhai S. Primary results of abdominal aortic aneurysm screening in the at-risk residents in middle China. BMC cardiovascular disorders. 2018 Apr 3:18(1):60. doi: 10.1186/s12872-018-0793-5. Epub 2018 Apr 3 [PubMed PMID: 29614976]
Thompson SG, Bown MJ, Glover MJ, Jones E, Masconi KL, Michaels JA, Powell JT, Ulug P, Sweeting MJ. Screening women aged 65 years or over for abdominal aortic aneurysm: a modelling study and health economic evaluation. Health technology assessment (Winchester, England). 2018 Aug:22(43):1-142. doi: 10.3310/hta22430. Epub [PubMed PMID: 30132754]
Söderberg P, Wanhainen A, Svensjö S. Five Year Natural History of Screening Detected Sub-Aneurysms and Abdominal Aortic Aneurysms in 70 Year Old Women and Systematic Review of Repair Rate in Women. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2017 Jun:53(6):802-809. doi: 10.1016/j.ejvs.2017.02.024. Epub 2017 Apr 4 [PubMed PMID: 28389251]
Level 1 (high-level) evidenceYing AJ, Affan ET. Abdominal Aortic Aneurysm Screening: A Systematic Review and Meta-analysis of Efficacy and Cost. Annals of vascular surgery. 2019 Jan:54():298-303.e3. doi: 10.1016/j.avsg.2018.05.044. Epub 2018 Aug 4 [PubMed PMID: 30081169]
Level 1 (high-level) evidenceSaw ST, Leong BDK, Abdul Aziz DA. Early Detection of Undiagnosed Abdominal Aortic Aneurysm and Sub-Aneurysmal Aortic Dilatations in Patients with High-Risk Coronary Artery Disease: The Value of Targetted Screening Programme. Vascular health and risk management. 2020:16():215-229. doi: 10.2147/VHRM.S250735. Epub 2020 Jun 9 [PubMed PMID: 32606718]
Guirguis-Blake JM, Beil TL, Senger CA, Coppola EL. Primary Care Screening for Abdominal Aortic Aneurysm: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA. 2019 Dec 10:322(22):2219-2238. doi: 10.1001/jama.2019.17021. Epub [PubMed PMID: 31821436]
Level 1 (high-level) evidenceJoergensen TM, Houlind K, Green A, Lindholt JS. Abdominal aortic diameter is increased in males with a family history of abdominal aortic aneurysms: results from the Danish VIVA-trial. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2014 Dec:48(6):669-75. doi: 10.1016/j.ejvs.2014.09.005. Epub 2014 Oct 22 [PubMed PMID: 25443525]
Fattahi N, Linné A, Roy J, Stenman M, Svensjö S, Nilsson O, Hultgren R. Prevalence of abdominal aortic aneurysm (AAA) in first-degree relatives: detecting AAA in adult offspring of AAA patients. BJS open. 2024 Jan 3:8(1):. doi: 10.1093/bjsopen/zrad163. Epub [PubMed PMID: 38195162]
Clevert DA, Rupp N, Reiser M, Jung EM. Improved diagnosis of vascular dissection by ultrasound B-flow: a comparison with color-coded Doppler and power Doppler sonography. European radiology. 2005 Feb:15(2):342-7 [PubMed PMID: 15449009]
Baliga RR, Nienaber CA, Bossone E, Oh JK, Isselbacher EM, Sechtem U, Fattori R, Raman SV, Eagle KA. The role of imaging in aortic dissection and related syndromes. JACC. Cardiovascular imaging. 2014 Apr:7(4):406-24. doi: 10.1016/j.jcmg.2013.10.015. Epub [PubMed PMID: 24742892]
Catalano O, Siani A. Ruptured abdominal aortic aneurysm: categorization of sonographic findings and report of 3 new signs. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2005 Aug:24(8):1077-83 [PubMed PMID: 16040822]
