Introduction
Hearing loss represents the third most common cause of years lived with disability globally, with 1.57 billion people (20.3% of the global population) affected in 2019 and projections of 2.45 billion by 2050. While age is the dominant driver in adults, with prevalence doubling each decade after 60 years, pediatric hearing loss has a distinct etiologic profile, with 60% of childhood cases attributable to preventable causes, including otitis media and meningitis.[1] The discussion primarily addresses the most common types of chronic sensorineural hearing loss, including presbycusis (age-related hearing loss), noise-induced hearing loss, and cases where medical treatment has failed.[2][3][4][5][6] Some forms of sensorineural hearing loss can be treated medically, including sudden sensorineural hearing loss, autoimmune inner ear disease, Ménière disease, infection-related sensorineural hearing loss, ototoxicity from medications, and hearing loss caused by acoustic neuroma. Treatments may include corticosteroids, immunosuppressants, dietary modifications, diuretics, and, in some cases, surgical procedures or radiation. The success of these treatments varies.
Beyond sensorineural hearing loss, other causes include conductive hearing loss, such as chronic otitis media, cholesteatoma, otosclerosis, ossicular discontinuity, and congenital ear anomalies. Mixed hearing loss, which combines conductive and sensorineural components, can also occur. Additional challenges include communication difficulties, such as difficulty understanding speech, tinnitus-related hearing issues, and permanent hearing loss in children, which can affect speech, language development, and learning.
Effective treatment of hearing loss may include functional support through digital hearing aids, cochlear implants, assistive listening devices, and comprehensive auditory rehabilitation, as well as various communication strategies (speechreading, cued speech, sign language). The activity will focus on digital hearing aids, which act as processors that convert sound waves into digital signals and amplify them to compensate for an individual's specific hearing impairment. These hearing aids tend to be less effective for individuals with profound hearing loss, poor speech discrimination, severely impaired auditory nerve function, or central auditory processing dysfunction.
Previous analog or conventional hearing aids amplified all sounds uniformly. True conventional analog hearing aids are now rare because major manufacturers have stopped producing them in favor of digital devices, which are vastly superior. Digital hearing aids convert sound into digital code, analyze different sound frequencies and environmental conditions, selectively amplify speech over background noise, and automatically adjust to changing conditions. They can also be specially programmed to match an individual's unique audiogram and specific needs. The common types of hearing aids discussed include:
- Behind-the-ear
- Receiver-in-canal
- In-the-ear
- Completely-in-canal
Key components of digital hearing aids include a microphone, a digital signal processor chip, an amplifier, a receiver, and, typically, a rechargeable power source, which eliminates the need for battery replacement. Modern hearing aids include several advanced features, such as feedback suppression to reduce or eliminate whistling, Bluetooth® connectivity, smartphone app control, tinnitus masking, noise reduction, and directional microphones.
Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Function
The main functions of hearing aids are to improve communication and make sounds, particularly speech, more audible and understandable. Clinicians should recognize that hearing aids do not restore normal hearing and cannot replace normal cochlear function. Hearing aids are not associated with meaningful improvements in memory or executive function in older adults with hearing loss. However, the use of corrective hearing technology is associated with a lower long-term risk of dementia.[7] Hearing aids may improve the following:
Sound Detection and Amplification
- Receive sound through a microphone
- Digitally process the sound
- Amplify sound frequencies that the person cannot hear, such as greater amplification of consonant sounds like "s," "f," and "th," in patients with high-frequency sensorineural hearing loss
- Deliver a modified, improved sound to the ear
Improve Speech Understanding
- In various environments, noisy and quiet
- Through phones or other devices, such as televisions and computers
Sound Localization
- Improve awareness of surroundings for safety and communication
- Hearing in complex environments, especially occupational settings
Traditionally, hearing aids should be fitted following a medical consultation and a hearing assessment conducted by a prescribing clinician, typically an otolaryngologist–head and neck surgeon, and an audiologist. This recommendation is particularly important if the patient has one of the following:
- Sudden hearing loss
- Hearing loss in only one ear
- Severe hearing loss
- Dizziness or vertigo
- Ear pain or drainage
- Rapidly worsening hearing
- Tinnitus in one ear
- Poor speech understanding
- Diagnostic uncertainty about the cause of hearing loss
