Introduction
Anemia is one of the most common chronic conditions worldwide and has significant morbidity. Circulating red blood cells (RBCs) contain the protein hemoglobin, which has 4 polypeptide chains and 1 heme ring containing iron in its reduced form.[1] Iron is the main component of hemoglobin and is the prime carrier of oxygen. Iron deficiency causes a profound global burden, affecting over 2 billion people worldwide. Iron deficiency is estimated to affect about 40% of the population in developing countries and 10% in developed countries, making it the most common cause of anemia worldwide. Iron is essential for multiple important biological functions. Additionally, it is necessary for the synthesis of hemoglobin and myoglobin, oxygen transport, hormone synthesis, cell regulation and proliferation, DNA synthesis, mitochondrial electron transport, and antioxidation.[2][3] Iron also plays a vital role in regulating both innate and adaptive immunity.[4]
The etiologies of chronic iron deficiency vary widely by demographics, including gender, age, geographic region, and diet. The primary cause of iron deficiency worldwide is a lack of enough iron-containing food. Other common causes include blood loss, gastrointestinal (GI) malabsorption, and genetic conditions. Quantifiable iron deficiency can result from inadequate intake, impaired absorption, or blood loss. Iron deficiency can be with or without anemia, both of which have clinical implications. Inflammatory states can also cause functional iron deficiency, in which iron stores are adequate but are sequestered by macrophages and unavailable for systemic use; this is referred to as anemia of chronic disease.
Less commonly, thalassemias and lead toxicity may cause hypochromic anemia. Both conditions result from decreased hemoglobin content and cause microcytic hypochromic anemia. Reticulocyte count, iron indices, serum electrophoresis, lead levels, microscopy, and DNA studies can help distinguish these etiologies from iron deficiency.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Because most of the body's iron is in RBCs, bleeding from any site can cause iron deficiency. Bleeding from the GI tract or menstruation is the most common cause of iron deficiency in developed countries, as a Western diet typically provides enough iron. Overt causes of bleeding, such as hematemesis, menorrhagia, multiple pregnancies, and childbirth, can easily be recognized based on history alone. Other causes, such as occult GI bleeding, malabsorption, and frequent blood donations, can be overlooked.[5][6]
Inadequate dietary intake is rare in developed nations. Dietary iron exists in 2 forms: heme iron, derived from animal sources and more efficiently absorbed, and nonheme iron, found in plant-based food. Most dietary iron is consumed in the nonheme form. Individuals from lower socioeconomic backgrounds, vegetarians or vegans, and older patients who do not eat a balanced diet are prone to developing iron deficiency. In toddlers, excessive milk or juice intake, prolonged bottle-feeding, and frequent snacking contribute to iron deficiency. A typical American diet contains about 10 to 20 mg of iron, of which only 1 to 2 mg is absorbed.[7][8] About 25 mg of iron per day is required for erythropoiesis, indicating that the majority of this requirement is supplied by macrophages in the spleen and liver, which recycle iron from senescent blood cells.[9]
GI sources of iron deficiency are common in developed countries. Etiologies of blood loss include inflammatory bowel disease, gastric or duodenal ulcers, gastroduodenal erosions, Mallory-Weiss tears, arteriovenous malformations, GI cancers, esophagitis, gastritis, varices, diverticuli, polyps, and hemorrhoids. GI bleeding can be classified into upper and lower sources and can be life-threatening. Gastroenterologists must be involved, and rarely, surgical involvement is necessary.[10][11][12][13] Please see StatPearls' companion resource, "Gastrointestinal Bleeding," for further information.
Malabsorption of iron can occur in celiac disease, atrophic gastritis, Helicobacter pylori infection, and bariatric surgery. Up to 14% of patients with inflammatory bowel disease and 46% of patients with celiac disease have iron deficiency anemia. Reduced iron absorption can also occur in association with dietary elements such as tannins, phosphates, phytates, oxalates, and calcium. Certain medications can interfere with iron absorption. Examples include gastric acid-suppressing drugs, antibiotics, levodopa, levothyroxine, and ibandronate.[14] In some low-resource countries, parasitic infections, including Stronglyloides, Schistosoma, and helminths, are significant contributors to iron deficiency.[15]
Iron deficiency also occurs in conditions such as chronic kidney disease (CKD), chronic heart failure, inflammatory bowel disease, certain malignancies, and rheumatoid arthritis. Please see StatPearls' companion resources, "Anemia" and "Anemia of Chronic Kidney Disease," for further reference.
Genetic Conditions
Genetic disorders affecting iron metabolism can also cause iron deficiency; these conditions can be part of a syndrome or single-gene abnormalities. Syndromes associated with chronic iron deficiency include ATR-X syndrome.[16] SLC11A2 mutations and iron-refractory iron deficiency anemia due to TMPRSS6 mutations are rare inherited conditions characterized by elevated hepcidin levels and iron deficiency. These conditions often do not respond to oral iron supplements and require intravenous (IV) iron.[17][18][19] Mutations in any of the enzymes involved in iron metabolism, such as divalent metal transporter 1 (DMT1), transferrin, and ceruloplasmin, can also cause iron deficiency.[20] Hereditary sideroblastic anemias are caused by various genetic defects, resulting in a functional lack of iron with high or normal iron reserves. Please see StatPearls' companion resource, "Sideroblastic Anemia," for further information.[18]
Iron Deficiency in Pregnancy
Pregnant patients require 500 to 1100 mg of additional iron during their pregnancy. These patients experience dilutional anemia from increased intravascular volume, and a normal hemoglobin level in a pregnant patient is less than 11 g/dL in the first trimester and less than 10 g/dL in the second and third trimesters. Erythrocyte mass should increase by about 25% to accommodate the increased volume (mediated by increased erythropoietin); inadequate iron stores can impair this response.
Iron deficiency is the most common cause of anemia during pregnancy, occurring in up to 26% of pregnant patients, depending on the parameters measured. Iron deficiency is associated with increased adverse events and poorer perinatal and neonatal outcomes. A large study found increased rates of autism spectrum disorder, attention deficit hyperactivity syndrome, and intellectual disability in patients whose mother had anemia before 30 weeks of gestation. Other possible associations include severe maternal morbidity, postpartum hemorrhage, preeclampsia, placenta previa, and need for hospital admission.[6][21]
Thalassemias
Thalassemias are caused by genetic defects in globin chain synthesis, which disrupt normal hemoglobin production. Deficient alpha- or beta-globin synthesis results in an excess of the corresponding globin chain, which precipitates in erythroid precursors, leading to apoptosis and ineffective erythropoiesis.[22] Chronic anemia and hypoxia stimulate marrow hyperplasia and extramedullary hematopoiesis. Iron overload occurs from both increased absorption (due to suppressed hepcidin via erythroid signals such as erythroferrone) and repeated transfusions.[23] In addition, thalassemias damage red cell precursors and shorten RBC lifespan.[24]
The combination of defective globin synthesis, ineffective erythropoiesis, peripheral hemolysis, and iron overload distinguishes thalassemia pathophysiologically from pure iron deficiency, but mild thalassemia trait may present with mild microcytosis and normal iron parameters.[24][25][26] Please see StatPearls' companion resources, "Alpha Thalassemia" and "Beta Thalassemia."