Diaz O, Eilbert W. Ruptured abdominal aortic aneurysm identified on point-of-care ultrasound in the emergency department. International journal of emergency medicine. 2020 May 14:13(1):25. doi: 10.1186/s12245-020-00279-9. Epub 2020 May 14 [PubMed PMID: 32410576]
Huang D, Wanchu R, Cho M, Leon L, Ganti L. Emergency department point-of-care ultrasound diagnosis of active bleeding into the intraluminal thrombus of an abdominal aortic aneurysm. Radiology case reports. 2023 Jun:18(6):2116-2120. doi: 10.1016/j.radcr.2023.03.002. Epub 2023 Apr 5 [PubMed PMID: 37089970]
Level 3 (low-level) evidenceBeeman BR, Murtha K, Doerr K, McAfee-Bennett S, Dougherty MJ, Calligaro KD. Duplex ultrasound factors predicting persistent type II endoleak and increasing AAA sac diameter after EVAR. Journal of vascular surgery. 2010 Nov:52(5):1147-52. doi: 10.1016/j.jvs.2010.06.099. Epub 2010 Aug 5 [PubMed PMID: 20691559]
Jansen LC, Schwab HM, van de Vosse FN, van Sambeek MRHM, Lopata RGP. Local and global distensibility assessment of abdominal aortic aneurysms in vivo from probe tracked 2D ultrasound images. Frontiers in medical technology. 2022:4():1052213. doi: 10.3389/fmedt.2022.1052213. Epub 2023 Jan 6 [PubMed PMID: 36699662]
Li X, Cokkinos D, Gadani S, Rafailidis V, Aschwanden M, Levitin A, Szaflarski D, Kirksey L, Staub D, Partovi S. Advanced ultrasound techniques in arterial diseases. The international journal of cardiovascular imaging. 2022 Aug:38(8):1711-1721. doi: 10.1007/s10554-022-02558-3. Epub 2022 Feb 23 [PubMed PMID: 35195805]
Jean-Baptiste E, Feugier P, Cruzel C, Sarlon-Bartoli G, Reix T, Steinmetz E, Chaufour X, Chavent B, Salomon du Mont L, Ejargue M, Maurel B, Spear R, Midy D, Thaveau F, Desgranges P, Rosset E, Hassen-Khodja R, Association Universitaire de Recherche en Chirurgie Vasculaire. Computed Tomography-Aortography Versus Color-Duplex Ultrasound for Surveillance of Endovascular Abdominal Aortic Aneurysm Repair: A Prospective Multicenter Diagnostic-Accuracy Study (the ESSEA Trial). Circulation. Cardiovascular imaging. 2020 Jun:13(6):e009886. doi: 10.1161/CIRCIMAGING.119.009886. Epub 2020 Jun 8 [PubMed PMID: 32507018]
Abraha I, Luchetta ML, De Florio R, Cozzolino F, Casazza G, Duca P, Parente B, Orso M, Germani A, Eusebi P, Montedori A. Ultrasonography for endoleak detection after endoluminal abdominal aortic aneurysm repair. The Cochrane database of systematic reviews. 2017 Jun 9:6(6):CD010296. doi: 10.1002/14651858.CD010296.pub2. Epub 2017 Jun 9 [PubMed PMID: 28598495]
Level 1 (high-level) evidenceIscan HZ, Unal EU, Akkaya B, Daglı M, Karahan M, Civelek I, Ozbek MH, Okten RS. Color Doppler ultrasound for surveillance following EVAR as the primary tool. Journal of cardiac surgery. 2021 Jan:36(1):111-117. doi: 10.1111/jocs.15194. Epub 2020 Nov 22 [PubMed PMID: 33225510]
Schmieder GC, Stout CL, Stokes GK, Parent FN, Panneton JM. Endoleak after endovascular aneurysm repair: duplex ultrasound imaging is better than computed tomography at determining the need for intervention. Journal of vascular surgery. 2009 Nov:50(5):1012-7; discussion 1017-8. doi: 10.1016/j.jvs.2009.06.021. Epub [PubMed PMID: 19878784]