In October 2022, the National Institute on Deafness and Other Communication Disorders announced that adults aged 18 and older with perceived mild-to-moderate hearing loss can legally purchase certain over-the-counter hearing aids without a clinician's or audiologist's advice. Over-the-counter hearing aids are not intended for the treatment of severe or profound hearing loss, according to the US Food and Drug Administration Reauthorization Act of 2017 and the final rule finalized in August 2022.[National Institute on Deafness and Other Communication Disorders. Over-the-Counter Hearing Aids][Federal Registrar. Medical Devices; Ear, Nose, and Throat Devices; Establishing Over-the-Counter Hearing Aids]
Self-fitting air-conduction hearing aids under this act are subject to a special control requiring usability testing, which inherently includes testing the directions for use. Further, any device must have labeling bearing adequate directions for use unless subject to an exemption.[Code of Federal Regulations. Self-Fitting Air-Conduction Hearing Aids][Code of Federal Regulations. Part 801 Labeling] The choice of aid type depends mainly on the hearing loss, the anatomy of the outer ear, the patient's dexterity, the choice of a battery-operated product, and the patient's aesthetic concerns.[8][Code of Regulations. Self-Fitting Air-Conduction Hearing Aid] Technological advances have improved the usability of hearing aids. Recommendations for hearing aid fitting should include:
- Cognitive status, motivation, and patient dexterity
- Daily wear time as a criterion for compliance
- Stereophonic fitting
- Real-time measurement to adjust amplification
- Real-time adjustment to optimize speech understanding, prioritized
- Regular audiology follow-up tailored to patient-centered care
- If the patient's hearing or overall medical status changes, a new medical and audiologic opinion should be obtained [8]
Selection
Various hearing aids are available, and their selection is not a one-size-fits-all approach (see Image. Styles of Hearing Aids). Selection is influenced by factors such as audiometric deficit (laterality, frequency, and degree of loss), cosmesis, and the patient’s needs, lifestyle, and priorities.[9] The following sections describe the advantages and limitations of commonly used hearing aids.
Behind-the-ear hearing aids: These devices sit behind the pinna in a hard plastic case that houses the microphone, amplifier, processor, and battery. A plastic tube connects the hearing aid to an earmold or an open silicone ear tip, depending on the patient's needs. Behind-the-ear hearing aids are commonly used because they can provide various levels of amplification, and their power and performance can be adjusted relatively easily.[10] They are robust and easier for patients with reduced dexterity to manipulate. Patients with moderate-to-profound hearing loss who require amplification will require an earmold, which may be less cosmetically appealing than the open-fitting option. The advantages are that behind-the-ear hearing aids are suitable for all degrees of hearing loss, are easier for patients with dexterity issues to handle, have longer battery life, are durable, are easy to clean, and can accommodate more advanced technology. The disadvantages are that they are more visible, can be affected by wind noise, and may feel bulky. The types of behind-the-ear hearing aids include standard behind-the-ear hearing aids, which are larger and more powerful and are used in moderate to profound hearing loss, and mini behind-the-ear or open-fit hearing aids, which are smaller and more discreet and are used for mild to moderate high-frequency hearing loss.
Receiver-in-canal and receiver-in-ear hearing aids: These devices are designed so that the speaker, or receiver, sits in the ear canal in an open silicone earpiece rather than in the main housing near the microphone and amplifier, providing a more natural sound quality and less occlusion. This design allows higher amplification levels and clearer sound because the sound is delivered closer to the tympanic membrane without the risk of acoustic feedback, which occurs when sound escapes the canal and loops back through the hearing aid because the ear canal remains open. These hearing aids are especially suitable for patients with high-frequency ski-slope hearing loss and for those who value the device's appearance. High-frequency ski-slope hearing loss is named for the downward sloping shape it creates on a pure-tone audiogram. A challenge for patients with ski-slope hearing loss is that hearing aids do not adequately amplify the mid- to high-frequency range necessary for speech perception. Conversely, a cochlear implant may damage low-frequency hearing.[11] The most common type of hearing loss is high-frequency hearing loss, including presbycusis and noise-induced hearing loss.[12] Receiver-in-canal and receiver-in-ear hearing aids are smaller and more discreet, and offer a wider fitting range.
Disadvantages of receiver-in-canal and receiver-in-ear hearing aids include exposure of the receiver to cerumen, moisture, and the environment. The receiver wire is fragile and requires periodic replacement due to wear and tear. These hearing aids are not suitable for severe or profound hearing loss and are susceptible to ambient sound distortion and noise feedback. Patients with reduced manual dexterity, including older adults, pediatric patients, and those with arthritis, may find these devices harder to use, and they are more prone to noise feedback. These hearing aids are less suitable for patients with recurrent ear infections.