Lead Poisoning
Chronic lead poisoning, though less common, can cause microcytic anemia, particularly in children and individuals in developing countries. Common sources of exposure include environmental lead, such as paint in older homes and contaminated water; occupational exposure; and ingestion of lead-containing herbs. Signs of lead poisoning include weakness, abdominal pain, and neurologic symptoms. Chronic lead poisoning can also cause microcytic anemia by interfering with enzymes involved in hemoglobin production, such as erythrocyte pyrimidine-specific 5'-nucleotidase and erythrocyte nucleotidase, resulting in microcytic hypochromic anemia and hemolytic anemia. Basophilic stippling in erythrocytes on Wright stain, caused by RNA clumping, is considered pathognomonic for chronic lead poisoning. Please see StatPearls' companion resource, "Lead Toxicity," for further information.[27][28][29]
Epidemiology
According to the Global Burden of Disease Study 2021, the disease-adjusted life years for iron deficiency increased between 1990 and 2021, with the highest burden observed in low socioeconomic areas.[30] According to the National Health and Nutrition Examination Survey, approximately 14% of adults in the United States have iron deficiency anemia.[6] The prevalence of iron deficiency among nonpregnant adults in the United States varies by the ferritin threshold. This prevalence is estimated at 5.9 million using a threshold of 15 ng/mL, but increases by 3.3 million when the threshold is changed to 45 ng/mL.[31]
In the United States, iron deficiency is observed in 9% of children aged 1 to 2. Compared to White children, Hispanic children are twice as likely to have an iron deficiency. The prevalence in adolescent girls and women in the reproductive age group is between 9% and 11%. Iron deficiency is most common in multiparous women from low-income minority populations. In males, it is observed in around 1% of the population, with a slightly higher prevalence of 2% to 4% in middle-aged and older men.[7][32] A positive correlation has also been observed between obesity and the risk of developing iron deficiency, likely due to increased hepcidin production by adipocytes.[6][15]
Alpha thalassemia traits are believed to be protective against malaria; in regions with high malaria incidence, the trait can be found in up to 90% of the population. Hemoglobin H disease is similar and found mostly in warm climates. The regions with the highest incidence are Southeast Asia, the Mediterranean, and the Middle East. Hemoglobin Constant Spring is the most common form of non-deletion alpha thalassemia. About 1% to 2% of individuals living in northeastern Thailand, 5% to 8% of those in southern China, and one-quarter of women in an ethnic minority population in Vietnam have Hemoglobin Constant Spring.[33][34]
The prevalence of beta thalassemia also parallels that of malaria as a proposed survival advantage for carriers of these genes. Gene drift and founder effects are other reasons why thalassemia is more frequent in certain areas.[35] The frequency of beta-thalassemia mutations varies across regions of the world, with the highest prevalence in the Mediterranean, the Middle East, and Southeast and Central Asia. Over 60,000 children are born with beta-thalassemia yearly; however, the true number is likely higher, given that many are born in countries with minimal health care. The prevalence of beta-thalassemia is estimated at 80 to 90 million carriers, representing approximately 1.5% of the global population.[36][37] In Cyprus, the reported carrier prevalence among Greek and Turkish populations is as high as 15%.[38]
Pathophysiology
Iron homeostasis is maintained by balancing absorption and iron losses. Dietary iron comes in 2 forms: heme iron, which is reduced (Fe2+) and is directly absorbed, and nonheme iron (Fe3+), which must be reduced before absorption. Absorption of both types occurs primarily in the proximal intestine, but through different receptors. Heme iron is absorbed through the heme carrier-1 protein, which is responsive to hypoxia.[9][39] The absorption of nonheme iron is more complex. The first nonheme iron is reduced in the duodenum by reductases such as cytochrome B (DCYTB). Nonheme iron is absorbed by enterocytes in the brush border as the divalent form via DMT1. Iron is then transported to the bloodstream by ferroportin-1 on the basolateral enterocytes. Ferroportin-1 works with the ferroxidase hephaestin, which oxidizes ferrous iron to facilitate its binding to transferrin. Hepcidin is an inhibitory protein synthesized by the liver that downregulates ferroportin and decreases iron absorption. Hepcidin levels are often increased in chronic disease and inflammatory states.[8][17][40][41]
Once absorbed, iron is sequestered in ferritin if body stores are adequate. Ferritin is a primarily intracellular protein—with small amounts circulating in the blood—located in the bone marrow, spleen, and liver, which is responsible for the storage and release of iron. Ferritin is also an acute-phase reactant, and its levels may be elevated in chronic disease, inflammatory states, and malignancy.[6][9][42] Iron is released through ferritin degradation, after which free iron is oxidized by ferroxidases such as ceruloplasmin. Iron then binds to the transferrin receptor and is transported to cells for metabolism.[9][41] Transferrin is also involved in iron recycling by transporting iron from reticuloendothelial cells and the liver to proliferating cells throughout the body. Transferrin is synthesized in the liver and, unlike ferritin, it is involved exclusively in iron metabolism. Transferrin synthesis is regulated by hypoxia and iron levels. Low iron levels upregulate iron-regulatory proteins 1 and 2, thereby optimizing cellular iron availability by increasing the expression of multiple genes.[43] Hypoxia induces hypoxia-inducible factor α and β, which increase transferrin expression.[9]
Iron deficiency occurs in 3 stages. In the prelatent stage, iron stores are low or absent, but serum iron concentration is normal. In the latent stage, transferrin saturation and serum iron are reduced, along with low ferritin. The last stage is marked by a drop in hemoglobin, depletion of iron stores, and reductions in serum iron and transferrin saturation.[44][45][44] Because hemoglobin levels decline only in the late stage, they are an insensitive marker of early iron deficiency and do not reliably reflect iron stores.[46]
Histopathology
On peripheral smear, hypochromia is evident as an enlarged central zone of pallor (>1/3 of the RBC diameter) and a thin hemoglobinized rim. Microcytosis is reflected by a reduced mean corpuscular volume (<80 fL in adults with iron deficiency). In iron deficiency anemia, anisopoikilocytosis is common; pencil cells (elongated elliptocytes) and target cells may be present, with elevated red cell distribution width supporting heterogeneous cell sizes. In iron deficiency anemia, bone marrow shows reduced to absent stainable iron on Perls (Prussian blue) staining of aspirate particles or macrophages; in severe deficiency, iron may be completely absent. These marrow iron assessments remain the gold standard for documenting depleted iron stores. However, they are invasive and are now often supplanted by ferritin-first algorithms (see Images Iron Deficiency Anemia and Normal Versus Iron Deficiency Anemia).[47][48]
In thalassemias, peripheral smear also shows microcytosis and hypochromia, but typically with more uniform microcytosis (often normal red cell distribution width), numerous target cells, and sometimes basophilic stippling; overall RBC count is often normal or high relative to the degree of anemia. Alpha thalassemia (hemoglobin H disease) features hemoglobin H inclusion bodies (β4 tetramers) detectable on brilliant cresyl blue (supravital) staining.[49] Beta-thalassemia shows marrow erythroid hyperplasia with ineffective erythropoiesis—expansion of early erythroid precursors with apoptosis of late forms—driven by globin chain imbalance (excess unpaired alpha-chains), oxidative stress, and downstream hepcidin suppression; chronic cases develop extramedullary hematopoiesis and iron overload from increased absorption or transfusion.[50] Marrow iron stores in thalassemia are normal to increased, unless coexisting iron deficiency is present.[51] Ring sideroblasts are not a feature of thalassemia per se; they indicate sideroblastic processes or myelodysplastic syndromes. However, Perls staining is routinely used in marrow evaluation to document iron distribution and, when indicated, exclude sideroblastic change.[52]
Lead poisoning also causes microcytic, hypochromic anemia. Hematologically, lead causes anemia by interfering with the function of several enzymes involved in heme synthesis and in maintaining erythrocyte membrane integrity, such as δ-aminolevulinic acid dehydratase, leading to decreased erythrocyte production and increased erythrocyte destruction.[53] Lead toxicity can also cause bone marrow suppression by inhibiting Wnt3a/β-catenin signaling.[54] The classic appearance of basophilic stippling is thought to represent clumps of degraded RNA, which is normally cleared by the enzyme pyrimidine-5’-nucleotidase, which is inhibited by lead.[55] Basophilic stippling can be observed in disordered erythropoiesis and erythrocyte maturation. Basophilic stippling is considered a pathognomonic finding in lead poisoning in conjunction with hypochromic microcytic anemia—though normocytic anemia may occur—and deposition of lead in the gingiva and joints.[56][57] Occasionally, circulating nucleated RBCs and mild poikilocytosis may be noted (see Image. Basophilic Stippling).[58]
History and Physical
Patients with iron deficiency can exhibit symptoms both in the presence and absence of anemia. The symptoms of iron deficiency without anemia are similar to those with anemia, but less severe. The majority of symptoms are nonspecific and can include, but are not limited to, generalized weakness, fatigue, poor concentration, mood changes, irritability, headaches, shortness of breath on exertion, dry mouth, hair loss, dysphagia, brittle fingernails, restless leg syndrome, and decreased exercise capacity. These symptoms are attributable to low oxygen delivery to tissues and reduced activity of iron-containing enzymes. Pallor is typically a late sign of iron deficiency anemia. Restless leg syndrome is associated with decreased brain iron on magnetic resonance imaging, and up to 40% of patients with this condition may have iron deficiency, with or without anemia.[6]
Pica, a symptom of craving and consumption of non-nutritious and non-food substances, occurs in approximately half of patients with absolute iron deficiency. Pagophagia (craving for ice) is quite specific to iron deficiency.[6][59] Patients may have a history of dry mouth, hair loss, dysphagia, brittle fingernails, and restless leg syndrome.
The physical examination can be normal or may reveal dry skin, hair loss, atrophic glossitis, cheilosis, pallor, brittle nails, and koilonychia (spoon-shaped nails). Cardiac auscultation may reveal a systolic flow murmur. Pallor and pale conjunctivae are later signs of iron deficiency anemia (see Images Atrophic Glossitis: Atrophy of Filiform Taste Bud and Iron Deficiency: Spoon-Shaped Nail).[6][60]
Beeturia is a finding that is not specific to iron deficiency but is more common in individuals with iron deficiency. This condition results from a change in GI function caused by severe iron deficiency and is characterized by red discoloration of the urine after eating beets.[61] Please see StatPearls' companion resource, "Beeturia," "Alpha Thalassemia," "Beta Thalassemia," and "Lead Poisoning," for further information.
