Introduction
Benign essential blepharospasm (BEB) is a persistent focal cranial dystonia characterized by involuntary, repeated, and frequently debilitating spasms of the orbicularis oculi muscles. Blepharospasm is a disease characterized by an increased rate of bilateral eyelid closure, mainly due to involuntary contraction of the orbicularis oculi muscles (see Image. Typical Blepharospasm). The disorder typically begins with excessive blinking, ocular discomfort, or sporadic eyelid fluttering, and may progress to persistent, powerful spasms that obstruct vision. Once regarded as a purely motor disorder, recent research indicates that BEB represents a multifaceted malfunction within central sensorimotor networks, encompassing the basal ganglia, cerebellum, thalamus, and cortical inhibitory pathways. These anomalies diminish the capacity to inhibit reflexive blinking and enhance motor reactions to sensory stimuli. Over time, the natural history typically demonstrates progressive symptom exacerbation, with several people eventually experiencing functional blindness—characterized by an inability to maintain sufficient eyelid elevation for visual tasks. Contemporary cohort studies validate the progressive and debilitating characteristics of BEB, evidencing significant declines in quality of life and social engagement.[1] Extensive epidemiological data underscore BEB as a chronic neurological condition with considerable individual and social impact.[2]
Blepharospasm is a type of dystonia, a movement disorder characterized by sustained or intermittent muscle contractions that lead to abnormal, repetitive movements or postures, often patterned and sometimes twisting or tremulous. In most dystonias, voluntary action typically leads to exacerbation of dystonia due to overactivation of muscles.[3]
Dystonia can potentially affect any part of the body and can present at a wide range of ages.[4] This disorder can be classified according to its distribution across the body:
- Focal dystonia refers to dystonia that affects only 1 isolated region of the body.
- Segmental dystonia refers to dystonia that affects 2 or more contiguous regions of the body.
- Multifocal dystonia refers to dystonia affecting 2 or more noncontiguous regions.
- Hemidystonia refers to a form of dystonia that affects half of the body.
- Generalized dystonia refers to dystonia affecting the trunk and 3 other sites.
Dystonia can have a static or progressive course. Furthermore, the variability of symptoms can be classified according to how often they occur:[3]
- Persistent dystonia refers to dystonia that remains at the same level throughout the day.
- Action-specific dystonia refers to dystonia that occurs only when performing a specific activity.
- Diurnal fluctuation refers to dystonia that varies throughout the day, with circadian variation in severity.
- Paroxysmal dystonia refers to sudden episodes of dystonia typically induced by a trigger.
Examples of focal dystonia include blepharospasm, oromandibular dystonia, writer's cramp, spasmodic dysphonia, and torticollis. Blepharospasm is a focal dystonia characterized by simultaneous contraction of agonist and antagonist muscles, resulting in involuntary eyelid closure; the first report of patients with blepharospasm was a description of 10 patients by Henri Meige in 1910. The patients reported in this study had involuntary eyelid closure associated with jaw muscle contraction. In his paper, Meige named this phenomenon Convulsions de la Face ("convulsions of the face").[5]
BEB originates from the dysregulated function of the orbicularis oculi muscle, which is innervated by the facial nerve and modulated by brainstem and basal ganglia circuits. Pathological excitability in these circuits leads to heightened blinking responses to trivial stimuli, such as bright light, dryness, or emotional stress. Neurophysiological investigations indicate increased blink reflex sensitivity and diminished inhibitory control, suggesting that BEB disrupts normal sensorimotor gating. Furthermore, ocular surface disorders significantly contribute to symptom exacerbation. Dry eye disease is prevalent in BEB, and elevated blink frequency appears to be both a catalyst and a result of tear-film instability. Research indicates that tear hyperosmolarity, elevated levels of inflammatory cytokines, and mechanical irritation of the ocular surface may exacerbate dystonic contractions, thereby creating a positive feedback loop between sensory irritation and motor dysfunction.[6]
Alterations in the ocular surface constitute an additional aspect of the normal progression of BEB. Excessive blinking intensity and frequency lead to tear-film instability, lid wiper epitheliopathy, meibomian gland strain, and epithelial microtrauma. Research investigating the ocular surface pre- and post-botulinum toxin injections demonstrates persistent anomalies, such as diminished tear breakup time, heightened corneal staining, and mechanical damage in the lid wiper area, which frequently ameliorate following the regulation of spasms.[7] Long-term observational data indicate that BEB is linked to significant psychological effects, including anxiety, depression, and sleep disturbances, all of which correlate with heightened dystonic severity.[8] These non-motor manifestations further underscore the multimodal nature of BEB and its significant impact on patient well-being.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of BEB is not well understood but appears to result from a multifaceted interplay of neurological, sensory, genetic, and environmental factors. Once considered an idiopathic condition, contemporary research identifies BEB as a disorder characterized by impaired sensory integration within the central nervous system. Pathological excitability in brainstem blink reflex circuits and diminished cortical inhibition create a conducive environment in which modest sensory stimuli—such as light, wind, or ocular irritation—can provoke excessive contractions of the orbicularis oculi. Neurophysiological studies over the past decade have consistently revealed increased blink reflex sensitivity and diminished inhibitory control in patients with blepharospasm, indicating dysfunction in the basal ganglia-thalamocortical pathways that govern voluntary and reflexive eyelid movements.[9] The cerebral disinhibition appears to be an important mechanism contributing to the onset of dystonic spasms.
Non-Inherited Risk Factors
Several environmental risk factors have been associated with an increased risk of developing BEB, including high levels of urbanization and employment in white-collar occupations, both of which are often linked to chronic stress and lifestyle-related strain. Occupational and environmental factors, including extended screen usage, elevated visual demands, intense lighting, and arid indoor conditions, impose more stress on the ocular surface and blink mechanism, establishing a persistent cycle of increased sensory input that exacerbates dystonic responses. Other factors loosely associated with an increased risk of developing blepharospasm include reading, watching television, and using a computer screen.[10] Eye strain from these activities is thought to exacerbate the condition.[2]
Environmental and psychosocial factors significantly influence neuronal excitability and sensory input. Stress and exhaustion are frequently identified as primary symptom triggers, with numerous patients indicating that symptoms emerge at times of significant mental or physical strain. Elevated sympathetic activation under stress may enhance blink reflex sensitivity and reduce inhibitory control, therefore promoting dystonic activity. Research shows a substantial correlation between BEB and mood disorders, sadness, and sleep disturbances, which exacerbate symptoms and may occur before diagnosis. Patients suffering from psychiatric conditions such as obsessive-compulsive disorder, depression, and anxiety appear to have an increased risk of developing blepharospasm.[11]
Increasing evidence shows the significance of ocular surface disease as a primary etiological factor. Dry eye disease is prevalent among patients with BEB, with chronic tear-film instability acting as a continuous peripheral sensory stimulus that can initiate or exacerbate spasms. Research has demonstrated that individuals with BEB exhibit elevated blink frequency, reduced tear breakup time, and ocular surface inflammation.[12] Corneal and conjunctival irritation activates trigeminal sensory pathways, enhancing afferent input to brainstem blink circuits and leading to maladaptive plasticity in motor networks. This sensory-motor feedback loop may help explain why treatment for dry eye disease can reduce the severity of BEB in certain people.[13]
In addition, mechanical stress from repetitive blinking may destabilize the ocular surface, exacerbating chronic irritation and encouraging dystonic patterns. Collectively, these data demonstrate that BEB is not merely a motor problem but a multifaceted neurological syndrome influenced by the interplay of central dysfunction, peripheral sensory irregularities, hereditary susceptibility, and environmental factors. Conte et al showed that 40% to 60% of patients present with ophthalmic symptoms such as burning, dryness, or grittiness, which precede the development of blepharospasm.[14] Furthermore, anterior segment disorders, such as keratoconjunctivitis and blepharitis, have been associated with an increased risk of developing blepharospasm. However, this is more accurately classified as secondary blepharospasm, as symptoms often improve when the underlying condition is appropriately treated.[15][16]
Inherited Risk Factors
Genetic predisposition adds further risk. BEB seems to be polygenic, with many genetic variants likely affecting synaptic plasticity, inhibitory neurotransmission, and motor circuit excitability. Several genetic mutations have been implicated in the development of the disease. Studies have reported that 20% to 30% of cases have a positive family history of BEB, and some genes have been associated with greater susceptibility to developing the disease.[17] Other factors implicated in the pathogenesis of the disease include neurotransmitter dysregulation, structural damage, and underlying eye disorders.[18][19] Familial studies indicate an increased incidence of focal dystonias in first-degree relatives, implying a genetic predisposition. Neurobiological alterations associated with aging exacerbate this risk. BEB often presents between the ages of 50 and 70, corresponding with a reduction in GABAergic inhibitory tone and an increase in neuronal noise within motor pathways. These age-related changes may reduce the threshold for dystonia onset in genetically predisposed individuals.[20] Trauma, inflammation, or persistent sensory irritation may serve as extrinsic catalysts that transform latent susceptibility into clinical disease.
The finding of multiple affected individuals within families suggests a genetic contribution to the disease.[21] In such cases, the inheritance pattern appears to be autosomal dominant with reduced penetrance. GNAL, CIZ1, TOR1A, DRD5, and REEP4 are genes reported to play a role in the development of BEB.[22][23]
The GNAL gene encodes the Gα subunit of the G protein–coupled receptor and is found in the olfactory epithelium, helping to mediate odorant signaling.[23] The GNAL gene is also expressed in striatal neurons found in the basal ganglia. Mouse models have shown that GNAL plays a role in coupling adenyl cyclase in response to dopamine and adenosine via the Drd1 and Adora2a receptors.[24] Mutations in the GNAL gene have been associated with autosomal dominant dystonia-25 and are thought to contribute to dystonia by impairing DRD1/Adora2A-mediated signaling.[25]
The CIZ1 gene encodes for the CDKN1A-interacting zinc finger protein 1.[26] This protein interacts with CIP1 to regulate its distribution. CIZ1 has been found to be associated with autosomal dominant cervical dystonia.[22]
The TOR1A gene encodes torsin-1A, an adenosine triphosphatase that aids in a wide range of cellular activities.[27] TOR1A is highly expressed in melanized neurons in the pars compacta (substantia nigra), dentate gyrus, cerebellum, and stratum pyramidale of CA3 (hippocampus).[28] Mutations in the TOR1A gene are believed to alter TOR1A interactions within the nuclear envelope, leading to structural and functional defects of the nuclear membrane that contribute to the development of dystonia.[29] TOR1A mutations are associated with torsion dystonia and are inherited in an autosomal dominant pattern.[30]
The DRD5 gene encodes the dopamine receptor D1B. DRD5 increases adenylate cyclase activity, thereby elevating intracellular cAMP levels.[31] Polymorphisms in the D5 receptor gene have been associated with blepharospasm.[23][32]
Epidemiology
BEB is a rare yet clinically important focal dystonia with a worldwide prevalence. Despite regional variations in prevalence estimates due to methodological discrepancies and underdiagnosis, the majority of recent epidemiological research indicates prevalence rates of 16 to 133 cases per million individuals.[33] In the United States and Europe, blepharospasm is less common than cervical dystonia, whereas in countries such as Italy and Japan, blepharospasm appears to be more prevalent.[19] These variances indicate not only genetic and demographic influences but also disparities in healthcare accessibility, diagnostic recognition, and cultural attitudes towards movement disorders. The incidence of BEB increases with advancing age and is significantly higher among individuals older than 50. Extensive population-based studies indicate that BEB seldom manifests during childhood or adolescence, reinforcing the notion that age-related neurobiological alterations—such as diminished inhibitory neurotransmission and heightened neural plasticity—may increase susceptibility to dystonia in older adults. Although infrequent, BEB significantly affects public health owing to its chronic nature, functional impairment, and correlation with many neurological and mental comorbidities.