Cantador AA, Siqueira DE, Jacobsen OB, Baracat J, Pereira IM, Menezes FH, Guillaumon AT. Duplex ultrasound and computed tomography angiography in the follow-up of endovascular abdominal aortic aneurysm repair: a comparative study. Radiologia brasileira. 2016 Jul-Aug:49(4):229-233 [PubMed PMID: 27777476]
Level 2 (mid-level) evidenceKazimierczak W, Serafin Z, Kazimierczak N, Ratajczak P, Leszczyński W, Bryl Ł, Lemanowicz A. Contemporary imaging methods for the follow-up after endovascular abdominal aneurysm repair: a review. Wideochirurgia i inne techniki maloinwazyjne = Videosurgery and other miniinvasive techniques. 2019 Jan:14(1):1-11. doi: 10.5114/wiitm.2018.78973. Epub 2018 Oct 15 [PubMed PMID: 30766622]
Arko FR, Filis KA, Siedel SA, Johnson BL, Drake AR, Fogarty TJ, Zarins CK. Intrasac flow velocities predict sealing of type II endoleaks after endovascular abdominal aortic aneurysm repair. Journal of vascular surgery. 2003 Jan:37(1):8-15 [PubMed PMID: 12514572]
Maximus S, Skelly C, Milner R. Velocities of type II endoleaks on Doppler ultrasonography predict outcome. Journal of vascular surgery. 2020 May:71(5):1719-1725. doi: 10.1016/j.jvs.2019.07.078. Epub 2019 Oct 13 [PubMed PMID: 31619352]
Wang PS, Verma R. Endoleak. Ultrasound quarterly. 2017 Mar:33(1):96-97. doi: 10.1097/RUQ.0000000000000262. Epub [PubMed PMID: 28081021]
Ferguson EC, Krishnamurthy R, Oldham SA. Classic imaging signs of congenital cardiovascular abnormalities. Radiographics : a review publication of the Radiological Society of North America, Inc. 2007 Sep-Oct:27(5):1323-34 [PubMed PMID: 17848694]
Silvilairat S, Cetta F, Biliciler-Denktas G, Ammash NM, Cabalka AK, Hagler DJ, O'Leary PW. Abdominal aortic pulsed wave Doppler patterns reliably reflect clinical severity in patients with coarctation of the aorta. Congenital heart disease. 2008 Nov-Dec:3(6):422-30. doi: 10.1111/j.1747-0803.2008.00224.x. Epub [PubMed PMID: 19037983]
Morrissey S, Tan KT, Byrne JS. Takayasu arteritis with middle aortic syndrome and mesenteric ischemia treated by aortic stenting. Journal of vascular surgery cases and innovative techniques. 2017 Sep:3(3):168-170. doi: 10.1016/j.jvscit.2017.06.004. Epub 2017 Jul 23 [PubMed PMID: 29349411]
Level 3 (low-level) evidenceDinoto E, Pecoraro F, Ferlito F, Peluso A, Bajardi G. A rare case of infrarenal aortic coarctation in a young female. International journal of surgery case reports. 2020:77S(Suppl):S152-S156. doi: 10.1016/j.ijscr.2020.07.083. Epub 2020 Aug 24 [PubMed PMID: 32888881]
Level 3 (low-level) evidenceChaudhary R, Tiwari T, Sharma R, Goyal S. Midaortic syndrome in a middle-age female. BMJ case reports. 2021 Nov 9:14(11):. doi: 10.1136/bcr-2021-246530. Epub 2021 Nov 9 [PubMed PMID: 34753733]
Level 3 (low-level) evidenceStavros AT, Parker SH, Yakes WF, Chantelois AE, Burke BJ, Meyers PR, Schenck JJ. Segmental stenosis of the renal artery: pattern recognition of tardus and parvus abnormalities with duplex sonography. Radiology. 1992 Aug:184(2):487-92 [PubMed PMID: 1620853]
Jha SK, Bhusal A, Oli R. "Tardus-parvus waveform" the only initial clue to mid-aortic syndrome- a rare cause of youth onset hypertension: A case report and a comprehensive review. Radiology case reports. 2024 Feb:19(2):732-736. doi: 10.1016/j.radcr.2023.11.008. Epub 2023 Dec 1 [PubMed PMID: 38074442]