Evaluation
Evaluation for Iron Deficiency
The diagnosis of iron deficiency is based mainly on history, examination, and laboratory tests. In uncomplicated cases, serum iron, transferrin, serum ferritin, total iron-binding capacity, and transferrin saturation should be used for evaluation. Serum iron levels vary throughout the day and are influenced by diet. Iron indices should not be measured within 9 hours of consuming iron-containing foods.[6][44] Absolute iron deficiency is diagnosed when serum ferritin is less than 30 ng/mL or transferrin saturation is less than 20%. A ferritin level less than 30 ng/mL is 92% sensitive and 98% specific for absent bone marrow stores of iron. Transferrin saturation is calculated as (iron/total iron-binding capacity) × 100.[6][62][63] Healthy individuals generally have transferrin saturations of 25% to 35%. Hemoglobin does not drop until a significant percentage of body iron is depleted. Hence, normal hemoglobin does not exclude iron deficiency. Microcytosis is also not considered a sensitive indicator of iron deficiency.[6][46]
Other iron studies available for evaluating iron deficiency include the following.
- Soluble transferrin receptor and soluble transferrin receptor-ferritin index: Soluble transferrin receptor is elevated in iron deficiency because of the upregulation of transferrin receptors. Measurement of soluble transferrin receptor can help differentiate between absolute (increased soluble transferrin receptor) and functional iron deficiency (normal soluble transferrin receptor).[41][63][64]
- Zinc protoporphyrin/heme ratio: Decreased iron supply for the formation of hemoglobin leads to increased utilization of zinc and an increase in the zinc protoporphyrin/heme ratio; this test is preferable to the invasive bone marrow aspiration.[64]
- Reticulocyte hemoglobin content: This parameter provides an estimate of iron availability for RBC production over a few days before the test. Thus, it is a useful indicator of early iron deficiency, and sequential measurements can also help to guide response to parenteral iron therapy. Reticulocytosis (>2.5% reticulocytes) after iron repletion also suggests iron deficiency. Inflammation does not influence this parameter and is useful in determining iron status in patients with CKD.[64][65]
Screening
The European Hematology Association recommends screening individuals at high risk for iron deficiency, including athletes, vegetarians, frequent blood donors, reproductive-aged women, adults older than 65, individuals with malabsorptive syndromes or bleeding disorders, socioeconomically disadvantaged populations, individuals with chronic parasitic infections, and those with chronic diseases. The International Federation of Gynecology and Obstetrics and the European Hematology Association recommend screening all pregnant and reproductive-aged women for iron deficiency. In contrast, the American College of Obstetricians and Gynecologists recommends screening only anemic patients for iron deficiency. The American Gastroenterology Association recommends screening all iron-deficient patients with upper GI symptoms, such as dyspepsia, epigastric pain, and nausea, for Helicobacter pylori infection and celiac disease. Some guidelines recommend screening all patients without a clear cause of iron deficiency with esophagogastroduodenoscopy and colonoscopy.[6]
Evaluation for Thalassemias
When iron studies are normal or increased, thalassemia syndromes should be suspected.
- Complete blood count patterns: Thalassemia often shows a normal or elevated RBC count despite anemia, markedly reduced mean corpuscular volume (<70 fL), and normal red cell distribution width (in contrast to iron deficiency anemia).
- Peripheral smear: Shows target cells, basophilic stippling, and uniform microcytosis.
- Hemoglobin electrophoresis or high-performance liquid chromatography:
- In beta-thalassemia trait, HbA2 is greater than 3.5%, and sometimes HbF elevation is diagnostic.
- In alpha-thalassemia, electrophoresis may be normal; DNA analysis for alpha-globin gene deletions is required for confirmation.
- Ancillary markers: Reticulocyte hemoglobin content or zinc protoporphyrin can differentiate iron deficiency from thalassemia.[22][23]
If both conditions coexist, iron studies and hemoglobin electrophoresis results should be interpreted together.
Evaluation for Lead
Evaluation is primarily based on measurement of blood lead levels. Basophilic stippling on microscopy, along with symptoms of lead poisoning or microcytic hypochromic anemia, is pathognomonic for lead toxicity.
Please see StatPearls' companion resources, "Alpha Thalassemia," "Beta Thalassemia," "Laboratory Evaluation of Alpha Thalassemia," "Evaluation of Beta Thalassemia," and "Lead Poisoning," for further information.
Treatment / Management
Iron Deficiency
Patients with uncomplicated iron deficiency without comorbidities should receive treatment with oral iron therapy. Oral iron is readily available, inexpensive, effective, safe, and convenient. Common ferric salts include ferrous sulfate (35 mg elemental iron), ferrous fumarate (100 mg elemental iron), and ferrous gluconate (35 mg elemental iron). These salts typically come in 325 mg tablets, of which only a small percentage (5%-20%) is absorbed.[6][41][66] Vitamin C (200-500 mg) is often recommended in combination with oral iron to enhance its absorption, as it reduces Fe3+ to Fe2+.[67] GI adverse effects often limit patient compliance. These adverse effects occur in up to 70% of patients taking oral iron, leading to treatment nonadherence. GI symptoms can be reduced with chelated iron.[62][64][68] Ferric complexes, including ferric polysaccharide, ferric polymaltose, and ferric polydextrose, are better tolerated than ferric salts. (B3)
Iron protein succinylate is comprised of iron bound to milk proteins; it is fairly well tolerated and highly effective, but is expensive. Ferric citrate is often used in patients with CKD or those undergoing dialysis because it also reduces phosphorus levels. Ferric maltol delivers iron to enterocytes while keeping the unabsorbed fraction chelated, therefore increasing tolerability in patients with irritable bowel disease. Sucrosomial iron and liposomal iron can be absorbed independently of DMT1 and may also be better tolerated than ferric salts in patients with irritable bowel disease. Carbonyl iron and heme iron polypeptides are also available as oral supplements, although data regarding their efficacy and safety remain limited.[66]
No meaningful clinical difference in hemoglobin has been found between daily and alternate-day oral iron dosing, but alternate-day dosing may improve tolerability and compliance. Enteric-coated and time-release formulations decrease iron absorption. The most robust response was observed with multiple daily doses, so therapy selection should be individualized based on the desired response and patient preference regarding adverse effects.[69] Treatment should continue until the ferritin, transferrin saturation, and hemoglobin are within normal ranges. Hemoglobin should increase by at least 1 g/dL within 2 to 4 weeks of starting oral iron. Expert guidelines recommend a 12-week course of oral iron/vitamin C supplementation in patients with restless leg syndrome who have transferrin saturation less than 45% or a ferritin level less than 75 ng/mL. In patients diagnosed with iron deficiency, hemoglobin should be monitored every 3 months for the first year, and then twice annually for the subsequent 2 years.[6][66](A1)
The recommended dietary allowance of iron for women of reproductive age is 18 mg/d, of which approximately 10% is absorbed. Notably, the average iron intake for women is 13 mg/d.[6] Red meat, liver, organ meats, sardines, and anchovies all contain high levels of bioavailable heme iron. However, most dietary iron comes from nonheme sources, including fortified grains and cereals, chickpeas, lentils, spinach, broccoli, and kale. As noted earlier, vitamin C and acidic environments facilitate iron absorption. Fiber, calcium, coffee, and tea decrease iron absorption. Please refer to the "Deterrence and Patient Education" section for more information on requirements by age/gender and dietary content of food.
Many patients cannot replete their iron stores with oral iron alone and require parenteral iron. This group includes patients with malabsorption, ongoing iron loss, irritable bowel syndrome, nonresponsiveness to oral iron, chronic disease, or those who are unable to tolerate oral supplementation. These patients should be treated with IV iron. IV iron is available in several forms, such as ferric carboxymaltose, ferric gluconate, ferric/iron sucrose, ferumoxytol, ferric derisomaltose, and low-molecular-weight iron dextran. No significant difference has been observed among the formulations; however, low-molecular-weight iron dextran, ferric carboxymaltose, ferric derisomaltose, and ferumoxytol allow single-infusion administration.[6][41]
There is a low risk of allergic reactions with all IV iron formulations. Anaphylaxis with IV iron is extremely rare, occurring with fewer than 1 in 200,000 administrations. High-molecular-weight dextran has been withdrawn due to a high frequency of serious anaphylactic reactions.[41] Complement activation–related pseudoallergy is the most common infusion reaction with IV iron. This reaction can occur at any time without prior sensitization and is not life-threatening. Most infusion reactions can be managed by stopping the infusion, hydration, and monitoring. Medications to consider if symptoms do not improve include IV steroids, 5-HT3 antagonists, and second-generation antihistamines.[70] Hypophosphatemia occurs with certain IV iron formulations and is observed within 2 weeks of administration. The highest incidence is observed with ferric carboxymaltose, and this agent should be avoided in patients prone to hypophosphatemia.[71](B3)
During pregnancy, oral iron supplementation is given in the first trimester, as the safety of IV iron in this period remains unestablished. According to the Centers for Disease Control and the American College of Obstetricians and Gynecologists, oral iron is given to all pregnant women who can tolerate it. One recommendation is to provide women with at least 27 mg of elemental iron during pregnancy and 9 mg during lactation. Exceptions include women with severe anemia, women with inflammatory bowel disease, and those who have undergone bariatric surgery. In these patients, IV iron is preferable. All IV forms have equal efficacy and safety except for some formulations of ferric gluconate, which utilize benzyl alcohol as a preservative and should be avoided because of the possibility of harm to the fetus.[72]
Testing should not be repeated within 4 weeks of IV Iron administration, as results can be misleading before then. Ferritin and transferrin saturation should be measured after 4 weeks, and iron supplementation should be given till both return to the normal range.[70] (B3)
Thalassemia Syndromes
Management of thalassemia requires a tailored approach based on transfusion dependence, iron overload, and ineffective erythropoiesis.