The sex distribution of BEB exhibits a persistent female predominance across most analyzed groups.[19] Current studies indicate that about 60% to 85% of patients with BEB are women,[2] with female-to-male ratios ranging from 1.7:1 to nearly 4:1.[1][34] Multiple hypotheses have been suggested to elucidate this sex disparity, encompassing hormonal effects on basal ganglia function, gender-specific variations in health-seeking behavior, and a heightened incidence of anxiety or dry eye disease in women, both acknowledged factors in the manifestation of BEB symptoms. Studies have reported that one of the contributing factors to an increased risk of blepharospasm in women is menopause.[35] Women may also present with a higher symptom frequency and severity.[36]
The age of onset varies by sex, with women generally presenting in their late 50s to early 60s, whereas men tend to show significantly earlier.[19] Geographical variation additionally influences epidemiological patterns. Analyses of Asian populations reveal lower mean incidence rates than those observed in Western cohorts, with a statewide survey indicating an annual incidence of roughly 0.10 per thousand individuals and a female predominance that aligns with global trends.[2] The regional variation suggests that cultural, environmental, and occupational factors may influence the risk of BEB.
Pathophysiology
BEB is a disease characterized by an increased rate of bilateral eyelid closure, mainly due to the involuntary contraction of orbicularis oculi muscles.[37] The exact pathophysiology of the disease remains unknown. Several pathophysiological mechanisms have been suggested. The pathophysiological mechanisms involved can be categorized as genetic, environmental, functional, and structural, which are not mutually exclusive. In many individuals, the coexistence of multiple mechanisms is required for the disease to develop. The two-hit hypothesis proposes that a predisposing factor and an environmental trigger must coexist for the disease to develop.[18][38] The role of environmental factors in BEB is supported by studies showing the association of underlying eye disease and the antecedent of a traumatic stressor as triggers of the disease.[39][40] Structural and functional mechanisms are thought to work together, as this condition results from a structural defect that leads to neurotransmitter dysregulation.
Blink Reflex
Patients with BEB have an increased blink rate and a greater response in the R2 phase of the trigeminal blink reflex. The trigeminal blink reflex is a physiological response that consists of 2 phases. The R1 phase begins with corneal stimulation and involves an afferent pathway that travels through the ophthalmic branch of the trigeminal nerve to the trigeminal nucleus in the brainstem. This phase is unilateral. After reaching the trigeminal nucleus, signals are sent to the facial nucleus bilaterally, which results in the R2 phase of the trigeminal blink reflex.
The R2 phase is the efferent phase of the reflex, and it is carried by the zygomatic, buccal, and temporal branches of the facial nerve to reach the muscles of facial expression and result in their contraction bilaterally. Patients with BEB exhibit a more intense R2 phase of the trigeminal blink reflex than healthy individuals.[41][42] Similarly, as there is a reflex that results in the stimulation of orbicularis oculi muscles, there is also a reflex for the inhibition of the levator palpebrae superioris. This inhibition reflex also comprises 2 phases—SP1 and SP2, the latter being more intense and longer-lasting than the former. In healthy individuals, inhibition of the levator palpebrae superioris occurs synchronously with orbicularis oculi muscle action.[40] Whether a pathological response to the inhibitory reflex of levator palpebrae superioris plays a role in the pathophysiology of BEB is not yet known.
Several authors have reported specific changes in brain structures. Studies by Etgen et al reported that patients with BEB exhibit bilateral increases in gray matter in the putamen, independent of blepharospasm duration, and gray matter decreases in the parietal lobes that appear to correlate with BEB duration. This finding is also supported by increased glucose metabolism in the thalamus, as evidenced by Suzuki et al.[43][44]
Functional magnetic resonance imaging has also been used to evaluate patients with BEB. Compared to healthy individuals, the anterior visual cortex, the thalamus, the anterior cingulate cortex, the primary motor cortex, and the superior cerebellum exhibited greater activation during voluntary and involuntary blinking.[45] Dopamine also appears to play a role in the pathogenesis of the disease. Studies have reported decreased dopamine binding to D2 receptors in the striatum of these patients compared to healthy individuals.[46]
Anterior Segment Disease
Given the association between prior anterior segment diseases of the eye and an increased risk of developing blepharospasm, it is proposed that in individuals predisposed to blepharospasm, because of either genetic abnormalities or abnormalities in neurological signaling, there is a failure to regulate the blinking reflex, leading to the development of trigeminal hyperexcitability and involuntary eyelid closure.[47] A multitude of patients have dry eye disease, tear-film instability, or lid-wiper epitheliopathy,[7][48] which stimulates trigeminal nociceptors and produces enduring afferent sensory input. This sensory overload facilitates the emergence and exacerbation of dystonic eyelid spasms. Hyperosmolar tears and ocular surface inflammation further activate blink reflex pathways, reducing the threshold for spasms to begin. The peripheral mechanisms may account for the common coexistence of BEB with photophobia and ocular discomfort, as well as for the reduction in BEB severity associated with treatments that enhance ocular surface health.[12]
History and Physical
Obtaining a detailed history is crucial for identifying BEB, as the disorder is clinically characterized and lacks specific laboratory or imaging findings. BEB is an underdiagnosed entity. A study conducted in Japan found that 60% of patients saw at least 5 clinicians before receiving a definitive diagnosis. One-third of patients are diagnosed within the first year of symptom onset, one-third within 1 to 5 years, and one-third within more than 5 years.[49] Patients frequently report a gradual onset of symptoms, characterized by increased blinking, ocular discomfort, or sporadic eyelid fluttering. These initial signs may be misidentified as dry eye illness, allergies, or general ocular pain. Patients often experience a gradual progression over months to several years, leading to more intense, involuntary spasms that disrupt tasks such as reading, driving, and prolonged visual focus. Commonly recognized triggers during history-taking include intense light, wind exposure, exhaustion, extended screen usage, and emotional stress. Numerous patients report ocular dryness or a foreign-body sensation before or during spasms, suggesting a link between ocular surface irritation and heightened blink reflex sensitivity. Inquiring about diurnal variation is informative, as symptoms often worsen as the day progresses and temporarily improve after sleep—a pattern consistent with reduced inhibitory control during states of fatigue.[1]
The physical examination in BEB emphasizes assessing the frequency, amplitude, and distribution of eyelid spasms. Assessment is optimally performed in a tranquil setting, with the patient positioned comfortably and instructed to engage in activities that may provoke symptoms, such as reading or exposure to intense light. In the initial stages of the disease, the physical manifestations may be inconspicuous, characterized solely by sporadic blinking or eyelid flickering. As the condition progresses, spasms intensify, frequently resulting in transient total eyelid closure. The motions are bilateral and symmetrical, a distinguishing characteristic of BEB compared to hemifacial spasm, which is unilateral. The spasms are generally nonrhythmic, involuntary, and difficult for the patient to control intentionally. Monitoring alterations in facial expressions can indicate the engagement of neighboring muscles, such as the procerus, frontalis, or zygomatic muscles, particularly in more advanced instances. Many patients exhibit sensory tricks or geste antagoniste, such as caressing the brow or temple, which temporarily diminishes the intensity of spasm—a characteristic of focal dystonia.
Precipitating Factors
The patient's psychological context is essential. BEB profoundly affects quality of life, leading many patients to experience humiliation, social disengagement, anxiety, and depressive symptoms due to the exacerbation of their facial spasms. Sleep disruptions are prevalent. Mood disorders and sleep disturbances may exacerbate dystonic activity by increasing neuronal excitability. A history of photophobia or ocular discomfort may suggest concurrent dry eye disease, which is common among patients with BEB. Inquiries about prior ocular surgery, prolonged contact lens use, trauma, or systemic neurological disorders help distinguish BEB from secondary etiologies of blepharospasm. A familial history of dystonia or movement disorders may indicate a genetic predisposition. Due to the propensity to spread to adjacent facial muscles over time, it is crucial to investigate symptoms such as jaw clenching, tongue movements, changes in speech, or neck tightness, which may suggest segmental cranial dystonia or progression toward Meige syndrome.
Lee et al have shown that 42.6% of patients experienced a stressful life event before symptom onset that included major life events such as divorce (19.8%), problems at work (13.9%), illness of a family member (2%), death of a parent (1%), moving house (1%), head trauma (1%), traffic accident (1%), and cerebral infarction (1%). In a Tokyo study involving 1116 participants, 9.7% reported symptoms following surgery, with cataract surgery being the most frequently implicated procedure.[39][49]
Motor Manifestations
Blepharospasm-related spasms are typically synchronous and bilateral, primarily involving the orbicularis oculi muscles. Symptom severity varies widely, from mild increases in blinking to functional blindness caused by sustained muscle contraction. In many cases, the condition progresses, initially affecting the orbicularis oculi and later extending to lower facial and neck muscles, a pattern referred to as Meige syndrome.[42]
Apraxia of Eyelid Opening
Some patients with blepharospasm may also present with apraxia of eyelid opening, an inability to reopen the eyes in the absence of orbicularis oculi muscle spasm, resulting from a spasm of the pretarsal orbicularis oculi muscle, which acts against eyelid opening.[50]
Non-Motor Manifestations
Depression and anxiety are commonly observed in patients with BEB, which occur either before the disease or as a consequence of it. The potential diagnosis should be sought during evaluation, and a psychiatric consultation should be considered.[2] Half of patients with BEB have accompanying ocular symptoms, most commonly eye dryness and photophobia.[51]
Relieving Factors
Certain activities have been reported to alleviate symptoms of blepharospasm in some patients, including resting (35.6%), concentrating on work (12.9%), and other activities such as singing, talking, eating, sleeping, and exercising, all reported at 2%. Studies have reported that 31.7% of patients, however, could not identify a relieving factor.[39]
Aggravating Factors
Several factors have been shown to exacerbate blepharospasm symptoms, including fatigue (55.4%), stressful events (46.5%), watching television (27.7%), bright lights (18.9%), dry eye symptoms (14.9%), feeling sick (10.9%), or reading a book (8.9%).