In-the-ear, in-the-canal, and completely-in-the-canal hearing aids: In-the-ear, in-the-canal, and completely-in-the-canal hearing aids are broadly grouped as custom-shape hearing aids. These are the most discreet hearing aids and, therefore, advantageous for a patient population that prefers improved aesthetics. These devices differ in size, visibility, power, and various features. They can be used in a range of hearing losses. Because the receiver is closer to the tympanic membrane, it amplifies high frequencies better, which is important for speech discrimination.[10] This feature is useful in environments with high background noise and in patients with presbycusis. However, like receiver-in-canal and open-canal hearing aids, custom-made hearing aids may not be suitable for high amplification because they use smaller batteries.
In-the-ear hearing aids: These hearing aids sit in the outer portion of the ear, the concha bowl, and are clearly visible. In-the-ear hearing aids require custom molding to the ear, have longer battery life or recharging options, and may include a more powerful amplifier, directional microphones, manual volume and program controls, and Bluetooth®. These devices may be best for patients who want a larger, easier-to-handle device, but they are susceptible to wind noise.
In-the-canal hearing aids: These hearing aids sit partly in the ear canal and partly in the concha bowl. In-the-canal hearing aids are smaller than in-the-ear hearing aids and less visible. These devices are also custom-molded and may include a moderate battery capacity, directional microphones, noise reduction, and Bluetooth®. The downside is that in-the-canal hearing aids may be more difficult to handle than in-the-ear hearing aids. Cerumen and moisture exposure increase as the size decreases.
Completely-in-the-canal hearing aids: Completely-in-the-canal hearing aids are nearly invisible because they sit deep inside the ear canal, making them the most discreet option. These devices often require pulling on a tiny removal tether, making them hard to clean and maintain. They have very small batteries, fewer microphones and features, and less directional processing. Completely-in-the-canal hearing aids are best for mild to moderate hearing loss only.
Special-use hearing aids: Contralateral routing of signals and bilateral contralateral routing of signals are used for unilateral and asymmetrical hearing loss, respectively, when a conventional or digital hearing aid provides little benefit. In contralateral routing of signals, a microphone is placed on the side of the ear with poorer hearing, and the signal is transmitted to the better-hearing ear, where it is amplified. For bilateral contralateral routing of signals, used in asymmetrical hearing loss (eg, mild to moderate hearing loss on 1 side and severe to profound hearing loss on the other side), there are 2 microphones, 1 in each ear, and sound from both microphones is amplified to the better-hearing ear. A contralateral routing of signals system does not restore binaural hearing or true localization. This system simply prevents the poorer hearing ear from missing sounds altogether. Bilateral contralateral routing of signals is used when 1 ear is unaidable, and the opposite ear has aidable hearing. This system theoretically helps reduce the head shadow effect and improve awareness of side sounds in hearing loss. Contralateral routing of signals and bilateral contralateral routing of signals may serve as alternatives to bone-anchored hearing systems and cochlear implants in some patients.
Issues of Concern
Accurate Diagnosis, Candidacy, and Patient Expectations
Accurate diagnosis requires evaluation of the type, configuration, and degree of hearing loss using pure-tone audiometry, bone conduction testing, tympanometry, acoustic reflexes, speech discrimination testing, speech-in-noise testing, and tuning fork tests, including Weber and Rinne testing. Additional testing, such as brainstem auditory evoked response and otoacoustic emissions, may be needed in selected patients (particularly young children). Candidacy should be determined after a thorough head and neck and otologic examination. Important considerations include ear canal anatomy and health, cerumen, conductive versus sensorineural components, asymmetric hearing loss, sudden sensorineural hearing loss, retrocochlear pathology, and other medical causes of hearing loss, such as ototoxicity. Patient expectations must be realistic and flexible, accounting for varying lifestyles and costs. Patient cognition and dexterity must also be considered. Bilateral hearing aids may improve speech recognition and localization but can increase interference, may be cosmetically less appealing, and are more expensive.[13]
Physical Fit and Comfort
Ear anatomy varies, and poor physical fitting can cause ear pain, skin irritation or infection, poor retention, acoustic feedback, and occlusion sensation. The pinna must be sufficient to support the hearing aid. The ear canal must also be adequate, without stenosis or atresia, and capable of accommodating postsurgical changes.
Acoustic Feedback (Whistling)
Poor hearing aid fitting may result in amplified sound leakage, which can cause acoustic feedback or whistling. Contributing factors include a poor earmold seal or design, excessive gain, cerumen obstruction, and mechanical issues such as clogged tubing. Many newer hearing aids use feedback suppression, but results vary.