1. Transfusion support
-
Transfusion-dependent thalassemia requires regular packed RBC transfusions to maintain pretransfusion hemoglobin levels around 9 to 10.5 g/dL, suppressing marrow expansion and improving growth and organ function.[22]
2. Iron chelation Therapy
-
Chronic transfusion can cause secondary iron overload and warrant chelation when serum ferritin is greater than 1000 ng/mL or liver iron is greater than 3 mg/g dry weight.
-
Chelating agents include:
-
Deferoxamine (parenteral)—gold standard for decades
-
Deferiprone (oral)—effective for cardiac iron
-
Deferasirox (oral)—convenient once-daily dosing
-
-
Combination therapy (deferiprone + deferoxamine) offers superior cardiac protection.[73]
(B3)
3. Stem cell transplant
- Stem cell transplant (bone marrow transplant) is a potential option in selected cases, such as children born with severe thalassemia, potentially eliminating the need for lifelong blood transfusions.[74] (B2)
- However, this procedure has complications, and the clinician must weigh them against the benefits. Risks include graft-versus-host disease, chronic immunosuppressive therapy, graft failure, and transplantation-related mortality.[75]
4. Gene therapy
- Gene therapy is a recent advance in the management of severe thalassemia. The procedure involves harvesting the patient's autologous hematopoietic stem cells and genetically modifying them with vectors that express the normal genes. The cells are reinfused into patients after they have undergone the required conditioning to eliminate existing hematopoietic stem cells. The modified stem cells then produce normal hemoglobin chains, restoring effective erythropoiesis.
- Genome editing techniques: Another recent approach is the editing of genomic libraries using zinc-finger nucleases, transcription activator-like effectors, and clustered regularly interspaced short palindromic repeats (CRISPR) with the Cas9 nuclease system. These techniques target specific mutation sites and replace them with the normal sequence. The limitation of this technique is its inability to produce a sufficient number of corrected genes to cure the disease.[76]
5. Splenectomy
- Patients with thalassemia major often undergo splenectomy to limit the number of required transfusions. Splenectomy is the usual recommendation when the annual transfusion requirement exceeds 200 to 220 mL RBCs/kg/year, with a hematocrit of 70%.
- Splenectomy not only limits the number of required transfusions but also controls the spread of extramedullary hematopoiesis.
- Postsplenectomy immunizations are necessary to prevent bacterial infections, including Pneumococcus, Meningococcus, and Haemophilus influenzae. Postsplenectomy sepsis is possible in children, so this procedure is deferred until 6 to 7 years of age, and then penicillin is given for prophylaxis until they reach a certain age.
6. Cholecystectomy
- Patients may develop cholelithiasis due to increased hemoglobin (Hb) breakdown and bilirubin deposition in the gallbladder. If it becomes symptomatic, patients should undergo cholecystectomy at the same time as they undergo splenectomy.
7. Diet and exercise
- Reports indicate that drinking tea reduces iron absorption from the GI tract.
- Vitamin C helps in iron excretion from the gut, especially when used with deferoxamine. But using vitamin C in large quantities and without concomitant deferoxamine use, there is a higher risk for fatal arrhythmias. Therefore, the recommendation is to use low doses of vitamin C in combination with iron chelators (eg, deferoxamine).[76]
8. Emerging and adjunctive therapies
- Luspatercept, an erythroid maturation agent, reduces transfusion burden by improving late-stage erythropoiesis by decreasing transforming growth factor-beta activity. Luspatercept is Food and Drug Administration-approved for the treatment of anemia in patients with ß-thalassemia.[73] (B3)
- Gene-editing therapies, such as CRISPR-Cas9–mediated correction of the beta-globin gene, are under evaluation to normalize erythropoiesis and minimize iron loading.[77]
Lead Toxicity
- Pediatric screening guidelines for lead vary by state because the prevalence of lead toxicity tends to be higher in older urban areas. However, the Early Periodic Screening, Diagnosis, and Treatment (EPSDT) component of Medicaid requires that all children enrolled in Medicaid receive screening at 12 and 24 months. Children aged 3 to 5 who have not previously been screened are also required to undergo testing.[78] (A1)
- The Occupational Safety and Health Administration requires employers to implement medical surveillance, including lead screening, for any employee who may be exposed to airborne lead at concentrations exceeding 30 mg/min averaged over 8 hours for more than 30 days/year.[79] Screening is typically performed using capillary blood due to its convenience and speed; however, any elevated capillary result (over 5 mcg/dL) should be confirmed with a venous whole blood sample. (B3)
- In patients with confirmed elevated whole blood venous lead levels, additional laboratory tests to assess iron status and anemia are recommended.
- An abdominal x-ray should be considered if the patient may have ingested a lead-containing foreign body, such as paint chips, a bullet, or a fishing weight.
- As with all patients in whom the toxin-mediated disease is suspected, the evaluation should include a detailed history and a thorough physical examination.
Differential Diagnosis
The differential diagnosis for iron deficiency without anemia is broad, as most symptoms are nonspecific and overlap with many other conditions. Potential causes include fatigue-related disorders such as fibromyalgia, chronic fatigue syndrome, depression or mood disorders, chronic medical conditions, and hypothyroidism. Other considerations include causes of pica, eating disorders, psychiatric conditions, malnutrition, causes of restless legs syndrome-like neurological conditions, and pregnancy. Causes of microcytosis in the absence of iron deficiency anemia include thalassemia; sideroblastic anemia; lead poisoning; copper deficiency; certain medications, such as isoniazid; and chloramphenicol.
Complications
Complications of iron deficiency and microcytic hypochromic anemia include the following:
- If untreated, iron deficiency is associated with significant cognitive impairment and poor quality of life.
- During pregnancy, untreated iron deficiency can affect fetal brain maturation, lead to low birth weight, and predispose the baby to iron deficiency. Maternal adverse outcomes include depression, increased risk of sepsis, and maternal mortality.[81][82]
- In patients undergoing cardiac or abdominal surgery, preoperative iron deficiency correlates with poor outcomes.[62]
- In patients with heart failure, chronic iron deficiency shows an association with an increase in mortality.
- Initially, iron repletion can transiently increase the risk of malaria or other infections in children in endemic areas.[66]
- If malignancy is the underlying cause of GI, uterine, or urinary bleeding, a diagnosis delay can lead to advanced disease and higher morbidity and mortality.
Deterrence and Patient Education
Patients should receive counselling from dieticians on consuming iron-rich foods, such as fruits and vegetables high in vitamin C. Heme iron can be found in animal sources, such as organ meats (especially liver), oysters, and anchovies. In babies born to iron-deficient mothers, delayed umbilical cord clamping can help prevent neonatal iron deficiency.[82]
Dietary Recommendations
In infants, iron should be supplemented by iron-fortified cereal and formula after 6 months of breastfeeding. Anti-helminthic drugs should be given to children with parasitic infections. In areas with high iron deficiency prevalence, women of reproductive age should take daily iron supplements.[41][81]
The heme iron in meats, fish, and poultry, called the MFP factor, significantly increases iron absorption from nonheme sources such as fruits, vegetables, and grains when consumed together. A study demonstrated that adding chicken, beef, or fish to a meal increased nonheme iron absorption 2- to 3-fold, whereas adding an equivalent amount of protein in the form of egg albumin did not produce the same effect.[83][84] The precise underlying mechanism is unclear, but evidence suggests that cysteine-containing peptides in animal products help form luminal carriers that promote iron transport.[85] Vitamin C enhances the absorption of nonheme iron by chelating and reducing ferric iron to ferrous, which is more soluble.[86][87] Vitamin C also counteracts inhibitors of iron absorption, including phytates in grains and legumes, polyphenols in tea, coffee, and red wine, and calcium in dairy products.[88] This physiologic effect supports the recommendation to take iron supplements with vitamin C–containing foods or juices rather than milk (see Table. Iron Recommendations).
Notably, cooking food in iron cookware, such as pots or skillets, can significantly increase the iron content of foods. Studies have shown that iron content and absorption are 1.5 to 3.3 times higher when meats, vegetables, and legumes are cooked in iron pots, resulting in higher hemoglobin levels than when cooked in non-iron vessels. This approach may be particularly effective for improving iron status in individuals in developing countries or those consuming low-iron diets.[89]
Enhancing Healthcare Team Outcomes
Chronic iron deficiency is a significant global health problem and is often overlooked because its presentation is frequently vague and nonspecific. In developing countries, inadequate dietary intake is the leading cause of chronic iron deficiency, whereas GI bleeding or menstruation is the leading cause in developed nations. The causes of iron deficiency can include a variety of gynecological, obstetrical, metabolic, and GI etiologies. The physical examination is often normal, and the cause cannot be determined without lab investigations.