Evaluation
The assessment of BEB is predominantly clinical, depending on a comprehensive history and observation of distinctive involuntary eyelid contractions. The diagnostic strategy for BEB, given the absence of a confirmed laboratory test or imaging marker, emphasizes excluding secondary causes and differentiating BEB from other disorders that result in excessive blinking or eyelid closure. A systematic and thorough evaluation enables professionals to achieve an accurate diagnosis promptly and commence suitable treatment. The clinical interview must investigate the onset, pattern, progression, and triggers of symptoms, as well as their effects on occupational, social, and psychological functioning. Assessing disease severity is crucial and is typically performed using validated metrics such as the Jankovic Rating Scale (JRS) or the Blepharospasm Disability Index (BSDI). These instruments are widely used in clinical practice and research, facilitating the standardization of assessments of severity, frequency, and functional handicap.[1] Documenting baseline severity is crucial for assessing treatment response to therapies like botulinum toxin.[52]
Clinical Assessment
A clinical history determining the nature of the eyelid spasm is highly important. Patients with blepharospasm complain of bilateral, synchronous, and stereotyped spasms of the orbicularis oculi muscle. These spasms may present as brief, repetitive blinking or persistent eye closure, leading to functional impairment. There is a diagnostic algorithm based on bilateral, synchronous, and stereotyped movements of the orbicularis oculi muscle, a sensory trick, or increased blinking.[53][54] This method has been shown to have a sensitivity of 93% and a specificity of 90% in differentiating BEB from other similar conditions.[54][55]
A thorough eye examination is essential for assessing blepharospasm, given its strong association with ocular surface disease. A slit-lamp examination may indicate reduced tear breakdown time, superficial punctate keratopathy, or meibomian gland dysfunction, all of which contribute to sensory discomfort and may aggravate dystonic spasms. Due to the potential for dry eye disease to mimic or exacerbate BEB symptoms, objective assessments such as Schirmer's test, tear osmolarity measurement, and fluorescein staining can help evaluate tear-film stability and ocular surface integrity. Recognizing and addressing ocular surface irregularities is crucial, as persistent sensory irritation can increase excitability of the blink reflex and affect disease severity. Sensory symptoms, such as dry eye sensation or photophobia, have been identified as associated with 94% specificity and 77% sensitivity in patients with BEB.[56]
Patients with blepharospasm may also suffer from related non-motor manifestations such as psychiatric disorders, sleep disorders, sensory symptoms, and cognitive disturbances. Psychiatric disorders, such as anxiety and depression, are associated with BEB. However, other related conditions are also associated with higher rates of anxiety and depression.[37]
Severity Assessment
Several scales have been developed to assess the severity of blepharospasm, including the JRS, Blepharospasm Severity Scale, Blepharospasm Disability Scale, and BDI.[42] The JRS is the most widely used scale, commonly used during the initial assessment and to monitor treatment response during patient follow-up. This scale separately evaluates severity and frequency, assigning scores from 0 to 4 to each domain (see Tables Jankovic Rating Scale for Blepharospasm Severity and Jankovic Rating Scale for Blepharospasm Frequency).[57] Additional scales exist for grading the severity of focal dystonias that are not specific to blepharospasm but are sometimes used when assessing BEB, including the Global Dystonia Rating Scale, Burke-Fahn-Marsden Dystonia Rating Scale, and Unified Dystonia Rating Scale.[53] In clinical practice, the choice of grading scale often depends on the clinician's discretion.
Table 1. Jankovic Rating Scale for Blepharospasm Severity
| Score | Description |
| 0 | None |
| 1 | Minimal, increased blinking present only with external stimuli |
| 2 | Mild, but spontaneous eyelid fluttering (without actual spasm), definitely noticeable, possibly embarrassing, but not functionally disabling |
| 3 | Moderate, very noticeable spasm of eyelids only, mildly incapacitating |
| 4 | Severe, incapacitating spasm of eyelids and possibly other facial muscles |
Table 2. Jankovic Rating Scale for Blepharospasm Frequency
| Score | Description |
| 0 | None |
| 1 | Slightly increased frequency of clinking |
| 2 | Eyelid fluttering lasting less than 1 second in duration |
| 3 | Eyelid spasm lasting more than 1 second, but eyes open more than 50% of the walking time |
| 4 | Functionally blind due to persistent eye closure for more than 50% of the walking time |
Neurophysiology and Imaging
The neurologic assessment aims to rule out other diagnoses. Myasthenia gravis may manifest as eyelid dysfunction; however, it is predominantly characterized by fatigability, ptosis, and weakening of the orbicularis oculi, rather than spasm.[58] Should clinical suspicion emerge, diagnostic procedures, including acetylcholine receptor antibody assays, repeated nerve stimulation, and edrophonium testing, may be warranted. Hemifacial spasm, a significant differential diagnosis, is characterized by unilateral, frequently synchronous facial muscle spasms resulting from neurovascular compression of the facial nerve.[59] Neuroimaging using magnetic resonance imaging of the brain and posterior fossa is advised when hemifacial spasm or secondary etiologies of dystonia are suspected.[60] A magnetic resonance imaging is indicated if structural lesions, including brainstem tumors, demyelinating diseases, or previous trauma, may explain the symptoms. In most patients with classic bilateral blepharospasm and a normal neurological examination, routine neuroimaging is unnecessary; however, a low threshold for imaging is warranted in unusual cases or when the presentation deviates from the standard pattern observed in focal dystonia.[61] Dystonia is characterized by muscle contractions involving antagonistic muscles, which can be evaluated using electromyography; however, this assessment is not commonly performed in clinical practice.[62]
Blink Reflex
Assessment of the blink reflex is useful in evaluating BEB. The tapping of the forehead (glabella reflex) may be performed to induce reflexive blinking. Repeated tapping of the forehead can assess the patient's ability to inhibit the glabella reflex, which is known as Myerson's maneuver.[37] Another way to induce reflexive blinking is to use a startling stimulus, such as a visual or auditory stimulus. In practice, the blink reflex is most commonly induced by electrically stimulating the supraorbital nerve while recording electromyography from the orbicularis oculi muscle.[37] The trigemino-facial blink reflex consists of an early ipsilateral R1 component and a late bilateral R2 component. The pons facilitates the R1 component, whereas the R2 component is dependent on both the pons and the lateral medulla.
The blink reflex can be assessed using the paired-shock technique. Both of the supraorbital nerves are stimulated with an impulse of identical intensity.[63] The first stimulus, which induces a change in the excitability of the reflex circuits (conditioning), is followed by the second stimulus (test), delivered at varying intervals (100-1000 ms) as a probe. The size of the induced response is measured, and the test stimulus is compared to the conditioning stimulus across varying stimulus intervals. A normal patient presents with no R2 response during small intervals (100-200 ms), whereas a patient suffering from blepharospasm may have an R2 response with small intervals (100-200 ms).[37] This test does not have high specificity for dystonia, but can be used to rule out psychogenic dystonia, which presents with normal features.
Treatment / Management
The exact cause of BEB is not well understood, and, as such, there is no definitive cure for BEB. There are, however, a range of treatment options available. The management of BEB focuses on regulating involuntary eyelid spasms, enhancing functional capacity, and treating related ocular surface illness. BEB is a chronic focal dystonia lacking a curative treatment; thus, treatment emphasizes alleviating symptoms, improving quality of life, and preventing consequences, including corneal exposure or functional blindness. The therapy strategy tends to be incremental, commencing with nonpharmacological interventions and advancing to pharmacological and surgical alternatives when required. Patient education is essential, as several individuals benefit from recognizing triggers such as intense light, fatigue, and emotional stress. These treatments are often inadequate in cases of moderate or severe disease, necessitating tailored medical therapies for most individuals.
Photochromatic Modulation
Studies have demonstrated that patients with blepharospasm can tolerate light intensities similar to those tolerated by patients without blepharospasm. However, when lens tints block specific wavelengths, patients with blepharospasm tend to no longer tolerate similar light intensities, suggesting that photophobia in blepharospasm depends on both light intensity and wavelength. Studies have shown symptomatic improvement in patients treated with photochromatic modulation.[64] In particular, the FL-41 lens tint has been shown to reduce photophobia symptoms in patients with blepharospasm.[65][66](B2)
Botulinum Toxin Injections
Botulinum toxins: Botulinum toxin has seven serotypes (A, B, C, D, E, F, and G), but only serotypes A and B are available for clinical use.[67] In the United States, the only botulinum toxin products approved for use in blepharospasm are botulinum toxin type A formulations,[68] including abobotulinumtoxinA, onabotulinumtoxinA, and incobotulinumtoxinA.[69] Studies have shown that abobotulinumtoxinA may have a longer duration of action compared to incobotulinumtoxinA.[70](A1)
Mode of action: Botulinum toxin injection is the standard treatment for patients with BEB. This injection inhibits acetylcholine release at the neuromuscular junction, leading to transient chemodenervation of the orbicularis oculi muscles and a decrease in spasm severity, thereby reducing muscle contraction.[71]
Technique: Treatment is individualized based on the distribution of spasms, prior responses, and the adverse-effect profile. Approximately 1.25 to 5 units of botulinum toxin are used per injection site.[70] In some patients, repeated injections may necessitate progressively higher doses, either due to antibody formation or progression of the underlying condition. Common injection sites include the lateral lower and upper eyelid margins, the lateral canthi, and the medial upper eyelid.[72] The toxin is generally injected into the procerus, corrugator, and orbicularis oculi muscles. The total dose of onabotulinumtoxinA should not exceed 200 units within 30 days.[70]
Clinical response to botulinum toxin injection typically begins within 48 hours, although the magnitude of response is highly variable. Most patients experience a reduction in abnormal movements. Treatment response and the duration of the effect appear to be dose-related, potentially lasting up to 170 days.[73] On average, most patients become significantly symptomatic about 90 days after injection. Botulinum toxin injections are recommended every 3 to 4 months. Some studies report a more intense effect seen with the first round of injections and decreasing efficacy with subsequent doses.[64](B3)
Potential causes of a poor response to botulinum toxin injections include the development of antibodies to the toxin, poor injection technique, and apraxia of eyelid opening.[67] Antibodies against botulinum toxin are more likely to develop when there is a short interval between injections, when booster injections are used, when doses are increasingly larger over time, and when botulinum toxin injection therapy is initiated early.[74] Common adverse effects include temporary ptosis, lagophthalmos, worsening of dry eye, and localized ecchymosis. Clinicians should monitor for incomplete eyelid closure and promptly manage any associated ocular surface complications (see Image. Botulinum Toxin Injections for Blepharospasm).(B2)
Ocular Surface Management
Adjunctive therapy for ocular surface disease is crucial given the high prevalence of dry eye symptoms in BEB.[75] Tear-film instability enhances excitability of the blink reflex and exacerbates dystonic activity, establishing a loop of sensory irritation and motor overactivity. Management encompasses preservative-free artificial tears, lubricating ointments, warm compresses, eyelid hygiene, and therapy for meibomian gland dysfunction. Topical cyclosporine or lifitegrast, as anti-inflammatory treatments, may be advantageous for patients with persistent surface inflammation.[76] Certain individuals experience symptom relief with moisture-retaining contact lenses or punctal occlusion, especially in cases of extreme dryness. Treating ocular surface illness not only alleviates discomfort but may also enhance the overall efficacy of botulinum toxin therapy by reducing sensory input.(B2)
Oral Pharmacotherapy
Oral medicines have traditionally been used in the management of BEB but typically offer only a minimal advantage.[64] Medication includes benzodiazepines, anticholinergics (benztropine and trihexyphenidyl), levodopa, baclofen, VMAT2 inhibitors (tetrabenazine), lithium, valproate, methylphenidate, and zolpidem.[42] Although these agents have a limited role, they may be considered in refractory cases before pursuing surgical interventions or as adjunctive therapy to botulinum toxin injections. Oral pharmacotherapy is also associated with potentially undesirable adverse effects, drowsiness, cognitive adverse effects, and variable efficacy, along with the potential risk of developing dependence on benzodiazepines.[64][77](B3)
Surgical Management
Surgical intervention is considered for patients who fail to respond to medical therapy, remain unresponsive toadequate doses of botulinum toxin, and have persisting symptoms. Surgical management is performed with the intent to improve functionality and reduce the frequency of spasms. In patients whose disease is refractory to standard treatments, procedures such as neuroectomies,[78] myomectomies,[79] and deep-brain stimulation (DBS)[80] represent appropriate treatment alternatives. About half of patients treated with myomectomies or neurectomies require botulinum toxin injection 5 years after surgery, but at lower doses than previously needed. Deep brain stimulation, especially targeting the globus pallidus internus, has been investigated for severe, refractory cranial dystonias; however, its application in isolated blepharospasm is limited and generally reserved for a minority of patients with generalized or segmental dystonia.