Appropriate Amplification and Gain
Insufficient amplification may result in patient dissatisfaction, frustration, and poor speech comprehension. Excessive amplification may result in patient discomfort, sound distortion, loudness intolerance, and an increased risk of auditory damage. Audiologists use prescriptive formulas, real-ear measurements, and frequency-specific adjustments, all supported by up-to-date computer technology.
Speech Understanding in Noisy Environments
Even the most technologically advanced hearing aids may not restore normal hearing, which can decrease patient satisfaction and increase frustration. Important adjustments include directional microphones, noise reduction, and binaural fitting. Counseling should emphasize that hearing aids improve audibility and communication but do not fully restore normal cochlear function.
Occlusion Effect
The occlusion effect can occur with tight-fitting devices, especially in patients with cerumen impaction or moisture in the ear canal. Patients may report boomy sounds or a sensation of being plugged. Important adjustments include venting, open-fit designs, and receiver-in-canal systems.
Patient Expectations and Counseling
Patients must adapt to amplified environmental sounds, altered sound quality, and changes in sound perception. Auditory rehabilitation can be gradual, and patients should be counseled to remain patient during the adjustment period. Although social stigma associated with hearing aid use is less prominent today, some patients may still have concerns about appearance and device visibility.
Auditory Rehabilitation
Some patients experience listening fatigue, especially in complex listening environments. Patients may benefit from communication training and strategies that support speech understanding. Auditory rehabilitation should be individualized according to the patient’s hearing goals, listening environments, motivation, and functional needs.
Patient Factors
The hearing aid user’s lifestyle, concerns, and expectations should be explored. Each user’s communication needs will vary, including the occupational or social setting and frequency of communication. Small devices may be difficult for patients with arthritis, tremor, poor vision, or cognitive impairment. Battery maintenance, cleaning, device insertion and removal, and use of Bluetooth® or smartphone apps may pose challenges for some patients. Patients may also have concerns about cost, cosmesis, sound quality, and the dexterity required to operate the hearing aid.[9] Affordability may be affected by insurance coverage, maintenance expenses, and brand options. Successful fitting requires real-ear verification, speech testing, patient feedback, motivation, involvement, and ongoing audiology care and adjustment.
Clinical Significance
Despite being common, hearing loss is often misunderstood and underestimated, and many clinicians have limited training in hearing impairment and its treatment. Many healthcare professionals are unaware of who might benefit from hearing aids or other hearing rehabilitation options, but the initial step should start at the primary care level. Sources of confusion regarding hearing aids include the fact that hearing aids assist rather than correct hearing, unlike corrective lenses for vision. Hearing aids may amplify sounds a person does not want to hear, such as background noise, making speech comprehension more challenging. Not all patients are candidates for hearing aids, cochlear implants, or other devices. Hearing aids vary in style, function, and capabilities, and not every hearing aid is right for every person. Hearing loss may fluctuate, and hearing aid adjustments may be necessary throughout life.
According to the National Institute on Deafness and Other Communication Disorders statistics:
- About 2 to 3 out of every 1000 children in the United States are born with a detectable level of hearing loss in one or both ears.[14]
- More than 90% of children who are deaf are born to hearing parents.
- Approximately 15% of American adults (37.5 million) ages 18 and older report hearing difficulty.[15]
- Age is the strongest predictor of hearing loss among adults aged 20 to 69 years, with the greatest hearing loss in the 60- to 69-year age group.[16]
- Men are almost twice as likely as women to have hearing loss among adults ages 20 to 69 years.[16]
- White adults are more likely than adults in other racial and ethnic groups to have hearing loss; Black adults have the lowest prevalence of hearing loss among adults ages 20 to 69 years.[16]
- Among adults ages 20 to 69 years who report 5 or more years of exposure to very loud noise at work, about 18% have speech-frequency hearing loss in both ears. Among adults who report no occupational noise exposure, 5.5% have speech-frequency hearing loss in both ears.[16]
- One in 8 people in the United States (13%, or 30 million) ages 12 or older have hearing loss in both ears, based on standard hearing examinations.[17]
- About 5% of adults aged 45 to 54 years have disabling hearing loss. The rate increases to 10% for adults aged 55 to 64 years. Twenty-two percent of those ages 65 to 74 years and 55% of those who are 75 and older have disabling hearing loss.[National Institute on Deafness and Other Communication Disorders. Quick Statistics About Hearing, Balance, and Dizziness].
According to the 2026 World Health Organization statistics:
- By 2050, nearly 2.5 billion people are projected to have some degree of hearing loss, and more than 700 million will require hearing rehabilitation.
- Around 95.1 million children aged 5 to 19 years worldwide live with hearing loss.