Level 3 (low-level) evidenceMonticone S, Veglio F, Mulatero P. Atypical secondary hypertension due to mid-aortic syndrome. European heart journal. 2012 Sep:33(18):2248. doi: 10.1093/eurheartj/ehs029. Epub 2012 Feb 23 [PubMed PMID: 22362516]
Kadoya Y, Zen K, Saburi M, Matoba S. Mid-aortic Syndrome: A Rare Cause of Juvenile Hypertension. Internal medicine (Tokyo, Japan). 2018 Feb 1:57(3):447. doi: 10.2169/internalmedicine.9337-17. Epub 2017 Nov 1 [PubMed PMID: 29093417]
Jiang X, Liu J, Zhang Y, Sun X. Ultrasound diagnosis and follow-up of Takayasu arteritis with femoral vein involvement. Journal of vascular surgery. Venous and lymphatic disorders. 2019 Jul:7(4):587-590. doi: 10.1016/j.jvsv.2018.07.009. Epub 2018 Oct 29 [PubMed PMID: 30385136]
de Oliveira Campos JL, Bitencourt L, Pedrosa AL, Silva DF, Lin FJJ, de Oliveira Dias LT, Simões E Silva AC. Renovascular hypertension in pediatric patients: update on diagnosis and management. Pediatric nephrology (Berlin, Germany). 2021 Dec:36(12):3853-3868. doi: 10.1007/s00467-021-05063-2. Epub 2021 Apr 13 [PubMed PMID: 33851262]
Jennette JC. Overview of the 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Clinical and experimental nephrology. 2013 Oct:17(5):603-606. doi: 10.1007/s10157-013-0869-6. Epub 2013 Sep 27 [PubMed PMID: 24072416]
Level 3 (low-level) evidenceKeser G, Aksu K. Diagnosis and differential diagnosis of large-vessel vasculitides. Rheumatology international. 2019 Feb:39(2):169-185. doi: 10.1007/s00296-018-4157-3. Epub 2018 Sep 17 [PubMed PMID: 30221327]
Keser G, Atagunduz P, Soy M. Recent advances in the diagnosis and therapy of large vessel vasculitis. Polish archives of internal medicine. 2022 Jun 29:132(6):. pii: 16272. doi: 10.20452/pamw.16272. Epub 2022 Jun 6 [PubMed PMID: 35699647]
Level 3 (low-level) evidenceMonti S, Bartoletti A, Bellis E, Delvino P, Montecucco C. Fast-Track Ultrasound Clinic for the Diagnosis of Giant Cell Arteritis Changes the Prognosis of the Disease but Not the Risk of Future Relapse. Frontiers in medicine. 2020:7():589794. doi: 10.3389/fmed.2020.589794. Epub 2020 Dec 8 [PubMed PMID: 33364248]
Antoniou A, Vlahos L, Mourikis D. Abdominal Takayasu's arteritis: imaging with color duplex sonography. European radiology. 1998:8(4):547-9 [PubMed PMID: 9569319]
Svensson C, Eriksson P, Zachrisson H. Vascular ultrasound for monitoring of inflammatory activity in Takayasu arteritis. Clinical physiology and functional imaging. 2020 Jan:40(1):37-45. doi: 10.1111/cpf.12601. Epub 2019 Nov 10 [PubMed PMID: 31605660]
Schmidt WA, Nerenheim A, Seipelt E, Poehls C, Gromnica-Ihle E. Diagnosis of early Takayasu arteritis with sonography. Rheumatology (Oxford, England). 2002 May:41(5):496-502 [PubMed PMID: 12011371]
Civilibal M, Sever L, Numan F, Altun G, Ocak S, Candan C, Kasapcopur O, Caliskan S, Cantasdemir M, Arisoy N. Dissection of the abdominal aorta in a child with Takayasu's arteritis. Acta radiologica (Stockholm, Sweden : 1987). 2008 Feb:49(1):101-4 [PubMed PMID: 17963085]