Surgical myectomy: Surgical myectomy involves the resection of the protractor muscles, including corrugator supercilii, orbicularis oculi, procerus, and depressor supercilii.[64] Gillum and Anderson described the surgical technique for complete myectomy, which is effective in controlling blepharospasm, with reported improvement in approximately 88% of patients. However, this approach may be associated with postoperative lymphedema, lagophthalmos, and facial anesthesia. Currently, modified and partial myectomy is the preferred technique, performed in addition to correcting the effects of blepharospasm, including brow ptosis, dermatochalasis, and lateral canthal dystopia (see Image. Limited Myectomy for Blepharospasm).[81][82](B2)
Differential Diagnosis
The differential diagnosis of BEB is comprehensive and requires meticulous clinical evaluation, as numerous neurological, ocular, and systemic disorders may imitate or exacerbate eyelid spasms or heightened blinking. Differentiating BEB from these entities is essential for precise therapy planning, as management tactics vary significantly among illnesses. The defining characteristics of BEB—bilateral, involuntary, nonrhythmic spasms of the orbicularis oculi that exacerbate with sensory inputs and ameliorate with rest—establish a basis for distinction. A systematic method that assesses the onset, pattern of muscle involvement, concomitant symptoms, and neuro-ophthalmic findings allows clinicians to diagnose primary BEB and rule out alternative conditions.
Apraxia of Eyelid Opening
Most cases of apraxia of eyelid opening present in the context of extrapyramidal disorders. However, reports of apraxia of eyelid opening as an isolated finding in healthy individuals are available. Apraxia of eyelid opening shares several demographic and clinical features with BEB, including a higher prevalence in the sixth decade of life, a female predominance of approximately 2:1, frequent bilateral involvement, and the use of sensory tricks by many patients. Anxiety and depression are also common before and after diagnosis. In patients with isolated apraxia of eyelid opening, instead of contraction of the orbicularis oculi muscle, contraction of the frontalis muscle opens the eyes. In some cases, it is not possible to differentiate between BEB and apraxia of eyelid opening, as many patients with BEB also have apraxia of eyelid opening, and some who initially present as apraxia of eyelid opening later develop blepharospasm, typically after 1.5 years. Apraxia of eyelid opening is also treated with botulinum toxin injections, and surgery is reserved for refractory cases.[83]
Hemifacial Spasm
Hemifacial spasm has the same female-to-male distribution (2:1), and the age at onset is from 40 to 59 years. The estimated prevalence of hemifacial spasm is 11 per 100,000 people, 7.4 per 100,000 in men, and 14.5 per 100,000 in women.[84] The condition is characterized by involuntary muscle contractions confined to one side of the face. These muscle contractions are typically intermittent, clonic, or tonic. The muscle is relaxed between the spasm episodes. Voluntary facial movements, fatigue, stress, or a change in head position aggravate this condition. Patients may complain of persistent hemifacial spasms during sleep.[85] In contrast, blepharospasm is not observed in sleep. Hemifacial spasms may be relieved by the consumption of alcohol, relaxation, or the touching of the affected areas.[86] Electromyography may reveal distinctive lateral spread responses in hemifacial spasm, thereby differentiating it from blepharospasm. Hemifacial spasms may be associated with low-pitched tinnitus, which is believed to occur due to contraction of the stapedius muscle.[87] Compression by an ectatic vessel, typically the vertebral artery or the anterior/posterior cerebellar artery, is the most common underlying cause of hemifacial spasm.[85] Following botulinum toxin injection, 85% to 90% of patients experience improvement in their symptoms. Patients refractory to botulinum toxin injection may benefit from vascular decompression.[84] This condition is different from BEB, which is bilateral and originates from central dystonia.
Myasthenia Gravis
Myasthenia gravis needs to be considered in the differential diagnosis, especially when eyelid dysfunction is pronounced. In myasthenia gravis, fluctuating ptosis, diplopia, and orbicularis oculi weakness are prevalent. Spontaneous spasms, however, are generally absent.[88] Fatigability with prolonged upgaze, amelioration with rest, and affirmative results on acetylcholine receptor antibody assays or recurrent nerve stimulation favor myasthenia gravis over blepharospasm.
Post-Facial Palsy Synkinesis
Nerve regeneration occurs after an episode of facial nerve palsy. If there is aberrant muscle reinnervation, synkinesis between the lower and upper facial muscles may occur following facial palsy. This condition typically occurs 6 months after an episode of Bell's palsy.[89] This condition does not tend to present with spontaneous spasms.[90] The prevalence of synkinesis following facial nerve palsy ranges from 8.9% to 51%.[91] Postparalytic synkinesis has been reported more frequently in patients with infectious or idiopathic causes of facial nerve palsy, as well as in those who experienced partial paralysis without requiring reanimation surgery.[91] Patients suffering from post-facial palsy synkinesis tend to present with abnormal, involuntary facial movements. There are different patterns of synkinesis, such as oral-ocular, which presents with non-intended eye closure on voluntary movement of the muscles of the mouth. Ocular-oral synkinesis occurs when voluntary eye movements lead to non-intended movements of the muscles of the mouth.[92]
Psychogenic Facial Spasm
Psychogenic or functional movement disorders may sometimes resemble blepharospasm. Patients with these disorders often exhibit erratic, distractible, or nonphysiological eyelid movements that do not align with dystonic patterns. Studies have shown that the mean age of psychogenic spasms is 34.6 years.[93] Individuals suffering from psychogenic facial spasm tend to present with a non-patterned, variable facial spasm.[89] The facial spasm is distractible, such that asking the patient to perform a task reduces symptoms. The facial spasms are also bilateral and asynchronous, and worsen with anxiety and stress.[85] Characteristics such as sudden onset, attentional fluctuations, or unexpected enhancement during assessment suggest functional causes. Patients suffering from psychogenic facial spasms may be differentiated from dystonic conditions by the presence of particular clinical signs. Psychogenic facial spasm typically involves the muscles of the lower face (downward deviation of the angle of the mouth). Furthermore, the brow-lift sign may be observed, which consists of the frontalis and orbicularis oculi muscles contracting, leading to a raising of the eyebrow during occlusion of the eye.
Facial Motor Tics
Facial motor tics tend to be brief and stereotyped. The motor tic may resemble a normal, coordinated voluntary movement. A patient with facial motor tics may have a sudden urge or premonitory feeling to perform the movement. As such, the patient may be able to suppress the movement with effort.[85] These motor tics may be associated with limb motor tics and other features of Tourette syndrome.[94]
Facial Myokymia
Myokymia is characterized by undulating, rippling movements affecting individual muscle fascicles, which may involve either the upper or lower eyelid. This condition is associated with sleep deprivation, excessive caffeine consumption, and excessive fatigue.[89] Electromyography in patients with facial myokymia reveals brief, sudden bursts of doublets, triplets, or higher-order multiples arising from repetitively firing motor unit potentials. Facial myokymia is typically self-limiting but may need botulinum toxin injections in some cases. In most patients, a single injection cures the condition.
Tardive Dyskinesia
Tardive dyskinesia is characterized by repetitive, involuntary movements involving the orofacial region, including lip smacking, tongue protrusion, and excessive blinking. These movements are typically irregular and asynchronous and may involve muscles not innervated by the facial nerve, such as the masseter or the extrinsic tongue muscles. Tardive dyskinesia is a potential complication of long-term neuroleptic use.[89]
Reflex Blepharospasm
Another significant factor is reflex blepharospasm, which originates from ocular surface irritation rather than dystonia. Individuals with dry eye disease, corneal foreign bodies, trichiasis, uveitis, or blepharitis may exhibit excessive blinking or eyelid closure in response to nociceptive stimuli. In contrast to BEB, reflex blepharospasm generally subsides upon rectification of the underlying ocular condition.[95] Symptoms, including photophobia, foreign-body sensation, and ocular pain, are more prominent in reflex blepharospasm, although the dystonic nature of the spasms is less apparent. Slit-lamp examination and ocular surface testing are consequently key components of the diagnostic workup. The high incidence of dry eye disease in individuals with blepharospasm complicates this differentiation; nonetheless, the presence of dystonic patterns and bilateral involvement supports a diagnosis of blepharospasm rather than reflex-induced spasm.[75]
Staging
Staging BEB has distinct issues, as BEB is a functional neurological illness lacking clear anatomical progression or biomarker-defined stages. In contrast to neoplastic or degenerative diseases, BEB does not exhibit a linear or predictable progression, and there is no universally recognized staging scheme. Clinicians evaluate severity, functional impairment, and disease distribution with standardized grading scales that act as practical substitutes for staging. These instruments enable clinicians to categorize patients by symptom severity, frequency, and impact on daily activities, facilitating personalized treatment strategies and ongoing assessment over time. Contemporary clinical research and worldwide movement disorder recommendations endorse the utilization of functional staging measures, highlighting the importance of standardized evaluation for clinical care and research.[1]
The JRS is the most widely used clinical instrument for assessing the severity of blepharospasm.[96] The JRS comprises 2 domains—the severity of eyelid closure and the frequency of spasms. Each domain is rated on a scale of 0 to 4, with 0 indicating normal blinking and 4 indicating debilitating spasms that severely hinder visual function. The JRS, initially designed as a clinical grading scale rather than a disease staging system, efficiently categorizes individuals into mild (scores 1-2), moderate (3), and severe (4) classifications based on functional impairment. A cumulative JRS score of 6 or higher is commonly used to classify patients with functionally significant BEB who may require active intervention. Recent extensive studies assessing quality of life and botulinum toxin outcomes have used JRS as the primary measure of disease severity, thereby solidifying its role as a de facto staging instrument in clinical and research contexts.
The BSDI evaluates functional status by measuring difficulty with 6 daily activities—reading, watching television, shopping, walking, driving, and performing routine duties.[97] Scores vary from 0 (no handicap) to 4 (complete inability to execute the task). The BSDI offers a perspective on how BEB diminishes functional capacity and visually reliant activities. Studies suggest a substantial correlation between BSDI scores and JRS severity, as well as with patient-reported quality-of-life metrics. Functional staging is particularly crucial because BEB severity frequently varies with environmental stimuli, emotional stress, and sleep quality, rendering physician observation alone inadequate for assessing disease burden.
Prognosis
BEB is characterized by a chronic, non–life-threatening condition that can cause considerable functional impairment. BEB generally has a progressive trajectory, spanning several months to years, commencing with heightened blinking or eyelid discomfort and progressing to involuntary spasms that disrupt everyday activities. Although the illness does not affect life expectancy, its impact on the quality of life can be significant, affecting employment, driving, social relationships, and psychological well-being. Longitudinal observational studies indicate that BEB rarely experiences spontaneous remission. Most patients endure persistent symptoms that vary in intensity with stress, fatigue, visual tasks, and ocular surface conditions. In the absence of treatment, numerous individuals report a gradual deterioration that ultimately restricts their capacity to execute visually dependent activities.