- Unaddressed hearing loss costs the global economy almost $1 trillion (US dollars) annually.
- More than 1 billion young adults are at risk of permanent, avoidable hearing loss due to unsafe listening practices.
- An additional annual investment of less than US $1.40 per person is needed to scale up ear and hearing care services globally.
- Over 10 years, this promises a return of nearly US $16 for every USD invested.
Hearing aids play a major role in hearing health. Unfortunately, many patients continue to face obstacles in obtaining hearing aids or other solutions to their hearing impairment. Many patients do not want the expense, believe they are not candidates, or think they can get along without them. Unaddressed hearing loss can lead to many adverse effects, including social isolation, loneliness, stigma, limitations on communication, speech, and personal safety, limitations in education, training, and employment, and increased risks of dementia and cognitive decline.[18] The impact of hearing aids on the development of effective communication skills, speech, and language is well established.[19][20][21] Finally, hearing aids may positively impact brain function in older adults by improving attention and memory.[22][23]
Other Issues
Modern digital hearing aids represent a major advancement in auditory technology, yet they still face significant limitations and unresolved challenges. The industry is increasingly developing artificial intelligence–powered devices, moving beyond traditional sound amplification methods. However, even artificial intelligence–powered hearing aids cannot completely replicate the brain's natural ability to distinguish speech from background noise. One of the biggest challenges remains listening in complex social environments, such as restaurants, group conversations, crowded public venues, cars, and reverberant rooms.
Additional limitations include frustrations with Bluetooth® capabilities, such as app instability, pairing issues, operating system compatibility, latency, difficulties with device switching, and smartphone compatibility. Battery limitations include battery degradation, shorter streaming and artificial intelligence feature runtimes, dependence on charging stations, and reduced lifespan. Continued problems include cerumen impaction, moisture exposure, durability, cost, and social stigma, because many people are reluctant to show signs of aging or disclose a disability.
The most promising upgrades for 2026 include artificial intelligence–driven processing, which leverages machine learning, adaptive scene analysis, and deep neural networks. These upcoming features aim to identify and address common issues, including speech discrimination, traffic noise, and wind noise. The goal is to alleviate patient frustrations and facilitate adaptation to using hearing aids.
Bluetooth® low-energy Audio and Auracast™ have been introduced as next-generation broadcasting technologies. Auracast allows a single audio source, such as a television or phone, to stream audio to compatible receivers, such as hearing aids, without pairing. This technology is based on the power-efficient Low Complexity Communication Codec and enables hearing-aid users to access both public and personal audio broadcasts. In the future, hearing aid users may be able to bypass traditional hearing aid loop systems by scanning a QR code to connect their hearing aids at airports, public venues, workplaces, and educational settings. Adoption and implementation of the Auracast™ infrastructure are still progressing. Future hearing aid systems may also include biometric and health-monitoring integration.[Bluetooth. Bluetooth® LE Audio, Auracast™ Broadcast Audio, and the Future of Bluetooth Audio]
Enhancing Healthcare Team Outcomes
Hearing aids play a vital role in hearing health care. Early detection and treatment of hearing loss are essential for maintaining social interaction, preventing isolation and depression, supporting speech and language development, and slowing cognitive decline. Providing effective care requires collaboration among healthcare professionals to ensure patient-centered approaches and better outcomes. Hearing health care typically begins in infancy or later, when patients age, are exposed to noise, or experience medical issues affecting hearing. Primary care clinicians, pediatricians, family practitioners, emergency department clinicians, otolaryngologists, neurologists, advanced practice clinicians, nurses, audiologists, speech therapists, and other relevant healthcare professionals should have the necessary skills and knowledge to identify conditions affecting hearing and emphasize early intervention.
A strategic approach is key to diagnosing and treating patients with hearing loss who choose hearing aids. Ethical and social considerations should guide decision-making, respecting patient autonomy and family dynamics. Often, hearing aids benefit not only the patient but also family members, friends, and coworkers. Each healthcare professional must understand their responsibilities, whether they involve referring patients to otolaryngologists and audiologists for further assessment and fitting or advising patients on hearing protection. Effective interprofessional communication is essential to ensure smooth information exchange and collaborative decision-making among team members. Care coordination is critical to optimize hearing aid functionality and monitor for medical concerns such as cerumen impaction, foreign bodies, eg, hearing aid parts falling into the ear canal, infections, or hearing deterioration caused by conditions like cholesteatoma or otosclerosis, which may require medical or surgical treatment. By embracing principles of clinical skill, strategic planning, ethics, responsibility, communication, and care coordination, healthcare professionals can provide patient-focused hearing health care, enhance outcomes, and keep patients informed about new hearing aid technologies that might benefit them.