Management requires a multidisciplinary approach. A primary care provider should always be involved in the patient's care, with referral to a hematologist, obstetrician/gynecologist, or gastroenterologist as indicated. A dietitian can play an essential role in the primary prevention of iron deficiency through dietary adjustments. Laboratory technologists play a vital role in diagnosing chronic iron deficiency. Social workers can help patients with food insecurity. Pharmacists can help determine the appropriate oral or intravenous iron formulation that best meets the patient's needs. Nurses not only educate the patients but also assist in treatment administration. Effective collaboration and communication among healthcare professionals can help ensure optimal outcomes for all patients.
A strategic approach is equally crucial, involving evidence-based strategies to optimize treatment plans and minimize adverse effects. Ethical considerations must guide decision-making, ensuring informed consent and respecting patient autonomy in treatment choices. Each healthcare professional must be aware of their responsibilities and contribute their unique expertise to the patient's care plan, fostering a multidisciplinary approach. Effective interprofessional communication is paramount, allowing seamless information exchange and collaborative decision-making among the team members. Care coordination plays a pivotal role in ensuring that the patient's journey from diagnosis to treatment and follow-up is well-managed, minimizing errors and enhancing patient safety. By embracing these principles of skill, strategy, ethics, responsibilities, interprofessional communication, and care coordination, healthcare professionals can deliver patient-centered care, ultimately improving patient outcomes and enhancing team performance in the management of iron deficiency and microcytic hypochromic anemia.
Media
(Click Image to Enlarge)
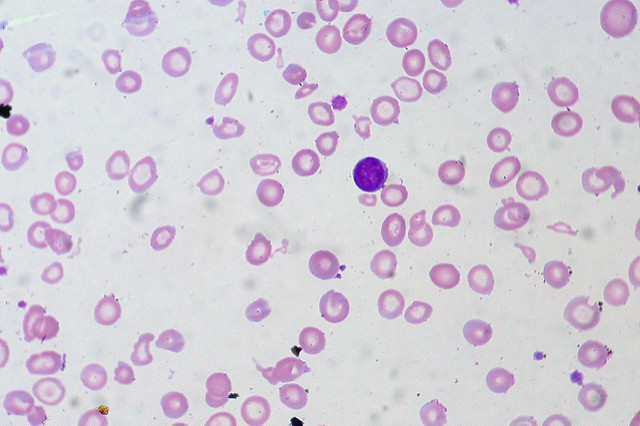
Iron Deficiency Anemia. Peripheral smear demonstrates microcytic, hypochromic red blood cells with an enlarged central zone of pallor (>1/3 of the RBC diameter) and a thin hemoglobinized rim. Anisopoikilocytosis with occasional pencil cells and target cells may be present, reflecting heterogeneous cell size.
Ed Uthman, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
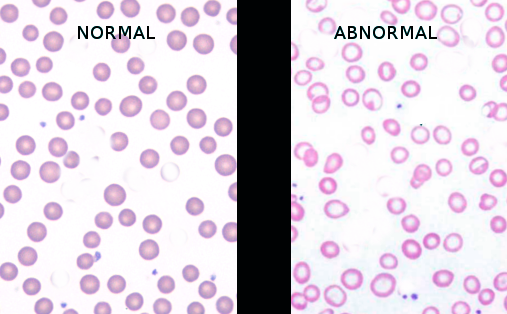
Normal Versus Iron Deficiency Anemia. The image shows a comparison of normal red blood cells and microcytic, hypochromic red blood cells in iron deficiency anemia, characterized by increased central pallor and variability in size and shape.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
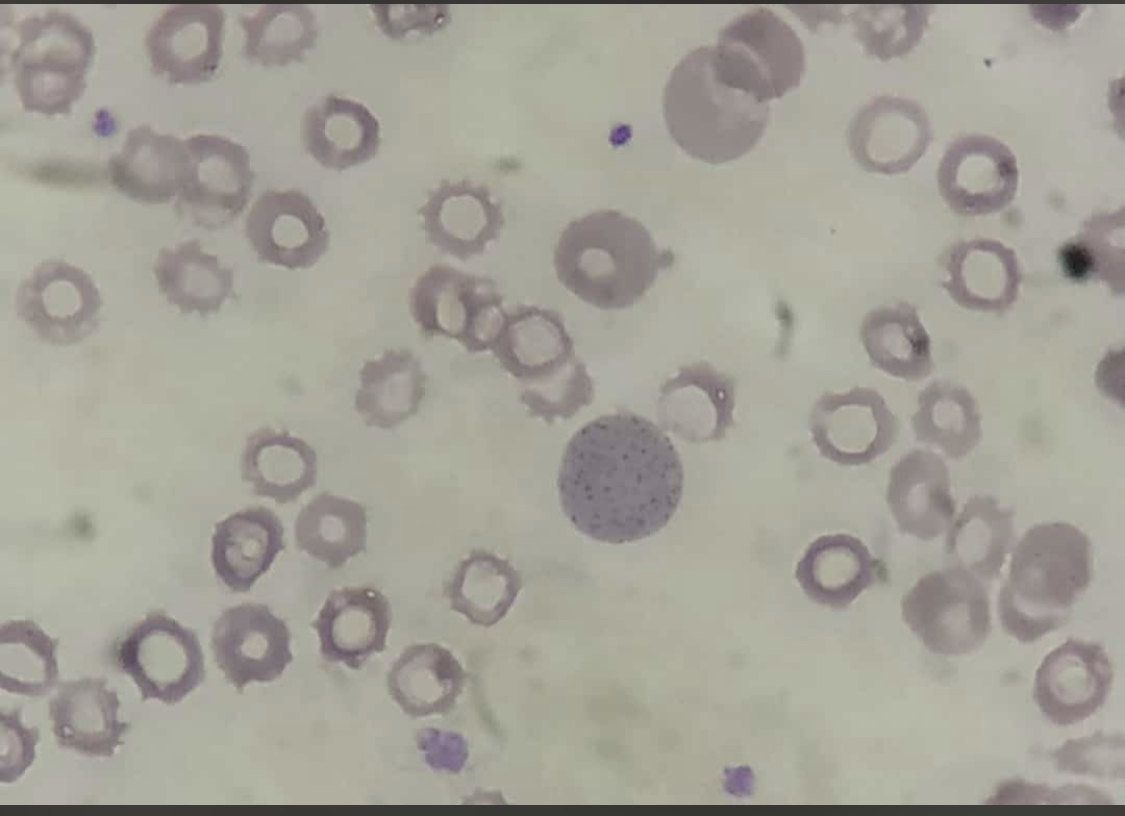
Basophilic Stippling. Red blood cells show coarse, punctate granules dispersed within the cytoplasm, representing abnormal RNA remnants. This finding is commonly associated with lead poisoning, thalassemia, and other disorders of erythropoiesis.
Contributed by AI Khan, MD
(Click Image to Enlarge)

Atrophic Glossitis: Atrophy of Filiform Taste Bud. The image shows atrophy of the fungiform and filiform papillae, thought to be due to vitamin B or iron deficiency.
Centers for Disease Control and Prevention
(Click Image to Enlarge)

Iron Deficiency: Spoon-Shaped Nail. The image shows a fingernail with a spoon-like appearance (koilonychia), where the nail curves upward and away from the nail bed. This classic finding is associated with iron deficiency anemia.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
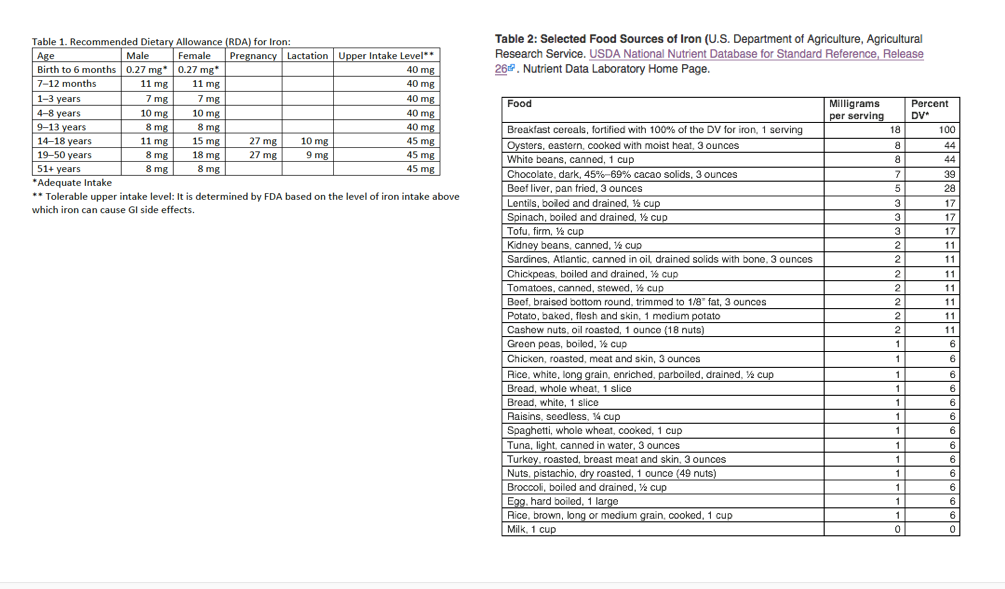
Iron Recommendations: recommended dietary requirement of iron. Iron content in different food sources described by American department of Agriculture.