The life expectancy of patients with isolated BEB appears unaffected by the disease. However, it poses a tremendous impact on the quality of life. In a series of 238 patients with BEB or Meige syndrome reported by Castelbuono and Miller, 27 (11.3%) experienced spontaneous remission and good quality of life. Several patients experience a constant fear of the disease worsening, reaching a point where they need increasing doses of botulinum toxin to achieve symptom improvement or worsen to a level where the response to the botulinum toxin is inadequate.[98] There is also a sense of insecurity and embarrassment when performing social tasks, which, in turn, results in social withdrawal.[99][100]
The prognosis of BEB is significantly affected by prompt diagnosis, tailored treatment, and comprehensive control of relevant factors. With proper management, most patients can maintain functional autonomy and quality of life despite the chronicity of the condition. Progress in understanding brain circuit dysfunction may facilitate the development of more precise therapeutics in the future, potentially enhancing long-term outcomes beyond those achievable with symptomatic treatment alone.
Complications
Complications associated with BEB arise from the inherent disease progression and its treatments. Although BEB does not endanger life expectancy, its complications can profoundly impact visual function, autonomy, and overall quality of life. Functional blindness is one of the most significant complications and occurs when involuntary eyelid closure prevents reliable visual input despite anatomically intact eyes. This issue results in challenges executing fundamental activities such as reading, walking securely, or driving. Numerous patients describe instances of sudden visual impairment due to prolonged spasms that render them incapable of actively opening their eyelids. These functional impairments elevate the risk of falls, injuries, and vehicular accidents. Observational studies indicate that a subset of patients with BEB experience accidents directly linked to compromised eyelid control, underscoring the safety risks associated with inadequate treatment or severe disease manifestations (Hirunwiwatkul et al, 2023, PMID: 36915360).
Botulinum toxin therapy, although highly effective, may be associated with adverse effects related to its pharmacological action. The predominant unfavorable consequence is ptosis, caused by the inadvertent passage of the toxin to the levator palpebrae muscle.[70] The incidence of ptosis following botulinum toxin injection for blepharospasm has been reported to vary between studies (5.88%-20%), and this variability is thought to result from differences in injection technique and the amount of botulinum toxin injected. Methods that have been shown to reduce the likelihood of ptosis following botulinum toxin injection include staying away from the eyelid center when injecting the toxin.
Weakness of the orbicularis oculi muscle can lead to lagophthalmos, which may cause dry eye and exposure keratitis. Other potential adverse effects include lagophthalmos, worsening of dry eye, diplopia, and localized bruising.[67] The majority of difficulties are temporary, subsiding within days to weeks as neuromuscular connections recuperate. Prolonged safety investigations indicate that repeated injections over several years are well tolerated and do not result in cumulative harm.[101] Some patients may produce neutralizing antibodies that diminish the effectiveness of therapy, requiring an alteration in toxin composition or treatment approach. Overcorrection or unbalanced injection techniques might result in uneven eyelid closure or distorted facial expressions, underscoring the necessity for skilled injectors.
Because many patients with blepharospasm exhibit varying degrees of apraxia of eyelid opening, injections are typically administered into the pretarsal portion of the orbicularis oculi muscle. Patients should be advised to apply lubricating ointment to the eyes for the first 2 to 3 weeks after injections and to increase the use of topical lubrication during this period. Botulinum toxin injection has been shown to cause reduced lacrimal drainage as a result of a lower blink rate and laxity of the lower eyelid due to paralysis of the lacrimal portion of the orbicularis oculi muscle.[72]
Comorbid disorders cansignificantly affect prognosis. Psychiatric comorbidities, including anxiety and depression, are widespread in BEB and correlate with heightened spasm intensity, diminished quality-of-life scores, and decreased therapy efficacy.[102] Mood disorders may intensify brain excitability in motor networks, leading to enduring or variable symptoms.[8] Likewise, sleep problems have been recognized as both factors exacerbating symptoms and outcomes of chronic dystonia.[103] Effective management of these comorbidities—through pharmacological treatment, counseling, or lifestyle changes—can significantly improve BEB outcomes. Additionally, ocular surface disease represents a critical prognostic factor.
Deterrence and Patient Education
Patient education and counseling are fundamental elements in the management of BEB, given that the illness is chronic, functionally restrictive, and responsive to environmental and behavioral influences. Early education of patients along the disease trajectory facilitates their recognition of triggers, adoption of compensatory techniques, and understanding of the significance of continuous therapy. Symptoms of BEB frequently vary with stress, fatigue, light exposure, and ocular surface abnormalities; hence, enabling patients to recognize and manage these factors is crucial for symptom regulation. Clinicians must clarify that while BEB is a benign, non–life-threatening condition, it can lead to considerable disability if not properly controlled. Providing comprehensive information about the chronic course of the disease and the role of botulinum toxin as a long-term therapy fosters realistic expectations, improves adherence, and reduces anxiety. Patients who comprehend the regular cycle of discomfort alleviation and recurrence post-injection often express more satisfaction and reduced anxiety concerning treatment time.
Environmental modification is an actionable technique that patients can adopt without delay. Intense illumination, wind, and visually taxing activities frequently worsen spasms; hence, using tinted lenses, wraparound eyewear, and environmental modifications can significantly reduce symptom severity. Numerous individuals benefit from tinted lenses, which have been shown to minimize photophobia and blinking frequency in patients with light sensitivity. Patients should be instructed to adjust screen brightness, increase font size, and take regular breaks during visually demanding tasks. Proper sleep hygiene is a crucial educational component, as sleep deprivation and irregular sleep cycles frequently exacerbate the severity of dystonia. Adhering to a regular sleep schedule, limiting evening caffeine intake, and reducing screen exposure at night can help stabilize symptoms. Moreover, stress management strategies—such as mindfulness, breathing exercises, or counseling—can diminish central neuronal excitability and enhance symptom regulation. These lifestyle improvements synergistically complement medical therapy.
Pearls and Other Issues
Several key clinical insights can enhance the diagnosis and management of BEB. Diagnosis is primarily clinical, with careful observation often providing more valuable insights than laboratory or imaging examinations. The pattern of involuntary eyelid closure—bilateral, nonrhythmic, and responsive to stimuli—differentiates BEB from other etiologies of excessive blinking. A significant diagnostic indicator is the presence of a sensory trick, or geste antagoniste, in which gentle contact with the brow or temple momentarily alleviates spasms. This condition is indicative of dystonia and can assist in distinguishing BEB from psychogenic or reflex blepharospasm. Another significant point is that BEB frequently commences insidiously, characterized by heightened blinking or ocular discomfort, and may be erroneously ascribed to dry eye or allergies. Neglecting to identify early signs may result in avoidable treatment delays, underscoring the need for physicians to maintain heightened skepticism when assessing persistent blinking abnormalities.[1]
Enhancing Healthcare Team Outcomes
Optimal management of patients with BEB requires a collaborative, interdisciplinary approach that integrates the expertise of ophthalmologists, neurologists, primary care physicians, nurses, pharmacists, and allied health practitioners. Due to BEB being a chronic neurological disorder with considerable functional and psychosocial ramifications, collaborative management improves diagnostic precision, refines treatment approaches, and promotes long-term results.[51] Ophthalmologists and neurologists frequently collaborate to verify the diagnosis and distinguish blepharospasm from disorders such as hemifacial spasm, myasthenia gravis, or ocular surface disease.[99] Neurologists provide specialized knowledge of movement disorders and injection techniques, whilst ophthalmologists evaluate ocular surface integrity and address complications such as exposure keratopathy or dry eye syndrome. Primary care physicians are crucial in detecting early symptoms, identifying comorbidities, and facilitating quick referrals to specialists. This collaborative structure ensures a comprehensive approach to BEB, rather than treating it as a single motor problem.
Nurses are essential in facilitating patient education, assessing the efficacy of therapy, and identifying complications associated with botulinum toxin injections. Their role is fundamental in pre- and post-injection care, assisting patients in understanding anticipated symptom relief and potential adverse effects, and enhancing communication between patients and clinicians. Allied health professionals, such as optometrists, occupational therapists, psychologists, and social workers, improve the multidisciplinary team. Optometrists facilitate ocular surface assessment, tear-film regulation, and the detection of refractive or visual elements that may exacerbate blinking. They also assist patients with choosing suitable tinted lenses or adaptive visual aids. Occupational therapists help patients in altering work surroundings, driving behaviors, and daily activities to mitigate symptom triggers and promote autonomy. Psychologists are crucial in managing anxiety, depression, and social withdrawal, which are prevalent and can intensify dystonia by heightening neuronal excitability. Social workers assist patients in obtaining community resources, disability benefits, support groups, or counseling services, thereby enhancing coping methods and alleviating the isolation sometimes encountered by those with BEB.
Media
(Click Video to Play)
Typical Blepharospasm. This video illustrates a typical case of blepharospasm, characterized by an increased blink rate and intermittent but random squeezing of the eyelids and periorbital tissues. An overaction of the corrugator, procerus, and orbicularis muscles can be observed. In addition, brow ptosis, ptosis, and dermatochalasis can be observed, all of which are exacerbated by blepharospasm.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)

Botulinum Toxin Injections for Blepharospasm. Botulinum toxin injections may be administered at various sites. The dosage varies depending on the severity of the blepharospasm and apraxia of eyelid opening at each specific point. Pretarsal injections are administered to specifically counteract apraxia of eyelid opening. Injections just lateral to the lateral nasal wall aim to alleviate the squeezing of the nasalis muscle, which is observed in some patients. Injections into the corrugator and procerus muscles reduce the downward movement of the brow, consequently aiding eyelid control. Injections just below the brows provide a chemical lift, thereby improving the ability to open the eyelids. Caution is warranted to inject a minimal amount over the zygomaticus major and minor muscles to prevent the appearance of lower facial weakness following injections.
Contributed by BCK Patel, MD, FRCS
(Click Image to Enlarge)
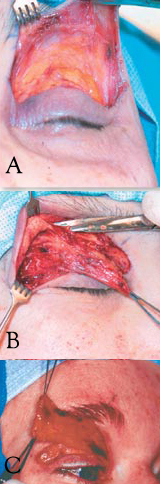
Limited Myectomy for Blepharospasm. The upper eyelid orbital and preseptal orbicularis muscle are dissected from the skin through an eyelid crease incision. The degree to which the pretarsal muscle is removed is determined by the extent of apraxia of eyelid opening (A). Care is exercised to safeguard the skin through meticulous dissection (B). The image illustrates en bloc removal of the orbicularis muscle (C).