Nursing, Allied Health, and Interprofessional Team Interventions
Management of hearing loss is inherently interdisciplinary, with allied health professionals and nursing playing central roles across screening, diagnosis support, rehabilitation, communication, and long-term care coordination. Outcomes are significantly improved when care is interprofessional and patient-centered, rather than clinician-only.
Audiologists' primary responsibilities include:
- Diagnostic testing: audiometry, tympanometry, otoacoustic emissions, and auditory brainstem response.
- Hearing aid selection, fitting, verification, and programming
- Cochlear implant candidacy evaluation and mapping
- Ototoxicity monitoring and early detection of threshold shifts
- Longitudinal follow-up and outcome assessment
Nursing, Allied Health, and Interprofessional Team Monitoring
Monitoring in hearing loss care is a continuous, structured process aimed at detecting progression, treatment effects, device performance, and functional outcomes. Allied health professionals and nursing staff are central to this process through serial assessment, early detection of change, documentation, and escalation of care.
Allied professionals and nurses monitor across 4 key domains:
- Auditory function: thresholds, speech perception, asymmetry, progression
- Device function and use: hearing aids, cochlear implants, assistive devices
- Functional communication: real-world hearing ability, participation, safety
- Treatment-related effects: especially ototoxicity, postoperative changes
Media
(Click Image to Enlarge)
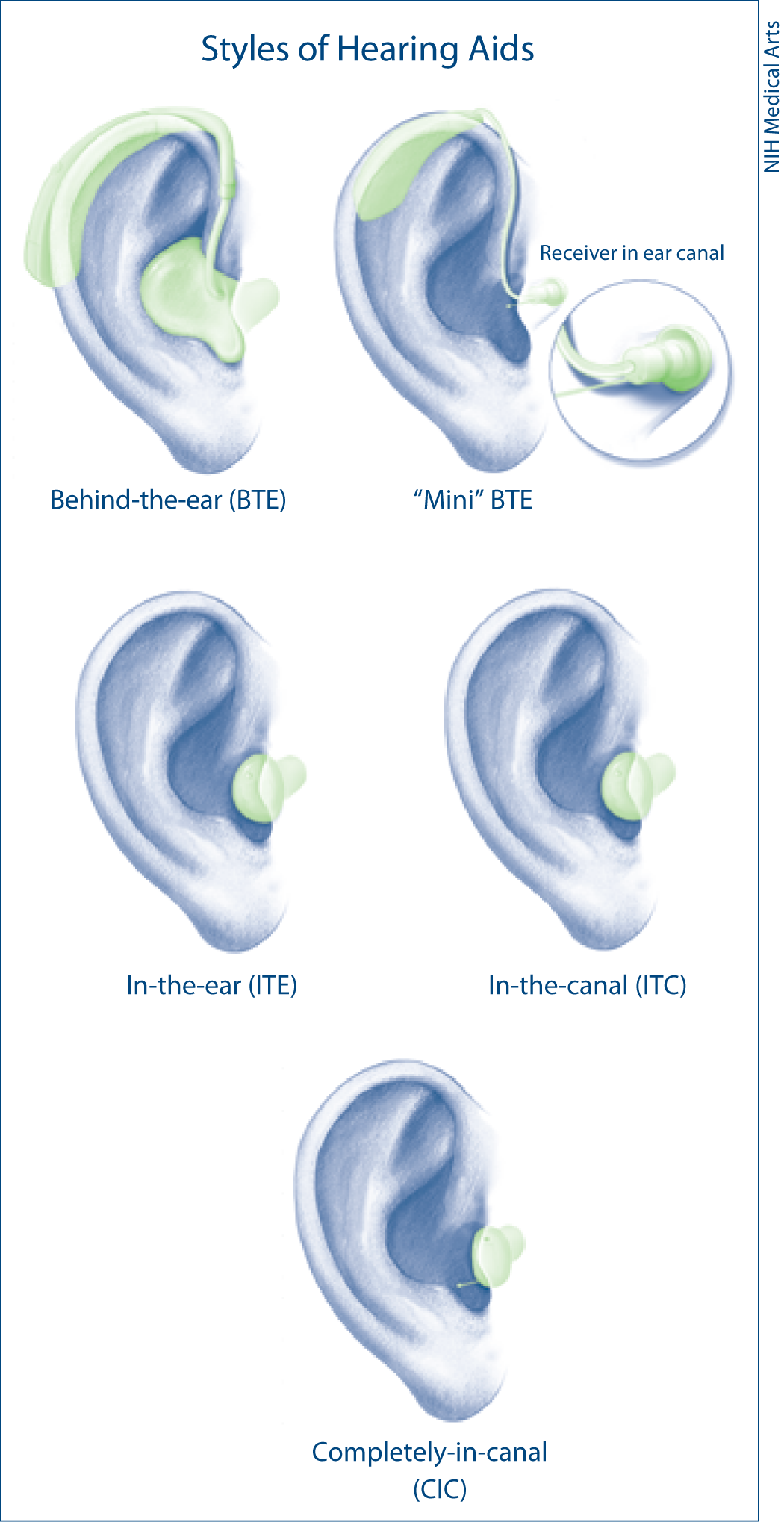
Styles of Hearing Aids. External visibility and anatomy for behind-the-ear, in-the-ear, in-the-canal, and completely-in-canal auditory prostheses.