Contributed by Dr. Fady Moustarah, MD
References
Rampon K. Anemia: Microcytic Anemia. FP essentials. 2023 Jul:530():12-16 [PubMed PMID: 37390396]
Rusu IG, Suharoschi R, Vodnar DC, Pop CR, Socaci SA, Vulturar R, Istrati M, Moroșan I, Fărcaș AC, Kerezsi AD, Mureșan CI, Pop OL. Iron Supplementation Influence on the Gut Microbiota and Probiotic Intake Effect in Iron Deficiency-A Literature-Based Review. Nutrients. 2020 Jul 4:12(7):. doi: 10.3390/nu12071993. Epub 2020 Jul 4 [PubMed PMID: 32635533]
Philip KEJ, Sadaka AS, Polkey MI, Hopkinson NS, Steptoe A, Fancourt D. The prevalence and associated mortality of non-anaemic iron deficiency in older adults: a 14 years observational cohort study. British journal of haematology. 2020 May:189(3):566-572. doi: 10.1111/bjh.16409. Epub 2020 Feb 18 [PubMed PMID: 32072619]
Ni S, Yuan Y, Kuang Y, Li X. Iron Metabolism and Immune Regulation. Frontiers in immunology. 2022:13():816282. doi: 10.3389/fimmu.2022.816282. Epub 2022 Mar 23 [PubMed PMID: 35401569]
Cançado RD, Chiattone CS, Alonso FF, Langhi Júnior DM, Alves Rde C. Iron deficiency in blood donors. Sao Paulo medical journal = Revista paulista de medicina. 2001 Jul 5:119(4):132-4; discussion 131 [PubMed PMID: 11500785]
Auerbach M, DeLoughery TG, Tirnauer JS. Iron Deficiency in Adults: A Review. JAMA. 2025 May 27:333(20):1813-1823. doi: 10.1001/jama.2025.0452. Epub [PubMed PMID: 40159291]
Brotanek JM, Gosz J, Weitzman M, Flores G. Iron deficiency in early childhood in the United States: risk factors and racial/ethnic disparities. Pediatrics. 2007 Sep:120(3):568-75 [PubMed PMID: 17766530]
Talarico V, Giancotti L, Mazza GA, Miniero R, Bertini M. Iron Deficiency Anemia in Celiac Disease. Nutrients. 2021 May 17:13(5):. doi: 10.3390/nu13051695. Epub 2021 May 17 [PubMed PMID: 34067622]
MacKenzie EL, Iwasaki K, Tsuji Y. Intracellular iron transport and storage: from molecular mechanisms to health implications. Antioxidants & redox signaling. 2008 Jun:10(6):997-1030. doi: 10.1089/ars.2007.1893. Epub [PubMed PMID: 18327971]
Kate V, Sureshkumar S, Gurushankari B, Kalayarasan R. Acute Upper Non-variceal and Lower Gastrointestinal Bleeding. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract. 2022 Apr:26(4):932-949. doi: 10.1007/s11605-022-05258-4. Epub 2022 Jan 26 [PubMed PMID: 35083723]
Samuel R, Bilal M, Tayyem O, Guturu P. Evaluation and management of Non-variceal upper gastrointestinal bleeding. Disease-a-month : DM. 2018 Jul:64(7):333-343. doi: 10.1016/j.disamonth.2018.02.003. Epub 2018 Mar 7 [PubMed PMID: 29525375]
Nelms DW, Pelaez CA. The Acute Upper Gastrointestinal Bleed. The Surgical clinics of North America. 2018 Oct:98(5):1047-1057. doi: 10.1016/j.suc.2018.05.004. Epub 2018 Jul 29 [PubMed PMID: 30243446]
Strate LL, Ayanian JZ, Kotler G, Syngal S. Risk factors for mortality in lower intestinal bleeding. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2008 Sep:6(9):1004-10; quiz 955-. doi: 10.1016/j.cgh.2008.03.021. Epub 2008 Jun 16 [PubMed PMID: 18558513]
Level 2 (mid-level) evidenceMuñoz M, García-Erce JA, Remacha ÁF. Disorders of iron metabolism. Part II: iron deficiency and iron overload. Journal of clinical pathology. 2011 Apr:64(4):287-96. doi: 10.1136/jcp.2010.086991. Epub 2010 Dec 20 [PubMed PMID: 21177268]
Zhao L, Zhang X, Shen Y, Fang X, Wang Y, Wang F. Obesity and iron deficiency: a quantitative meta-analysis. Obesity reviews : an official journal of the International Association for the Study of Obesity. 2015 Dec:16(12):1081-93. doi: 10.1111/obr.12323. Epub 2015 Sep 23 [PubMed PMID: 26395622]
Level 1 (high-level) evidenceLeón NY, Harley VR. ATR-X syndrome: genetics, clinical spectrum, and management. Human genetics. 2021 Dec:140(12):1625-1634. doi: 10.1007/s00439-021-02361-5. Epub 2021 Sep 15 [PubMed PMID: 34524523]
Pagani A, Nai A, Silvestri L, Camaschella C. Hepcidin and Anemia: A Tight Relationship. Frontiers in physiology. 2019:10():1294. doi: 10.3389/fphys.2019.01294. Epub 2019 Oct 9 [PubMed PMID: 31649559]
Gunshin H, Fujiwara Y, Custodio AO, Direnzo C, Robine S, Andrews NC. Slc11a2 is required for intestinal iron absorption and erythropoiesis but dispensable in placenta and liver. The Journal of clinical investigation. 2005 May:115(5):1258-66 [PubMed PMID: 15849611]
Hoving V, Donker AE, Schols SEM, Swinkels DW. How I treat iron-refractory iron deficiency anaemia-An expert opinion-based treatment guidance for children and adults. British journal of haematology. 2025 Apr:206(4):1067-1076. doi: 10.1111/bjh.20030. Epub 2025 Feb 22 [PubMed PMID: 39985323]
Level 3 (low-level) evidenceBrissot P, Bernard DG, Brissot E, Loréal O, Troadec MB. Rare anemias due to genetic iron metabolism defects. Mutation research. Reviews in mutation research. 2018 Jul-Sep:777():52-63. doi: 10.1016/j.mrrev.2018.06.003. Epub 2018 Jun 22 [PubMed PMID: 30115430]
Means RT. Iron Deficiency and Iron Deficiency Anemia: Implications and Impact in Pregnancy, Fetal Development, and Early Childhood Parameters. Nutrients. 2020 Feb 11:12(2):. doi: 10.3390/nu12020447. Epub 2020 Feb 11 [PubMed PMID: 32053933]
Kattamis A, Kwiatkowski JL, Aydinok Y. Thalassaemia. Lancet (London, England). 2022 Jun 18:399(10343):2310-2324. doi: 10.1016/S0140-6736(22)00536-0. Epub 2022 Jun 9 [PubMed PMID: 35691301]
Pinto VM, Forni GL. Management of Iron Overload in Beta-Thalassemia Patients: Clinical Practice Update Based on Case Series. International journal of molecular sciences. 2020 Nov 20:21(22):. doi: 10.3390/ijms21228771. Epub 2020 Nov 20 [PubMed PMID: 33233561]
Level 2 (mid-level) evidenceBajwa H, Basit H. Thalassemia. StatPearls. 2026 Jan:(): [PubMed PMID: 31424735]
Correnti M, Gammella E, Cairo G, Recalcati S. Iron Absorption: Molecular and Pathophysiological Aspects. Metabolites. 2024 Apr 17:14(4):. doi: 10.3390/metabo14040228. Epub 2024 Apr 17 [PubMed PMID: 38668356]
Camaschella C, Nai A, Silvestri L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica. 2020:105(2):260-272. doi: 10.3324/haematol.2019.232124. Epub 2020 Jan 31 [PubMed PMID: 31949017]
Janus J, Moerschel SK. Evaluation of anemia in children. American family physician. 2010 Jun 15:81(12):1462-71 [PubMed PMID: 20540485]
Halmo L, Nappe TM. Lead Toxicity. StatPearls. 2026 Jan:(): [PubMed PMID: 31082141]
Valentine WN, Paglia DE, Fink K, Madokoro G. Lead poisoning: association with hemolytic anemia, basophilic stippling, erythrocyte pyrimidine 5'-nucleotidase deficiency, and intraerythrocytic accumulation of pyrimidines. The Journal of clinical investigation. 1976 Oct:58(4):926-32 [PubMed PMID: 965496]
Level 3 (low-level) evidenceHuang S, Li H, Zhang L, Chen H, Gao C. Global Burden of Diseases Associated With Iron Deficiency: GBD 2021. International journal for vitamin and nutrition research. Internationale Zeitschrift fur Vitamin- und Ernahrungsforschung. Journal international de vitaminologie et de nutrition. 2025 May 14:95(3):31351. doi: 10.31083/IJVNR31351. Epub [PubMed PMID: 40613395]
Al Ta'ani O, Mayrer BM, Luche NM, Siddique SM, Peslak SA, Anderson TS, Vajravelu RK. Diagnostic Serum Ferritin Thresholds and Prevalence of Iron Deficiency Anemia. JAMA internal medicine. 2025 Oct 1:185(10):1284-1285. doi: 10.1001/jamainternmed.2025.2311. Epub [PubMed PMID: 40853683]