Contributed by BCK Patel, MD, FRCS
References
Hirunwiwatkul P, Supawatjariyakul W, Jariyakosol S, Apinyawasisuk S, Sriratanaban J, Chongpison Y, Jagota P, Aui-Aree N, Witthayaweerasak J, Setthawatcharawanich S, Kitthaweesin K, Chirapapaisan N, Chaimongkoltrakul P, Laowanapiban P, Hansapinyo L, Panpitpat S, Kurathong S, Nimworaphan J, Thitiwichienlert S, Vanikieti K, Samipak N, Srimanan W, Mekhasingharak N, Chaitanuwong P. Health-related quality of life of daily-life-affected benign essential blepharospasm: Multi-center observational study. PloS one. 2023:18(3):e0283111. doi: 10.1371/journal.pone.0283111. Epub 2023 Mar 15 [PubMed PMID: 36920965]
Level 2 (mid-level) evidenceSun Y, Tsai PJ, Chu CL, Huang WC, Bee YS. Epidemiology of benign essential blepharospasm: A nationwide population-based retrospective study in Taiwan. PloS one. 2018:13(12):e0209558. doi: 10.1371/journal.pone.0209558. Epub 2018 Dec 26 [PubMed PMID: 30586395]
Level 2 (mid-level) evidenceAlbanese A, Bhatia K, Bressman SB, Delong MR, Fahn S, Fung VS, Hallett M, Jankovic J, Jinnah HA, Klein C, Lang AE, Mink JW, Teller JK. Phenomenology and classification of dystonia: a consensus update. Movement disorders : official journal of the Movement Disorder Society. 2013 Jun 15:28(7):863-73. doi: 10.1002/mds.25475. Epub 2013 May 6 [PubMed PMID: 23649720]
Level 3 (low-level) evidenceJinnah HA, Factor SA. Diagnosis and treatment of dystonia. Neurologic clinics. 2015 Feb:33(1):77-100. doi: 10.1016/j.ncl.2014.09.002. Epub [PubMed PMID: 25432724]
Gautam P, Bhatia MS, Kaur J, Rathi A. Meige's syndrome. Industrial psychiatry journal. 2016 Jul-Dec:25(2):232-233. doi: 10.4103/0972-6748.207853. Epub [PubMed PMID: 28659707]
Poonyathalang A, Tiraset N, Rattanathamsakul N. Effectiveness of 0.3% Hyaluronic Acid Eye Drops for Benign Essential Blepharospasm and Hemifacial Spasm with Botulinum Toxin-induced Dry Eye. Plastic and reconstructive surgery. Global open. 2024 Aug:12(8):e6050. doi: 10.1097/GOX.0000000000006050. Epub 2024 Aug 13 [PubMed PMID: 39139840]
Altin Ekin M, Erkose Erbay G, Soylev Bajin M. Lid wiper epitheliopathy and ocular surface dysfunction in benign essential blepharospasm before and after botulinum toxin-A injection. International ophthalmology. 2025 Nov 13:45(1):473. doi: 10.1007/s10792-025-03871-1. Epub 2025 Nov 13 [PubMed PMID: 41231346]
Zhou Y, Wang W, Lin Z, Lin T, Gong L. Relations between nonmotor manifestations and motor disorders in patients with benign essential blepharospasm. Graefe's archive for clinical and experimental ophthalmology = Albrecht von Graefes Archiv fur klinische und experimentelle Ophthalmologie. 2023 Dec:261(12):3615-3623. doi: 10.1007/s00417-023-06141-x. Epub 2023 Jun 21 [PubMed PMID: 37341835]
Girard BC, Abdellaoui M, de Saint Sauveur G, Huang A, Lévy P. Blepharospasm, dry eye and extractable nuclear antigen antibodies. Journal francais d'ophtalmologie. 2020 Sep:43(7):e211-e215. doi: 10.1016/j.jfo.2020.06.001. Epub 2020 Jun 10 [PubMed PMID: 32532571]
Bali J, Navin N, Thakur BR. Computer vision syndrome: a study of the knowledge, attitudes and practices in Indian ophthalmologists. Indian journal of ophthalmology. 2007 Jul-Aug:55(4):289-94 [PubMed PMID: 17595478]
Level 2 (mid-level) evidenceKuyper DJ, Parra V, Aerts S, Okun MS, Kluger BM. Nonmotor manifestations of dystonia: a systematic review. Movement disorders : official journal of the Movement Disorder Society. 2011 Jun:26(7):1206-17. doi: 10.1002/mds.23709. Epub 2011 Apr 11 [PubMed PMID: 21484874]
Level 1 (high-level) evidenceDefazio G, Jinnah HA, Berardelli A, Perlmutter JS, Berkmen GK, Berman BD, Jankovic J, Bäumer T, Comella C, Cotton AC, Ercoli T, Ferrazzano G, Fox S, Kim HJ, Moukheiber ES, Richardson SP, Weissbach A, Wrigth LJ, Hallett M. Diagnostic criteria for blepharospasm: A multicenter international study. Parkinsonism & related disorders. 2021 Oct:91():109-114. doi: 10.1016/j.parkreldis.2021.09.004. Epub 2021 Sep 8 [PubMed PMID: 34583301]
Yakut B, Atac A, Yilmaz A, Onder F. The Role of Serum Vitamin and Mineral Levels in Benign Essential Blepharospasm: A Comparative Study. Beyoglu eye journal. 2025:10(3):149-153. doi: 10.14744/bej.2025.92260. Epub 2025 Sep 25 [PubMed PMID: 41059242]
Level 2 (mid-level) evidenceConte A, Ferrazzano G, Defazio G, Fabbrini G, Hallett M, Berardelli A. INCREASED BLINKING MAY BE A PRECURSOR OF BLEPHAROSPASM: A LONGITUDINAL STUDY. Movement disorders clinical practice. 2017 Sep-Oct:4(5):733-736. doi: 10.1002/mdc3.12499. Epub 2017 Jun 2 [PubMed PMID: 29082270]
Conte A, Berardelli I, Ferrazzano G, Pasquini M, Berardelli A, Fabbrini G. Non-motor symptoms in patients with adult-onset focal dystonia: Sensory and psychiatric disturbances. Parkinsonism & related disorders. 2016 Jan:22 Suppl 1():S111-4. doi: 10.1016/j.parkreldis.2015.09.001. Epub 2015 Sep 3 [PubMed PMID: 26360238]
Defazio G, Berardelli A, Abbruzzese G, Lepore V, Coviello V, Acquistapace D, Capus L, Carella F, De Berardinis MT, Galardi G, Girlanda P, Maurri S, Albanese A, Bertolasi L, Liguori R, Rossi A, Santoro L, Tognoni G, Livrea P. Possible risk factors for primary adult onset dystonia: a case-control investigation by the Italian Movement Disorders Study Group. Journal of neurology, neurosurgery, and psychiatry. 1998 Jan:64(1):25-32 [PubMed PMID: 9436723]
Level 2 (mid-level) evidenceDong H, Luo Y, Fan S, Yin B, Weng C, Peng B. Screening Gene Mutations in Chinese Patients With Benign Essential Blepharospasm. Frontiers in neurology. 2019:10():1387. doi: 10.3389/fneur.2019.01387. Epub 2020 Jan 23 [PubMed PMID: 32038460]
Hallett M, Evinger C, Jankovic J, Stacy M, BEBRF International Workshop. Update on blepharospasm: report from the BEBRF International Workshop. Neurology. 2008 Oct 14:71(16):1275-82. doi: 10.1212/01.wnl.0000327601.46315.85. Epub [PubMed PMID: 18852443]
Level 3 (low-level) evidenceDefazio G, Hallett M, Jinnah HA, Conte A, Berardelli A. Blepharospasm 40 years later. Movement disorders : official journal of the Movement Disorder Society. 2017 Apr:32(4):498-509. doi: 10.1002/mds.26934. Epub 2017 Feb 10 [PubMed PMID: 28186662]
Mascia MM, Dagostino S, Defazio G. Does the network model fits neurophysiological abnormalities in blepharospasm? Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2020 Aug:41(8):2067-2079. doi: 10.1007/s10072-020-04347-z. Epub 2020 Mar 25 [PubMed PMID: 32215851]
Hammer M, Abravanel A, Peckham E, Mahloogi A, Majounie E, Hallett M, Singleton A. Blepharospasm: A genetic screening study in 132 patients. Parkinsonism & related disorders. 2019 Jul:64():315-318. doi: 10.1016/j.parkreldis.2019.04.003. Epub 2019 Apr 2 [PubMed PMID: 30956059]
Xiao J, Uitti RJ, Zhao Y, Vemula SR, Perlmutter JS, Wszolek ZK, Maraganore DM, Auburger G, Leube B, Lehnhoff K, LeDoux MS. Mutations in CIZ1 cause adult onset primary cervical dystonia. Annals of neurology. 2012 Apr:71(4):458-69. doi: 10.1002/ana.23547. Epub 2012 Mar 23 [PubMed PMID: 22447717]
Misbahuddin A, Placzek MR, Chaudhuri KR, Wood NW, Bhatia KP, Warner TT. A polymorphism in the dopamine receptor DRD5 is associated with blepharospasm. Neurology. 2002 Jan 8:58(1):124-6 [PubMed PMID: 11781417]
Corvol JC, Studler JM, Schonn JS, Girault JA, Hervé D. Galpha(olf) is necessary for coupling D1 and A2a receptors to adenylyl cyclase in the striatum. Journal of neurochemistry. 2001 Mar:76(5):1585-8 [PubMed PMID: 11238742]
Level 3 (low-level) evidenceFuchs T, Saunders-Pullman R, Masuho I, Luciano MS, Raymond D, Factor S, Lang AE, Liang TW, Trosch RM, White S, Ainehsazan E, Hervé D, Sharma N, Ehrlich ME, Martemyanov KA, Bressman SB, Ozelius LJ. Mutations in GNAL cause primary torsion dystonia. Nature genetics. 2013 Jan:45(1):88-92. doi: 10.1038/ng.2496. Epub 2012 Dec 9 [PubMed PMID: 23222958]
Mitsui K, Matsumoto A, Ohtsuka S, Ohtsubo M, Yoshimura A. Cloning and characterization of a novel p21(Cip1/Waf1)-interacting zinc finger protein, ciz1. Biochemical and biophysical research communications. 1999 Oct 22:264(2):457-64 [PubMed PMID: 10529385]
Konakova M, Huynh DP, Yong W, Pulst SM. Cellular distribution of torsin A and torsin B in normal human brain. Archives of neurology. 2001 Jun:58(6):921-7 [PubMed PMID: 11405807]
Level 3 (low-level) evidenceAugood SJ, Penney JB Jr, Friberg IK, Breakefield XO, Young AB, Ozelius LJ, Standaert DG. Expression of the early-onset torsion dystonia gene (DYT1) in human brain. Annals of neurology. 1998 May:43(5):669-73 [PubMed PMID: 9585364]
Hewett J, Gonzalez-Agosti C, Slater D, Ziefer P, Li S, Bergeron D, Jacoby DJ, Ozelius LJ, Ramesh V, Breakefield XO. Mutant torsinA, responsible for early-onset torsion dystonia, forms membrane inclusions in cultured neural cells. Human molecular genetics. 2000 May 22:9(9):1403-13 [PubMed PMID: 10814722]
Level 3 (low-level) evidenceOzelius LJ, Hewett JW, Page CE, Bressman SB, Kramer PL, Shalish C, de Leon D, Brin MF, Raymond D, Corey DP, Fahn S, Risch NJ, Buckler AJ, Gusella JF, Breakefield XO. The early-onset torsion dystonia gene (DYT1) encodes an ATP-binding protein. Nature genetics. 1997 Sep:17(1):40-8 [PubMed PMID: 9288096]