National Institutes of Health Medical Arts
References
GBD 2019 Hearing Loss Collaborators. Hearing loss prevalence and years lived with disability, 1990-2019: findings from the Global Burden of Disease Study 2019. Lancet (London, England). 2021 Mar 13:397(10278):996-1009. doi: 10.1016/S0140-6736(21)00516-X. Epub [PubMed PMID: 33714390]
Yang CH, Schrepfer T, Schacht J. Age-related hearing impairment and the triad of acquired hearing loss. Frontiers in cellular neuroscience. 2015:9():276. doi: 10.3389/fncel.2015.00276. Epub 2015 Jul 27 [PubMed PMID: 26283913]
Wang J, Puel JL. Presbycusis: An Update on Cochlear Mechanisms and Therapies. Journal of clinical medicine. 2020 Jan 14:9(1):. doi: 10.3390/jcm9010218. Epub 2020 Jan 14 [PubMed PMID: 31947524]
Fetoni AR, Pisani A, Rolesi R, Paciello F, Viziano A, Moleti A, Sisto R, Troiani D, Paludetti G, Grassi C. Early Noise-Induced Hearing Loss Accelerates Presbycusis Altering Aging Processes in the Cochlea. Frontiers in aging neuroscience. 2022:14():803973. doi: 10.3389/fnagi.2022.803973. Epub 2022 Feb 7 [PubMed PMID: 35197842]
Ege T, Tao L, North BJ. The Role of Molecular and Cellular Aging Pathways on Age-Related Hearing Loss. International journal of molecular sciences. 2024 Sep 7:25(17):. doi: 10.3390/ijms25179705. Epub 2024 Sep 7 [PubMed PMID: 39273652]
Yuan C, Feng C, Ma T, Li S, Liu M, Tang G, Han L, Xing Y, Zhang T. NRH attenuates age-related hearing loss by suppressing cochlear ferroptosis and cellular senescence via Sirt3 activation. Free radical biology & medicine. 2026 May:248():450-468. doi: 10.1016/j.freeradbiomed.2026.02.051. Epub 2026 Feb 25 [PubMed PMID: 41759794]
Cribb L, Moreno-Betancur M, Pase MP, Wolfe R, Britt C, Zhou Z, Shah RC, Rance G, Sheets KM, Chong TT, Woods RL, Murray AM, Owen A, Ryan J. Treating Hearing Loss With Hearing Aids for the Prevention of Cognitive Decline and Dementia. Neurology. 2026 Feb 10:106(3):e214572. doi: 10.1212/WNL.0000000000214572. Epub 2026 Jan 14 [PubMed PMID: 41534012]
Thai-Van H, Mosnier I, Dejean F, Ambert-Dahan E, Bakhos D, Belmin J, Bonnard D, Borel S, Ceccato JC, Coez A, Damien M, Del Rio M, El Yagoubi M, Genin A, Gros A, Harichaux M, Idriss S, Ionescu E, Joly CA, Salmon PK, Marianowski R, Marx M, Mom T, Parietti-Winkler C, Potier M, Renard C, Roman S, Roy T, Tronche S, Venail F, Vincent C, Reynard P. Early management of presbycusis: recommendations from the French Society of Otorhinolaryngology and Head and Neck Surgery, the French Society of Audiology, and the French Society of Geriatrics and Gerontology. Geriatrie et psychologie neuropsychiatrie du vieillissement. 2023 May 1:():1-11. doi: 10.1684/pnv.2023.1094. Epub 2023 May 1 [PubMed PMID: 37170803]
Brooks DN. Some factors influencing choice of type of hearing aid in the UK: behind-the-ear or in-the-ear. British journal of audiology. 1994 Apr:28(2):91-8 [PubMed PMID: 7841893]
Fagan JJ. Open Access Publishing of Textbooks and Guidelines for Otolaryngologists in Developing Countries. OTO open. 2019 Jul-Sep:3(3):2473974X19861567. doi: 10.1177/2473974X19861567. Epub 2019 Jul 10 [PubMed PMID: 31428730]
Kim Y, Han JH, Yoo HS, Choi BY. Molecular aetiology of ski-slope hearing loss and audiological course of cochlear implantees. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2022 Oct:279(10):4871-4882. doi: 10.1007/s00405-022-07317-7. Epub 2022 Feb 25 [PubMed PMID: 35212774]