Looker AC, Dallman PR, Carroll MD, Gunter EW, Johnson CL. Prevalence of iron deficiency in the United States. JAMA. 1997 Mar 26:277(12):973-6 [PubMed PMID: 9091669]
Byrd KA, Williams TN, Lin A, Pickering AJ, Arnold BF, Arnold CD, Kiprotich M, Dentz HN, Njenga SM, Rao G, Colford JM Jr, Null C, Stewart CP. Sickle Cell and α+-Thalassemia Traits Influence the Association between Ferritin and Hepcidin in Rural Kenyan Children Aged 14-26 Months. The Journal of nutrition. 2018 Dec 1:148(12):1903-1910. doi: 10.1093/jn/nxy229. Epub [PubMed PMID: 30517728]
Zhao P, Wu H, Weng R. Molecular analysis of hemoglobinopathies in a large ethnic Hakka population in southern China. Medicine. 2018 Nov:97(45):e13034. doi: 10.1097/MD.0000000000013034. Epub [PubMed PMID: 30407298]
Weatherall DJ, Williams TN, Allen SJ, O'Donnell A. The population genetics and dynamics of the thalassemias. Hematology/oncology clinics of North America. 2010 Dec:24(6):1021-31. doi: 10.1016/j.hoc.2010.08.010. Epub 2010 Sep 29 [PubMed PMID: 21075278]
Origa R. β-Thalassemia. Genetics in medicine : official journal of the American College of Medical Genetics. 2017 Jun:19(6):609-619. doi: 10.1038/gim.2016.173. Epub 2016 Nov 3 [PubMed PMID: 27811859]
Galanello R, Origa R. Beta-thalassemia. Orphanet journal of rare diseases. 2010 May 21:5():11. doi: 10.1186/1750-1172-5-11. Epub 2010 May 21 [PubMed PMID: 20492708]
Ashiotis T, Zachariadis Z, Sofroniadou K, Loukopoulos D, Stamatoyannopoulos G. Thalassaemia in Cyprus. British medical journal. 1973 Apr 7:2(5857):38-42 [PubMed PMID: 4695698]
Shayeghi M, Latunde-Dada GO, Oakhill JS, Laftah AH, Takeuchi K, Halliday N, Khan Y, Warley A, McCann FE, Hider RC, Frazer DM, Anderson GJ, Vulpe CD, Simpson RJ, McKie AT. Identification of an intestinal heme transporter. Cell. 2005 Sep 9:122(5):789-801 [PubMed PMID: 16143108]
Fuqua BK, Vulpe CD, Anderson GJ. Intestinal iron absorption. Journal of trace elements in medicine and biology : organ of the Society for Minerals and Trace Elements (GMS). 2012 Jun:26(2-3):115-9. doi: 10.1016/j.jtemb.2012.03.015. Epub 2012 May 8 [PubMed PMID: 22575541]
Level 3 (low-level) evidenceLopez A, Cacoub P, Macdougall IC, Peyrin-Biroulet L. Iron deficiency anaemia. Lancet (London, England). 2016 Feb 27:387(10021):907-16. doi: 10.1016/S0140-6736(15)60865-0. Epub 2015 Aug 24 [PubMed PMID: 26314490]
Koorts AM, Viljoen M. Ferritin and ferritin isoforms I: Structure-function relationships, synthesis, degradation and secretion. Archives of physiology and biochemistry. 2007 Feb:113(1):30-54 [PubMed PMID: 17522983]
Kotze MJ, van Velden DP, van Rensburg SJ, Erasmus R. Pathogenic Mechanisms Underlying Iron Deficiency and Iron Overload: New Insights for Clinical Application. EJIFCC. 2009 Aug:20(2):108-23 [PubMed PMID: 27683335]
Özdemir N. Iron deficiency anemia from diagnosis to treatment in children. Turk pediatri arsivi. 2015 Mar:50(1):11-9. doi: 10.5152/tpa.2015.2337. Epub 2015 Mar 1 [PubMed PMID: 26078692]
Gaweda AE. Markers of iron status in chronic kidney disease. Hemodialysis international. International Symposium on Home Hemodialysis. 2017 Jun:21 Suppl 1(Suppl 1):S21-S27. doi: 10.1111/hdi.12556. Epub 2017 Mar 22 [PubMed PMID: 28328097]
Ning S, Zeller MP. Management of iron deficiency. Hematology. American Society of Hematology. Education Program. 2019 Dec 6:2019(1):315-322. doi: 10.1182/hematology.2019000034. Epub [PubMed PMID: 31808874]
Nerune SM, Rao H R S, Pallavi K, Lavate AP, Das SK, Pagi S. Optimizing the Diagnosis of Microcytic Hypochromic Anemia: A Comparative Evaluation of Erythrocyte and Reticulocyte Parameters. Cureus. 2024 Sep:16(9):e69244. doi: 10.7759/cureus.69244. Epub 2024 Sep 12 [PubMed PMID: 39398855]
Level 2 (mid-level) evidenceMassey AC. Microcytic anemia. Differential diagnosis and management of iron deficiency anemia. The Medical clinics of North America. 1992 May:76(3):549-66 [PubMed PMID: 1578956]
Musallam KM, Cappellini MD, Coates TD, Kuo KHM, Al-Samkari H, Sheth S, Viprakasit V, Taher AT. Αlpha-thalassemia: A practical overview. Blood reviews. 2024 Mar:64():101165. doi: 10.1016/j.blre.2023.101165. Epub 2024 Jan 3 [PubMed PMID: 38182489]
Level 3 (low-level) evidenceCazzola M. Ineffective erythropoiesis and its treatment. Blood. 2022 Apr 21:139(16):2460-2470. doi: 10.1182/blood.2021011045. Epub [PubMed PMID: 34932791]
Sanchez-Villalobos M, Blanquer M, Moraleda JM, Salido EJ, Perez-Oliva AB. New Insights Into Pathophysiology of β-Thalassemia. Frontiers in medicine. 2022:9():880752. doi: 10.3389/fmed.2022.880752. Epub 2022 Apr 12 [PubMed PMID: 35492364]
Lours C, Cottin L, Wiber M, Andrieu V, Baccini V, Baseggio L, Brouzes C, Chatelain B, Daliphard S, Fenneteau O, Geneviève F, Girard S, Leymarie V, Maloum K, Rieu JB, Sebahoun G, Sudaka I, Troussard X, Wagner-Ballon O, Wuilleme S, Bardet V, Lesesve JF. Perls' Stain Guidelines from the French-Speaking Cellular Hematology Group (GFHC). Diagnostics (Basel, Switzerland). 2022 Jul 12:12(7):. doi: 10.3390/diagnostics12071698. Epub 2022 Jul 12 [PubMed PMID: 35885602]
Mitra P, Sharma S, Purohit P, Sharma P. Clinical and molecular aspects of lead toxicity: An update. Critical reviews in clinical laboratory sciences. 2017 Nov-Dec:54(7-8):506-528. doi: 10.1080/10408363.2017.1408562. Epub 2017 Dec 7 [PubMed PMID: 29214886]
Zhao Y, Wu J, Xu H, Li Q, Zhang Y, Zhai Y, Tang M, Liu Y, Liu T, Ye Y, He M, He R, Xu Y, Zhou Z, Kan H, Zhang Y. Lead exposure suppresses the Wnt3a/β-catenin signaling to increase the quiescence of hematopoietic stem cells via reducing the expression of CD70 on bone marrow-resident macrophages. Toxicological sciences : an official journal of the Society of Toxicology. 2023 Aug 29:195(1):123-142. doi: 10.1093/toxsci/kfad067. Epub [PubMed PMID: 37436718]
Chan NCN, Chan KP. Coarse basophilic stippling in lead poisoning. Blood. 2017 Jun 15:129(24):3270. doi: 10.1182/blood-2017-03-773499. Epub [PubMed PMID: 28620106]
Tsai MT, Huang SY, Cheng SY. Lead Poisoning Can Be Easily Misdiagnosed as Acute Porphyria and Nonspecific Abdominal Pain. Case reports in emergency medicine. 2017:2017():9050713. doi: 10.1155/2017/9050713. Epub 2017 May 29 [PubMed PMID: 28630774]
Level 3 (low-level) evidenceSanchez JR, Lynch DT. Histology, Basophilic Stippling. StatPearls. 2026 Jan:(): [PubMed PMID: 31424843]
Bain BJ. Lead poisoning. American journal of hematology. 2014 Dec:89(12):1141. doi: 10.1002/ajh.23852. Epub 2014 Sep 26 [PubMed PMID: 25220013]
Rector WG Jr. Pica: its frequency and significance in patients with iron-deficiency anemia due to chronic gastrointestinal blood loss. Journal of general internal medicine. 1989 Nov-Dec:4(6):512-3 [PubMed PMID: 2585159]
Bermejo F, García-López S. A guide to diagnosis of iron deficiency and iron deficiency anemia in digestive diseases. World journal of gastroenterology. 2009 Oct 7:15(37):4638-43 [PubMed PMID: 19787826]
Tunnessen WW, Smith C, Oski FA. Beeturia. A sign of iron deficiency. American journal of diseases of children (1960). 1969 Apr:117(4):424-6 [PubMed PMID: 5773410]