Level 3 (low-level) evidenceGrandy DK, Zhang YA, Bouvier C, Zhou QY, Johnson RA, Allen L, Buck K, Bunzow JR, Salon J, Civelli O. Multiple human D5 dopamine receptor genes: a functional receptor and two pseudogenes. Proceedings of the National Academy of Sciences of the United States of America. 1991 Oct 15:88(20):9175-9 [PubMed PMID: 1833775]
Level 3 (low-level) evidencePolymeropoulos MH, Xiao H, Merril CR. The human D5 dopamine receptor (DRD5) maps on chromosome 4. Genomics. 1991 Nov:11(3):777-8 [PubMed PMID: 1774076]
Level 3 (low-level) evidenceSteeves TD, Day L, Dykeman J, Jette N, Pringsheim T. The prevalence of primary dystonia: a systematic review and meta-analysis. Movement disorders : official journal of the Movement Disorder Society. 2012 Dec:27(14):1789-96. doi: 10.1002/mds.25244. Epub 2012 Oct 31 [PubMed PMID: 23114997]
Level 1 (high-level) evidenceDefazio G, Livrea P. Epidemiology of primary blepharospasm. Movement disorders : official journal of the Movement Disorder Society. 2002 Jan:17(1):7-12 [PubMed PMID: 11835433]
Martino D, Livrea P, Giorelli M, Masi G, Aniello MS, Defazio G. Menopause and menarche in patients with primary blepharospasm: an exploratory case-control study. European neurology. 2002:47(3):161-4 [PubMed PMID: 11914554]
Level 2 (mid-level) evidenceSnir M, Weinberger D, Bourla D, Kristal-Shalit O, Dotan G, Axer-Siegel R. Quantitative changes in botulinum toxin a treatment over time in patients with essential blepharospasm and idiopathic hemifacial spasm. American journal of ophthalmology. 2003 Jul:136(1):99-105 [PubMed PMID: 12834676]
Level 2 (mid-level) evidenceValls-Sole J, Defazio G. Blepharospasm: Update on Epidemiology, Clinical Aspects, and Pathophysiology. Frontiers in neurology. 2016:7():45. doi: 10.3389/fneur.2016.00045. Epub 2016 Mar 31 [PubMed PMID: 27064462]
Evinger C. Benign Essential Blepharospasm is a Disorder of Neuroplasticity: Lessons From Animal Models. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2015 Dec:35(4):374-9. doi: 10.1097/WNO.0000000000000317. Epub [PubMed PMID: 26576017]
Level 3 (low-level) evidenceLee JM, Baek JS, Choi HS, Kim SJ, Jang JW. Clinical Features of Benign Essential Blepharospasm in Korean Patients. Korean journal of ophthalmology : KJO. 2018 Oct:32(5):339-343. doi: 10.3341/kjo.2018.0038. Epub [PubMed PMID: 30311455]
Hallett M. Blepharospasm: recent advances. Neurology. 2002 Nov 12:59(9):1306-12 [PubMed PMID: 12434791]
Level 3 (low-level) evidenceJankovic J, Havins WE, Wilkins RB. Blinking and blepharospasm. Mechanism, diagnosis, and management. JAMA. 1982 Dec 17:248(23):3160-4 [PubMed PMID: 7143695]
Hwang CJ, Eftekhari K. Benign Essential Blepharospasm: What We Know and What We Don't. International ophthalmology clinics. 2018 Winter:58(1):11-24. doi: 10.1097/IIO.0000000000000207. Epub [PubMed PMID: 29239874]
Suzuki Y, Mizoguchi S, Kiyosawa M, Mochizuki M, Ishiwata K, Wakakura M, Ishii K. Glucose hypermetabolism in the thalamus of patients with essential blepharospasm. Journal of neurology. 2007 Jul:254(7):890-6 [PubMed PMID: 17325818]
Etgen T, Mühlau M, Gaser C, Sander D. Bilateral grey-matter increase in the putamen in primary blepharospasm. Journal of neurology, neurosurgery, and psychiatry. 2006 Sep:77(9):1017-20 [PubMed PMID: 16690695]
Level 2 (mid-level) evidenceBaker RS, Andersen AH, Morecraft RJ, Smith CD. A functional magnetic resonance imaging study in patients with benign essential blepharospasm. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2003 Mar:23(1):11-5 [PubMed PMID: 12616082]
Level 2 (mid-level) evidenceHorie C, Suzuki Y, Kiyosawa M, Mochizuki M, Wakakura M, Oda K, Ishiwata K, Ishii K. Decreased dopamine D receptor binding in essential blepharospasm. Acta neurologica Scandinavica. 2009 Jan:119(1):49-54. doi: 10.1111/j.1600-0404.2008.01053.x. Epub 2008 Jun 5 [PubMed PMID: 18540899]
Jinnah HA, Berardelli A, Comella C, Defazio G, Delong MR, Factor S, Galpern WR, Hallett M, Ludlow CL, Perlmutter JS, Rosen AR, Dystonia Coalition Investigators. The focal dystonias: current views and challenges for future research. Movement disorders : official journal of the Movement Disorder Society. 2013 Jun 15:28(7):926-43. doi: 10.1002/mds.25567. Epub [PubMed PMID: 23893450]
Romero-Caballero MD, Salmerón Ato MP, Palazón-Cabanes A, Caravaca-Alegría A. Lid wiper epitheliopathy in patients with blepharospasm and/or hemifacial spasm. Archivos de la Sociedad Espanola de Oftalmologia. 2022 Jul:97(7):376-380. doi: 10.1016/j.oftale.2022.03.008. Epub 2022 Mar 12 [PubMed PMID: 35292220]
Wakakura M, Yamagami A, Iwasa M. Blepharospasm in Japan: A Clinical Observational Study From a Large Referral Hospital in Tokyo. Neuro-ophthalmology (Aeolus Press). 2018 Oct:42(5):275-283. doi: 10.1080/01658107.2017.1409770. Epub 2018 Jan 9 [PubMed PMID: 30258472]
Level 2 (mid-level) evidenceKrack P, Marion MH. "Apraxia of lid opening," a focal eyelid dystonia: clinical study of 32 patients. Movement disorders : official journal of the Movement Disorder Society. 1994 Nov:9(6):610-5 [PubMed PMID: 7845400]
Elston JS, Marsden CD, Grandas F, Quinn NP. The significance of ophthalmological symptoms in idiopathic blepharospasm. Eye (London, England). 1988:2 ( Pt 4)():435-9 [PubMed PMID: 3253136]
Hirunwiwatkul P, Permsuwan U, Ngamkiatphaisan S, Chirapapaisan N, Sriratanaban J. Cost-utility analysis of botulinum toxin type A versus oral drug treatment in patients with severe blepharospasm in Thailand. PloS one. 2025:20(4):e0319926. doi: 10.1371/journal.pone.0319926. Epub 2025 Apr 21 [PubMed PMID: 40257973]
Defazio G, Hallett M, Jinnah HA, Stebbins GT, Gigante AF, Ferrazzano G, Conte A, Fabbrini G, Berardelli A. Development and validation of a clinical scale for rating the severity of blepharospasm. Movement disorders : official journal of the Movement Disorder Society. 2015 Apr:30(4):525-30. doi: 10.1002/mds.26156. Epub [PubMed PMID: 25847472]
Level 1 (high-level) evidenceDefazio G, Hallett M, Jinnah HA, Berardelli A. Development and validation of a clinical guideline for diagnosing blepharospasm. Neurology. 2013 Jul 16:81(3):236-40. doi: 10.1212/WNL.0b013e31829bfdf6. Epub 2013 Jun 14 [PubMed PMID: 23771487]
Level 1 (high-level) evidenceDefazio G, Conte A, Gigante AF, Fabbrini G, Berardelli A. Is tremor in dystonia a phenotypic feature of dystonia? Neurology. 2015 Mar 10:84(10):1053-9. doi: 10.1212/WNL.0000000000001341. Epub 2015 Feb 6 [PubMed PMID: 25663232]
Martino D, Defazio G, Alessio G, Abbruzzese G, Girlanda P, Tinazzi M, Fabbrini G, Marinelli L, Majorana G, Buccafusca M, Vacca L, Livrea P, Berardelli A. Relationship between eye symptoms and blepharospasm: a multicenter case-control study. Movement disorders : official journal of the Movement Disorder Society. 2005 Dec:20(12):1564-70 [PubMed PMID: 16092106]
Level 2 (mid-level) evidenceJankovic J, Orman J. Botulinum A toxin for cranial-cervical dystonia: a double-blind, placebo-controlled study. Neurology. 1987 Apr:37(4):616-23 [PubMed PMID: 3561773]
Level 1 (high-level) evidenceGarcía Estévez DA, Pardo Fernández J. Myasthenia gravis. Update on diagnosis and therapy. Medicina clinica. 2023 Aug 11:161(3):119-127. doi: 10.1016/j.medcli.2023.04.006. Epub 2023 May 27 [PubMed PMID: 37248131]
Jesuthasan A, Natalwala A, Davagnanam I, Saifee T, Zrinzo L. Hemifacial spasm: an update on pathophysiology, investigations and management. Journal of neurology. 2025 Jul 10:272(8):502. doi: 10.1007/s00415-025-13220-y. Epub 2025 Jul 10 [PubMed PMID: 40640398]
Nguyen P, Kelly D, Glickman A, Argaw S, Shelton E, Peterson DA, Berman BD. Abnormal Neural Responses During Reflexive Blinking in Blepharospasm: An Event-Related Functional MRI Study. Movement disorders : official journal of the Movement Disorder Society. 2020 Jul:35(7):1173-1180. doi: 10.1002/mds.28042. Epub 2020 Apr 6 [PubMed PMID: 32250472]
Jinnah HA. The Dystonias. Continuum (Minneapolis, Minn.). 2019 Aug:25(4):976-1000. doi: 10.1212/CON.0000000000000747. Epub [PubMed PMID: 31356290]
Grandas F, Traba A, Perez-Sanchez JR, Esteban A. Pretarsal blepharospasm: Clinical and electromyographic characteristics. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2020 Jul:131(7):1678-1685. doi: 10.1016/j.clinph.2020.03.016. Epub 2020 Apr 2 [PubMed PMID: 32280019]
Kimura J. Disorder of interneurons in Parkinsonism. The orbicularis oculi reflex to paired stimuli. Brain : a journal of neurology. 1973:96(1):87-96 [PubMed PMID: 4695726]
Yen MT. Developments in the treatment of benign essential blepharospasm. Current opinion in ophthalmology. 2018 Sep:29(5):440-444. doi: 10.1097/ICU.0000000000000500. Epub [PubMed PMID: 29916840]
Level 3 (low-level) evidenceHerz NL, Yen MT. Modulation of sensory photophobia in essential blepharospasm with chromatic lenses. Ophthalmology. 2005 Dec:112(12):2208-11 [PubMed PMID: 16242188]
Level 2 (mid-level) evidenceBlackburn MK, Lamb RD, Digre KB, Smith AG, Warner JE, McClane RW, Nandedkar SD, Langeberg WJ, Holubkov R, Katz BJ. FL-41 tint improves blink frequency, light sensitivity, and functional limitations in patients with benign essential blepharospasm. Ophthalmology. 2009 May:116(5):997-1001. doi: 10.1016/j.ophtha.2008.12.031. Epub [PubMed PMID: 19410958]
Level 2 (mid-level) evidenceAbabneh OH, Cetinkaya A, Kulwin DR. Long-term efficacy and safety of botulinum toxin A injections to treat blepharospasm and hemifacial spasm. Clinical & experimental ophthalmology. 2014 Apr:42(3):254-61. doi: 10.1111/ceo.12165. Epub 2013 Aug 4 [PubMed PMID: 23844601]