Atcherson SR, Moreland C, Zazove P, McKee MM. Hearing Loss: Hearing Augmentation. FP essentials. 2015 Jul:434():18-23 [PubMed PMID: 26161524]
Holmes AE. Bilateral amplification for the elderly: are two aids better than one? International journal of audiology. 2003 Jul:42 Suppl 2():2S63-7 [PubMed PMID: 12918631]
Level 3 (low-level) evidenceCenters for Disease Control and Prevention (CDC). Identifying infants with hearing loss - United States, 1999-2007. MMWR. Morbidity and mortality weekly report. 2010 Mar 5:59(8):220-3 [PubMed PMID: 20203554]
Blackwell DL, Lucas JW, Clarke TC. Summary health statistics for U.S. adults: national health interview survey, 2012. Vital and health statistics. Series 10, Data from the National Health Survey. 2014 Feb:(260):1-161 [PubMed PMID: 24819891]
Level 3 (low-level) evidenceHoffman HJ, Dobie RA, Losonczy KG, Themann CL, Flamme GA. Declining Prevalence of Hearing Loss in US Adults Aged 20 to 69 Years. JAMA otolaryngology-- head & neck surgery. 2017 Mar 1:143(3):274-285. doi: 10.1001/jamaoto.2016.3527. Epub [PubMed PMID: 27978564]
Lin FR, Niparko JK, Ferrucci L. Hearing loss prevalence in the United States. Archives of internal medicine. 2011 Nov 14:171(20):1851-2. doi: 10.1001/archinternmed.2011.506. Epub [PubMed PMID: 22083573]
Level 3 (low-level) evidenceBisogno A, Scarpa A, Di Girolamo S, De Luca P, Cassandro C, Viola P, Ricciardiello F, Greco A, Vincentiis M, Ralli M, Di Stadio A. Hearing Loss and Cognitive Impairment: Epidemiology, Common Pathophysiological Findings, and Treatment Considerations. Life (Basel, Switzerland). 2021 Oct 17:11(10):. doi: 10.3390/life11101102. Epub 2021 Oct 17 [PubMed PMID: 34685474]
Catts HW, Fey ME, Tomblin JB, Zhang X. A longitudinal investigation of reading outcomes in children with language impairments. Journal of speech, language, and hearing research : JSLHR. 2002 Dec:45(6):1142-57 [PubMed PMID: 12546484]
Ruben RJ. Redefining the survival of the fittest: communication disorders in the 21st century. The Laryngoscope. 2000 Feb:110(2 Pt 1):241-5 [PubMed PMID: 10680923]
Tomblin JB, Oleson JJ, Ambrose SE, Walker E, Moeller MP. The influence of hearing aids on the speech and language development of children with hearing loss. JAMA otolaryngology-- head & neck surgery. 2014 May:140(5):403-9. doi: 10.1001/jamaoto.2014.267. Epub [PubMed PMID: 24700303]
Level 2 (mid-level) evidenceDella Volpe A, Ippolito V, Roccamatisi D, Garofalo S, De Lucia A, Gambacorta V, Longari F, Ricci G, Di Stadio A. Does Unilateral Hearing Loss Impair Working Memory? An Italian Clinical Study Comparing Patients With and Without Hearing Aids. Frontiers in neuroscience. 2020:14():905. doi: 10.3389/fnins.2020.00905. Epub 2020 Sep 8 [PubMed PMID: 33013298]
Di Stadio A, Ralli M, Roccamatisi D, Scarpa A, Della Volpe A, Cassandro C, Ricci G, Greco A, Bernitsas E. Hearing loss and dementia: radiologic and biomolecular basis of their shared characteristics. A systematic review. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2021 Feb:42(2):579-588. doi: 10.1007/s10072-020-04948-8. Epub 2021 Jan 7 [PubMed PMID: 33409831]
Level 1 (high-level) evidence