Wang J, Lee YZ, Cheng Y, Zheng Y, Gao J, Tang X, Wang T, Zhang C. Sonographic Characterization of Arterial Dissections in Takayasu Arteritis. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2016 Jun:35(6):1177-91. doi: 10.7863/ultra.15.07042. Epub 2016 Apr 22 [PubMed PMID: 27105948]
Steinl DC, Kaufmann BA. Ultrasound imaging for risk assessment in atherosclerosis. International journal of molecular sciences. 2015 Apr 29:16(5):9749-69. doi: 10.3390/ijms16059749. Epub 2015 Apr 29 [PubMed PMID: 25938969]
Cismaru G, Serban T, Tirpe A. Ultrasound Methods in the Evaluation of Atherosclerosis: From Pathophysiology to Clinic. Biomedicines. 2021 Apr 13:9(4):. doi: 10.3390/biomedicines9040418. Epub 2021 Apr 13 [PubMed PMID: 33924492]
de Korte CL, Hansen HH, van der Steen AF. Vascular ultrasound for atherosclerosis imaging. Interface focus. 2011 Aug 6:1(4):565-75. doi: 10.1098/rsfs.2011.0024. Epub 2011 Jun 1 [PubMed PMID: 22866231]
Tuveson V, Löfdahl HE, Hultgren R. Patients with abdominal aortic aneurysm have a high prevalence of popliteal artery aneurysms. Vascular medicine (London, England). 2016 Aug:21(4):369-75. doi: 10.1177/1358863X16648404. Epub 2016 May 23 [PubMed PMID: 27216869]
Cervin A, Wanhainen A, Björck M. Popliteal Aneurysms are Common Among Men With Screening Detected Abdominal Aortic Aneurysms, and Prevalence Correlates With the Diameters of the Common Iliac Arteries. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2020 Jan:59(1):67-72. doi: 10.1016/j.ejvs.2019.07.042. Epub 2019 Nov 19 [PubMed PMID: 31757587]
Styczynski G, Szmigielski C, Leszczynski J, Abramczyk P, Kuch-Wocial A, Szulc M. Descending aortic Doppler flow pattern in patients with proximal peripheral artery disease. The American journal of cardiology. 2009 Jun 15:103(12):1774-6. doi: 10.1016/j.amjcard.2009.02.034. Epub 2009 Apr 16 [PubMed PMID: 19539092]
CHOA GH, RASSIM HS, WONG WL. THROMBO-OBLITERATIVE VASCULAR DISEASE OF EARLY ONSET AND LONG DURATION. British heart journal. 1963 Nov:25(6):814-6 [PubMed PMID: 14072605]
Hardman RL, Lopera JE, Cardan RA, Trimmer CK, Josephs SC. Common and rare collateral pathways in aortoiliac occlusive disease: a pictorial essay. AJR. American journal of roentgenology. 2011 Sep:197(3):W519-24. doi: 10.2214/AJR.10.5896. Epub [PubMed PMID: 21862782]
Marak JR, Narayan S, Lal NR, Raj G, Gara H. Leriche syndrome: Clinical and diagnostic approach of a rare infrarenal aortoiliac occlusive disease. Radiology case reports. 2024 Feb:19(2):540-546. doi: 10.1016/j.radcr.2023.10.077. Epub 2023 Nov 22 [PubMed PMID: 38044901]
Level 3 (low-level) evidenceCarsten CG 3rd, Kalbaugh CA, Langan EM 3rd, Cass AL, Cull DL, Snyder BA, York JW, Taylor SM. Contemporary outcomes of iliofemoral bypass grafting for unilateral aortoiliac occlusive disease: a 10-year experience. The American surgeon. 2008 Jun:74(6):555-9; discussion 559-60 [PubMed PMID: 18557000]
Chiu KW, Davies RS, Nightingale PG, Bradbury AW, Adam DJ. Review of direct anatomical open surgical management of atherosclerotic aorto-iliac occlusive disease. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2010 Apr:39(4):460-71. doi: 10.1016/j.ejvs.2009.12.014. Epub 2010 Mar 20 [PubMed PMID: 20303805]