Level 2 (mid-level) evidenceNoor MA, Abul A, Saleki M, Alkhabbaz A, Abel A, Karam M, Al-Youha S. Botulinum Toxin Injection for Hemifacial Spasm and Benign Essential Blepharospasm: A Systematic Review and Meta-Analysis Comparing Pretarsal and Preseptal Injection Techniques. Aesthetic plastic surgery. 2025 Jul:49(13):3618-3628. doi: 10.1007/s00266-025-04913-w. Epub 2025 May 29 [PubMed PMID: 40442495]
Level 1 (high-level) evidenceHellman A, Torres-Russotto D. Botulinum toxin in the management of blepharospasm: current evidence and recent developments. Therapeutic advances in neurological disorders. 2015 Mar:8(2):82-91. doi: 10.1177/1756285614557475. Epub [PubMed PMID: 25922620]
Level 3 (low-level) evidenceAnwar MS, Zafar H. Efficacy of botulinum toxin in benign essential Blepharospasm: Desirable & undesirable effects. Pakistan journal of medical sciences. 2013 Nov:29(6):1389-93 [PubMed PMID: 24550960]
Ramirez-Castaneda J, Jankovic J. Long-term efficacy and safety of botulinum toxin injections in dystonia. Toxins. 2013 Feb 4:5(2):249-66. doi: 10.3390/toxins5020249. Epub 2013 Feb 4 [PubMed PMID: 23381141]
Yang H, Lu J, Zhao X, Ding X, Wang Z, Cai X, Luo Y, Lu L. Comparison of Two Botulinum Neurotoxin A Injection Patterns with or without the Medial Lower Eyelid in the Treatment of Blepharospasm. Journal of ophthalmology. 2016:2016():5957812. doi: 10.1155/2016/5957812. Epub 2016 Jan 14 [PubMed PMID: 26885381]
Scott AB, Kennedy RA, Stubbs HA. Botulinum A toxin injection as a treatment for blepharospasm. Archives of ophthalmology (Chicago, Ill. : 1960). 1985 Mar:103(3):347-50 [PubMed PMID: 3977705]
Naumann M, Albanese A, Heinen F, Molenaers G, Relja M. Safety and efficacy of botulinum toxin type A following long-term use. European journal of neurology. 2006 Dec:13 Suppl 4():35-40 [PubMed PMID: 17112348]
Level 3 (low-level) evidenceOganov A, Yazdanpanah G, Jabbehdari S, Belamkar A, Pflugfelder S. Dry eye disease and blinking behaviors: A narrative review of methodologies for measuring blink dynamics and inducing blink response. The ocular surface. 2023 Jul:29():166-174. doi: 10.1016/j.jtos.2023.05.011. Epub 2023 May 29 [PubMed PMID: 37257694]
Level 3 (low-level) evidenceGirard B, Begnaud S. [Dry eye and qualitative tear alteration in essential blepharospasm]. Journal francais d'ophtalmologie. 2022 Mar:45(3):288-297. doi: 10.1016/j.jfo.2021.09.008. Epub 2022 Feb 8 [PubMed PMID: 35148903]
Level 2 (mid-level) evidenceHassell TJW, Charles D. Treatment of Blepharospasm and Oromandibular Dystonia with Botulinum Toxins. Toxins. 2020 Apr 22:12(4):. doi: 10.3390/toxins12040269. Epub 2020 Apr 22 [PubMed PMID: 32331272]
Weller C, Leyngold I. The Facial Nerve and Selective Neurectomy for Treatment of Benign Essential Blepharospasm. International ophthalmology clinics. 2018 Winter:58(1):89-95. doi: 10.1097/IIO.0000000000000204. Epub [PubMed PMID: 29239881]
Jinnah HA. Medical and Surgical Treatments for Dystonia. Neurologic clinics. 2020 May:38(2):325-348. doi: 10.1016/j.ncl.2020.01.003. Epub 2020 Mar 2 [PubMed PMID: 32279713]
Gaudiano G, Boogers A, Grippe T, Cilia R, Eleopra R, Chen R, Fasano A. Rhythmic Eyelid Closure Responsive to STN-DBS: Blepharoclonus, Blepharospasm, Eyelid Opening Apraxia, or Eyelid Tremor? Movement disorders clinical practice. 2025 Jul:12(7):1020-1023. doi: 10.1002/mdc3.70030. Epub 2025 Mar 11 [PubMed PMID: 40067087]
Anderson RL, Patel BC, Holds JB, Jordan DR. Blepharospasm: past, present, and future. Ophthalmic plastic and reconstructive surgery. 1998 Sep:14(5):305-17 [PubMed PMID: 9783280]
Level 2 (mid-level) evidenceGillum WN, Anderson RL. Blepharospasm surgery. An anatomical approach. Archives of ophthalmology (Chicago, Ill. : 1960). 1981 Jun:99(6):1056-62 [PubMed PMID: 7236103]
Kerty E, Eidal K. Apraxia of eyelid opening: clinical features and therapy. European journal of ophthalmology. 2006 Mar-Apr:16(2):204-8 [PubMed PMID: 16703535]
Rosenstengel C, Matthes M, Baldauf J, Fleck S, Schroeder H. Hemifacial spasm: conservative and surgical treatment options. Deutsches Arzteblatt international. 2012 Oct:109(41):667-73. doi: 10.3238/arztebl.2012.0667. Epub 2012 Oct 12 [PubMed PMID: 23264807]
Tan NC, Chan LL, Tan EK. Hemifacial spasm and involuntary facial movements. QJM : monthly journal of the Association of Physicians. 2002 Aug:95(8):493-500 [PubMed PMID: 12145388]
Wang A, Jankovic J. Hemifacial spasm: clinical findings and treatment. Muscle & nerve. 1998 Dec:21(12):1740-7 [PubMed PMID: 9843077]
Chang WS, Kim BS, Lee JE, Jung HH, Kim K, Kwon HC, Lee YH, Chang JW. 'Is tinnitus accompanied by hemifacial spasm in normal-hearing patients also a type of hyperactive neurovascular compression syndrome? : A magnetoencephalography study. BMC neurology. 2013 May 8:13():42. doi: 10.1186/1471-2377-13-42. Epub 2013 May 8 [PubMed PMID: 23651913]
Naum R, Morena J. Apraxia of Eyelid Opening in Myasthenia Gravis. JAMA neurology. 2025 Jun 1:82(6):627. doi: 10.1001/jamaneurol.2025.0704. Epub [PubMed PMID: 40193110]
Lefaucheur JP, Ben Daamer N, Sangla S, Le Guerinel C. Diagnosis of primary hemifacial spasm. Neuro-Chirurgie. 2018 May:64(2):82-86. doi: 10.1016/j.neuchi.2017.12.003. Epub 2018 Apr 16 [PubMed PMID: 29673578]
Oge AE, Yayla V, Demir GA, Eraksoy M. Excitability of facial nucleus and related brain-stem reflexes in hemifacial spasm, post-facial palsy synkinesis and facial myokymia. Clinical neurophysiology : official journal of the International Federation of Clinical Neurophysiology. 2005 Jul:116(7):1542-54 [PubMed PMID: 15953558]
Salles AG, da Costa EF, Ferreira MC, do Nascimento Remigio AF, Moraes LB, Gemperli R. Epidemiologic Overview of Synkinesis in 353 Patients with Longstanding Facial Paralysis under Treatment with Botulinum Toxin for 11 Years. Plastic and reconstructive surgery. 2015 Dec:136(6):1289-1298. doi: 10.1097/PRS.0000000000001802. Epub [PubMed PMID: 26595022]
Level 3 (low-level) evidencePourmomeny AA, Asadi S. Management of synkinesis and asymmetry in facial nerve palsy: a review article. Iranian journal of otorhinolaryngology. 2014 Oct:26(77):251-6 [PubMed PMID: 25320703]
Tan EK, Jankovic J. Psychogenic hemifacial spasm. The Journal of neuropsychiatry and clinical neurosciences. 2001 Summer:13(3):380-4 [PubMed PMID: 11514645]
Level 3 (low-level) evidenceSzejko N, Jakubczyk A, Dunalska A, Janik P. Dystonic tics in patients with Gilles de la Tourette syndrome. Neurologia i neurochirurgia polska. 2019:53(5):335-340. doi: 10.5603/PJNNS.a2019.0046. Epub 2019 Oct 17 [PubMed PMID: 31621889]
Paik JS, Kwon MJ, Nam GH, Han K, Whang WJ, Hwang HS, Yang SW, Kim HS, Na KS, Cho WK. Tear film lipid layer thickness and blink dynamics in patients with blepharospasm. BMC ophthalmology. 2025 Jan 16:25(1):22. doi: 10.1186/s12886-025-03852-z. Epub 2025 Jan 16 [PubMed PMID: 39819317]
Doğan S, Yilmaz İE, Ari Ş. Effectiveness of Minimally Invasive Partial Orbicularis Myectomy for Treating Benign Essential Blepharospasm: A Study Using the Jankovic Scale and Blepharospasm Disability Index. Ophthalmic plastic and reconstructive surgery. 2025 Sep-Oct 01:41(5):560-564. doi: 10.1097/IOP.0000000000002914. Epub 2025 Feb 13 [PubMed PMID: 39945360]
Fezza J, Burns J, Woodward J, Truong D, Hedges T, Verma A. A cross-sectional structured survey of patients receiving botulinum toxin type A treatment for blepharospasm. Journal of the neurological sciences. 2016 Aug 15:367():56-62. doi: 10.1016/j.jns.2016.05.033. Epub 2016 May 16 [PubMed PMID: 27423565]
Level 2 (mid-level) evidenceTucha O, Naumann M, Berg D, Alders GL, Lange KW. Quality of life in patients with blepharospasm. Acta neurologica Scandinavica. 2001 Jan:103(1):49-52 [PubMed PMID: 11153888]
Level 2 (mid-level) evidenceHall TA, McGwin G Jr, Searcey K, Xie A, Hupp SL, Owsley C, Kline LB. Health-related quality of life and psychosocial characteristics of patients with benign essential blepharospasm. Archives of ophthalmology (Chicago, Ill. : 1960). 2006 Jan:124(1):116-9 [PubMed PMID: 16401794]
Level 2 (mid-level) evidenceCastelbuono A, Miller NR. Spontaneous remission in patients with essential blepharospasm and Meige syndrome. American journal of ophthalmology. 1998 Sep:126(3):432-5 [PubMed PMID: 9744377]
Level 2 (mid-level) evidenceWabbels B, Fimmers R, Roggenkämper P. Ultra-Long-Term Therapy of Benign Essential Blepharospasm with Botulinumtoxin A-30 Years of Experience in a Tertiary Care Center. Toxins. 2022 Feb 7:14(2):. doi: 10.3390/toxins14020120. Epub 2022 Feb 7 [PubMed PMID: 35202148]
Yin B, Peng B, Luo Y, Fan S, Xiao T, Zou X, Dong H. Efficacy of Repetitive Transcranial Magnetic Stimulation Combined with Botulinum Toxin Type A for Benign Essential Blepharospasm Patients Accompanied by Anxiety and Depression. Neuropsychiatric disease and treatment. 2021:17():2707-2711. doi: 10.2147/NDT.S316163. Epub 2021 Aug 17 [PubMed PMID: 34429606]
Zhang HN, Gao Q, Xie JJ, Ye J. Correlation between blepharospasm and psychological diseases: the anxiety, depression and sleep disorder study. International journal of ophthalmology. 2024:17(11):2007-2013. doi: 10.18240/ijo.2024.11.05. Epub 2024 Nov 18 [PubMed PMID: 39559314]