Muñoz M, Gómez-Ramírez S, Besser M, Pavía J, Gomollón F, Liumbruno GM, Bhandari S, Cladellas M, Shander A, Auerbach M. Current misconceptions in diagnosis and management of iron deficiency. Blood transfusion = Trasfusione del sangue. 2017 Sep:15(5):422-437. doi: 10.2450/2017.0113-17. Epub [PubMed PMID: 28880842]
Peyrin-Biroulet L, Williet N, Cacoub P. Guidelines on the diagnosis and treatment of iron deficiency across indications: a systematic review. The American journal of clinical nutrition. 2015 Dec:102(6):1585-94. doi: 10.3945/ajcn.114.103366. Epub 2015 Nov 11 [PubMed PMID: 26561626]
Level 1 (high-level) evidenceClark SF. Iron deficiency anemia: diagnosis and management. Current opinion in gastroenterology. 2009 Mar:25(2):122-8. doi: 10.1097/MOG.0b013e32831ef1cd. Epub [PubMed PMID: 19262200]
Level 3 (low-level) evidenceBrugnara C, Schiller B, Moran J. Reticulocyte hemoglobin equivalent (Ret He) and assessment of iron-deficient states. Clinical and laboratory haematology. 2006 Oct:28(5):303-8 [PubMed PMID: 16999719]
Pantopoulos K. Oral iron supplementation: new formulations, old questions. Haematologica. 2024 Sep 1:109(9):2790-2801. doi: 10.3324/haematol.2024.284967. Epub 2024 Sep 1 [PubMed PMID: 38618666]
DeLoughery TG, Jackson CS, Ko CW, Rockey DC. AGA Clinical Practice Update on Management of Iron Deficiency Anemia: Expert Review. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2024 Aug:22(8):1575-1583. doi: 10.1016/j.cgh.2024.03.046. Epub 2024 Jun 12 [PubMed PMID: 38864796]
Boggs DR. Fate of a ferrous sulfate prescription. The American journal of medicine. 1987 Jan:82(1):124-8 [PubMed PMID: 3799670]
Pasupathy E, Kandasamy R, Thomas K, Basheer A. Alternate day versus daily oral iron for treatment of iron deficiency anemia: a randomized controlled trial. Scientific reports. 2023 Feb 1:13(1):1818. doi: 10.1038/s41598-023-29034-9. Epub 2023 Feb 1 [PubMed PMID: 36725875]
Level 1 (high-level) evidenceVan Doren L, Steinheiser M, Boykin K, Taylor KJ, Menendez M, Auerbach M. Expert consensus guidelines: Intravenous iron uses, formulations, administration, and management of reactions. American journal of hematology. 2024 Jul:99(7):1338-1348. doi: 10.1002/ajh.27220. Epub 2024 Jan 29 [PubMed PMID: 38282557]
Level 3 (low-level) evidenceGlaspy JA, Wolf M, Strauss WE. Intravenous Iron-Induced Hypophosphatemia: An Emerging Syndrome. Advances in therapy. 2021 Jul:38(7):3531-3549. doi: 10.1007/s12325-021-01770-2. Epub 2021 May 30 [PubMed PMID: 34053011]
Level 3 (low-level) evidenceBenson AE, Shatzel JJ, Ryan KS, Hedges MA, Martens K, Aslan JE, Lo JO. The incidence, complications, and treatment of iron deficiency in pregnancy. European journal of haematology. 2022 Dec:109(6):633-642. doi: 10.1111/ejh.13870. Epub 2022 Oct 4 [PubMed PMID: 36153674]
Cappellini MD, Taher AT. The use of luspatercept for thalassemia in adults. Blood advances. 2021 Jan 12:5(1):326-333. doi: 10.1182/bloodadvances.2020002725. Epub [PubMed PMID: 33570654]
Level 3 (low-level) evidenceJariwala K, Mishra K, Ghosh K. Comparative study of alloimmunization against red cell antigens in sickle cell disease & thalassaemia major patients on regular red cell transfusion. The Indian journal of medical research. 2019 Jan:149(1):34-40. doi: 10.4103/ijmr.IJMR_940_17. Epub [PubMed PMID: 31115372]
Level 2 (mid-level) evidenceSarkar SK, Shah MS, Begum M, Yunus AM, Aziz MA, Kabir AL, Khan MR, Rahman F, Rahman A. Red Cell Alloantibodies in Thalassaemia Patients Who Received Ten or More Units of Transfusion. Mymensingh medical journal : MMJ. 2019 Apr:28(2):364-369 [PubMed PMID: 31086152]
Darvishi Khezri H, Emami Zeydi A, Sharifi H, Jalali H. Is Vitamin C Supplementation in Patients with β-Thalassemia Major Beneficial or Detrimental? Hemoglobin. 2016 Aug:40(4):293-4. doi: 10.1080/03630269.2016.1190373. Epub [PubMed PMID: 27492769]
Farmakis D, Porter J, Taher A, Domenica Cappellini M, Angastiniotis M, Eleftheriou A. 2021 Thalassaemia International Federation Guidelines for the Management of Transfusion-dependent Thalassemia. HemaSphere. 2022 Aug:6(8):e732. doi: 10.1097/HS9.0000000000000732. Epub 2022 Jul 29 [PubMed PMID: 35928543]
Wengrovitz AM, Brown MJ, Advisory Committee on Childhood Lead Poisoning, Division of Environmental and Emergency Health Services, National Center for Environmental Health, Centers for Disease Control and Prevention. Recommendations for blood lead screening of Medicaid-eligible children aged 1-5 years: an updated approach to targeting a group at high risk. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports. 2009 Aug 7:58(RR-9):1-11 [PubMed PMID: 19661858]
Level 1 (high-level) evidenceKosnett MJ, Wedeen RP, Rothenberg SJ, Hipkins KL, Materna BL, Schwartz BS, Hu H, Woolf A. Recommendations for medical management of adult lead exposure. Environmental health perspectives. 2007 Mar:115(3):463-71 [PubMed PMID: 17431500]
Level 3 (low-level) evidenceCOUNCIL ON ENVIRONMENTAL HEALTH. Prevention of Childhood Lead Toxicity. Pediatrics. 2016 Jul:138(1):. pii: e20161493. doi: 10.1542/peds.2016-1493. Epub 2016 Jun 20 [PubMed PMID: 27325637]
Abbaspour N, Hurrell R, Kelishadi R. Review on iron and its importance for human health. Journal of research in medical sciences : the official journal of Isfahan University of Medical Sciences. 2014 Feb:19(2):164-74 [PubMed PMID: 24778671]
Miller JL. Iron deficiency anemia: a common and curable disease. Cold Spring Harbor perspectives in medicine. 2013 Jul 1:3(7):. doi: 10.1101/cshperspect.a011866. Epub 2013 Jul 1 [PubMed PMID: 23613366]
Level 3 (low-level) evidenceLynch SR, Hurrell RF, Dassenko SA, Cook JD. The effect of dietary proteins on iron bioavailability in man. Advances in experimental medicine and biology. 1989:249():117-32 [PubMed PMID: 2658489]
Level 3 (low-level) evidenceBjörn-Rasmussen E, Hallberg L. Effect of animal proteins on the absorption of food iron in man. Nutrition and metabolism. 1979:23(3):192-202 [PubMed PMID: 570683]
Level 3 (low-level) evidenceTaylor PG, Martínez-Torres C, Romano EL, Layrisse M. The effect of cysteine-containing peptides released during meat digestion on iron absorption in humans. The American journal of clinical nutrition. 1986 Jan:43(1):68-71 [PubMed PMID: 3942093]
Lynch SR, Cook JD. Interaction of vitamin C and iron. Annals of the New York Academy of Sciences. 1980:355():32-44 [PubMed PMID: 6940487]
Level 3 (low-level) evidenceConrad ME, Schade SG. Ascorbic acid chelates in iron absorption: a role for hydrochloric acid and bile. Gastroenterology. 1968 Jul:55(1):35-45 [PubMed PMID: 5663503]
Level 3 (low-level) evidenceCarpenter CE, Mahoney AW. Contributions of heme and nonheme iron to human nutrition. Critical reviews in food science and nutrition. 1992:31(4):333-67 [PubMed PMID: 1581009]
Sharma S, Khandelwal R, Yadav K, Ramaswamy G, Vohra K. Effect of cooking food in iron-containing cookware on increase in blood hemoglobin level and iron content of the food: A systematic review. Nepal journal of epidemiology. 2021 Jun:11(2):994-1005. doi: 10.3126/nje.v11i2.36682. Epub 2021 Jun 30 [PubMed PMID: 34290890]
Level 1 (high-level) evidence